Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Survey Tools
2.3. Data Management and Analysis
3. Results
3.1. Study Population
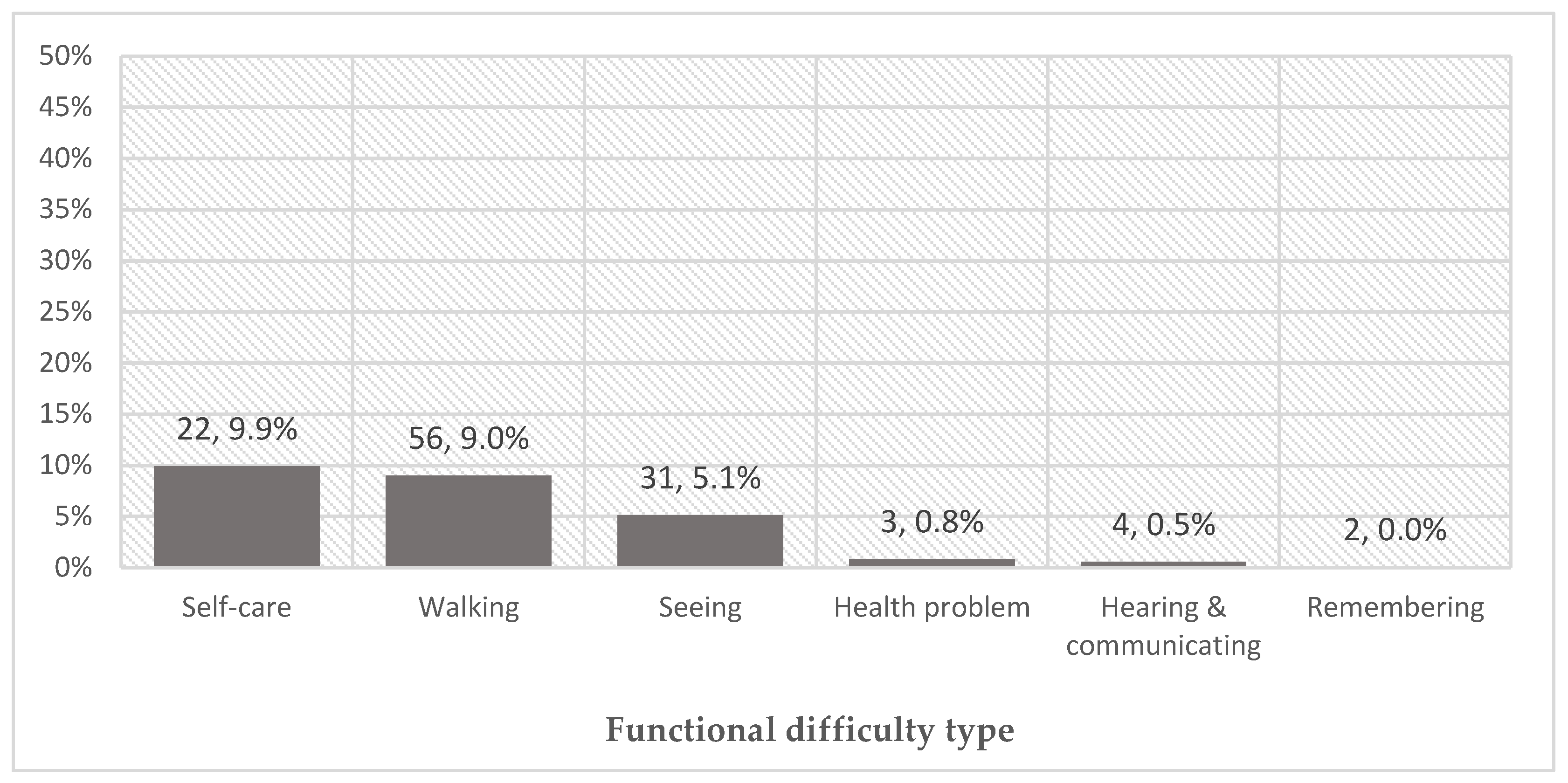
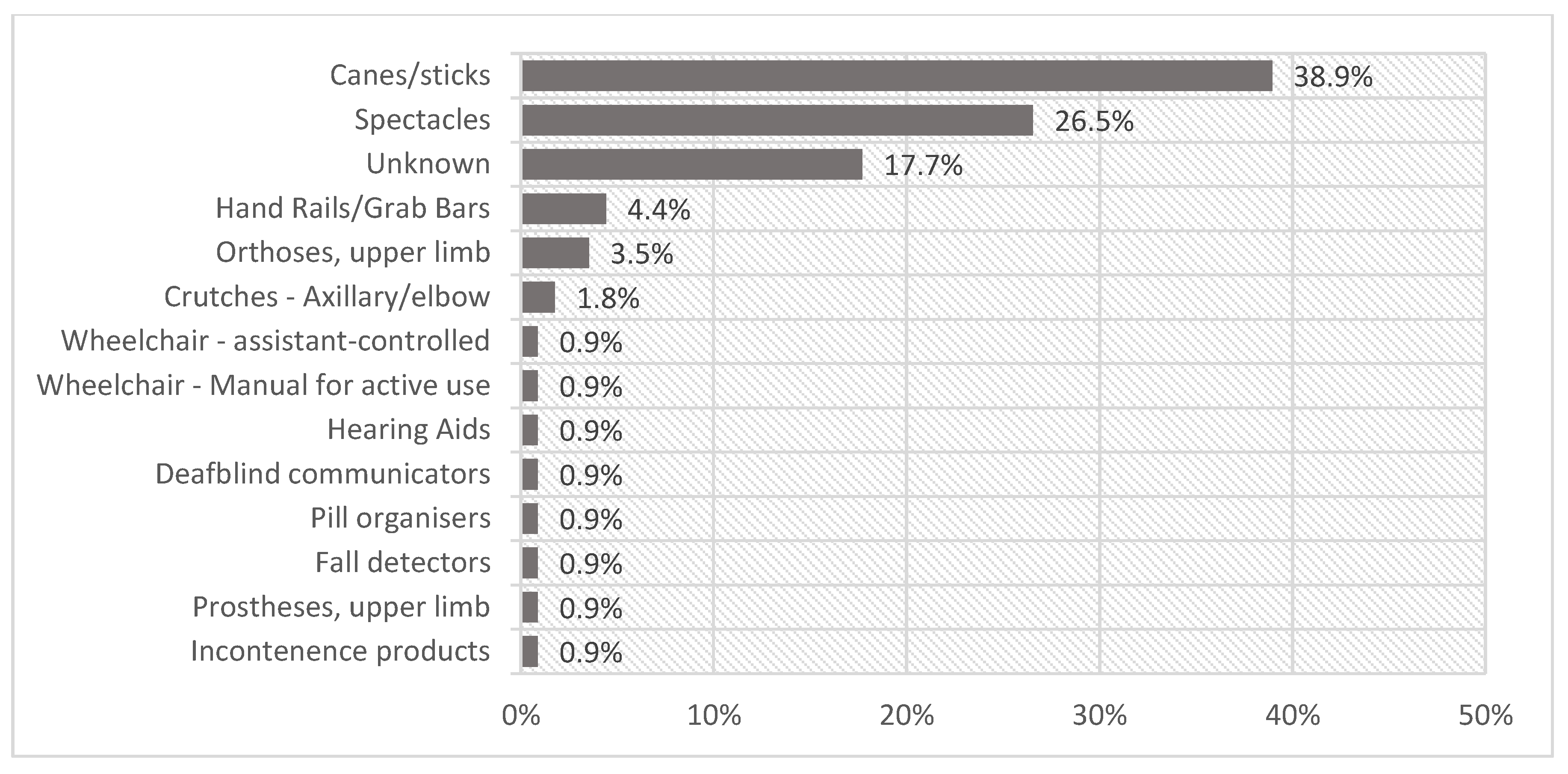
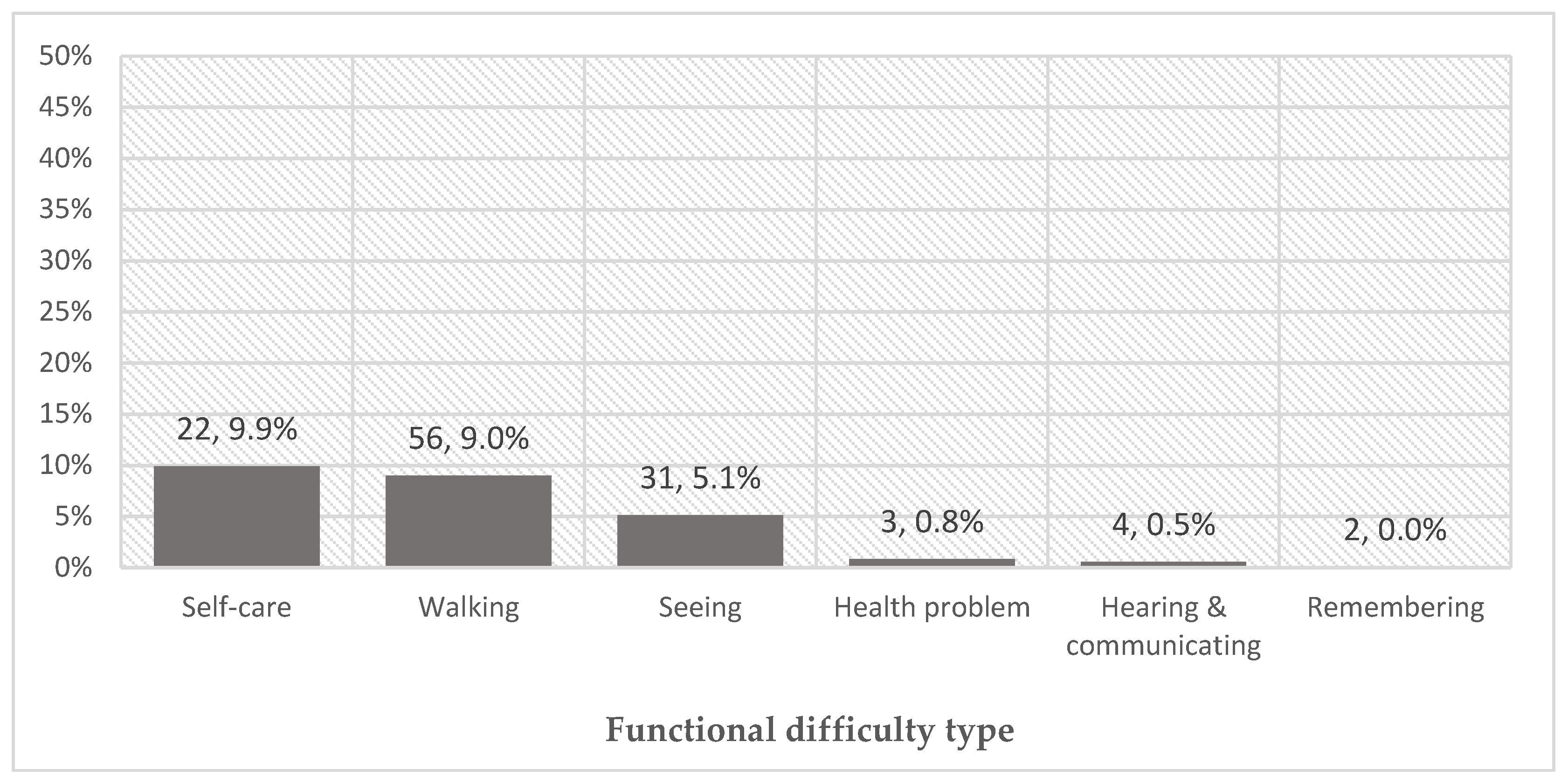
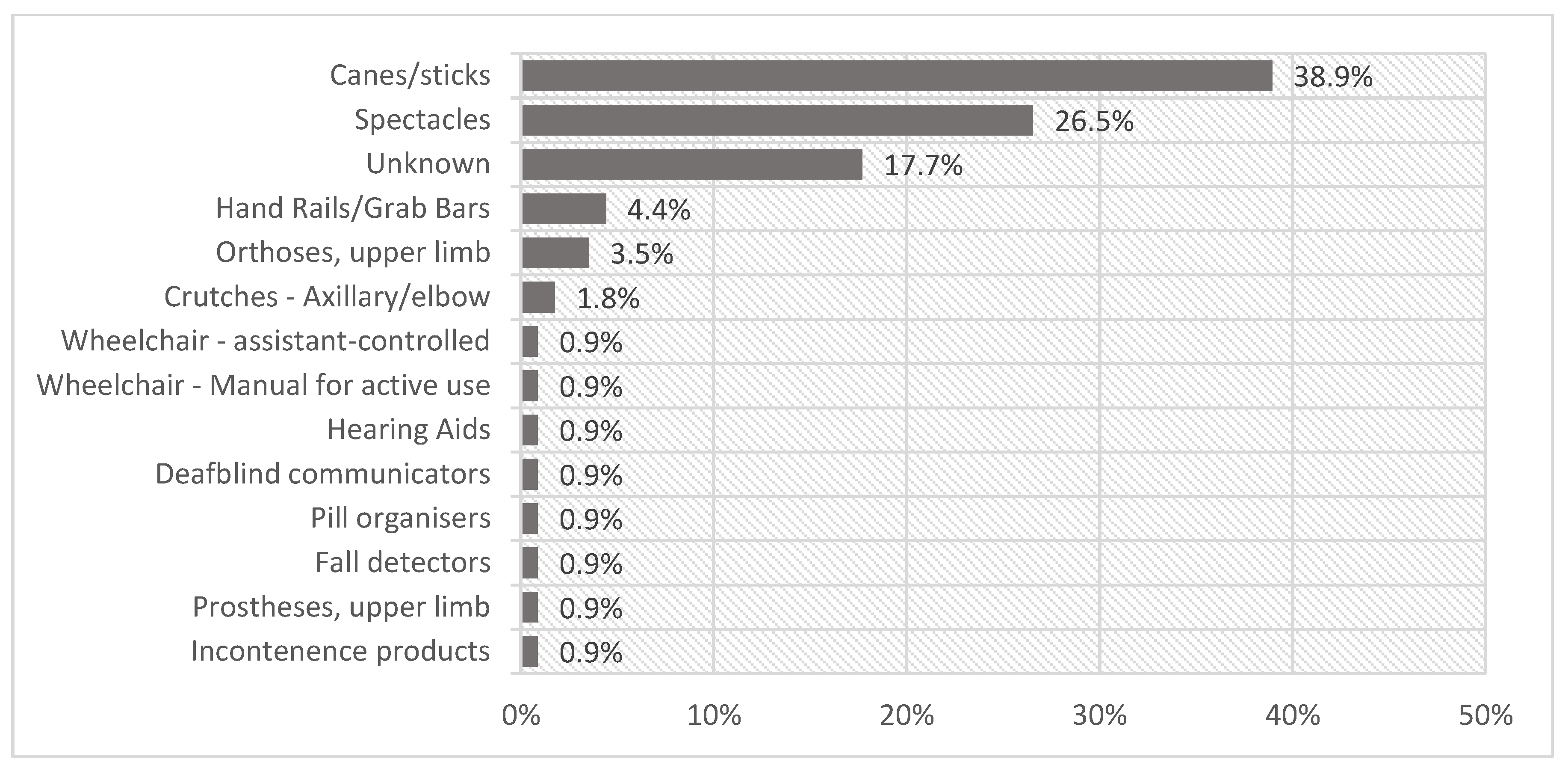
3.2. The Use of Assistive Products
3.3. Unmet Needs
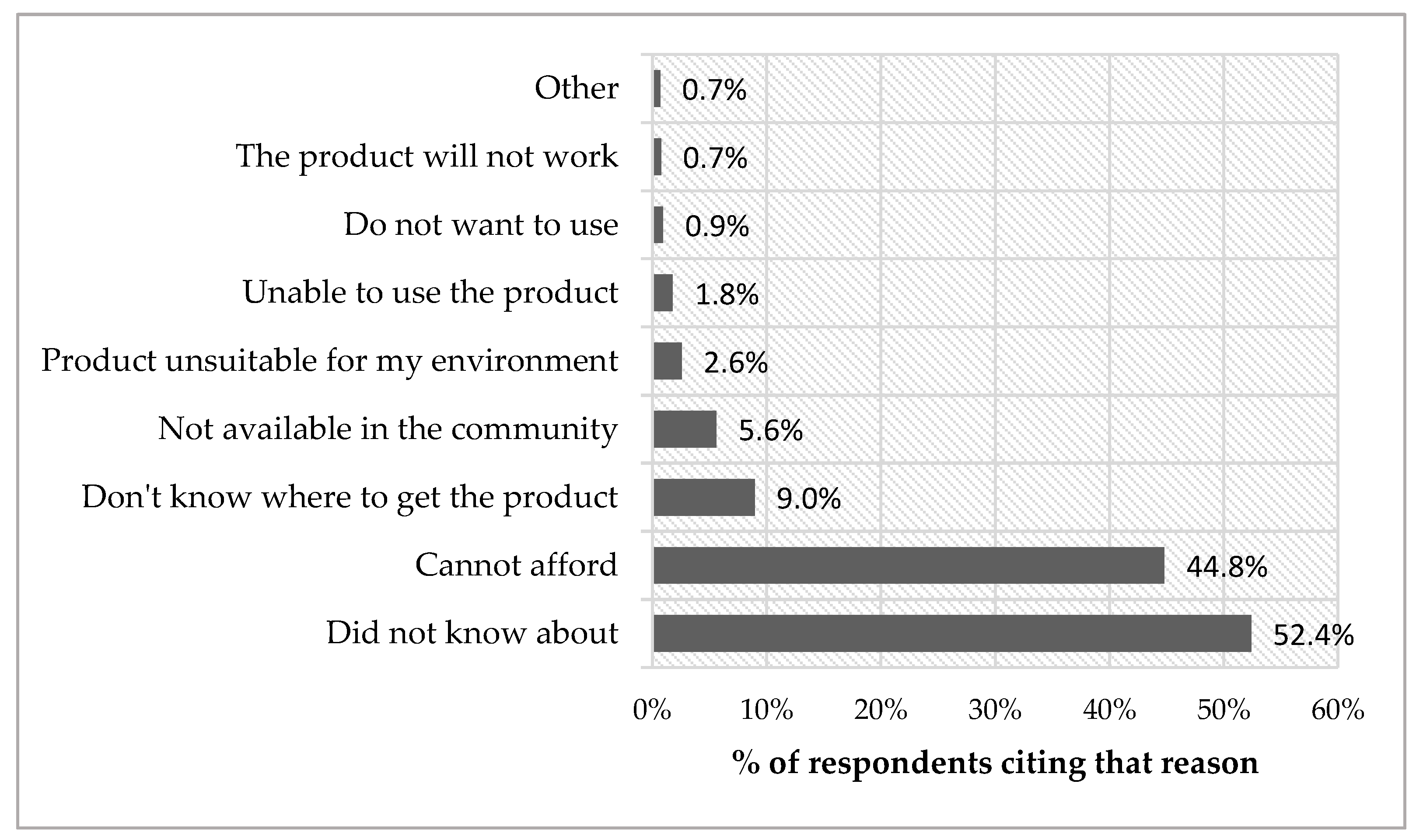
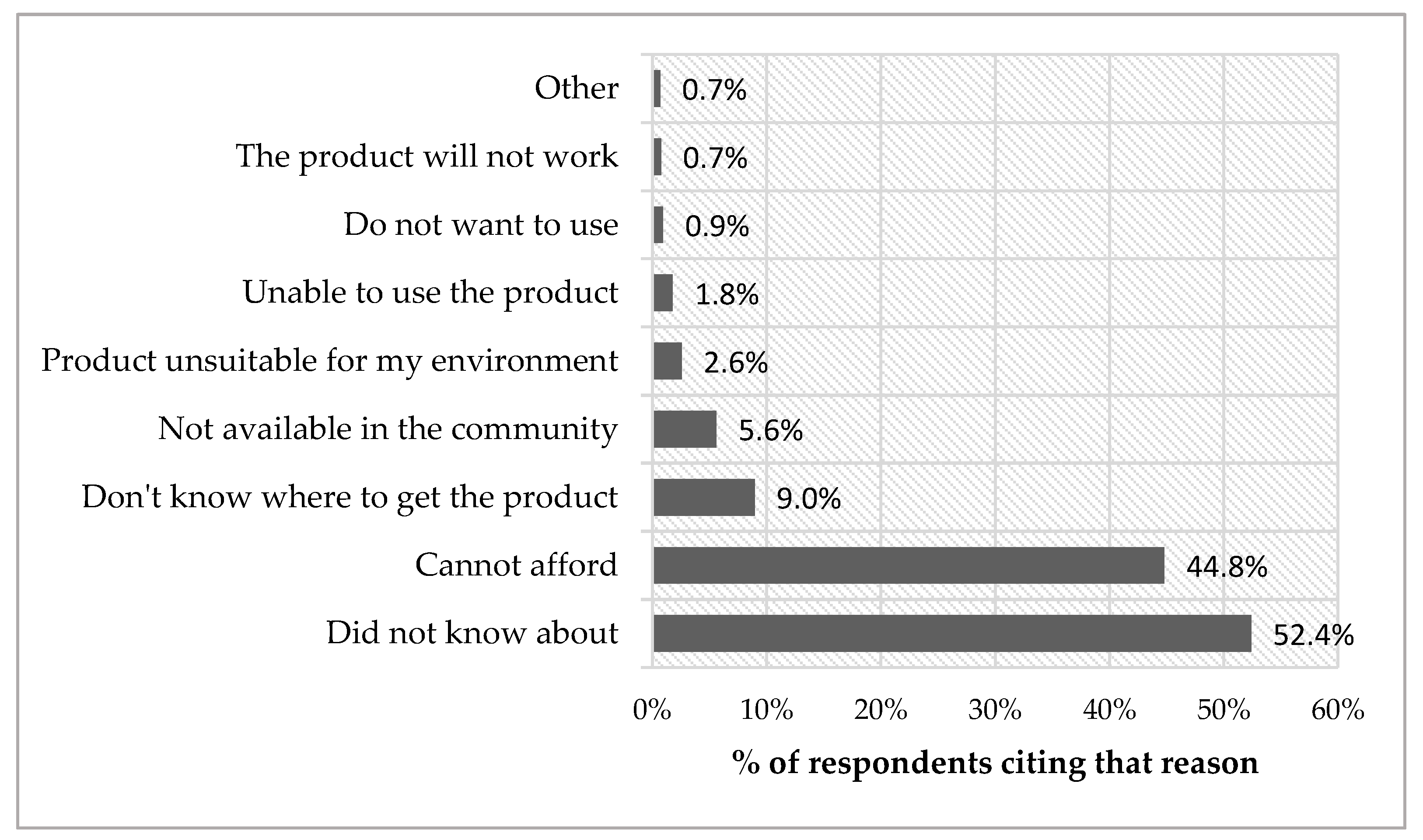
3.4. Market Conditions: Facilitators and Barriers for Using AP
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Level | Section | Questions | Skip Pattern | |
|---|---|---|---|---|
| LEVEL 1—(short version) Need and unmet need | A—Personal details | 1–10 | Sociodemographic characteristics | |
| B—Met and unmet need | ||||
| WG-extended set (example here for walking or climbing steps) | 11 | In the last 6 months, have you had difficulties WALKING or CLIMBING STEPS?0—no difficulty; 1—some difficulty; 2—a lot of difficulty; 3—cannot do at all | If “0”, go to next function Q; If“2–4”, go to Q12 | |
