Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample and Design
2.2. Instruments
2.3. Methodology
2.4. Data Analysis
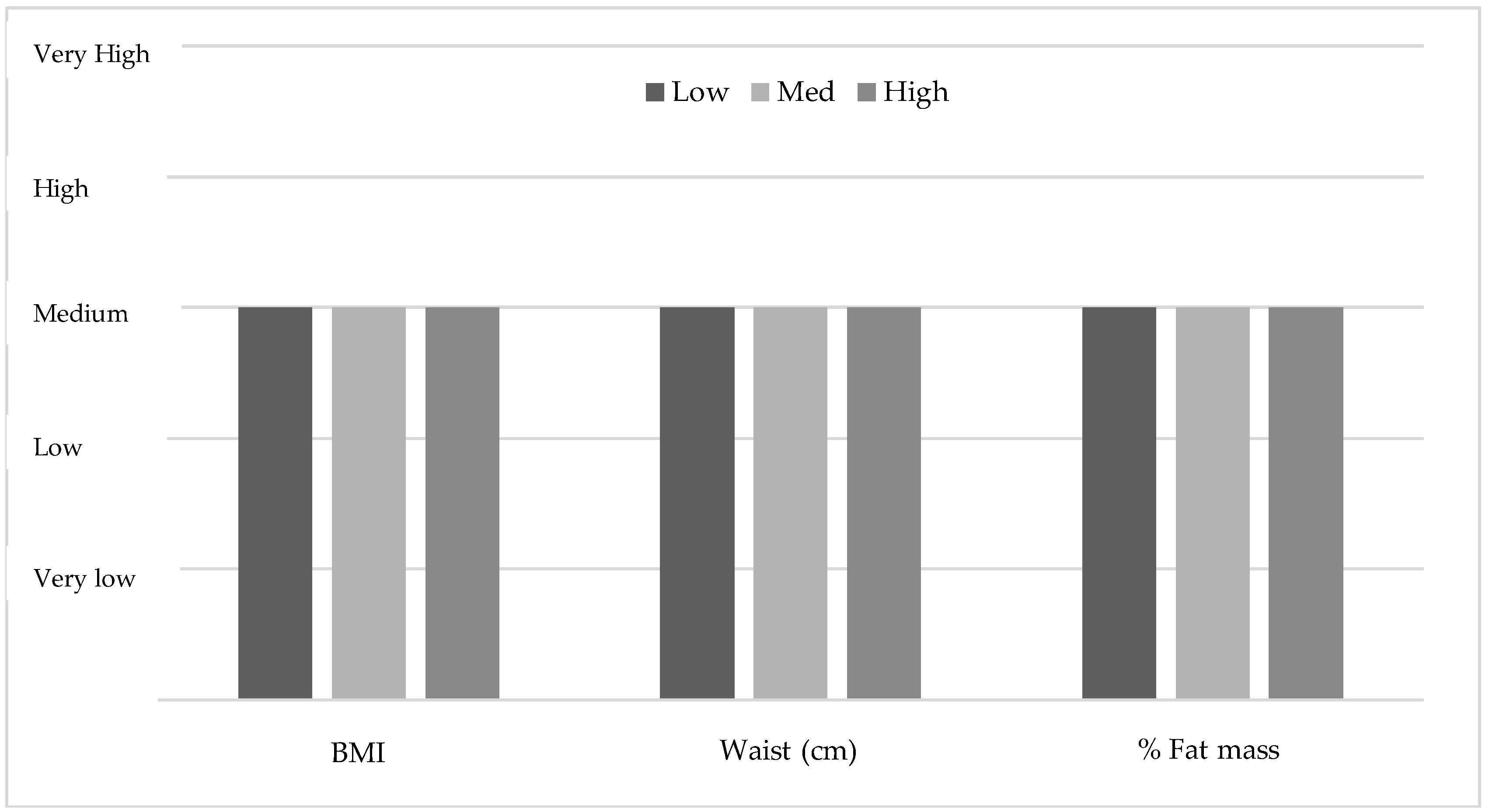
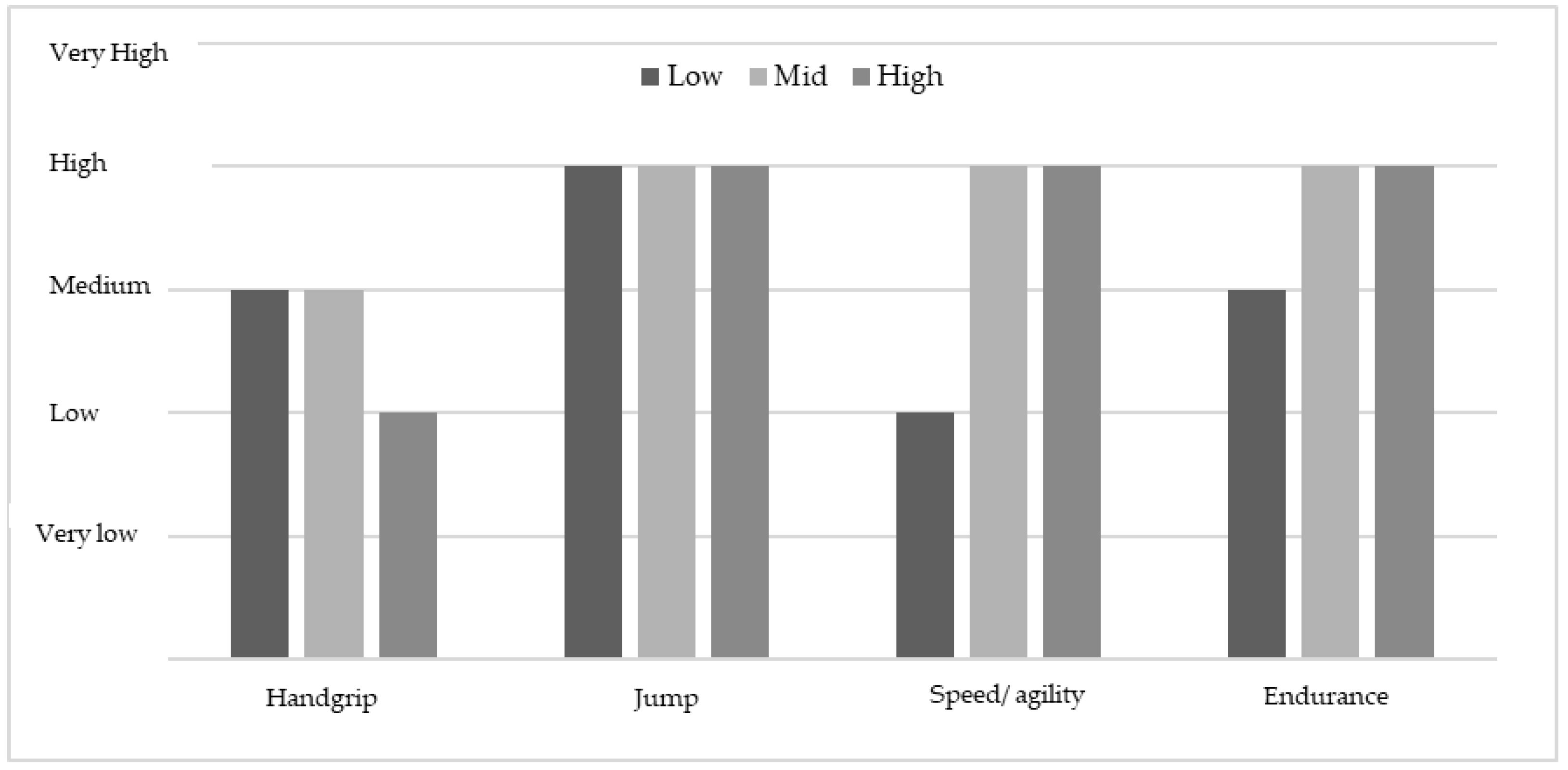
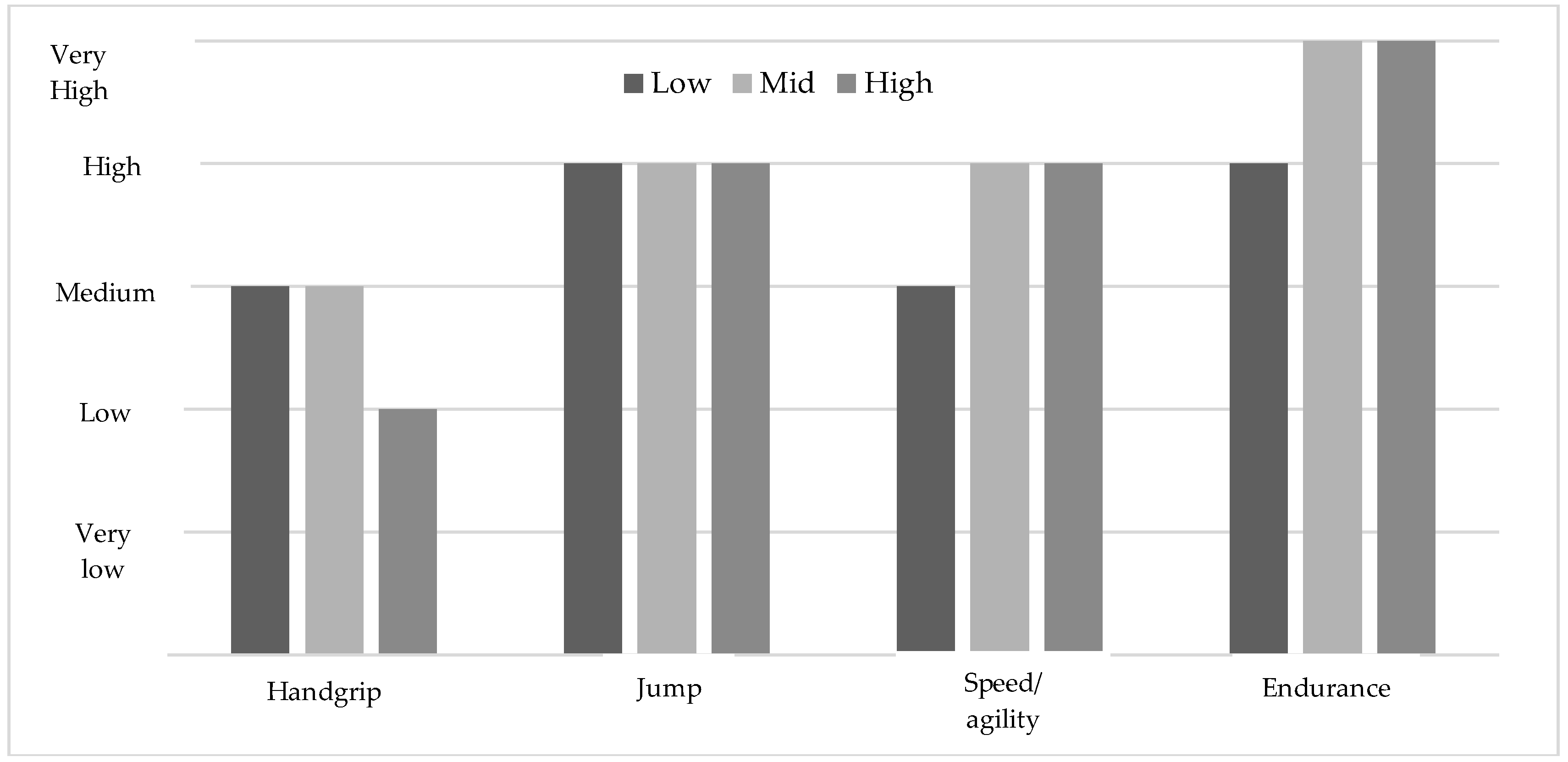
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sánchez-Oliver, A.J.; García, C.M.; Gálvez-Ruiz, P.; González-Jurado, J.A. Mortality and economic expenses of cardiovascular diseases caused by physical inactivity in Spain. J. Phys. Edu. Sport 2018, 18, 1420–1426. [Google Scholar]
- Diem, G.; Brownson, R.C.; Grabauskas, V.; Shatchkute, A.; Stachenko, S. Prevention and control of noncommunicable diseases through evidence-based public health: Implementing the NCD 2020 action plan. Glob. Health Promot. 2016, 23, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.; Guthold, R.; Cowan, M.; Savin, S.; Bhatti, L.; Armstrong, T.; Bonita, R. The World Health Organization STEPwise Approach to Noncommunicable Disease Risk-Factor Surveillance: Methods, Challenges, and Opportunities. Am. J. Public Health 2016, 106, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Tomba, E. Assessment of lifestyle in relation to health. In The Psychosomatic Assessment: Strategies to Improve Clinical Practice; Fava, G.A., Sonino, N., Wise, T.N., Eds.; Karger: Freiburg, Germany, 2012; Volume 32, pp. 72–96. ISBN 9783805598545. [Google Scholar]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Twig, G.; Yaniv, G.; Levine, H.; Leiba, A.; Goldberger, N.; Derazne, E.; Ben-Ami Shor, D.; Tzur, D.; Afek, A.; Shamiss, A.; et al. Body-Mass Index in 2.3 Million Adolescents and Cardiovascular Death in Adulthood. N. Engl. J. Med. 2016, 374, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.; Monasta, L.; Stamatakis, E.; Lioret, S.; Castetbon, K.; Frenken, F.; Manios, Y.; Moschonis, G.; Savva, S.; Zaborskis, A.; et al. Overweight and obesity in infants and pre-school children in the European Union: A review of existing data. Obes. Rev. 2010, 11, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Bennett, P.H.; Looker, H.C. Childhood Obesity, Other Cardiovascular Risk Factors, and Premature Death. N. Engl. J. Med. 2010, 362, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Goldsmith, R.; Berry, E.M. Demographic and lifestyle factors associated with adherence to the Mediterranean diet in relation to overweight/obesity among Israeli adolescents: Findings from the Mabat Israeli national youth health and nutrition survey. Public Health Nutr. 2017, 20, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Mårild, S.; Gronowitz, E.; Forsell, C.; Dahlgren, J.; Friberg, P. A controlled study of lifestyle treatment in primary care for children with obesity. Pediatr. Obes. 2013, 8, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 22, CD012651. [Google Scholar] [CrossRef] [PubMed]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 22, CD012691. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Carmona, W.; Sánchez-Oliver, A.; González-Jurado, J. Pathophysiology of obesity: Current view. Rev. Chil. Nutr. 2017, 44, 226–233. [Google Scholar]
- Caspersen, C.J.; Powell, K.E.; Christensen, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health- Related Research. Public Heal. Rec. 1985, 100, 126–131. [Google Scholar]
- Longmuir, P.; Colley, R.; Wherley, V.; Tremblay, M. Risks and benefits of childhood physical activity. Lancet Diabetes Endocrinol. 2014, 2, 861–862. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Gray, C.E.; Akinroye, K.; Harrington, D.M.; Katzmarzyk, P.T.; Lambert, E.V.; Liukkonen, J.; Maddison, R.; Ocansey, R.T.; Onywera, V.O.; et al. Physical Activity of Children: A Global Matrix of Grades Comparing 15 Countries. J. Phys. Act. Heal. 2014, 11, S113–S125. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R.; Global Matrix 2.0 Research Team. Introduction to the Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S85–S86. [Google Scholar] [CrossRef] [PubMed]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Freeman, L.B.; et al. Body-Mass Index and Mortality among 1.46 Million White Adults. N. Engl. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Blossner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action plan on Physical Activity 2018–2030: More Active People for a Healthier World; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Golden, N.H.; Abrams, S.A.; Committee on Nutrition. Optimizing bone health in children and adolescents. Pediatrics 2014, 134, e1229-43. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Janz, K.F.; Burns, T.L.; Levy, S.M. Tracking of activity and sedentary behaviors in childhood: The Iowa bone development study. Am. J. Prev. Med. 2005, 29, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Anderssen, S.A.; Froberg, K.; Sardinha, L.; Andersen, L.B.; Brage, S.; European Youth Heart Study Group. Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: The European youth heart study. Diabetologia 2007, 50, 1832–1840. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Mathers, J.C.; Rugg-Gunn, A.J.; Adamson, A.J. Longitudinal change in food habits between adolescence (11–12 years) and adulthood (32–33 years): The ASH30 study. J. Public Health 2006, 28, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Roman, B.; Estruch, R. Scientific evidence of interventions using the Mediterranean diet: A systematic review. Nutr. Rev. 2006, 64, S27–S47. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence about benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A.; Transmission, P.P. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2014, 337, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M.; Serra-Majem, L.; Lairon, D.; Estruch, R.; Trichopoulou, A. Mediterranean food pattern and the primary prevention of chronic disease: Recent developments. Nutr. Rev. 2009, 67 (Suppl. 1), S111–S116. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to mediterranean diet and risk of cancer: An updated systematic review and meta-analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Novak, D.; Štefan, L.; Prosoli, R.; Emeljanovas, A.; Mieziene, B.; Milanović, I.; Radisavljević-Janić, S. Mediterranean Diet and its Correlates among Adolescents in Non-Mediterranean European Countries: A Population-Based Study. Nutrients 2017, 9, 177. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Martin-Calvo, N.; Chavarro, J.E.; Falbe, J.; Hu, F.B.; Field, A.E. Adherence to the Mediterranean dietary pattern and BMI change among US adolescents. Int. J. Obes. 2016, 40, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health Physical Inactivity: A Global Public Health Problem Physical Inactivity; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Sallis, J.F.; Glanz, K. Physical activity and food environments: Solutions to the obesity epidemic. Milbank Q. 2009, 87, 123–154. [Google Scholar] [CrossRef] [PubMed]
- Evaristo, O.S.; Moreira, C.; Lopes, L.; Abreu, S.; Agostinis-Sobrinho, C.; Oliveira-Santos, J.; Póvoas, S.; Oliveira, A.; Santos, R.; Mota, J. Associations between physical fitness and adherence to the Mediterranean diet with health-related quality of life in adolescents: Results from the LabMed Physical Activity Study. Eur. J. Public Health 2018, 28, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Agostinis-Sobrinho, C.; Santos, R.; Rosário, R.; Moreira, C.; Lopes, L.; Mota, J.; Martinkenas, A.; García-Hermoso, A.; Correa-Bautista, J.; Ramírez-Vélez, R.; et al. Optimal Adherence to a Mediterranean Diet May not Overcome the Deleterious Effects of Low Physical Fitness on Cardiovascular Disease Risk in Adolescents: A Cross-Sectional Pooled Analysis. Nutrients 2018, 10, 815. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Ojeda-Pardo, M.L.; Sandoval-Cuellar, C.; García-Hermoso, A.; Carrillo, H.A.; González-Ruíz, K.; Prieto-Benavides, D.H.; Tordecilla-Sanders, A.; Martinkėnas, A.; et al. Optimal Adherence to a Mediterranean Diet and High Muscular Fitness Are Associated with a Healthier Cardiometabolic Profile in Collegiate Students. Nutrients 2018, 10, 511. [Google Scholar] [CrossRef] [PubMed]
