Women’s Mid-Life Night Sweats and 2-Year Bone Mineral Density Changes: A Prospective, Observational Population-Based Investigation from the Canadian Multicentre Osteoporosis Study (CaMos)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Cross-Sectional Bone Mineral Density Values at Baseline and Two Years
3.3. Two-Year Bone Mineral Density Changes
3.4. Two-Year Incidence of Fragility Fractures
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| BMD | areal Bone Mineral Density |
| CaMos | Canadian Multicentre Osteoporosis Study |
| FN | Femoral neck |
| HR | Hazards ratio |
| Kg | kilograms |
| L1-4 or, if unknown segments, LS | Lumbar spine |
| OHT | ovarian hormone therapy |
| TH | Total hip |
| VMS | Vasomotor symptoms = hot flushes/flashes and night sweats |
| VMSn | Vasomotor symptoms occurring during sleep, Night sweats |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| First Author/Year | Number | Characteristics | BMD Site | Duration | Rate of Change in BMD (VMS vs. Controls) |
|---|---|---|---|---|---|
| Naessen, 1992 [7] | 40 | Swedish general population sample Age 51.3 ± 0.3 (SEM) year Sweating episodes/day by questionnaire | Distal radius | 24 mo | ~9% vs. 4%/year mean difference 4.3%/year, 95% CI (0.7–7.8), p = 0.023 |
| Salamone, 1998 [8] | 290 | USA—Women’s Healthy Lifestyle Project 47.2 ± 2.0 years Y/N to Interfering Hot flushes (yes in 14%) 40% had only night sweats—questionnaire | Lumbar Spine Total Hip | 30 mo. | −0.33 ± 1.1%/year vs. −0.26 ± 1.1%/year, p = 0.698 0.13 ± 0.9%/year vs. −0.11 ± 1.1%/year, p = 0.15 |
| Huang, 2007 [9] | 2418 | USA Raloxifene trial Analyzed treatment and placebo together VMS no/mild vs., mod./severe (n = 36) by questionnaire | Lumbar Spine | 36 mo. | −0.17%/year (−1.02, 0.68) vs. 0.36%/year (0.23, 0.48) p = 0.84 |
| Tuomikoski, 2014 [10] | 114 | Finland Menopausal, 71.3 ± 0.3 years VMS weekly score (per Sloan) | Lumbar Spine Left Total Hip Right Total Hip | 75 mo. | −0.3 ± 0.3% vs. −0.4 ± 0.3%/year −0.6 ± 0.2% vs. −0.7 ± 0.3%/year −0.8 ± 0.2% vs. −0.8 ± 0.2%/year (NS for all) |
References
