Pathways from Food Consumption Score to Cardiovascular Disease: A Seven-Year Follow-Up Study of Indonesian Adults




Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collections and Participants
2.2. Outcome Definitions
2.3. Blood Pressures and Physical Activity
2.4. Obesity Measures
2.5. Food Consumption Score and Sociodemographic Characteristics
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Assessment of Food Consumption Score and Obesity
3.3. Assessment of Physical Activity, Blood Pressure, and Health Outcome
3.4. Correlation of the Proposed Variables for the SEM
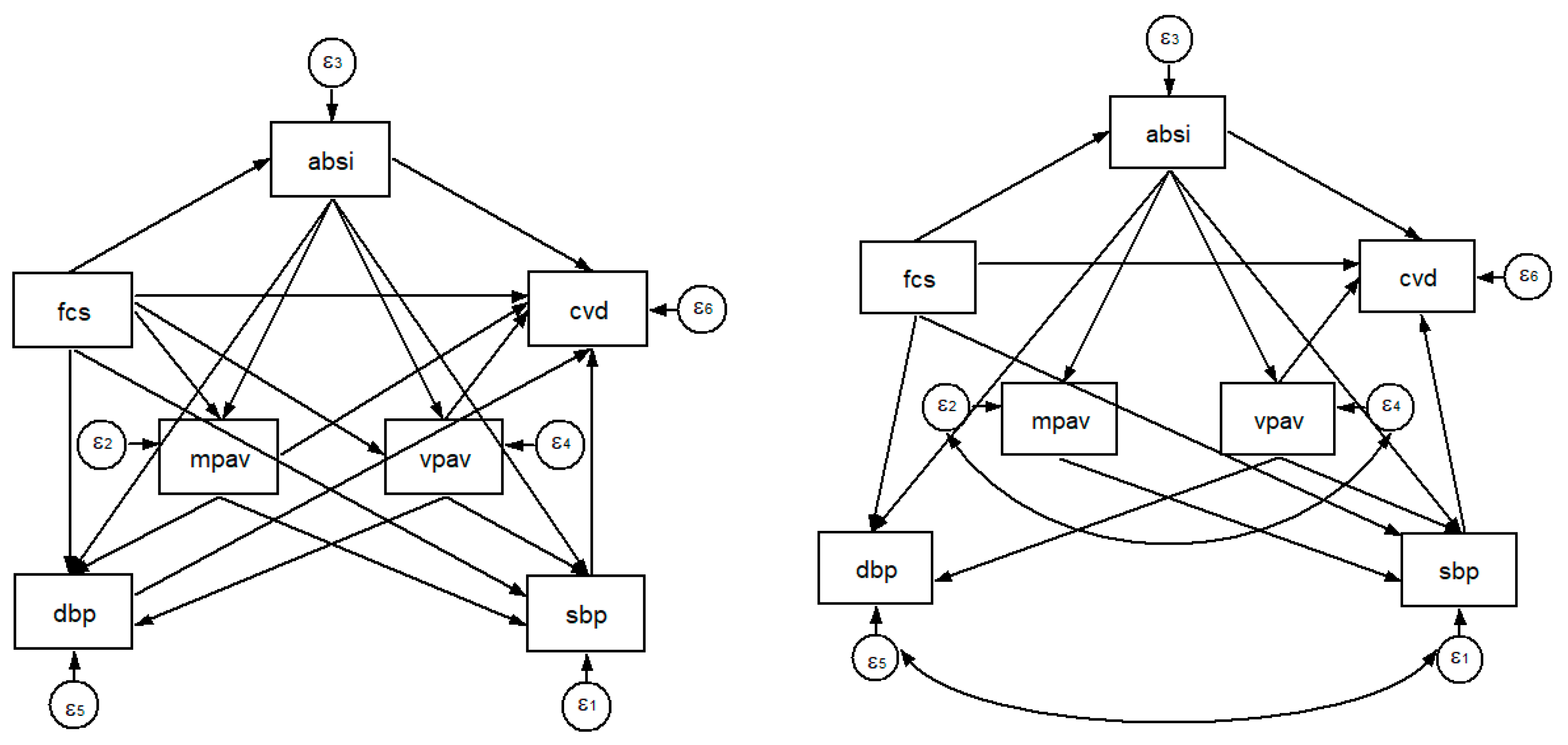
3.5. The SEM and Path Analysis
4. Discussion
4.1. Pathways from FCS to ABSI
4.2. Pathways from ABSI to MPAV and VPAV
4.3. Pathways from FCS to SBP and DBP
4.4. Pathways from FCS to CVD
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Seligman, H.K.; Laraia, B.A.; Kushel, M.B. Food insecurity is associated with chronic disease among low-income nhanes participants. J. Nutr. 2010, 140, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.; Jones, A.; Love, D.; Puckett, S.; Macklin, J.; White-Means, S. Exploring mediators of food insecurity and obesity: A review of recent literature. J. Community Health 2012, 37, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A. Food insecurity and chronic disease. Adv. Nutr. 2013, 4, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Wilde, P.E.; Peterman, J.N. Individual weight change is associated with household food security status. J. Nutr. 2006, 136, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Webb, P.; Coates, J.; Frongillo, E.A.; Rogers, B.L.; Swindale, A.; Bilinsky, P. Measuring household food insecurity: Why it’s so important and yet so difficult to do. J. Nutr. 2006, 136, 1404–1408. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.L.; Schiff, A.; Currivan, D.; Villamor, E. Food stamp program participation but not food insecurity is associated with higher adult bmi in massachusetts residents living in low-income neighbourhoods. Public Health Nutr. 2008, 11, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- World Food Programme. Food Consumption Score Nutritional Quality Analysis Guidelines (FCS-N); United Nations World Food Programme, Food security analysis (VAM): Rome, Italy, 2015. [Google Scholar]
- Seligman, H.K.; Bindman, A.B.; Vittinghoff, E.; Kanaya, A.M.; Kushel, M.B. Food insecurity is associated with diabetes mellitus: Results from the national health examination and nutrition examination survey (nhanes) 1999–2002. J. Gen. Intern. Med. 2007, 22, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Schillinger, D. Hunger and socioeconomic disparities in chronic disease. N. Engl. J. Med. 2010, 363, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, S.A.; Baggett, T.P.; Wexler, D.J.; Huskey, K.W.; Wee, C.C. Food insecurity and metabolic control among u.S. Adults with diabetes. Diabetes Care 2013, 36, 3093–3099. [Google Scholar] [CrossRef] [PubMed]