- Agostinis-Sobrinho, C.; Ramírez-Vélez, R.; García-Hermoso, A.; Rosário, R.; Moreira, C.; Lopes, L.; Martinkenas, A.; Mota, J.; Santos, R. The combined association of adherence to Mediterranean diet, muscular and cardiorespiratory fitness on low-grade inflammation in adolescents: A pooled analysis. Eur. J. Nutr. 2018, 3, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Albert Pérez, E.; Mateu Olivares, V.; Martínez-Espinosa, R.M.; Molina Vila, M.D.; Reig García-Galbis, M. New Insights about How to Make an Intervention in Children and Adolescents with Metabolic Syndrome: Diet, Exercise vs. Changes in Body Composition. A Systematic Review of RCT. Nutrients 2018, 10, 878. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; Estruch, R.; et al. PREDIMED-Plus investigators. Effect of a lifestyle intervention program with energy-restricted Mediterranean diet and exercise on weight loss and cardiovascular risk factors: One-year results of the PREDIMED-Plus trial. Diabetes Care. 1808, dc180836, (Epub ahead of print). [Google Scholar] [CrossRef]
- Ros, E.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Fitó, M.; Martínez, J.A.; Corella, D. Mediterranean Diet and Cardiovascular Health: Teachings of the PREDIMED Study. Adv. Nutr. 2014, 5, 330S–336S. [Google Scholar] [CrossRef] [PubMed]
- Organización Mundial de la Salud. Estrategia Mundial Para la Salud de la Mujer, el Niño y el Adolescente (2016–2030); Organización Mundial de la Salud: Geneva, Switzerland, 2015. [Google Scholar]
- Khatib, O. Noncommunicable diseases: Risk factors and regional strategies for prevention and care. East. Mediterr. Health J. 2004, 10, 778–788. [Google Scholar] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. Suppl. 2004, 5, 4–104. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; de Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12, CD001871. [Google Scholar] [CrossRef] [PubMed]
- Wolfenden, L.; Jones, J.; Williams, C.M.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2016, 10, CD011779. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- García Cabrera, S.; Herrera Fernández, N.; Rodríguez Hernández, C.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the Mediterranean Diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar] [PubMed]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.A.M.; Enez-Pavón, D.J.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Villa-González, E.; Ruiz, J.R.; Chillón, P. Associations between active commuting to school and health-related physical fitness in Spanish school-aged children: A cross-sectional study. Int. J. Environ. Res. Public Health 2015, 12, 10362–10373. [Google Scholar] [CrossRef] [PubMed]