- Hale, G.E.; Hitchcock, C.L.; Williams, L.A.; Vigna, Y.M.; Prior, J.C. Cyclicity of breast tenderness and night-time vasomotor symptoms in mid-life women: Information collected using the Daily Perimenopause Diary. Climacteric 2003, 6, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.E.; Kalilani, L.; DiBenedetti, D.B.; Zhou, X.; Granger, A.L.; Fehnel, S.E.; Levine, K.B.; Jordan, J.; Clark, R.V. Frequency and severity of vasomotor symptoms among peri- and postmenopausal women in the United States. Climacteric 2008, 11, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kanis, J.A. An association between osteoporosis and premenstrual symptoms and postmenopausal symptoms. Bone Miner. 1994, 24, 127–134. [Google Scholar] [CrossRef]
- Crandall, C.J.; Aragaki, A.; Cauley, J.A.; Manson, J.E.; LeBlanc, E.; Wallace, R.; Wactawski-Wende, J.; LaCroix, A.; O’sullivan, M.J.; Vitolins, M.; et al. Associations of menopausal vasomotor symptoms with fracture incidence. J. Clin. Endocrinol. Metab. 2015, 100, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Gast, G.C.; Grobbee, D.E.; Pop, V.J.; Keyzer, J.J.; Wijnands-van Gent, C.J.; Samsioe, G.N.; Nilsson, P.M.; van der Schouw, Y.T. Vasomotor symptoms are associated with a lower bone mineral density. Menopause 2009, 16, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Pal, L.; Norian, J.; Zeitlian, G.; Bevilacqua, K.; Freeman, R.; Santoro, N. Vasomotor symptoms in infertile premenopausal women: A hitherto unappreciated risk for low bone mineral density. Fertil. Steril. 2008, 90, 1626–1634. [Google Scholar] [CrossRef] [PubMed]
- Naessen, T.; Persson, I.; Ljunghall, S.; Bergstrom, R. Women with climacteric symptoms: A target group for prevention of rapid bone loss and osteoporosis. Osteoporos. Int. 1992, 2, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Salamone, L.M.; Gregg, E.; Wolf, R.L.; Epstein, R.S.; Black, D.; Palermo, L.; Kuller, L.H.; Cauley, J.A. Are menopausal symptoms associated with bone mineral density and changes in bone mineral density in premenopausal women? Maturitas 1998, 29, 179–187. [Google Scholar] [CrossRef]