| 12 | Do you use any assistive products to: support you in standing, sitting or lyingor move around inside or outside the house or manage other mobility difficulties | If YES, go to Q13; If NO, go to Q15 | ||
| 13 | Which ones do you use? | Go to Q14 | ||
| 14 | Do you need any other products to assist you in these activities? For example: [show corresponding card/s] | If YES, go to Q16; If NO, go to Q17 | ||
| 15 | Do you think you might benefit from any assistive products to assist you in these activities? For example: [show corresponding card/s] | If YES, go to Q16; If NO, go to Q17 | ||
| 16 | Which ones do you need? | Go to Q17 | ||
| LEVEL 2—(Full version)—Product procurement, performance, use, services, impact; abandonment, barriers | C—AP in use (Repeat for all products reported as used in section B) | |||
| Procurement | 48 | Where did you get the [name of product/s from section B]? | ||
| 49 | Approximately how much did you pay for [the product]? | |||
| 50 | How far did you have to travel to get [the product]? | |||
| 51 | How long have you been using the assistive product? | |||
| 52 | If the device was lost or broken, are you confident you could easily replace it? | |||
| 53 | When you first got [the product] was it new or had it already been used (second-hand)? | |||
| Performance | 54 | Does [the product] meet your needs? (does it do everything that you want it to do?) | ||
| 55 | In what condition is [the product]? | |||
| 56 | What kind of problems have you had with the assistive product? | |||
| 57 | In which way do you think [the product] could be better? (what, if anything would you like to change about it?) | |||
| Use | 58 | In the typical day, how many hours do you use [the product]? | ||