- España-Romero, V.; Artero, E.G.; Santaliestra-Pasias, A.M.; Gutierrez, A.; Castillo, M.J.; Ruiz, J.R. Hand Span Influences Optimal Grip Span in Boys and Girls Aged 6 to 12 Years. J. Hand Surg. Am. 2008, 33, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Mesana, M.I.; González-Gross, M.; Gil, C.M.; Fleta, J.; Wärnberg, J.; Ruiz, J.R.; Sarría, A.; Marcos, A.; Bueno, M.; et al. Anthropometric body fat composition reference values in Spanish adolescents. The AVENA Study. Eur. J. Clin. Nutr. 2006, 60, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Mesana, M.I.; González-Gross, M.; Gil, C.M.; Ortega, F.B.; Fleta, J.; Wärnberg, J.; León, J.F.; Marcos, A.; Bueno, M.; et al. Body fat distribution reference standards in Spanish adolescents: The AVENA Study. Int. J. Obes. 2007, 31, 1798–1805. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.; Artero, E.; Ruiz, J.; España-Romero, V.; Jiménez-Pavón, D.; Vicente-Rodriguez, G.; Moreno, L.; Manios, Y.; Béghin, L.; Ottevaere, C.; et al. Physical fitness levels among European adolescents: The HELENA study. Br. J. Sports Med. 2011, 45, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Barker, A.R.; Gracia-Marco, L.; Ruiz, J.R.; Castillo, M.J.; Aparicio-Ugarriza, R.; González-Gross, M.; Kafatos, A.; Androutsos, O.; Polito, A.; Molnar, D.; et al. Physical activity, sedentary time, TV viewing, physical fitness and cardiovascular disease risk in adolescents: The HELENA study. Int. J. Cardiol. 2018, 254, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Gualteros, J.A.; Torres, J.A.; Umbarila-Espinosa, L.M.; Rodríguez-Valero, F.J.; Ramírez-Vélez, R. A lower cardiorespiratory fitness is associated to an unhealthy status among children and adolescents from Bogotá, Colombia. Endocrinol. Nutr. 2015, 62, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, L.; Syväoja, H.; Kallio, J.; Kulmala, J.; Kujala, U.M.; Tammelin, T.H. Objectively measured physical activity, body composition and physical fitness: Cross-sectional associations in 9- to 15-year-old children. Eur. J. Sport Sci. 2018, 18, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Syväoja, H.J.; Kankaanpää, A.; Kallio, J.; Hakonen, H.; Kulmala, J.; Hillman, C.H.; Pesonen, A.-K.; Tammelin, T.H. The relation of physical activity, sedentary behaviors, and academic achievement is mediated by fitness and bedtime. J. Phys. Act. Health 2018, 15, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Wärnberg, J.; Ruiz, J.R.; Ortega, F.B.; Romeo, J.; González-Gross, M.; Moreno, L.A.; García-Fuentes, M.; Gómez, S.; Nova, E.; Díaz, L.E. Estudio AVENA (Alimentación y valoración del estado nutricional en adolescentes). Resultados obtenidos 2003–2006. Pediatr. Integr. 2006, 1, 50–55. [Google Scholar]
