Prevalence of Childhood Overweight and Obesity in Liverpool between 2006 and 2012: Evidence of Widening Socioeconomic Inequalities


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Childhood Overweight and Obesity
2.2.2. Socioeconomic Inequality
2.3. Analysis
3. Results
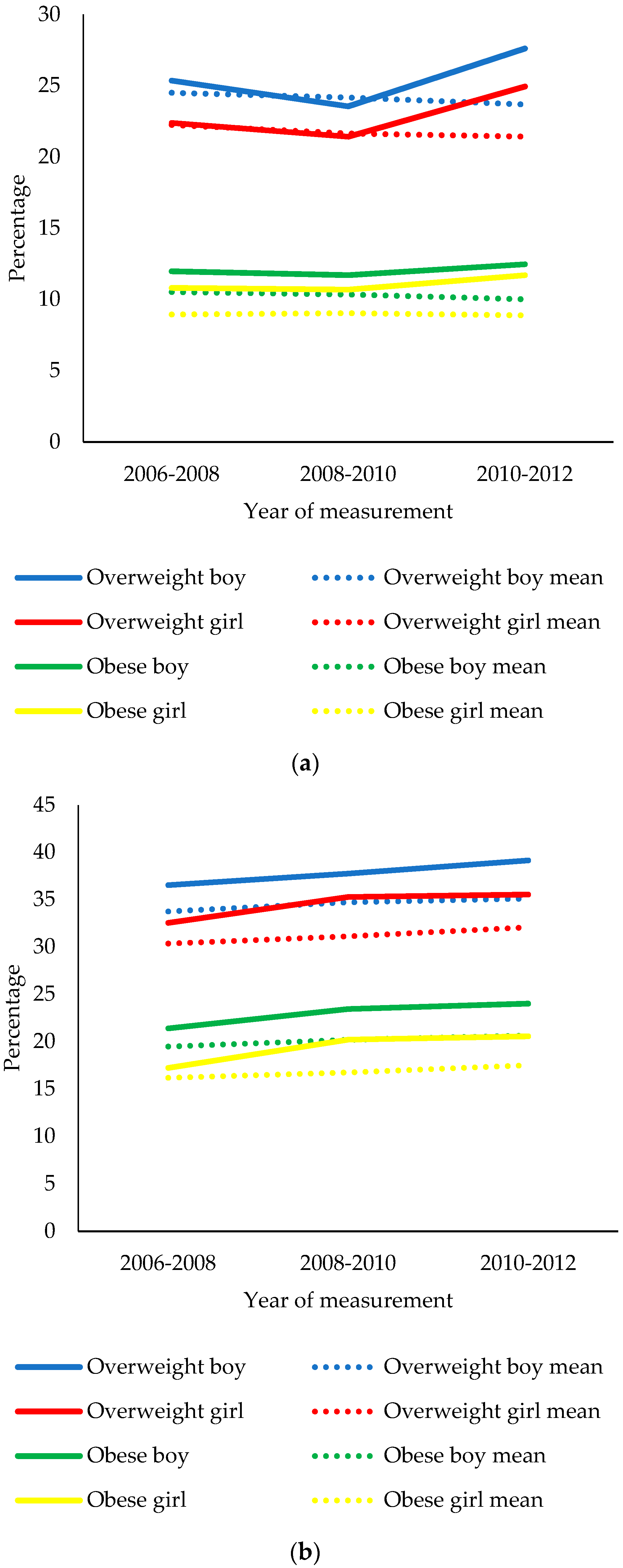
3.1. Study Aim 1
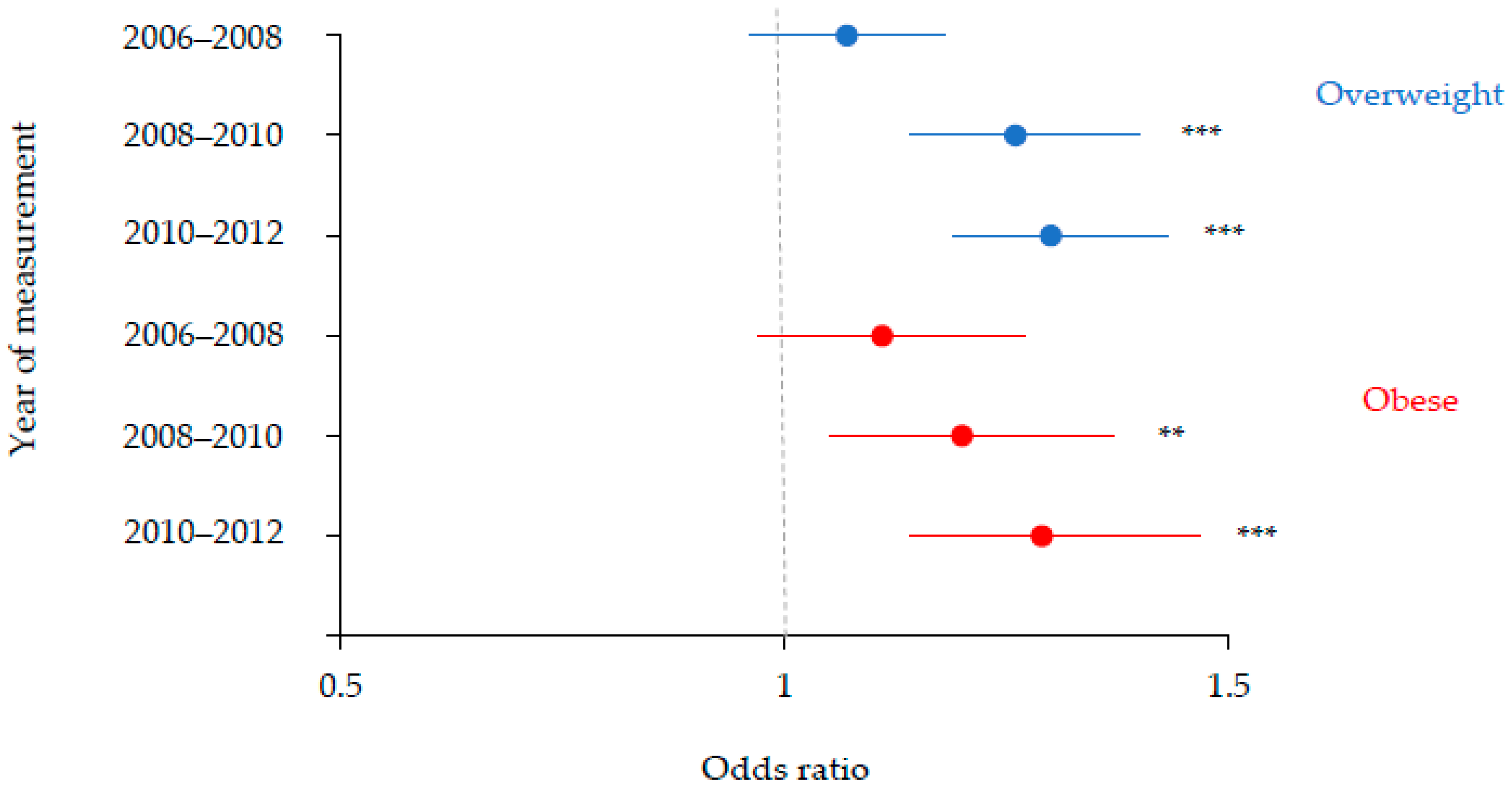
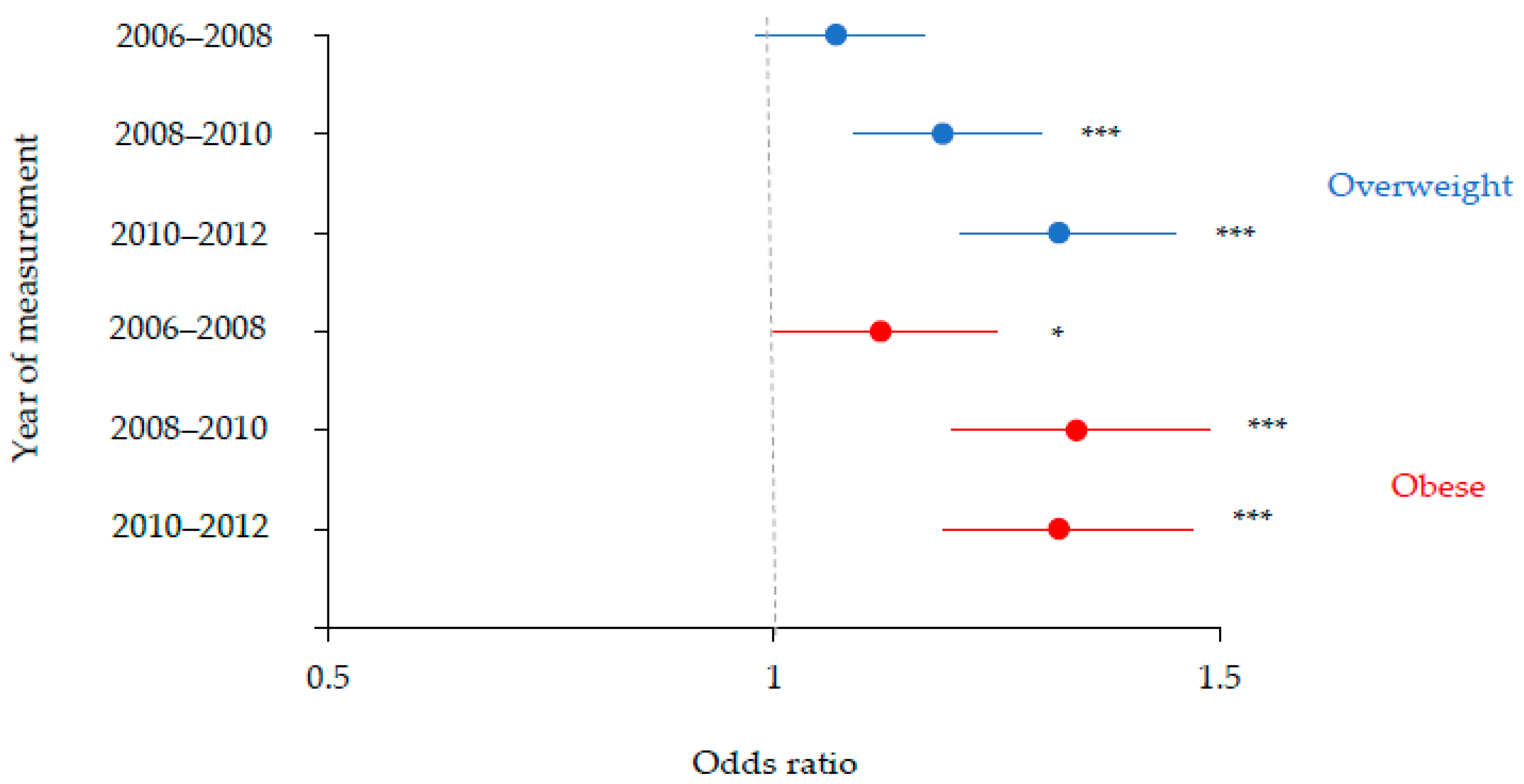
3.2. Study Aim 2
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Hayes, H.M.; Eisenmann, J.C.; Pfeiffer, K.; Carlson, J.J. Weight Status, Physical Activity, and Vascular Health in 9- to 12-Year-Old Children. J. Phys. Act. Health 2013, 10, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.H.; Byrne, C.D. ABC of obesity: Risk factors for diabetes and coronary heart disease. BMJ 2006, 333, 1009–1011. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Boddy, L.M.; Knowles, Z.R.; Fairclough, S.J. Cross-sectional associations between high-deprivation home and neighbourhood environments, and health-related variables among Liverpool children. BMJ Open 2016, 6, e008693. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Fairclough, S.J. Is there a deprivation and maternal education gradient to child obesity and moderate-to-vigorous physical activity? Findings from the Millennium Cohort Study. Pediatr. Obes. 2018, 13, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Stafford, M.; Marmot, M. Neighbourhood deprivation and health: Does it affect us all equally? Int. J. Epidemiol. 