Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study



Abstract
1. Introduction
2. Material and Methods
2.1. Data Sources
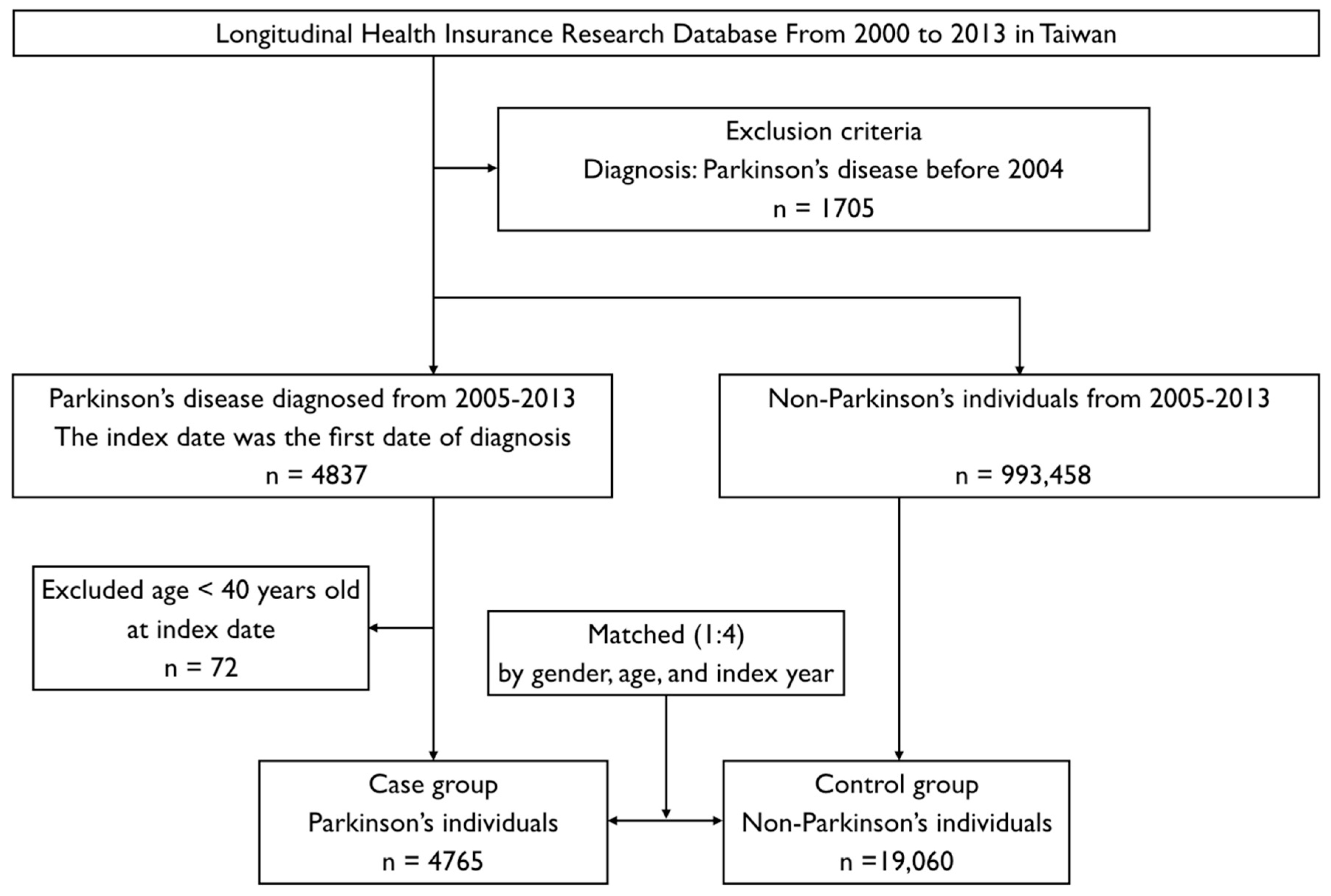
2.2. Study Design and Sampled Individuals
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of interest
References
- Kaur, T.; Uppoor, A.; Naik, D. Parkinson’s disease and periodontitis—The missing link? A review. Gerodontology 2016, 33, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Van Den Eeden, S.K.; Tanner, C.M.; Bernstein, A.L.; Fross, R.D.; Leimpeter, A.; Bloch, D.A.; Nelson, L.M. Incidence of Parkinson’s disease: Variation by age, gender, and race/ethnicity. Am. J. Epidemiol. 2003, 157, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.M.; Wu, R.M.; Lin, J.W.; Liu, Y.C.; Chang, C.H.; Lin, C.H. Time trends in the prevalence and incidence of Parkinson’s disease in Taiwan: A nationwide, population-based study. J. Formos. Med. Assoc. 2016, 115, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Diederich, N.J.; Moore, C.G.; Leurgans, S.E.; Chmura, T.A.; Goetz, C.G. Parkinson disease with old-age onset: A comparative study with subjects with middle-age onset. Arch. Neurol. 2003, 60, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.F.; Wagner, H.N., Jr.; Dannals, R.F.; Links, J.M.; Frost, J.J.; Ravert, H.T.; Wilson, A.A.; Rosenbaum, A.E.; Gjedde, A.; Douglass, K.H.; et al. Effects of age on dopamine and serotonin receptors measured by positron tomography in the living human brain. Science 1984, 226, 1393–1396. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.H.; Lee, W.J.; Chen, Y.H.; Chang, M.H.; Lin, C.H. Premotor Symptoms as Predictors of Outcome in Parkinsons Disease: A Case-Control Study. PLoS ONE 2016, 11, e0161271. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Cappelli, D. Acute-phase reactants in infections and inflammatory diseases. Periodontology 2000 2000, 23, 19–49. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Periodontal inflammatory disease is associated with the risk of Parkinson’s disease: A population-based retrospective matched-cohort study. PeerJ 2017, 5, e3647. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.G. The effect of subgingival scaling on gingival inflammation. J. Periodontol. 1969, 40, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Ho Chan, W.S. Taiwan’s healthcare report 2010. EPMA J. 2010, 1, 563–585. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Wahlqvist, M.L.; Lee, M.S.; Tsai, H.N. Incidence of dementia is increased in type 2 diabetes and reduced by the use of sulfonylureas and metformin. J. Alzheimers Dis. 2011, 24, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Romano, P.S.; Roos, L.L.; Jollis, J.G. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: Differing perspectives. J. Clin. Epidemiol. 1993, 46, 1075–1079; discussion 1081–1090. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chung, C.H.; Yeh, C.B.; Huang, R.Y.; Yuh, D.Y.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Chiang, W.S.; et al. Are Chronic Periodontitis and Gingivitis Associated with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Yang, Y.W.; Hsieh, T.F.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Chiang, J.H.; Li, T.C.; Lin, C.C. Increased risk of Parkinson disease with diabetes mellitus in a population-based study. Medicine 2017, 96, e5921. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.P.; Yang, C.J.; Hu, K.F.; Chao, A.C.; Chang, Y.H.; Hsieh, K.P.; Tsai, J.H.; Ho, P.S.; Lim, S.Y. Risk factors for pneumonia among patients with Parkinson’s disease: A Taiwan nationwide population-based study. Neuropsychiatr. Dis. Treat. 2016, 12, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, Z.; Mele, B.; Guo, S.; Hanson, H.; Jette, N.; Patten, S.; Pringsheim, T.; Holroyd-Leduc, J. Guidelines for dementia or Parkinson’s disease with depression or anxiety: A systematic review. BMC Neurol. 2016, 16, 244. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.C.; Chang, C.W.; Lee, H.L.; Chuang, C.C.; Chiu, H.C.; Li, W.Y.; Horng, J.T.; Fu, E. Association between History of Dental Amalgam Fillings and Risk of Parkinson’s Disease: A Population-Based Retrospective Cohort Study in Taiwan. PLoS ONE 2016, 11, e0166552. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.C.; Sheu, J.J.; Lin, H.C.; Jensen, D.A. Increased risk of Parkinsonism following chronic periodontitis: A retrospective cohort study. Mov. Disord. 2013, 28, 1307–1308. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.; Lin, Y.C.; Hong, L.Y.; Chen, T.T.; Ma, H.P.; Hsu, Y.H.; Tsai, S.H.; Lin, Y.F.; Wu, M.Y. Increased Long-Term Risk of Dementia in Patients With Carbon Monoxide Poisoning: A Population-Based Study. Medicine 2016, 95, e2549. [Google Scholar] [CrossRef] [PubMed]
- Bohatschek, M.; Werner, A.; Raivich, G. Systemic LPS injection leads to granulocyte influx into normal and injured brain: Effects of ICAM-1 deficiency. Exp. Neurol. 2001, 172, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal infections contribute to elevated systemic C-reactive protein level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Association between chronic periodontitis and the risk of Alzheimer’s disease: A retrospective, population-based, matched-cohort study. Alzheimers Res. Ther. 2017, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.M.; Buchanan, S.A.; Hoover, C.I.; Newbrun, E.; Taggart, E.J.; Armitage, G.C.; Robertson, P.B. Clinical and microbiologic effects of single-dose metronidazole or scaling and root planing in treatment of adult periodontitis. J. Clin. Periodontol. 1986, 13, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, P.B.; Brennan, M.T.; Thornhill, M.; Michalowicz, B.S.; Noll, J.; Bahrani-Mougeot, F.K.; Sasser, H.C. Poor oral hygiene as a risk factor for infective endocarditis-related bacteremia. J. Am. Dent. Assoc. 2009, 140, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, A.R.; Singh, S.P.; Martande, S.S.; Raju, A.P.; Rustagi, T.; Suke, D.K.; Naik, S.B. Clinical evaluation of the periodontal health condition and oral health awareness in Parkinson’s disease patients. Gerodontology 2015, 32, 100–106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Control Group without PD n = 19,060 | Case Group with PD n = 4765 | p-Value |
|---|---|---|---|
| Sex | 1.0000 | ||
| Female | 9624 (50.49%) | 2406 (50.49%) | |
| Male | 9436 (49.51%) | 2359 (49.51%) | |
| Age | 1.0000 | ||
| 40–69 | 5552 (29.13%) | 1388 (29.13%) | |
| ≥70 | 13,508 (70.87%) | 3377 (70.87%) | |
| Urbanization | <0.0001 | ||
| Level 1 | 10,369 (54.40%) | 2440 (51.21%) | |