| 59 | How easy is it for you to use [the product] within your home? | |||
| 60 | How easy is it for you to use [the product] outside home? | |||
| 61 | Do you need any assistance to set up [the product] before using it? | |||
| 62 | After set-up, do you need any assistance to use [the product]? | |||
| Services | 63 | Was [the product] prescribed for you following an assessment (i.e. looking at you/asking you questions/taking measures)? If yes, by whom? | ||
| 64 | Was [the product] fitted to you or customized to your needs? If yes, by whom? | |||
| 65 | Have you received any training on how to use and take care of [the product]? If yes, from whom? | |||
| 66 | If there is something wrong with [the product] is there somewhere you can go for repairs or maintenance? | |||
| Impact | 67 | How important is [the product] for you to do your work or go to school? | ||
| 68 | How important is [the product] for you to participate in social events and be an active member of your community? | |||
| 69 | How important is [the product] to your health? | |||
| 70 | How important is [the product] to your enjoyment or life? | |||
| Section D—Abandonment & Barriers | ||||
| Abandonment | 71 | Have you used an assistive product like [the product] in the past? | YES→ Q72; NO→Q76 | |
| 72 | Do you have an assistive product like [the product] that you no longer use? | YES→ Q73; NO→Q76 | ||
| 73 | How long have you had [product no longer in use]? | |||
| 74 | Is [product no longer in use] in working condition? | YES→Q75; NO→Q76 | ||
| 75 | Why are you no longer using [product no longer in use]? | |||
| Barriers | 76 | You told me that you do not use assistive products that could help you. What stops you from using them? | ||
References
- Tebbutt, E.; Brodmann, R.; Borg, J.; MacLachlan, M.; Khasnabis, C.; Horvath, R. Assistive products and the sustainable development goals (SDGs). Glob. Health 2016, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Borg, J.; Larsson, S.; Ostergren, P.O.; Rahman, A.A.; Bari, N.; Khan, A.N. Assistive technology use and human rights enjoyment: A cross-sectional study in bangladesh. BMC Int. Health Hum. Rights 2012, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Borg, J.; Ostergren, P.O.; Larsson, S.; Rahman, A.A.; Bari, N.; Khan, A.N. Assistive technology use is associated with reduced capability poverty: A cross-sectional study in bangladesh. Disabil. Rehabil. Assist. Technol. 2012, 7, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Priority Assistive Products List (APL). Available online: http://www.who.int/phi/implementation /assistive_technology/global_survey-apl/en/ (accessed on 10 December 2018).
- Improving Access to Assistive Technology. EB142.R6. Available online: http://apps.who.int/gb/ebwha/ pdf_files/EB142/B142_R6-en.pdf (accessed on 14 December 2018).
