Examining the Impact of Maternal Individual Features on Children’s Behavioral Problems in Adoptive Families: The Role of Maternal Temperament and Neurobiological Markers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
3. Results
3.1. Are Mothers’ Basic Temperament Traits Associated with Childrens’ Emotional and Behavioral Problems?
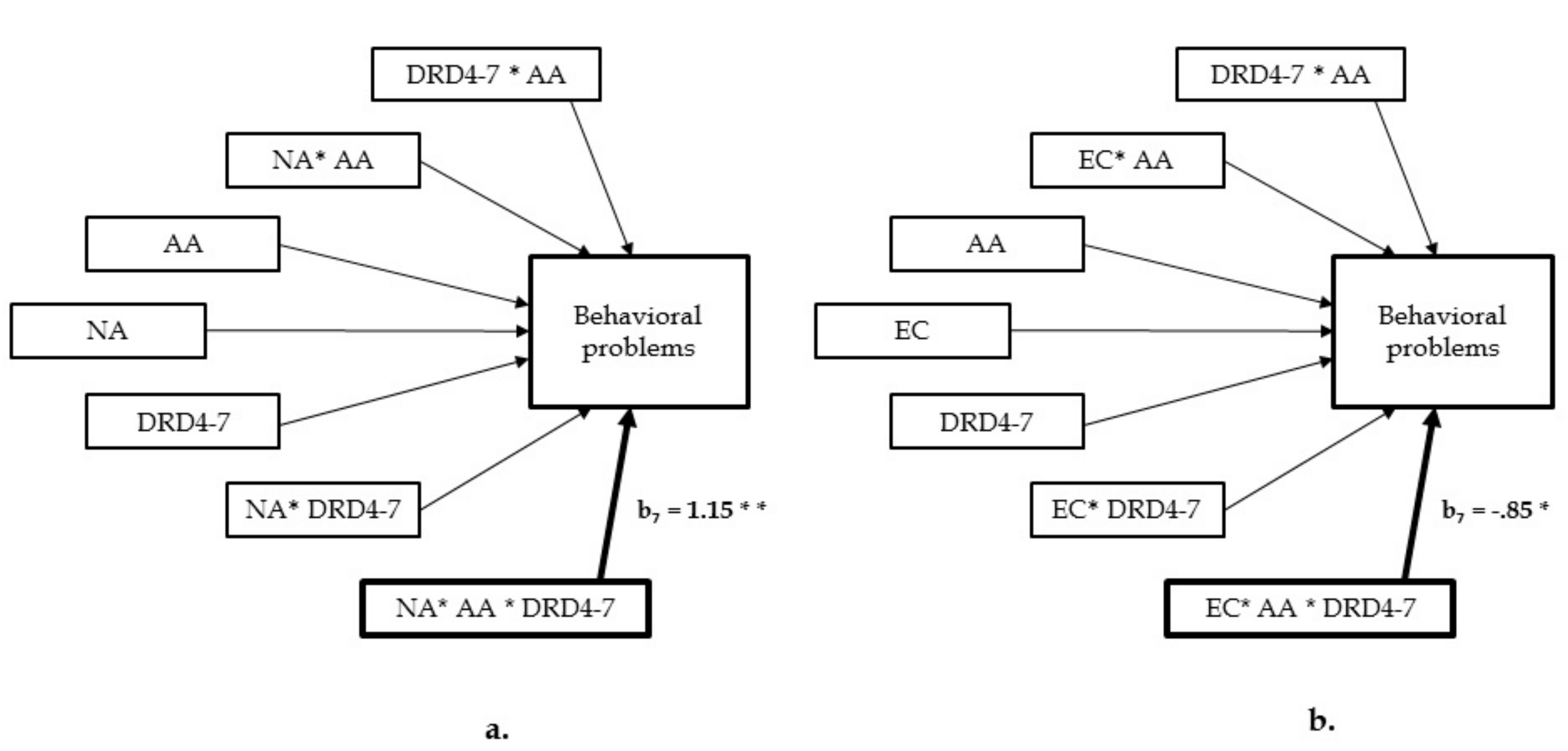
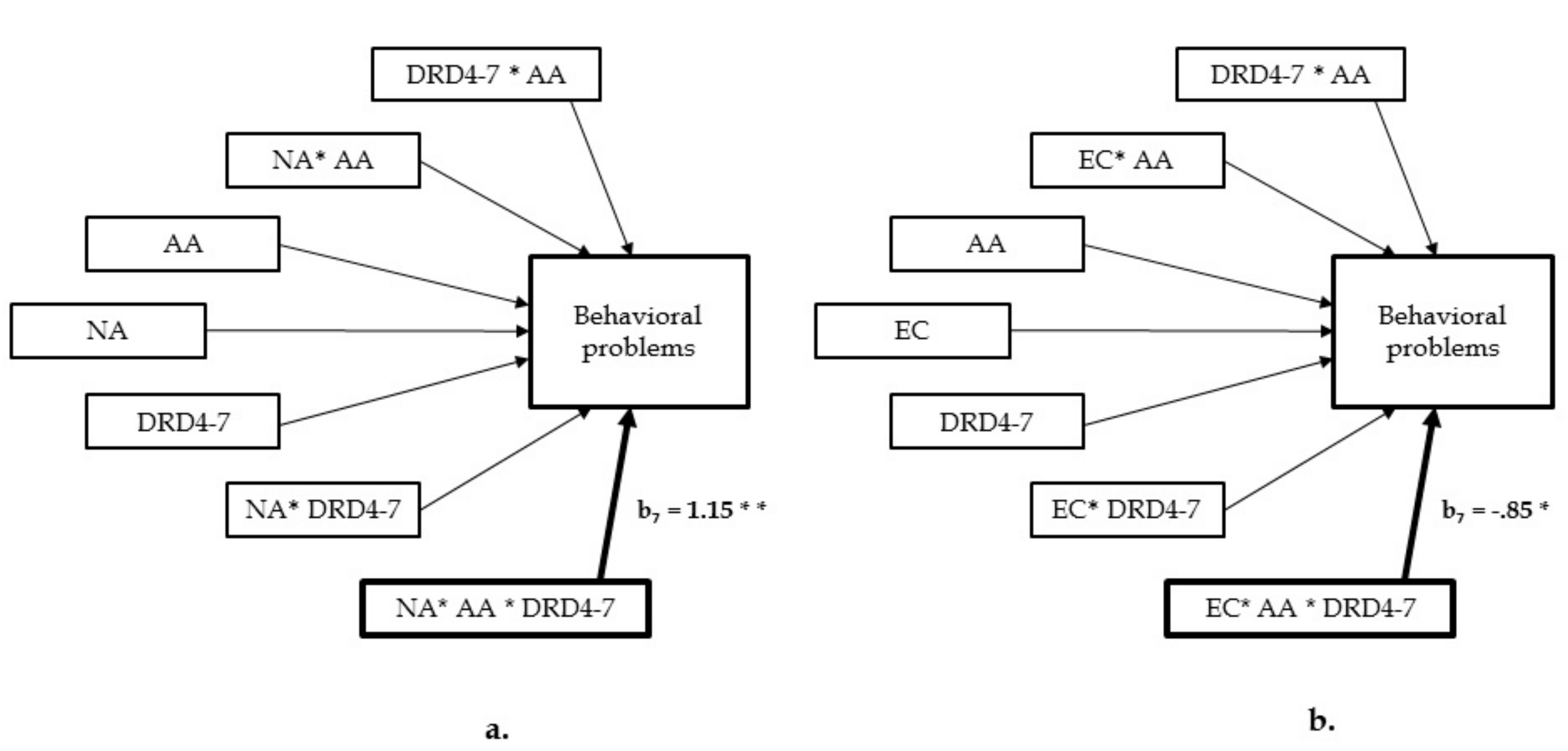
3.2. Do Maternal Genetic Markers and Children’s Age at Adoption Count in This Relationship?
3.3. Do Temperament Features of Children Count in This Relationship?
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Muhamedrahimov, R.J.; Grigorenko, E.L. Seeing the trees within the forest: Addressing the needs of children without parental care in the Russian Federation. New Dir. Child Adolesc. Dev. 2015, 147, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Van IJzendoorn, M.H.; Juffer, F.; Poelhuis, C.W.K. Adoption and cognitive development: A meta-analytic comparison of adopted and nonadopted children’s IQ and school performance. Psychol. Bull. 2005, 131, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Van der Vegt, E.J.M.; van der Ende, J.; Ferdinand, R.F.; Verhulst, F.C.; Tiemeier, H. Early childhood adversities and trajectories of psychiatric problems in adoptees: Evidence for long lasting effects. J. Abnorm. Child. Psychol. 2009, 37, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Maclean, K. The impact of institutionalization on child development. Dev. Psychopathol. 2003, 15, 853–884. [Google Scholar] [CrossRef] [PubMed]
- Gunnar, M.R. Effects of early deprivation: Findings from orphanage-reared infants and children. In Handbook of Developmental Cognitive Neuroscience; Nelson, C.A., Luciana, M., Eds.; MIT Press: Cambridge, MA, USA, 2001; pp. 617–629. [Google Scholar]