- García-Sánchez, A.; Burgueño-Menjibar, R.; López-Blanco, D.; Ortega, F.B. Condición física, adiposidad y autoconcepto en adolescentes. Estudio piloto. Rev. Psicol. Deport. 2013, 22, 453–461. [Google Scholar]
- Secchi, J.D.; García, G.C.; España-Romero, V.; Castro-Piñero, J. Condición física y riesgo cardiovascular futuro en niños y adolescentes argentinos: Una introducción de la batería ALPHA. Arch. Argent. Pediatr. 2014, 112, 132–140. [Google Scholar] [PubMed]
- Fernández, I.; Canet, O.; Giné-Garriga, M. Assessment of physical activity levels, fitness and perceived barriers to physical activity practice in adolescents: Cross-sectional study. Eur. J. Pediatr. 2017, 176, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Buchan, D.S.; Boddy, L.M.; Young, J.D.; Cooper, S.M.; Noakes, T.D.; Mahoney, C.; Shields, J.P.H.; Baker, J.S. Relationships between Cardiorespiratory and Muscular Fitness with Cardiometabolic Risk in Adolescents. Res. Sport. Med. 2015, 23, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education, Science and Culture. Icelandic National Curriculum Guide for Compulsory Schools –with Subjects Areas; Ministry of Education, Science and Culture: Reykjavik, Iceland, 2014; p. 250. ISBN 978-9935-436-24-5. [Google Scholar]
- Bacopoulou, F.; Landis, G.; Rentoumis, A.; Tsitsika, A.; Efthymiou, V. Mediterranean diet decreases adolescent waist circumference. Eur. J. Clin. Invest. 2017, 47, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Muros, J.; Salvador, F.; Zurita, F.; Gamez, V.K.E. The association between healthy lifestyle behaviors and health-related quality of life among adolescents. J. Pediatr. 2017, 93, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Martino, F.; Puddu, P.E.; Lamacchia, F.; Colantoni, C.; Zanoni, C.; Barillà, F.; Martino, E.; Angelico, F. Mediterranean diet and physical activity impact on metabolic syndrome among children and adolescents from Southern Italy: Contribution from the Calabrian Sierras Community Study (CSCS). Int. J. Cardiol. 2016, 225, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Martino, F.; Puddu, P.E.; Pannarale, G.; Colantoni, C.; Zanoni, C.; Martino, E.; Barillà, F. Metabolic syndrome among children and adolescents from Southern Italy: Contribution from the Calabrian Sierras Community Study (CSCS). Int. J. Cardiol. 