- Isaura, E.R.; Chen, Y.C.; Yang, S.H. The association of food consumption scores, body shape index, and hypertension in a seven-year follow-up among indonesian adults: A longitudinal study. Int. J. Environ. Res. Public Health 2018, 15, 175. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Davis, T.C.; Schillinger, D.; Wolf, M.S. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J. Health Care Poor Underserved 2010, 21, 1227–1233. [Google Scholar] [PubMed]
- Mathiassen, A.; Hollema, S. What is the effect of physical activity level on food consumption, energy deficiency, and dietary diversity? Food Nutr. Bull. 2014, 35, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.A.; Glynn, R.J.; Buring, J.; Ridker, P.M. Impact of traditional and novel risk factors on the relationship between socioeconomic status and incident cardiovascular events. Circulation 2006, 114, 2619–2626. [Google Scholar] [CrossRef] [PubMed]
- Koolhaas, C.M.; Dhana, K.; Schoufour, J.D.; Ikram, M.A.; Kavousi, M.; Franco, O.H. Impact of physical activity on the association of overweight and obesity with cardiovascular disease: The rotterdam study. Eur. J. Prev. Cardiol. 2017, 24, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S. Global progress in prevention of cardiovascular disease. Cardiovasc. Diagn. Ther. 2017, 7, S32–S38. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Oh, C.M.; Choi, M.K.; Park, Y.K.; Chun, S.; Choi, M.; Yu, J.M.; Yoo, H.J. The influence of physical activity on risk of cardiovascular disease in people who are obese but metabolically healthy. PLoS ONE 2017, 12, e0185127. [Google Scholar] [CrossRef] [PubMed]
- Frankenberg, E.; Thomas, D. The Indonesia Family Life Survey (IFLS): Study Design and Results from Waves 1 and 2; DRU2238/1. NIA/NICHD; RAND: Santa Monica, CA, USA, 2000. [Google Scholar]
- Strauss, J.; Witoelar, F.; Sikoki, B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report; RAND: Santa Monica, CA, USA, 2016. [Google Scholar]
- Mendis, S.; Puska, P.; Norrving, B. Global Atlas on Cardiovascular Disease Prevention and Control; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Bell, K.; Twiggs, J.; Olin, B.R.; Date, I.R. Hypertension: The Silent Killer: Updated jnc-8 Guideline Recommendations; Alabama Pharmacy Association: Montgomery, AL, USA, 2015. [Google Scholar]
- Liu, X.; Zhang, D.; Liu, Y.; Sun, X.; Han, C.; Wang, B.; Ren, Y.; Zhou, J.; Zhao, Y.; Shi, Y.; et al. Dose-response association between physical activity and incident hypertension: A systematic review and meta-analysis of cohort studies. Hypertension 2017, 69, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.B. “A body shape index” in middle-age and older indonesian population: Scaling exponents and association with incident hypertension. PLoS ONE 2014, 9, e85421. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, G.R.; Auger, P.; Bogaty, P.; Gerstein, H.; Lonn, E.; Yi, Q.; Yusuf, S.; Investigators, H.S. Increased occurrence of diabetes in people with ischemic cardiovascular disease and general and abdominal obesity. Can. J. Cardiol. 2003, 19, 1387–1391. [Google Scholar] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- Indonesia, D.K.R.; Masyarakat, D.J.B.K.; Masyarakat, D.G. Petunjuk Teknis Pemantauan Status Gizi Orang Dewasa Dengan Indeks Massa Tubuh; Departemen Kesehatan RI: Jakarta, Indonesia, 2003; p. 27. [Google Scholar]