- Huang, A.; Grady, D.; Blackwell, T.; Bauer, D. Hot flushes, bone mineral density, and fractures in older postmenopausal women. Obstet. Gynecol. 2007, 109, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Tuomikoski, P.; Ylikorkala, O.; Mikkola, T.S. Postmenopausal hot flushes and bone mineral density: A longitudinal study. Acta Obstet. Gynecol. Scand. 2015, 94, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Prior, J.C. Perimenopause: The complex endocrinology of the menopausal transition. Endocr. Rev. 1998, 19, 397–428. [Google Scholar] [CrossRef] [PubMed]
- Kreiger, N.; Tenenhouse, A.; Joseph, L.; Mackenzie, T.; Poliquin, S.; Brown, J.P.; Prior, J.C.; Rittmaster, R.S. The Canadian Multicentre Osteoporosis Study (CaMos): Background, rationale, methods. Can. J. Aging 1999, 18, 376–387. [Google Scholar] [CrossRef]
- Hitchcock, C.L.; Elliott, T.G.; Norman, E.G.; Stajic, V.; Teede, H.; Prior, J.C. Hot flushes and night sweats differ in associations with cardiovascular markers in healthy early postmenopausal women. Menopause 2012, 19, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- The North American Menopause Society. The 2012 Hormone Therapy Position Statement of The North American Menopause Society. Menopause 2012, 19, 257–271. [Google Scholar]
- Prior, J.C.; Seifert-Klauss, V.R.; Hale, G. The endocrinology of perimenopause—New definitions and understandings of hormonal and bone changes. In Current Topics in Menopause; Dvoryk, V., Ed.; Bentham Science Publishers Ltd.: Emirate of Sharjah, United Arab Emirates, 2012; pp. 54–83. [Google Scholar]
- Ward, K.D.; Klesges, R.C. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif. Tissue Int. 2001, 68, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Johnell, O.; Odén, A.; Johansson, H.; De Laet, C.; Eisman, J.A.; Fujiwara, S.; Kroger, H.; McCloskey, E.V.; Mellstrom, D.; et al. Smoking and fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Cochran, C.J.; Gallicchio, L.; Miller, S.R.; Zacur, H.; Flaws, J.A. Cigarette smoking, androgen levels, and hot flushes in midlife women. Obstet. Gynecol. 2008, 112, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Gold, E.B.; Sternfeld, B.; Kelsey, J.L.; Brown, C.; Mouton, C.; Reame, N.; Salamone, L.; Stellato, R. Relation of demographic and lifestyle factors to symptoms in a multi-racial/ethnic population of women 40–55 years of age. Am. J. Epidemiol. 