- Borg, J.; Ostergren, P.O. Users‘ perspectives on the provision of assistive technologies in bangladesh: Awareness, providers, costs and barriers. Disabil. Rehabil. Assist. Technol. 2015, 10, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Matter, R.; Harniss, M.; Oderud, T.; Borg, J.; Eide, A.H. Assistive technology in resource-limited environments: A scoping review. Disabil. Rehabil. Assist. Technol. 2017, 12, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Borg, J.; Lindstrom, A.; Larsson, S. Assistive technology in developing countries: A review from the perspective of the convention on the rights of persons with disabilities. Prosthet. Orthot. Int. 2011, 35, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Rohwerder, B. Assistive technologies in developing countries. In K4d Helpdesk Report; Institute of Development Studies: Brighton, UK, 2018; p. 22. [Google Scholar]
- Bangladesh Bureau of Statistics. Household Income and Expenditure Survey (HIES), 2010; Bangladesh Bureau of Statistics—Ministry of Planning: Dhaka, Bangladesh, 2011. [Google Scholar]
- Madans, J.H.; Loeb, M.E.; Altman, B.M. Measuring disability and monitoring the un convention on the rights of persons with disabilities: The work of the washington group on disability statistics. BMC Public Health 2011, 11 Suppl 4, S4. [Google Scholar] [CrossRef]
- Marella, M.; Huq, N.L.; Devine, A.; Baker, S.M.; Quaiyum, M.A.; Keeffe, J.E. Prevalence and correlates of disability in bogra district of bangladesh using the rapid assessment of disability survey. BMC Public Health 2015, 15, 867. [Google Scholar] [CrossRef] [PubMed]
- Marella, M.; Devine, A.; Armencin, G.A.; Zayas, J.; Ma Jesusa, M.; Vaghan, C. Rapid Assessment of Disability in The Philippines (Submitted for Publication); Nossal Institute for Global Health: Melbourne, Victoria, Australia, 2016. [Google Scholar]
- Marella, M.; Daveta, M.; Sprunt, B.; Hoq, M.M. Access to Quality Education Program (AQEP)—Fiji: Rapid Assessment of Disability Baseline in the Access to Quality Education Program; Nossal Institute for Global Health: Melbourne, Victoria, Australia, 2015. [Google Scholar]
- Marella, M.; Busija, L.; Islam, F.M.; Devine, A.; Fotis, K.; Baker, S.M.; Sprunt, B.; Edmonds, T.J.; Huq, N.L.; Cama, A.; et al. Field-testing of the rapid assessment of disability questionnaire. BMC Public Health 2014, 14, 900. [Google Scholar] [CrossRef] [PubMed]
- Samant, D.; Matter, R.; Harniss, M. Realizing the potential of accessible icts in developing countries. Disabil. Rehabil. Assist. Technol. 2013, 8, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Rios, A.; Miguel Cruz, A.; Guarin, M.R.; Caycedo Villarraga, P.S. What factors are associated with the provision of assistive technologies: The bogota d.C. Case. Disabil. Rehabil. Assist. Technol. 2014, 9, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Okonji, P.E.; Ogwezzy, D.C. Awareness and barriers to adoption of assistive technologies among visually impaired people in nigeria. Assist. Technol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Mactaggart, I.; Kuper, H.; Murthy, G.V.; Sagar, J.; Oye, J.; Polack, S. Assessing health and rehabilitation needs of people with disabilities in Cameroon and India. Disabil. Rehabil. 2016, 38, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Cornman, J.C.; Freedman, V.A.; Agree, E.M. Measurement of assistive device use: Implications for estimates of device use and disability in late life. Gerontologist 2005, 45, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Hamid, L.N.; Kobusingye, O.; Baine, S.O.; Mayora, C.; Bentley, J.A. Disability characteristics of community-based rehabilitation participants in kayunga district, uganda. Ann. Glob. Health 2017, 83, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.; Pattni, S.; Greenberg, M.; Miller, A.; Hocker, E.; Ritter, S.; Mehta, K. Access to prosthetic devices in developing countries: Pathways and challenges. In Proceedings of the IEEE 2015 Global Humanitarian Technology Conference, Seattle, WA, USA, 8–11 October 2015; p. 7. [Google Scholar]
- Mactaggart, I.; Kuper, H.; Murthy, G.V.; Oye, J.; Polack, S. Measuring disability in population based surveys: The interrelationship between clinical impairments and reported functional limitations in cameroon and india. PLoS ONE 2016, 11, e0164470. [Google Scholar] [CrossRef] [PubMed]
- Development of Disability Measures for Surveys: The Extended Set on Functioning. Available online: http://www.washingtongroup-disability.com/wp-content/uploads/2016/01/ Development_of_Disability_Measures_for_Surveys_The_Extended_Set_on_Functioning.pdf (accessed on 20 December 2018).