- United Nations World Food Programme-Food security analysis (VAM). Consolidated Approach to Reporting Indicators of Food Security (cari) Guidelines; United Nations World Food Programme, Food Security Analysis (VAM): Rome, Italy, 2015. [Google Scholar]
- Lander, R.L.; Williams, S.M.; Costa-Ribeiro, H.; Mattos, A.P.; Barreto, D.L.; Houghton, L.A.; Bailey, K.B.; Lander, A.G.; Gibson, R.S. Understanding the complex determinants of height and adiposity in disadvantaged daycare preschoolers in salvador, ne brazil through structural equation modelling. BMC Public Health 2015, 15, 1086. [Google Scholar] [CrossRef] [PubMed]
- Hardin, J.W.; Hilbe, J.M. Generalized Estimating Equations, 2nd ed.; CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2013. [Google Scholar]
- Zeger, S.L.; Liang, K.Y.; Albert, P.S. Models for longitudinal data: A generalized estimating equation approach. Biometrics 1988, 44, 1049–1060. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Sem: An introduction. In Multivariate Data Analysis: A Global Perspective, 7 ed.; Pearson: Hoboken, NJ, USA, 2010; pp. 629–686. [Google Scholar]
- Singleton, R., Jr.; Straits, B.C.; Straits, M.M.; McAllister, R.J. Approaches to Social Research, 5th ed.; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Stuff, J.E.; Casey, P.H.; Szeto, K.L.; Gossett, J.M.; Robbins, J.M.; Simpson, P.M.; Connell, C.; Bogle, M.L. Household food insecurity is associated with adult health status. J. Nutr. 2004, 134, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Alimoradi, M.; Ajami, M.; Abdollahi, M.; Ahari, G.K. A review of the relationship between obesity and food insecurity. Int. J. Med. Rev. 2016, 3, 381–388. [Google Scholar]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Does diet cost mediate the relation between socioeconomic position and diet quality? Eur. J. Clin. Nutr. 2011, 65, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Obesity and the food environment: Dietary energy density and diet costs. Am. J. Prev. Med. 2004, 27, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Sowers, J.R. Obesity as a cardiovascular risk factor. Am. J. Med. 2003, 115, 37–41. [Google Scholar] [CrossRef]
- Popkin, B.M.; Kim, S.; Rusev, E.R.; Du, S.; Zizza, C. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes Rev. 2006, 7, 271–293. [Google Scholar] [CrossRef] [PubMed]