2000, 152, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Kanis, J.A.; Odén, A.; McCloskey, E.; Chapurlat, R.D.; Christiansen, C.; Cummings, S.R.; Diez-Perez, A.; Eisman, J.A.; Fujiwara, S.; et al. A meta-analysis of the association of fracture risk and body mass index in women. J. Bone Miner. Res. 2014, 29, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Berger, C.; Goltzman, D.; Langsetmo, L.; Joseph, L.; Jackson, S.; Kreiger, N.; Tenenhouse, A.; Davison, K.S.; Josse, R.G.; Prior, J.C.; et al. Peak bone mass from longitudinal data: Implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J. Bone Miner. Res. 2010, 25, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Fuerst, T.; Hui, S.; Genant, H.K. Standardization of bone mineral density at femoral neck, trochanter and Ward’s triangle. Osteoporos. Int. 2001, 12, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.L.; Gao, S.; Zhou, X.H.; Johnston, C.C.; Lu, Y.; Glüer, C.C.; Grampp, S.; Genant, H. Universal standardization of bone density measurements: A method with optimal properties for calibration among several instruments. J. Bone Miner. Res. 1997, 12, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Prior, J.C.; Langsetmo, L.; Lentle, B.C.; Berger, C.; Goltzman, D.; Kovacs, C.S.; Kaiser, S.M.; Adachi, J.D.; Papaioannou, A.; Anastassiades, T.; et al. Ten-year incident osteoporosis-related fractures in the population-based Canadian Multicentre Osteoporosis Study—Comparing site and age-specific risks in women and men. Bone 2014, 71, 237–243. [Google Scholar] [CrossRef] [PubMed]
- MacLennan, A.H.; Broadbent, J.L.; Lester, S.; Moore, V. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Cochrane Database Syst. Rev. 2004, 7, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Tremollieres, F.A.; Pouilles, J.M.; Ribot, C. Withdrawal of hormone replacement therapy is associated with significant vertebral bone loss in postmenopausal women. Osteoporos. Int. 2001, 12, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Berger, C.; Langsetmo, L.; Joseph, L.; Hanley, D.A.; Davison, K.S.; Josse, R.; Kreiger, N.; Tenenhouse, A.; Goltzman, D. Change in bone mineral density as a function of age in women and men and association with the use of antiresorptive agents. Can. Med. Assoc. J. 2008, 178, 1660–1668. [Google Scholar] [CrossRef] [PubMed]