- Juffer, F.; Van IJzendoorn, M.H. Behavior problems and mental health referrals of international adoptees: A meta-analysis. JAMA 2005, 293, 2501–2515. [Google Scholar] [CrossRef] [PubMed]
- Hawk, B.; McCall, R.B. CBCL behavior problems of post-institutionalized international adoptees. Clin. Child. Fam. Psychol. Rev. 2010, 13, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Barone, L.; Lionetti, F.; Green, J. A matter of attachment? How adoptive parents foster post-institutionalized children’s social and emotional adjustment. Attach. Hum. Dev. 2017, 19, 323–339. [Google Scholar] [CrossRef] [PubMed]
- Shaw, D.S.; Taraban, L.E. New directions and challenges in preventing conduct problems in early childhood. Child Dev. Perspect. 2017, 11, 85–89. [Google Scholar] [CrossRef]
- Groh, A.M.; Fearon, R.P.; Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H.; Steele, R.D.; Roisman, G.I. The significance of attachment security for children’s social competence with peers: A meta-analytic study. Attach. Hum. Dev. 2014, 16, 103–136. [Google Scholar] [CrossRef] [PubMed]
- Barros, L.; Goes, A.R.; Pereira, A.I. Parental self-regulation, emotional regulation and temperament: Implications for intervention. Estud. Psicol. 2015, 32, 295–306. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Bates, M.K. Temperament. In Handbook of Child Psychology: Social, Emotional, and Personality Development, 6th ed.; Damon, W., Lerner, R., Eisenberg, N., Eds.; Wiley: New York, NA, USA, 2006; Volume 3, pp. 99–106. [Google Scholar]
- Belsky, J.; Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. For better and for worse: Differential susceptibility to environmental influences. Curr. Dir. Psychol. Sci. 2007, 16, 300–304. [Google Scholar] [CrossRef]
- Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. The hidden efficacy of interventions: Gene×environment experiments from a differential susceptibility perspective. Annu. Rev. Psychol. 2015, 66, 381–409. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.; Pluess, M. Beyond diathesis stress: Differential susceptibility to environmental influences. Psychol. Bull. 2009, 135, 885–908. [Google Scholar] [CrossRef] [PubMed]
- Van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Mesman, J. Dopamine system genes associated with parenting in the context of daily hassles. Genes Brain Behav. 2008, 7, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Puri, B.; Hall, A.; Ho, R.C. Revision Notes in Psychiatry, 3rd ed.; CRC Press: New York, NA, USA, 2014; p. 631. [Google Scholar]
- Mak, K.K.; Kong, W.Y.; Mak, A.; Sharma, V.K.; Ho, R.C. Polymorphisms of the serotonin transporter gene and post-stroke depression: A meta-analysis. J. Neurol. Neurosurg. Psychiatry 2013, 84, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Van den Dries, L.; Juffer, F.; van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J. Fostering security? A meta-analysis of attachment in adopted children. Child. Youth Serv. Rev. 2009, 31, 410–421. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms & Profiles; University of Vermont, Research Center for Children, Youth and Families: Burlington, VT, USA, 2000. [Google Scholar]
- Frigerio, A. Questionario Sul Comportamento del Bambino; Associazione la Nostra Famiglia: Lecco, Italy, 2001. (In Italian) [Google Scholar]
- Evans, D.E.; Rothbart, M.K. Developing a model for adult temperament. J. Res. Personal. 2007, 41, 868–888. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Ahadi, S.A.; Hershey, S.A.; Fisher, P. Investigations of temperament at three to seven years: The Children’s Behavior Questionnaire. Child Dev. 2001, 72, 1394–1408. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. Available online: http://imaging. mrc-cbu. cam. ac. uk/statswiki/FAQ/SobelTest (accessed on 5 November 2017).