- Pietilainen, K.H.; Kaprio, J.; Borg, P.; Plasqui, G.; Yki-Jarvinen, H.; Kujala, U.M.; Rose, R.J.; Westerterp, K.R.; Rissanen, A. Physical inactivity and obesity: A vicious circle. Obesity 2008, 16, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Roemling, C.; Qaim, M. Obesity trends and determinants in indonesia. Appetite 2012, 58, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Barning, F.; Abarin, T. Assessing the causality factors in the association between (abdominal) obesity and physical activity among the newfoundland population-a mendelian randomization analysis. Genet. Epigenet. 2016, 8, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, S.A.; Seligman, H.K.; Choudhry, N.K. Treat or eat: Food insecurity, cost-related medication underuse, and unmet needs. Am. J. Med. 2014, 127, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Siega-Riz, A.M.; Gundersen, C. Household food insecurity is associated with self-reported pregravid weight status, gestational weight gain, and pregnancy complications. J. Am. Diet. Assoc. 2010, 110, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, S.A.; Berkowitz, T.S.Z.; Meigs, J.B.; Wexler, D.J. Trends in food insecurity for adults with cardiometabolic disease in the united states: 2005–2012. PLoS ONE 2017, 12, e0179172. [Google Scholar] [CrossRef] [PubMed]
- Sowers, J.R.; Epstein, M.; Frohlich, E.D. Diabetes, hypertension, and cardiovascular disease: An update. Hypertension 2001, 37, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Mora, S.; Cook, N.; Buring, J.E.; Ridker, P.M.; Lee, I.M. Physical activity and reduced risk of cardiovascular events: Potential mediating mechanisms. Circulation 2007, 116, 2110–2118. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.A.; Al Mamun, A.; Peters, S.A.; Woodward, M.; Huxley, R.R. The burden of cardiovascular disease attributable to major modifiable risk factors in indonesia. J. Epidemiol. 2016, 26, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Zhang, X.; Xu, Y.; Dong, H. Feasibility of body roundness index for identifying a clustering of cardiometabolic abnormalities compared to bmi, waist circumference and other anthropometric indices: The china health and nutrition survey, 2008 to 2009. Medicine 2016, 95, e4642. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Bastien, M.; Poirier, P.; Lemieux, I.; Despres, J.P. Overview of epidemiology and contribution of obesity to cardiovascular disease. Prog. Cardiovasc. Dis. 2014, 56, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Krause, N.; van der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (opa) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Richmond, R.C.; Davey Smith, G.; Ness, A.R.; den Hoed, M.; McMahon, G.; Timpson, N.J. Assessing causality in the association between child adiposity and physical activity levels: A mendelian randomization analysis. PLoS Med. 2014, 11, e1001618. [Google Scholar] [CrossRef] [PubMed]
- Gunter, K.B.; Jackson, J.; Tomayko, E.J.; John, D.H. Food insecurity and physical activity insecurity among rural oregon families. Prev. Med. Rep. 2017, 8, 38–41. [Google Scholar] [CrossRef] [PubMed]
- World Food Programme. World Food Programme: Indonesia. Available online: http://www1.wfp.org/countries/indonesia (accessed on 10 May 2018).