- Krall, E.A.; Dawson-Hughes, B. Smoking increases bone loss and decreases intestinal calcium absorption. J. Bone Miner. Res. 1999, 14, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Oncken, C.; Prestwood, K.; Kleppinger, A.; Wang, Y.; Raisz, K. Imparct of Smoking Cessation on Bone Mineral Density in Postmenopausal Women. J. Women’s Health 2006, 15, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Von Muhlen, D.G.; Soroko, S.; Kritz-Silverstein, D.; Barrett-Connor, E. Vasomotor symptoms are not associated with reduced bone mass in postmenopausal women: The Rancho Bernardo Study. J. Womens Health Gend. Based Med. 2000, 9, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Crandall, C.J.; Aragaki, A.K.; Chlebowski, R.T.; McTiernan, A.; Anderson, G.; Hendrix, S.L.; Cochrane, B.B.; Kuller, L.H.; Cauley, J.A. New-onset breast tenderness after initiation of estrogen plus progestin therapy and breast cancer risk. Arch. Intern. Med. 2009, 169, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Martinez Perez, J.A.; Palacios, S.; Chavida, F.; Perez, M. Severity of menopausal symptoms and cardiovascular and osteoporosis risk factors. Climacteric 2013, 16, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Özkaya, E.; Cakir, E.; Kara, F.; Okuyan, E.; Cakir, C.; Üstün, G.; Küçüközkan, T. Impact of hot flashes and night sweats on carotid intima-media thickness and bone mineral density among postmenopausal women. Int. J. Gynaecol. Obstet. 2011, 113, 235–238. [Google Scholar] [CrossRef] [PubMed]
| Characteristic | Absent/Mild VMSn | Clinically Important VMSn | * p-Value |
|---|---|---|---|
| N (%) | 1379 (87.8) | 191 (12.2) | |
| Age (years), mean (SD) | 55.3 (5.2) | 54.5 (4.6) | 0.020 |
| Weight (kg), mean (SD) | 71.2 (14.1) | 72.1 (15.6) | 0.457 |
| Height (cm), mean (SD) | 161.0 (6.1) | 160.9 (6.3) | 0.833 |