| Characteristics | AP Users | AP Non-Users | All (User + Non-User) | ||||
|---|---|---|---|---|---|---|---|
| Difficulty | No Difficulty | All AP Users | Difficulty | No Difficulty | All AP Non-Users | ||
| Level of difficulties | |||||||
| None | 44.6% | 70.9% | 69.0% | ||||
| Some | 37.6% | 26.2% | 27.1% | ||||
| A lot | 11.1% | 2.1% | 2.7% | ||||
| Cannot do | 6.7% | 0.8% | 1.2% | ||||
| Age | |||||||
| Mean 95% CI | 58.1 (55.2–61.0) | 41.1 (38.4–43.9) | 50.5 (48.1–53.0) | 46.2 (45.2–47.3) | 33.1 (32.5–33.7) | 36.9 (36.4–37.5) | 37.9 (37.3–38.5) |
| Sex | |||||||
| Female | 61.3% | 60.3% | 60.9% | 64.2% | 56.8% | 59.0% | 59.1% |
| Male | 38.7% | 39.7% | 39.1% | 35.8% | 43.2% | 41.0% | 40.9% |
| School attendance | |||||||
| Never attended | 43.4% | 11.3% | 29.1% | 57.6% | 26.8% | 35.7% | 35.3% |
| Ever attended | 56.6% | 88.7% | 70.9% | 42.4% | 73.2% | 64.3% | 64.7% |
| Working status | |||||||
| Not working | 80.6% | 66.4% | 74.3% | 69.0% | 64.2% | 65.6% | 66.2% |
| Working | 19.4% | 33.6% | 25.7% | 31.0% | 35.8% | 34.4% | 33.8% |
| District | |||||||
| Kurigram | 46.0% | 34.7% | 40.9% | 61.1% | 48.0% | 51.8% | 51.0% |
| Narsingdi | 54.0% | 65.3% | 59.1% | 38.9% | 52.0% | 48.2% | 49.0% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| N | 97,629 | 78,710 | 176,339 | 671,903 | 1,635,387 | 2,307,290 | 2,483,629 |
| n | 189 | 144 | 333 | 1167 | 2753 | 3920 | 4253 |
| Characteristics | Odds Ratio | 95% CI | |
|---|---|---|---|
| Level of difficulties | |||
| None (ref.) | 1 | ||
| Some | 2.11 | ** | 1.59–2.83 |
| A lot | 6.73 | ** | 3.83–11.86 |
| Cannot do at all | 11.03 | ** | 5.67–21.44 |
| Age | |||
| Youth (18–24 years-old) (ref.) | 1 | ||
| Older adults (25–59 years-old) | 2.74 | ** | 1.71–4.41 |
| Elderly (60+ years-old) | 7.52 | ** | 4.18–13.55 |
| Sex | |||
| Female (ref.) | 1 | ||
| Male | 1.00 | 0.68–1.48 | |
| School attendance | |||
| Never attended (ref.) | 1 | ||
| Ever attended | 2.92 | ** | 2.08–4.10 |
| Working status | |||
| Not working (ref.) | 1 | ||
| Working | 0.71 | 0.47–1.07 | |
| District of residence | |||
| Kurigram (ref.) | 1 | ||
| Narsingdi | 1.47 | * | 1.08–2.00 |
| Constant | 0.01 | ** | 0.00–0.01 |
| N | 2,483,629 | ||
| n | 4253 | ||
| Characteristics | % Reporting Unmet Needs | OR | 95% CI |
|---|---|---|---|
| Level of difficulties | |||
| Some | 67.9% | 1 | 0.71–7.05 |
| A lot | 83.4% | 2.24 | 0.20–2.64 |
| Cannot do | 60.2% | 0.73 | |
| Currently using AP | |||
| No | 68.2% | 1 | 1.52–15.30 |
| Yes | 88.3% | 4.82 ** | |
| Age group | |||
| Youth (18–24 years-old) | 77.6% | 1 | 0.22–1.96 |
| Older adults (25–59 years-old) | 67.1% | 0.65 | 0.32–3.42 |
| Elderly (60+ years-old) | 80.7% | 1.04 | |
| Sex | |||
| Female | 74.9% | 1 | 0.20–1.31 |
| Male | 74.4% | 0.51 | |
| School attendance | |||
| Never attended | 76.6% | 1 | 0.30–1.80 |
| Ever attended | 71.1% | 0.73 | |
| Working status | |||
| Not working | 71.4% | 1 | |
| Working | 86.2% | 5.71 * | 1.30–25.16 |
| District of residence | |||
| Kurigram | 85.0% | 1 | |
| Narsingdi | 59.4% | 0.34 * | 0.13–0.89 |
| All | 74.7% | ||
| Constant | 9.32 | 0.95–91.41 | |
| N | 96,815 | ||
| n | 180 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pryor, W.; Nguyen, L.; Islam, Q.N.; Jalal, F.A.; Marella, M. Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey. Int. J. Environ. Res. Public Health 2018, 15, 2901. https://doi.org/10.3390/ijerph15122901
Pryor W, Nguyen L, Islam QN, Jalal FA, Marella M. Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey. International Journal of Environmental Research and Public Health. 2018; 15(12):2901. https://doi.org/10.3390/ijerph15122901
Chicago/Turabian StylePryor, Wesley, Liem Nguyen, Qumrun Naher Islam, Faruk Ahmed Jalal, and Manjula Marella. 2018. "Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey" International Journal of Environmental Research and Public Health 15, no. 12: 2901. https://doi.org/10.3390/ijerph15122901
APA StylePryor, W., Nguyen, L., Islam, Q. N., Jalal, F. A., & Marella, M. (2018). Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey. International Journal of Environmental Research and Public Health, 15(12), 2901. https://doi.org/10.3390/ijerph15122901