- Ng, N.; Hakimi, M.; Van Minh, H.; Juvekar, S.; Razzaque, A.; Ashraf, A.; Masud Ahmed, S.; Kanungsukkasem, U.; Soonthornthada, K.; Huu Bich, T. Prevalence of physical inactivity in nine rural indepth health and demographic surveillance systems in five asian countries. Glob. Health Action 2009, 2, 1985. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Kelly, T.N.; Wu, X.; Chen, J.; Duan, X.; Huang, J.F.; Chen, J.C.; Whelton, P.K.; He, J. Blood pressure and risk of cardiovascular disease in chinese men and women. Am. J. Hypertens. 2008, 21, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; White, I.R.; Caulfield, M.J.; Deanfield, J.E.; Smeeth, L.; et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef]
- Franklin, S.S.; Gokhale, S.S.; Chow, V.H.; Larson, M.G.; Levy, D.; Vasan, R.S.; Mitchell, G.F.; Wong, N.D. Does low diastolic blood pressure contribute to the risk of recurrent hypertensive cardiovascular disease events? The framingham heart study. Hypertension 2015, 65, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Hasanah, A.; Mendolia, S.; Yerokhin, O. Labour migration, food expenditure, and household food security in eastern indonesia. Econ. Rec. 2017, 93, 122–143. [Google Scholar] [CrossRef]


{kind=link}
| Variable | All (N = 3955) | ||
|---|---|---|---|
| 2007 | 2014 | p Value a | |
| Age (years), mean | 47(5) | 54(5) | <0.001 |
| Gender, % | |||
| Women | 2056(51.98) | 2056(51.98) | |
| Men | 1899(48.02) | 1899(48.02) | |
| Education level, % | 0.614 | ||
| Low (<12 years) | 3041(76.89) | 3022(76.41) | |
| High (≥12 years) | 914(23.11) | 933(23.59) | |
| Marital status, % | 0.182 | ||
| Ever/Married | 3900(98.61) | 3913(98.94) | |
| Single/Never married | 55(1.39) | 42(1.06) | |
| Geographical residence, % | <0.001 | ||
| Rural | 1960(49.56) | 1651(41.74) | |
| Urban | 1995(50.44) | 2304(58.26) | |
| Smoking habit, % | 0.021 | ||
| No smoking | 2482(62.76) | 2382(60.23) | |
| Currently smoking | 1356(34.29) | 1291(32.64) | |
| Former smoking | 117(2.96) | 282(7.13) | |
| Food consumption score, mean | 52.02(22.76) | 34.81(15.77) | <0.001 |
| Food consumption group, % | <0.001 | ||
| Poor | 330(8.34) | 815(20.61) | |
| Borderline | 650(16.43) | 1278(32.31) | |
| Acceptable | 2975(75.22) | 1862(47.08) | |
| Vigorous physical activity volume (MET h/w), mean | 37.22(82.47) | 22.02(65.63) | <0.001 |
| Moderate physical activity volume (MET h/w), mean | 36.47(48.80) | 20.19(38.82) | <0.001 |
| Using cholesterol medication, % | <0.001 | ||
| No | 3955(100) | 3875(97.98) | |
| Yes | 0(0) | 80(2.02) | |
| Using diabetes medication, % | <0.001 | ||
| No | 3955(100) | 3879(98.08) | |
| Yes | 0(0) | 76(1.92) | |
| Using hypertension medication, % | <0.001 | ||
| No | 3955(100) | 3722(94.11) | |
| Yes | 0(0) | 233(5.89) | |
| Abdominal obesity b, % | <0.001 | ||
| No | 2328(58.86) | 1875(47.41) | |
| Yes | 1627(41.14) | 2080(52.59) | |
| Overweight c, % | <0.001 | ||
| No | 2575(65.11) | 2324(58.76) | |
| Yes | 1380(34.89) | 1631(41.24) | |
| WC (cm), mean | 82.60(10.23) | 86.11(10.75) | <0.001 |