| Body mass index kg/m2, mean (SD) | 27.5 (5.2) | 27.8 (5.7) | 0.380 |
| Reproductive status, n (%) | 0.261 | ||
| Premenopause | 358 (26.0) | 51 (26.7) | |
| Natural menopause | 866 (62.8) | 126 (66.0) | |
| Surgical menopause | 155 (11.2) | 14 (7.3) | |
| Mean age at menopause years, mean (SD) | 46.1 (7.2) | 46.3 (7.9) | 0.773 |
| Sex steroid therapy, n (%) | 708 (51.4) | 76 (39.8) | 0.003 |
| Regular physical activity, n (%) | 706 (51.2) | 85 (44.5) | 0.098 |
| Smoking status, n (%) | |||
| Current | 174 (12.6) | 36 (18.8) | 0.047 |
| Past | 512 (37.2) | 71 (37.2) | |
| Family history of fracture, n (%) | 621 (45.0) | 77 (40.3) | 0.249 |
| Family history of osteoporosis, n (%) | 243 (17.6) | 40 (20.9) | 0.308 |
| Presence of Fragility fracture, n (%) | 36 (2.6) | 4 (2.1) | 0.810 |
| Baseline BMD (g/cm2), mean (SD *) | |||
| L1-4 | 0.996 (0.151) | 0.991 (0.147) | 0.676 |
| FN | 0.762 (0.111) | 0.763 (0.117) | 0.909 |
| TH | 0.918 (0.127) | 0.921 (0.129) | 0.797 |
| BMD (g/cm2) at Year 2 mean (SD *) | |||
| L1-4 | 0.995 (0.152) | 0.986 (0.150) | 0.452 |
| FN | 0.754 (0.111) | 0.752 (0.114) | 0.771 |
| TH | 0.911 (0.128) | 0.911 (0.130) | 0.976 |
| Baseline Variables | 2-Year Percent Change in BMD (95% CI) | |
|---|---|---|
| In Model | Model 1 | Model 2 |
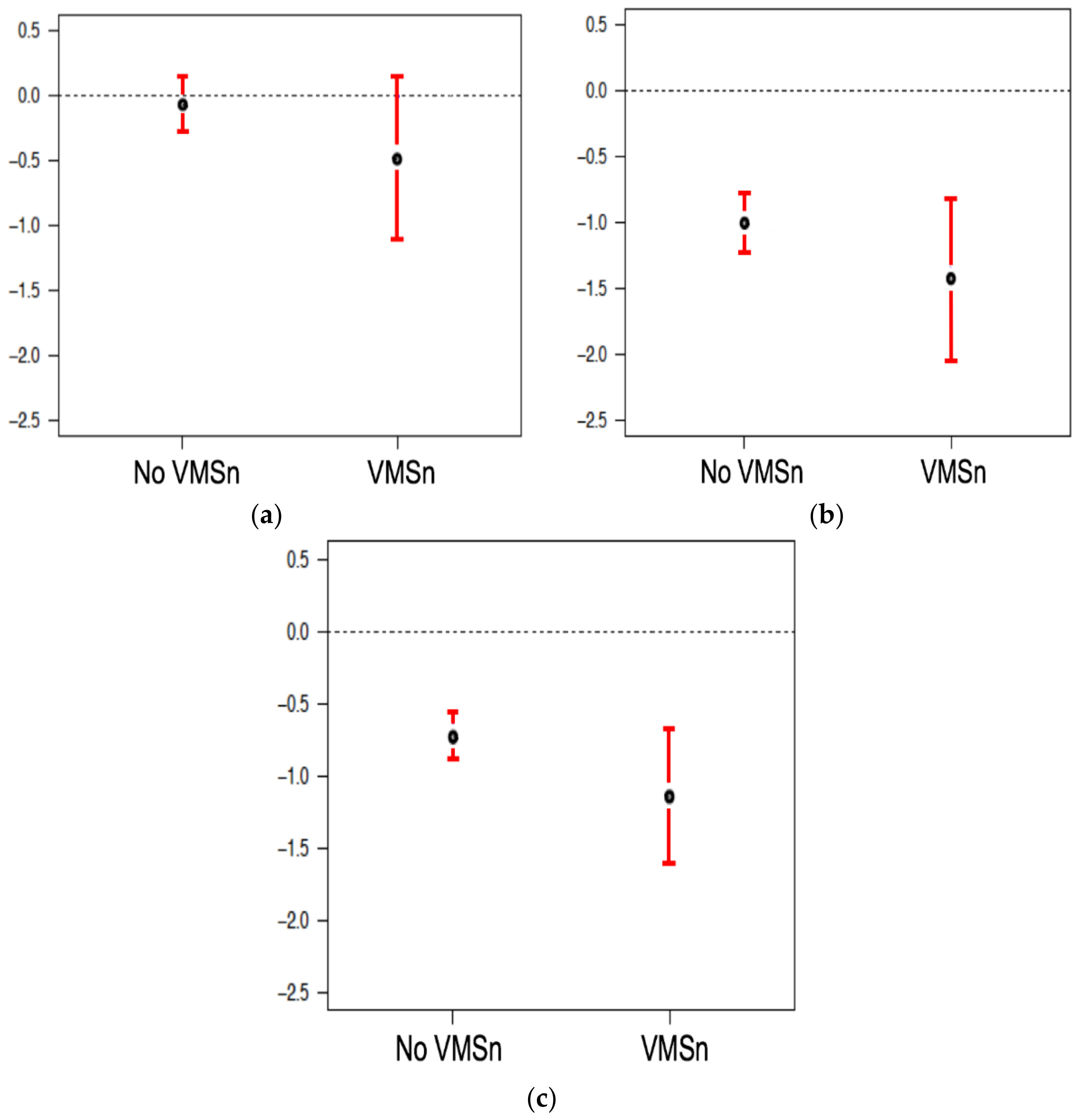
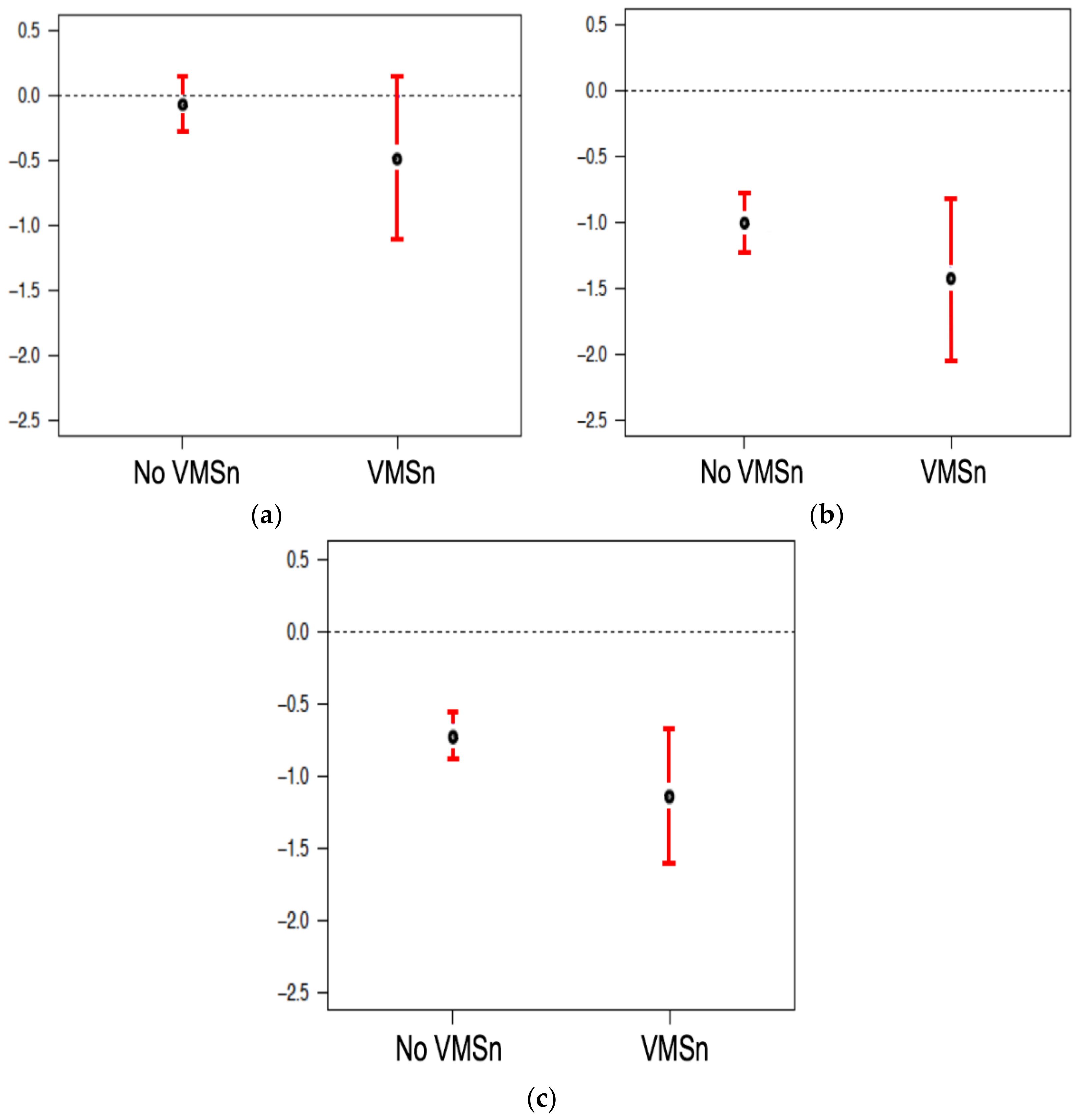
| Clinically important VMSn (vs. No or Mild VMSn) | −0.138 (−0.770, 0.493), p = 0.669 | −0.309 (−0.942, 0.324), p = 0.339 |
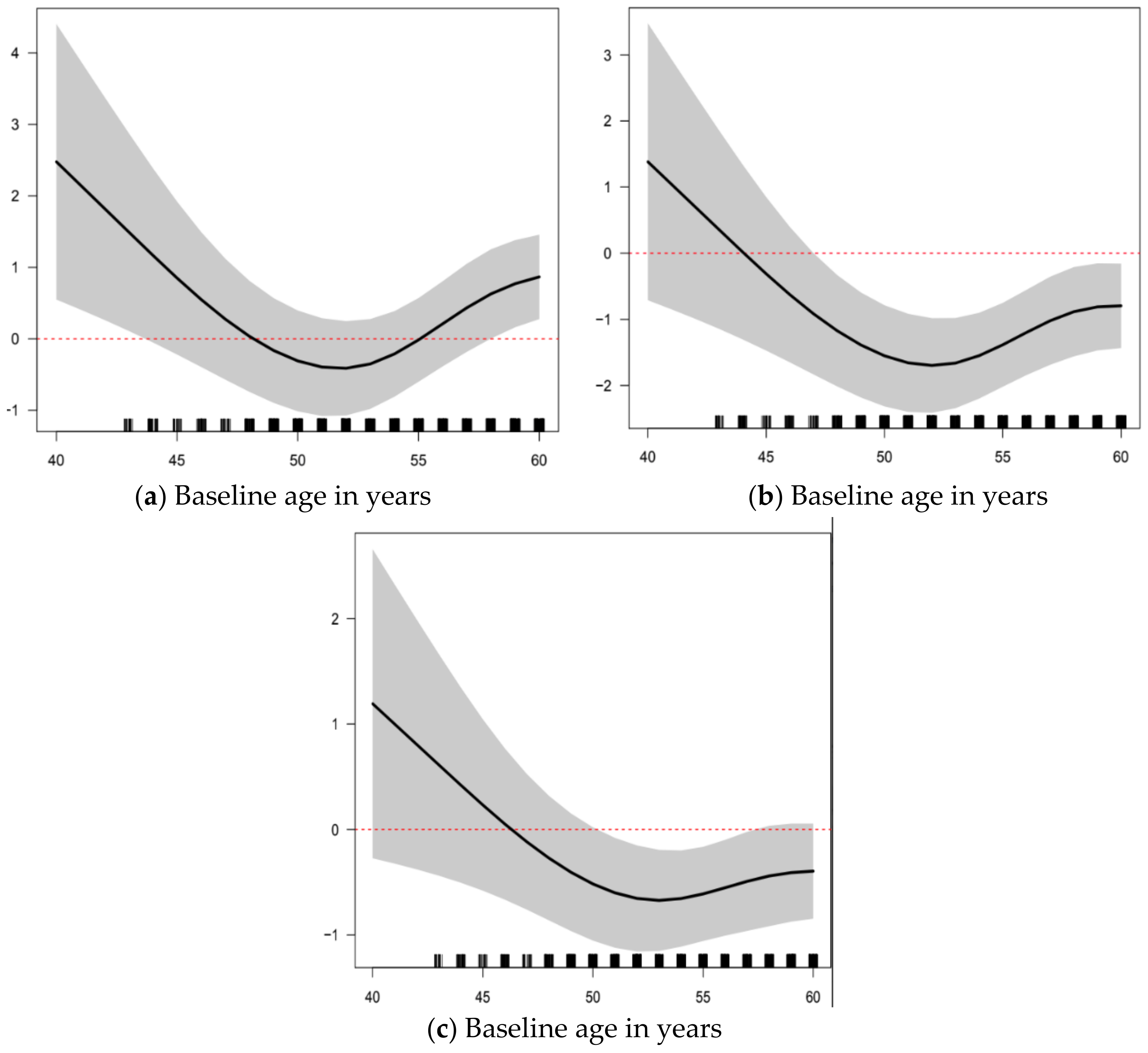
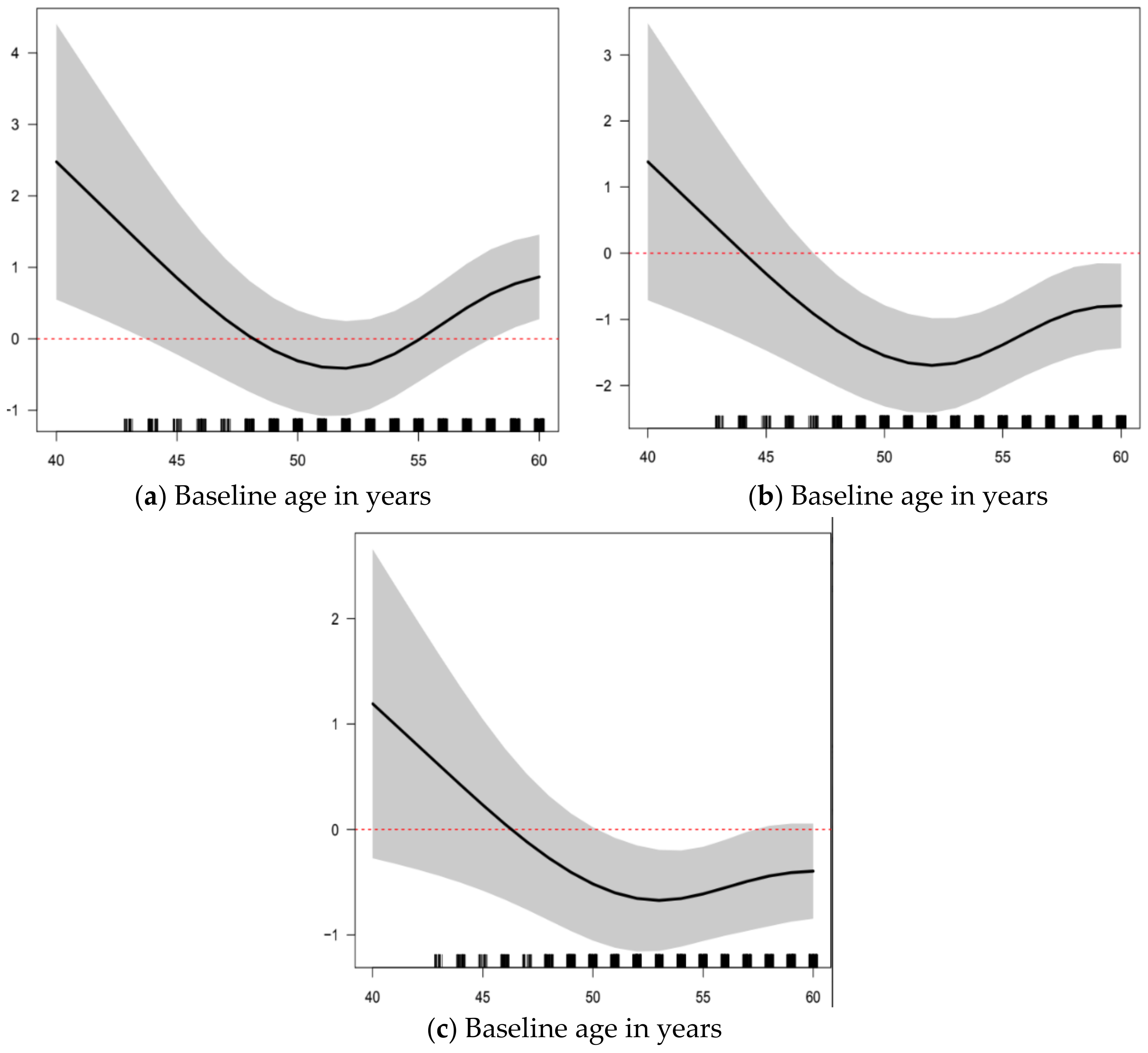
| Age (years) | (Figure 2a) | NA |
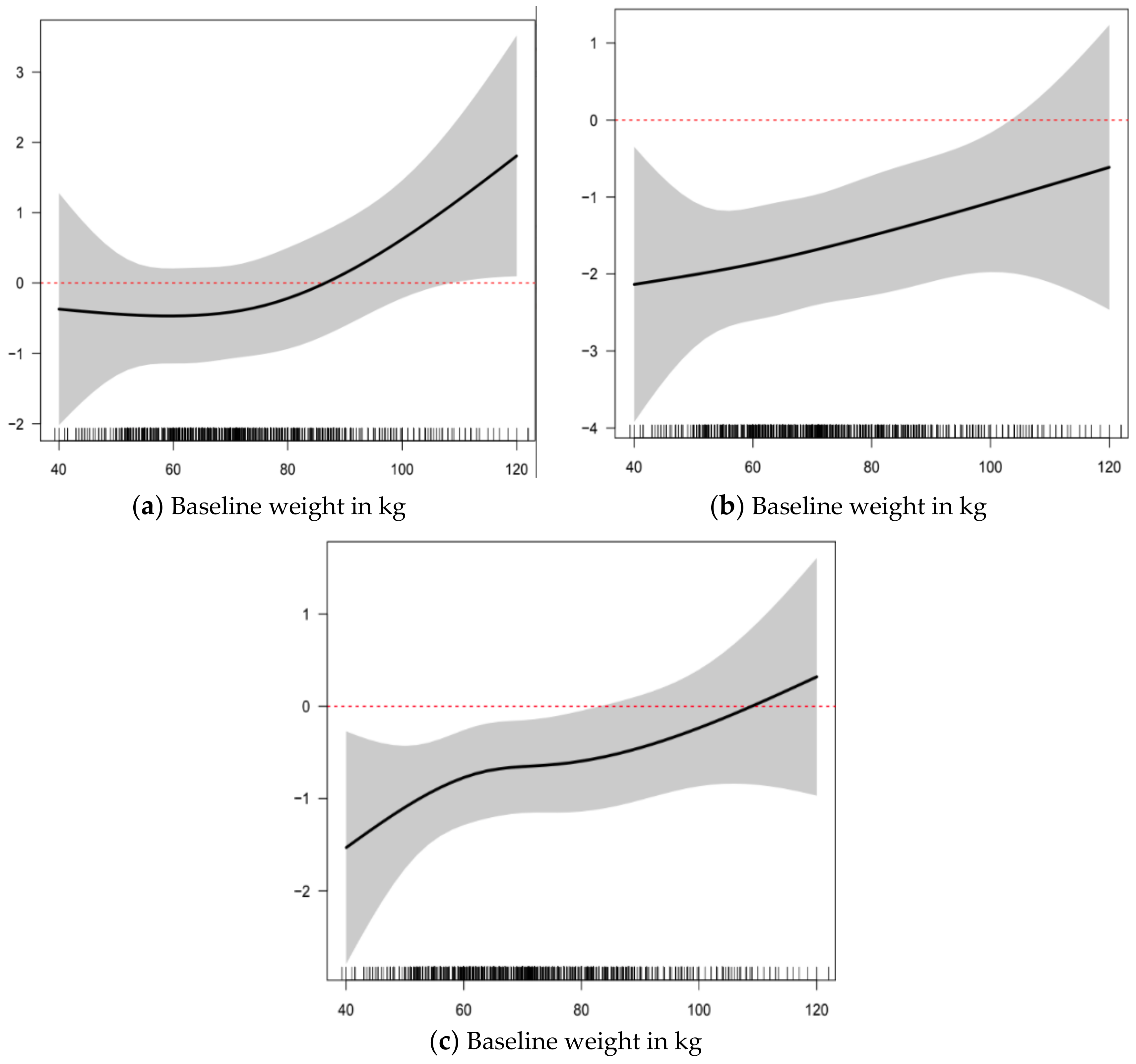
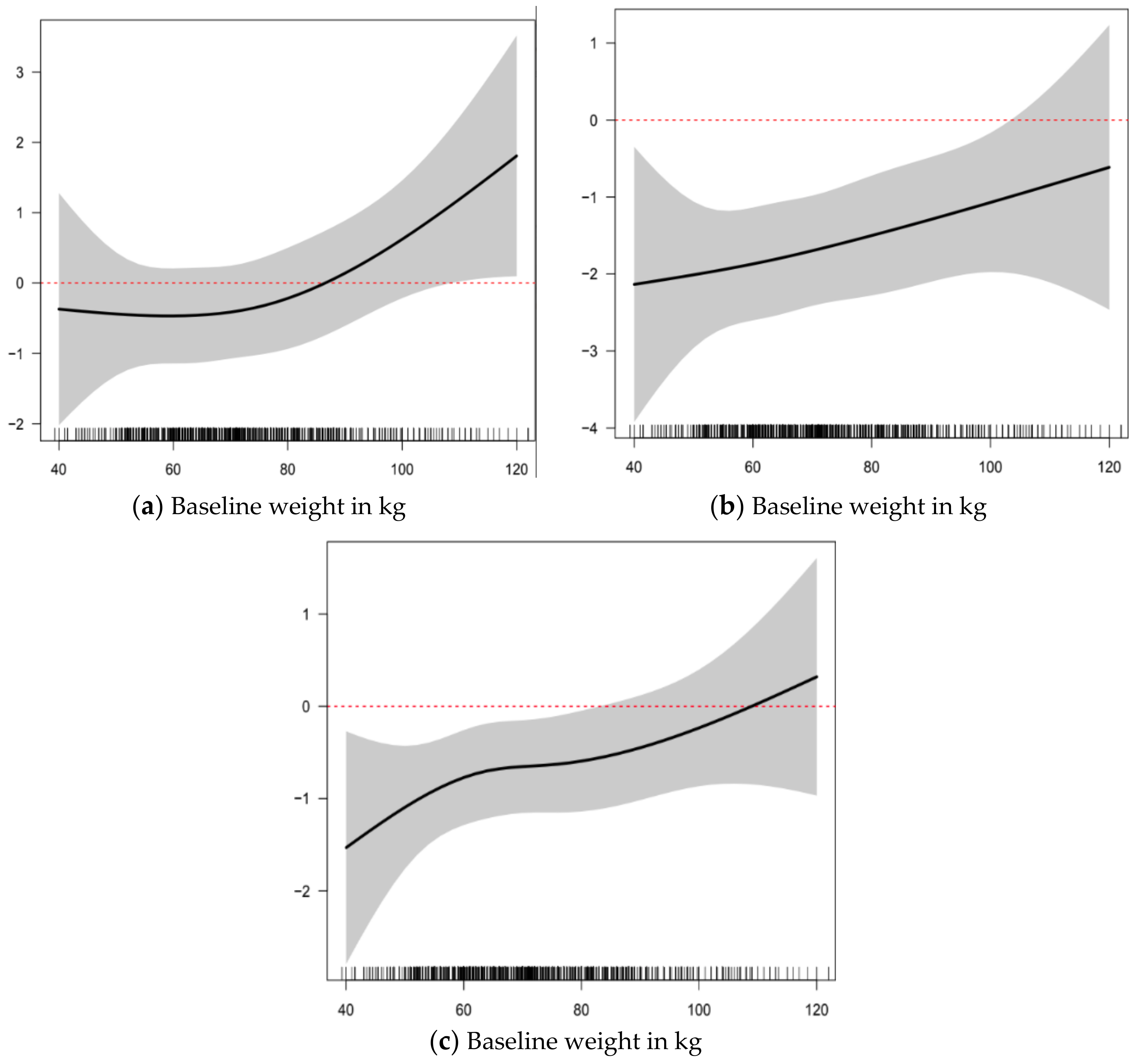
| Weight (kg) | (Figure 3a) | (Figure 3a) |
| Reproductive Status (vs. Premenopausal) | ||
| Naturally Menopausal | NA | 1.117 (0.612, 1.622), p < 0.01 |
| Surgically Menopausal | NA | 0.933 (0.128, 1.738), p = 0.024 |
| Regular physical activity (vs. None) | −0.352 (−0.776, 0.072), p = 0.105 | −0.320 (−0.746, 0.105), p = 0.141 |
| Family history of fracture (vs. None) | 0.030 (−0.391, 0.450), p = 0.891 | 0.039 (0.384, 0.463), p = 0.856 |
| Sex steroid therapy (vs. Never) | 0.491 (0.048, 0.933), p = 0.030 | 0.330 (−0.121, 0.780), p = 0.152 |