| Level 2 | 5642 (29.60%) | 1256 (26.36%) | |
| Level 3 | 3049 (16.00%) | 1069 (22.43%) | |
| Comorbidities | |||
| Periodontal inflammatory disease | 8554 (44.88%) | 2322 (48.73%) | <0.0001 |
| Diabetes mellitus | 6925 (36.33%) | 2146 (45.04%) | <0.0001 |
| Hypertension | 13,151 (69.00%) | 3784 (79.41%) | <0.0001 |
| Hyperlipidemia | 9066 (47.57%) | 2601 (54.59%) | <0.0001 |
| Chronic kidney disease | 4996 (26.21%) | 1658 (34.80%) | <0.0001 |
| Depression | 646 (3.39%) | 447 (9.38%) | <0.0001 |
| Stroke | 3217 (16.88%) | 1669 (35.03%) | <0.0001 |
| Traumatic brain injury | 5678 (29.79%) | 2598 (54.52%) | <0.0001 |
| Dental scaling * | <0.0001 | ||
| No treatment | 9773 (51.27%) | 2282 (47.89%) | |
| Not 5 consecutive years | 8615 (45.2%) | 2336 (49.02%) | |
| For 5 consecutive years | 672 (3.53%) | 147 (3.08%) |
| Variables | Individuals | Multivariable Analysis | ||
|---|---|---|---|---|
| aOR | 95% CI | p-Value | ||
| Subgroup 1: 40–69 years old | ||||
| No treatment without PID | 2336 | Reference | - | - |
| Not 5 consecutive years without PID | 1001 | 0.943 | 0.770–1.155 | 0.5698 |
| For 5 consecutive years without PID | 35 | 0.204 | 0.047–0.886 | 0.0339 |
| No treatment with PID | 515 | 1.030 | 0.801–1.324 | 0.8159 |
| Not 5 consecutive years with PID | 2781 | 1.056 | 0.908–1.228 | 0.4763 |
| For 5 consecutive years with PID | 272 | 0.718 | 0.495–1.040 | 0.0796 |
| Subgroup 2: ≥70 years old | ||||
| No treatment without PID | 7645 | Reference | - | - |
| Not 5 consecutive years without PID | 1866 | 1.171 | 1.026–1.336 | 0.0192 |
| For 5 consecutive years without PID | 66 | 1.132 | 0.604–2.124 | 0.6986 |
| No treatment with PID | 1559 | 1.160 | 1.008–1.336 | 0.0387 |
| Not 5 consecutive years with PID | 5303 | 1.234 | 1.123–1.356 | <0.0001 |
| For 5 consecutive years with PID | 446 | 1.133 | 0.885–1.452 | 0.3217 |
| Annual Dental Scaling without PID | aOR | 95% CI | p-Value |
|---|---|---|---|
| Within 1 year before index date | 0.974 | 0.731–1.297 | 0.856 |
| 2 consecutive years before index date | 0.742 | 0.464–1.187 | 0.213 |
| 3 consecutive years before index date | 0.479 | 0.23–0.998 | 0.049 |
| 4 consecutive years before index date | 0.233 | 0.07–0.774 | 0.017 |
| 5 consecutive years before index date | 0.204 | 0.05–0.886 | 0.034 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-K.; Huang, J.-Y.; Wu, Y.-T.; Chang, Y.-C. Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. Int. J. Environ. Res. Public Health 2018, 15, 1587. https://doi.org/10.3390/ijerph15081587
Chen C-K, Huang J-Y, Wu Y-T, Chang Y-C. Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. International Journal of Environmental Research and Public Health. 2018; 15(8):1587. https://doi.org/10.3390/ijerph15081587
Chicago/Turabian StyleChen, Chang-Kai, Jing-Yang Huang, Yung-Tsan Wu, and Yu-Chao Chang. 2018. "Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study" International Journal of Environmental Research and Public Health 15, no. 8: 1587. https://doi.org/10.3390/ijerph15081587
APA StyleChen, C.-K., Huang, J.-Y., Wu, Y.-T., & Chang, Y.-C. (2018). Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. International Journal of Environmental Research and Public Health, 15(8), 1587. https://doi.org/10.3390/ijerph15081587