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NA, USA, 2013. [Google Scholar]
- Mileva-Seitz, V.R.; Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. Genetic mechanisms of parenting. Horm. Behav. 2015, 77, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, B.E.; Bost, K.K. Attachment and temperament as intersecting developmental products and interacting. In Handbook of Attachment: Theory, Research, and Clinical Applications, 3rd ed.; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 202–222. [Google Scholar]
- Duncan, K.M.; MacGillivray, S.; Renfrew, M.J. Costs and savings of parenting interventions: Results of a systematic review. Child Care Health Dev. 2017, 43, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Barker, B.; Iles, J.E.; Ramchandani, P.G. Fathers, fathering and child psychopathology. Curr. Opin. Psychol. 2017, 15, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Sethna, V.; Murray, L.; Netsi, E.; Psychogiou, L.; Ramchandani, L. Paternal depression in the postnatal period and early father-infant interactions. Parent. Sci. Pract. 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Quek, Y.H.; Tam, W.W.; Zhang, M.W.; Ho, R. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Poston, W.S.C.; Ericsson, M.; Linder, J.; Haddock, C.K.; Hanis, C.L.; Nilsson, T.; Åström, M.; Foreyt, J.P. D4 dopamine receptor gene exon III polymorphism and obesity risk. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 1998, 3, 71–77. [Google Scholar] [CrossRef]
- Zeanah, C.H.; Gunnar, M.R.; McCall, R.B.; Kreppner, R.B.; Fox, N.A. Sensitive periods. Monogr. Soc. Res. Child. Dev. 2011, 76, 147. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| % | Mean (SD) | Range | |
|---|---|---|---|
| Age at assessment (months) | 43 (16.1) | 14–75 | |
| Age at adoption (months) | 33 (17.1) | 1–68 | |
| Gender | Male: 58 | ||
| Mothers’ age (years) | 42.7 (3.8) | 34–51 | |
| SES 1 | 31.1 (6.9) | 16.5–48.5 | |
| Length | 11.2 (3.7) | 3–20 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Child Total Problems | - | 0.26 * | −0.25 * | 0.22 * | 0.54 *** | −0.33 ** |
| 2. Mother Temperament-NA | - | −0.45 *** | 0.28 ** | 0.25 i | −0.10 | |
| 3. Mother Temperament-EC | - | 0.04 | −0.16 | −0.17 | ||
| 4. Age at Adoption | - | 0.23 | 0.06 | |||
| 5. Child Temperament-NA 1 | - | 0.01 | ||||
| 6. Child Temperament-EC 1 | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozturk, Y.; Barone, V.; Barone, L. Examining the Impact of Maternal Individual Features on Children’s Behavioral Problems in Adoptive Families: The Role of Maternal Temperament and Neurobiological Markers. Int. J. Environ. Res. Public Health 2018, 15, 196. https://doi.org/10.3390/ijerph15020196
Ozturk Y, Barone V, Barone L. Examining the Impact of Maternal Individual Features on Children’s Behavioral Problems in Adoptive Families: The Role of Maternal Temperament and Neurobiological Markers. International Journal of Environmental Research and Public Health. 2018; 15(2):196. https://doi.org/10.3390/ijerph15020196
Chicago/Turabian StyleOzturk, Yagmur, Virginia Barone, and Lavinia Barone. 2018. "Examining the Impact of Maternal Individual Features on Children’s Behavioral Problems in Adoptive Families: The Role of Maternal Temperament and Neurobiological Markers" International Journal of Environmental Research and Public Health 15, no. 2: 196. https://doi.org/10.3390/ijerph15020196
APA StyleOzturk, Y., Barone, V., & Barone, L. (2018). Examining the Impact of Maternal Individual Features on Children’s Behavioral Problems in Adoptive Families: The Role of Maternal Temperament and Neurobiological Markers. International Journal of Environmental Research and Public Health, 15(2), 196. https://doi.org/10.3390/ijerph15020196