| Smoking status (vs. Never) | ||
| Current | 0.106 (−0.545, 0.756), p = 0.751 | −0.031 (−0.685, 0.623), p = 0.928 |
| Past | 0.567 (0.109, 1.024), p = 0.016 | 0.553 (0.094, 1.011), p = 0.019 |
| Overall R2 | 0.046 | 0.035 |
| Adjusted R2 | 0.038 | 0.027 |
| Residual standard error | 3.959 (df = 1376) | 3.982 (df = 1377) |
| F statistic | 5.552 * (df = 12; 1376) | 4.493 (df = 11; 1377) |
| Baseline Variables | 2-Year Percent Change in BMD (95% CI) | |
|---|---|---|
| In Model | Model 1 | Model 2 |
| Clinically Important VMSn | −0.208 (−0.889, 0.473), p = 0.550 | −0.289 (−0.970, 0.391), p = 0.406 |
| Age (years) | (Figure 2b) | NA |
| Weight (kg) | (Figure 3b) | (Figure 3b) |
| Reproductive Status | ||
| Naturally Menopausal | NA | −0.012 (−0.554, 0.531), p = 0.967 |
| Surgically Menopausal | NA | 0.657 (−0.207, 1.521), p = 0.137 |
| Regular activity | 0.053 (−0.404, 0.510), p = 0.822 | 0.069 (−0.388, 0.527), p = 0.767 |
| Family history of fracture | 0.091 (−0.381, 0.606), p = 0.655 | 0.117 (−0.376, 0.609), p = 0.643 |
| Sex steroid therapy | 0.146 (−0.331, 0.623), p = 0.550 | 0.004 (−0.480, 0.488), p = 0.988 |
| Smoking status | ||
| Current | −0.371 (−1.070, 0.329), p = 0.300 | −0.405 (−1.107, 0.297), p = 0.259 |
| Past | 0.113 (−0.381, 0.606), p = 0.655 | 0.117 (−0.376, 0.609), p = 0.643 |
| Overall R2 | 0.016 | 0.009 |
| Adjusted R2 | 0.008 | 0.001 |
| Residual standard error | 4.273 (df = 1379) | 4.270 (df = 1369) |
| F statistic | 1.906 ** (df = 12; 1368) | 1.173 (df = 11; 1369) |
| Baseline Variables | 2-year Percent Change in BMD (95% CI) | |
|---|---|---|
| In Model | Model 1 | Model 2 |
| Clinically important VMSn | −0.393 (−0.873, 0.088), p = 0.110 | −0.440 (−0.920, 0.041), p = 0.074 |
| Age (years) | (Figure 2c) | NA |
| Weight (kg) | (Figure 3c) | (Figure 3c) |
| Reproductive Status | ||
| Naturally Menopausal | NA− | −0.188 (−0.569, 0.193), p = 0.334 |
| Surgically Menopausal | NA− | −0.337 (−0.942, 0.267), p = 0.275 |
| Regular activity | −0.137 (−0.459, 0.185), p = 0.405 | −0.151 (−0.472, 0.171), p = 0.359 |
| Family history of fracture | 0.009 (−0.310, 0.328), p = 0.956 | 0.009 (−0.311, 0.329), p = 0.958 |