2003, 32, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Cetateanu, A.; Jones, A. Understanding the relationship between food environments, deprivation and childhood overweight and obesity: Evidence from a cross sectional England-wide study. Health Place 2014, 27, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Maguire, E.R.; Burgoine, T.; Monsivais, P. Area deprivation and the food environment over time: A repeated cross-sectional study on takeaway outlet density and supermarket presence in Norfolk, UK, 1990–2008. Health Place 2015, 33, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.R.V.; Tong, T.Y.N.; Monsivais, P. Meeting UK dietary recommendations is associated with higher estimated consumer food costs: An analysis using the National Diet and Nutrition Survey and consumer expenditure data, 2008–2012. Public Health Nutr. 2017, 21, 948–956. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Kelly, B.; Chapman, K.; King, L.; Farrell, L. Parental perceptions of barriers to children’s participation in organised sport in Australia. J. Paediatr. Child Health 2010, 46, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, R.; Kasim, A.; Warren, J.; Akhter, N.; Bambra, C. Geographical inequalities in health in a time of austerity: Baseline findings from the Stockton-on-Tees cohort study. Health Place 2017, 48, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Conrad, D.; Capewell, S. Associations between deprivation and rates of childhood overweight and obesity in England, 2007–2010: An ecological study. BMJ Open 2012, 2, e000463. [Google Scholar] [CrossRef] [PubMed]
- Goisis, G.; Sacker, A.; Kelly, Y. Why are poorer children at higher risk of obesity and overweight? A UK cohort study. Eur. J. Public Health 2015, 26, 7–13. [Google Scholar] [CrossRef] [PubMed]