| BMI (kg/m2), mean | 23.95(3.96) | 24.57(3.90) | <0.001 |
| ABSI (m11/6 kg−2/3), mean | 0.0801(0.0062) | 0.0821(0.0056) | <0.001 |
| SBP (mmHg), mean | 135(21) | 143(25) | <0.001 |
| DBP (mmHg), mean | 83(12) | 85(14) | <0.001 |
| Hypertension d, % | <0.001 | ||
| No | 2392(60.48) | 1905(48.17) | |
| Yes | 1563(39.52) | 2050(51.83) | |
| Heart disease, % | <0.001 | ||
| No | 3955(100) | 3874(97.95) | |
| Yes | 0(0) | 81(2.05) | |
| Stroke, % | <0.001 | ||
| No | 3955(100) | 3919(99.09) | |
| Yes | 0(0) | 36(0.91) | |
| Cardiovascular disease e, % | <0.001 | ||
| No | 3955(100) | 3841(97.12) | |
| Yes | 0(0) | 114(2.88) | |
| Diabetes, % | <0.001 | ||
| No | 3955(100) | 3789(95.80) | |
| Yes | 0(0) | 166(4.20) | |
| FCS a | ABSI | VPAV | MPAV | SBP | DBP | CVD | |
|---|---|---|---|---|---|---|---|
| FCS a | 1.000 | ||||||
| ABSI | −0.057 ** | 1.000 | |||||
| VPAV | −0.003 | −0.114 ** | 1.000 | ||||
| MPAV | 0.058 ** | −0.075 ** | 0.224 ** | 1.000 | |||
| SBP | −0.123 ** | 0.127 ** | −0.075 ** | −0.067 ** | 1.000 | ||
| DBP | −0.045 ** | 0.078 ** | −0.084 ** | −0.043 ** | 0.767 ** | 1.000 | |
| CVD | −0.049 ** | 0.036 * | −0.036 * | −0.027 * | 0.059 * | 0.042 ** | 1.000 |
| DV | IV | Unadjusted | Model 1 | Model 2 | Model 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β Coef. | CI | p-Value | β Coef. | CI | p-Value | β Coef. | CI | p-Value | β Coef. | CI | p-Value | ||
| SBP | FCS a | −0.13 | (−0.16, −0.11) | <0.001 | −0.08 | (−0.10, −0.05) | <0.001 | −0.08 | (−0.10, −0.05) | <0.001 | −0.08 | (−0.11, −0.06) | <0.001 |
| ABSI | 497.29 | (411.49, 583.09) | <0.001 | 263.16 | (176.24, 350.08) | <0.001 | 263.30 | (176.37, 350.23) | <0.001 | 261.95 | (175.08, 348.82) | <0.001 | |
| VPAV | −2.34 × 10−2 | (−3.03 × 10−2, −1.65 × 10−2) | <0.001 | −1.31 × 10−2 | (−2.00 × 10−2, −6.17 × 10−3) | <0.001 | −1.35 × 10−2 | (−2.05 × 10−2, −6.49 × 10−3) | <0.001 | −1.30 × 10−2 | (−2.00 × 10−2, −5.96 × 10−3) | <0.001 | |
| MPAV | −3.53 × 10−2 | (−4.68 × 10−2, −2.38 × 10−2) | <0.001 | −1.58 × 10−2 | (−2.72 × 10−2, −4.50 × 10−3) | 0.006 | −1.60 × 10−2 | (−2.73 × 10−2, −4.60 × 10−3) | 0.006 | −1.62 × 10−2 | (−2.76 × 10−2, −4.85 × 10−3) | 0.005 | |
| DBP | FCS a | −0.03 | (−0.04, −0.01) | <0.001 | −0.02 | (−0.03, −0.01) | 0.003 | −0.03 | (−0.04, −0.01) | <0.001 | −0.03 | (−0.04, −0.01) | <0.001 |
| ABSI | 168.26 | (120.76, 215.76) | <0.001 | 143.27 | (93.99, 192.55) | <0.001 | 141.44 | (92.23, 190.64) | <0.001 | 140.67 | (91.50, 189.85) | <0.001 | |
| VPAV | −1.45 × 10−2 | (−1.83 × 10−2, −1.07 × 10−2) | <0.001 | −1.31 × 10−2 | (−1.70 × 10−2, −9.19 × 10−3) | <0.001 | −1.18 × 10−2 | (−1.58 × 10−2, −7.83 × 10−3) | <0.001 | −1.15 × 10−2 | (−1.55 × 10−2, −7.54 × 10−3) | <0.001 | |
| MPAV | −1.25 × 10−2 | (−1.89 × 10−2, −6.19 × 10−3) | <0.001 | −1.03 × 10−2 | (−1.67 × 10−2, −3.86 × 10−3) | 0.002 | −9.21 × 10−3 | (−1.56 × 10−2, −2.79 × 10−3) | 0.005 | −9.35 × 10−3 | (−1.58 × 10−2, −2.93 × 10−3) | 0.004 | |
| VPAV | FCS a | −0.01 | (−0.09, 0.07) | 0.779 | −0.10 | (−0.18, −0.03) | 0.008 | −0.01 | (−0.09, 0.07) | 0.800 | −3.47 × 10−3 | (−8.05 × 10−2, 7.36 × 10−2) | 0.930 |