| Sex steroid therapy | 0.322 (−0.014, 0.657), p = 0.061 | 0.286 (−0.054, 0.625), p = 0.100 |
| Smoking status | ||
| Current | −0.197 (−0.690, 0.296), p = 0.435 | −0.189 (−0.682, 0.305), p = 0.455 |
| Past | 0.052 (−0.295, 0.398), p = 0.770 | 0.060 (−0.286, 0.405), p = 0.736 |
| Overall R2 | 0.016 | 0.011 |
| Adjusted R2 | 0.007 | 0.003 |
| Residual standard error | 2.965 (df = 1342) | 2.971 (df = 1343) |
| F statistic | 1.809 ** (df = 12; 1342) | 1.416 (df = 11; 1343) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, E.M.M.; Tomlinson, G.; Pinto, M.M.; Berger, C.; Cheung, A.M.; Prior, J.C. Women’s Mid-Life Night Sweats and 2-Year Bone Mineral Density Changes: A Prospective, Observational Population-Based Investigation from the Canadian Multicentre Osteoporosis Study (CaMos). Int. J. Environ. Res. Public Health 2018, 15, 1079. https://doi.org/10.3390/ijerph15061079
Wong EMM, Tomlinson G, Pinto MM, Berger C, Cheung AM, Prior JC. Women’s Mid-Life Night Sweats and 2-Year Bone Mineral Density Changes: A Prospective, Observational Population-Based Investigation from the Canadian Multicentre Osteoporosis Study (CaMos). International Journal of Environmental Research and Public Health. 2018; 15(6):1079. https://doi.org/10.3390/ijerph15061079
Chicago/Turabian StyleWong, Evelyn M. M., George Tomlinson, Marsha M. Pinto, Claudie Berger, Angela M. Cheung, and Jerilynn C. Prior. 2018. "Women’s Mid-Life Night Sweats and 2-Year Bone Mineral Density Changes: A Prospective, Observational Population-Based Investigation from the Canadian Multicentre Osteoporosis Study (CaMos)" International Journal of Environmental Research and Public Health 15, no. 6: 1079. https://doi.org/10.3390/ijerph15061079
APA StyleWong, E. M. M., Tomlinson, G., Pinto, M. M., Berger, C., Cheung, A. M., & Prior, J. C. (2018). Women’s Mid-Life Night Sweats and 2-Year Bone Mineral Density Changes: A Prospective, Observational Population-Based Investigation from the Canadian Multicentre Osteoporosis Study (CaMos). International Journal of Environmental Research and Public Health, 15(6), 1079. https://doi.org/10.3390/ijerph15061079