2014, 177, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Mistretta, A.; Marventano, S.; Antoci, M.; Cagnetti, A.; Giogianni, G.; Nolfo, F.; Rametta, S.; Pecora, G.; Marranzano, M. Mediterranean diet adherence and body composition among Southern Italian adolescents. Obes. Res. Clin. Pract. 2017, 11, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Ozen, A.E.; Bibiloni, M.D.M.; Murcia, M.A.; Pons, A.; Tur, J.A. Adherence to the Mediterranean diet and consumption of functional foods among the Balearic Islands’ adolescent population. Public Health Nutr. 2015, 18, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Galvano, F. Mediterranean diet adherence in children and adolescents in southern European countries. NFS J. 2016, 3, 13–19. [Google Scholar] [CrossRef]
- Santomauro, F.; Lorini, C.; Tanini, T.; Indiani, L.; Lastrucci, V.; Comodo, N.; Bonaccorsi, G. Adherence to Mediterranean diet in a sample of Tuscan adolescents. Nutrition 2014, 30, 1379–1383. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Mendez, M.A.; Ribas-Barba, L.; Covas, M.-I.; Serra-Majem, L. Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int. J. Pediatr. Obes. 2010, 5, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.S.; Oliver, J.L. The youth physical development model: A new approach to long-term athletic development. Strength Cond. J. 2012, 34, 61–72. [Google Scholar] [CrossRef]
- de Oliveira, B.F.; de Carvalho, L.V.; de Souza Mourão, D.; da Costa, R.D.; de Castro, H.A.; Artaxo, P.; Junger, W.L.; Hacon, S. Environmental Exposure Associated with Oxidative Stress Biomarkers in Children and Adolescents Residents in Brazilian Western Amazon. J. Environ. Prot. 2018, 09, 347–367. [Google Scholar] [CrossRef]
- Damian, M.; Oltean, A.; Damian, C. The impact of sedentary behavior on health and the need for physical activity in children and adolescents. Rev. Rom. Pentru Educ. Multidimens. 2018, 10, 71. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD | Boys (n = 209) | Girls (n = 178) | p-Value |
|---|---|---|---|---|
| Age (year) | 13.48 ± 1.14 | 13.57 ± 1.13 | 13.38 ± 1.14 | 0.097 |
| Weight (kg) | 57.29 ± 13.53 | 59.20 ± 14.21 | 55.05 ± 12.36 | 0.010 * |
| Height (m) | 1.64 ± 0.10 | 1.67 ± 0.11 | 1.61 ± 0.81 | <0.001 * |
| BMI (kg/m2) | 22.26 ± 4.72 | 22.17 ± 4.91 | 22.37 ± 4.49 | 0.241 |
| Body fat (%) | 21.37 ± 8.79 | 17.37 ± 8.44 | 26.07 ± 6.61 | <0.001 * |
| Waist (cm) | 72.05 ± 10.12 | 73.91 ± 10.41 | 69.86 ± 9.34 | <0.001 * |
| Handgrip (kg) | 25.95 ± 7.01 | 28.18 ± 7.90 | 23.33 ± 4.58 | <0.001 * |
| Jump (cm) | 171.94 ± 1.51 | 182.94 ± 28.60 | 159.02 ± 25.51 | <0.001 * |
| 4 × 10 m (s) | 11.80 ± 1.40 | 11.53 ± 1.59 | 12.11 ± 1.06 | <0.001 * |
| Endurance (CRF) | 6.73 ± 2.52 | 7.52 ± 2.62 | 5.80 ± 2.04 | <0.001 * |