| ABSI | −1430.28 | (−1704.20, −1156.36) | <0.001 | −877.46 | (−1154.20, −600.72) | <0.001 | −848.37 | (−1121.64, −575.10) | <0.001 | −843.14 | (−1116.13, −570.14) | <0.001 | |
| MPAV | FCS a | 0.12 | (0.08, 0.17) | <0.001 | 4.90 × 10−2 | (2.06 × 10−3, 9.59 × 10−2) | 0.041 | 0.08 | (0.03, 0.12) | 0.002 | 0.07 | (0.03, 0.12) | 0.002 |
| ABSI | −560.45 | (−725.02, −395.88) | <0.001 | −277.39 | (−446.58, −108.20) | 0.001 | −269.95 | (−438.78, −101.11) | 0.002 | −270.84 | (−439.67, −102.01) | 0.002 | |
| Pathway | Model for Cardiovascular Diseases | ||||
|---|---|---|---|---|---|
| Coef. | SE | z | p Value | CI | |
| Direct | |||||
| ABSI ← FCS | −0.057 | 0.011 | −5.13 | <0.001 | (−0.079, −0.035) |
| MPAV ← ABSI | −0.075 | 0.011 | −6.69 | <0.001 | (−0.097, −0.053) |
| VPAV ← ABSI | −0.114 | 0.011 | −10.3 | <0.001 | (−0.136, −0.093) |
| Indirect | |||||
| SBP ← | |||||
| ABSI | 0.112 | 0.011 | 10.09 | <0.001 | (0.090, 0.133) |
| FCS | −0.115 | 0.011 | −10.5 | <0.001 | (−0.137, −0.094) |
| MPAV | −0.025 | 0.007 | −3.46 | 0.001 | (−0.040, −0.011) |
| VPAV | −0.057 | 0.011 | −5.05 | <0.001 | (−0.079, −0.035) |
| DBP ← | |||||
| ABSI | 0.067 | 0.011 | 5.94 | <0.001 | (0.045, 0.089) |
| FCS | −0.041 | 0.011 | −3.71 | <0.001 | (−0.063, −0.020) |
| VPAV | −0.077 | 0.011 | −6.83 | <0.001 | (−0.098, −0.055) |
| CVD ← | |||||
| ABSI | 0.024 | 0.011 | 2.12 | 0.034 | (0.002, 0.046) |
| FCS | −0.042 | 0.011 | −3.73 | <0.001 | (−0.064, −0.020) |
| SBP | 0.049 | 0.011 | 4.29 | <0.001 | (0.026, 0.071) |
| VPAV | −0.030 | 0.011 | −2.66 | 0.008 | (−0.052, −0.008) |
| Correlation | |||||
| SBP ← DBP | 0.766 | 0.005 | 165.1 | <0.001 | (0.757, 0.775) |
| VPAV ← MPAV | 0.218 | 0.011 | 20.34 | <0.001 | (0.197, 0.239) |
| Model fitness | |||||
| Chi-square test of model fit (p value) | <0.001 | ||||
| CFI | 0.997 | ||||
| TLI | 0.992 | ||||
| SRMR | 0.011 | ||||
| RMSEA | 0.019 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isaura, E.R.; Chen, Y.-C.; Yang, S.-H. Pathways from Food Consumption Score to Cardiovascular Disease: A Seven-Year Follow-Up Study of Indonesian Adults. Int. J. Environ. Res. Public Health 2018, 15, 1567. https://doi.org/10.3390/ijerph15081567
Isaura ER, Chen Y-C, Yang S-H. Pathways from Food Consumption Score to Cardiovascular Disease: A Seven-Year Follow-Up Study of Indonesian Adults. International Journal of Environmental Research and Public Health. 2018; 15(8):1567. https://doi.org/10.3390/ijerph15081567
Chicago/Turabian StyleIsaura, Emyr Reisha, Yang-Ching Chen, and Shwu-Huey Yang. 2018. "Pathways from Food Consumption Score to Cardiovascular Disease: A Seven-Year Follow-Up Study of Indonesian Adults" International Journal of Environmental Research and Public Health 15, no. 8: 1567. https://doi.org/10.3390/ijerph15081567
APA StyleIsaura, E. R., Chen, Y.-C., & Yang, S.-H. (2018). Pathways from Food Consumption Score to Cardiovascular Disease: A Seven-Year Follow-Up Study of Indonesian Adults. International Journal of Environmental Research and Public Health, 15(8), 1567. https://doi.org/10.3390/ijerph15081567