- van Jaarsveld, C.H.M.; Gulliford, M.C. Childhood obesity trends from primary care electronic health records in England between 1994 and 2013: Population-based cohort study. Arch. Dis. Child. 2015, 100, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Wabitsch, M.; Moss, A.; Kromeyer-Hauschild, K. Unexpected plateauing of childhood obesity rates in developed countries. BMC Med. 2014, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Wardle, J.; Cole, T.J. Childhood obesity and overweight prevalence trends in England: Evidence for growing socioeconomic disparities. Int. J. Obes. 2010, 34, 41–47. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Rehkopf, D.; Mortensen, L.H. Trends in socioeconomic inequalities in body mass index, underweight and obesity among English children, 2007–2008 to 2011–2012. PLoS ONE 2016, 11, e0147614. [Google Scholar] [CrossRef] [PubMed]
- Department for Communities and Local Government. The English Indices of Deprivation 2015; Communities and Local Government Publications: Wetherby, UK, 2015.
- Public Health England. Child Health Profile; Public Health England: London, UK, 2018.
- Boddy, L.M.; Hackett, A.F.; Stratton, G. Changes in BMI and prevalence of obesity and overweight in children in Liverpool, 1998–2006. Perspect. Public Health 2009, 129, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. PSA Obesity Target; Department of Health, the Department of Culture Media and Sport and the Department for Education and Skills: London, UK, 2004.