| KIDMED Index | 5.83 ± 2.31 | 5.82 ± 2.18 | 5.84 ± 2.46 | 0.940 |
| Variables | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| Low (n = 58/387) | Med (n = 235/387) | High (n = 94/387) | p-Value | Low (n = 58/387) | Med (n = 235/387) | High (n = 94/387) | p-Value | |
| Age (year) | 13.37 ± 1.30 | 13.61 ± 1.10 | 13.58 ± 1.13 | 0.562 | 13.18 ± 0.98 | 13.29 ± 1.11 | 13.07 ± 1.11 | 0.678 |
| Weight (kg) | 61.15 ± 15.62 | 59.72 ± 14.51 | 56.80 ± 12.48 | 0.332 | 57.34 ± 9.90 | 55.31 ± 12.78 | 52.83 ± 12.67 | 0.308 |
| High (m) | 1.64 ± 0.10 | 1.67 ± 0.11 | 1.66 ± 0.11 | 0.338 | 1.62 ± 0.60 | 1.61 ± 0.09 | 1.60 ± 0.07 | 0.586 |
| BMI (kg/m2) | 23.90 ± 6.06 | 22.07 ± 4.71 | 21.41 ± 4.52 | 0.080 | 22.34 ± 5.01 | 22.52 ± 4.40 | 22.01 ± 4.43 | 0.824 |
| Body fat (%) | 21.84 ± 10.01 a | 16.79 ± 7.92 | 16.21 ± 8.03 | 0.006 * | 26.50 ± 6.52 | 25.93 ± 6.69 | 26.16 ± 6.60 | 0.919 |
| Waist (cm) | 76.95 ± 11.75 | 73.87 ± 10.68 | 72.24 ± 8.56 | 0.142 | 70.48 ± 8.57 | 70.29 ± 9.54 | 68.33 ± 9.36 | 0.479 |
| Handgrip average (kg) | 27.99 ± 8.43 | 28.81 ± 7.88 | 26.75 ± 7.59 | 0.286 | 24.36 ± 3.69 | 23.40 ± 4.47 | 22.45 ± 5.31 | 0.225 |
| Jump (cm) | 177.2 ± 31.4 | 185.0 ± 27.7 | 181.3 ± 29.1 | 0.362 | 155.75 ± 25.68 | 160.02 ± 26.42 | 158.62 ± 23.33 | 0.730 |
| 4 × 10 m (s) | 12.42 ± 2.00 a | 11.29 ± 1.21 | 11.59 ± 1.96 | <0.002 * | 12.46 ± 0.90 | 12.04 ± 1.16 | 12.07 ± 1.17 | 0.174 |
| Endurance (CRF) | 6.28 ± 2.64 a | 7.68 ± 2.43 | 7.85 ± 2.88 | <0.018 * | 4.63 ± 1.32 a | 6.04 ± 2.12 | 5.94 ± 1.99 | 0.004 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galan-Lopez, P.; Ries, F.; Gisladottir, T.; Domínguez, R.; Sánchez-Oliver, A.J. Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. Int. J. Environ. Res. Public Health 2018, 15, 2632. https://doi.org/10.3390/ijerph15122632
Galan-Lopez P, Ries F, Gisladottir T, Domínguez R, Sánchez-Oliver AJ. Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. International Journal of Environmental Research and Public Health. 2018; 15(12):2632. https://doi.org/10.3390/ijerph15122632
Chicago/Turabian StyleGalan-Lopez, Pablo, Francis Ries, Thordis Gisladottir, Raúl Domínguez, and Antonio J. Sánchez-Oliver. 2018. "Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students" International Journal of Environmental Research and Public Health 15, no. 12: 2632. https://doi.org/10.3390/ijerph15122632
APA StyleGalan-Lopez, P., Ries, F., Gisladottir, T., Domínguez, R., & Sánchez-Oliver, A. J. (2018). Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. International Journal of Environmental Research and Public Health, 15(12), 2632. https://doi.org/10.3390/ijerph15122632