- Parnell, D.; Millward, P.; Widdop, P.; King, N.; May, A. Sport policy and politics in an era of austerity. Int. J. Sport Policy Politics 2018, 10, 1–5. [Google Scholar] [CrossRef]
- Dawson, J.; Huikuri, S.; Armada, F. Liverpool Active City 2005–2010: Increasing Population Physical Activity Levels Through Intersectoral Action. J. Phys. Act. Health 2015, 12, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Taste for Health. Available online: http://www. tasteforhealth.com (accessed on 10 October 2018).
- Taylor, S.; Hackett, A.; Stratton, G.; Lamb, L. SportsLinx: Improving the health and fitness of Liverpool’s youth. Educ. Health 2004, 22, 3–7. [Google Scholar]
- National Children’s Bureau. Cuts That Cost: Trends in Funding for Early Intervention Services; National Children’s Bureau: London, UK, 2015.
- UK Parliament. Impact of the Spending Review on Health and Social Care. 2016. Available online: https://www.publications.parliament.uk/pa/cm201617/cmselect/cmhealth/139/13902.htm?utm_source=139&utm_medium=fullbullet&utm_campaign=Modulereports (accessed on 12 May 2018).
- The Guardian. In Liverpool, Tory Cuts Have Brought a City and Its People to Breaking Point. 2017. Available online: https://www.theguardian.com/commentisfree/2017/mar/23/liverpooltory-cuts-city-benefits-poorest (accessed on 12 May 2018).
- Davis, A.; Hirsch, D.; Padley, M. A Minimum Income Standard for the UK in 2014; Joseph Rowntree Foundation: York, UK, 2014. [Google Scholar]
- Public Health England. National Child Measurement Programme Operational Guidance; Public Health England: London, UK, 2014.
- Cole, T.J.; Freeman, J.V.; Preece, M.A. Body mass index reference curves for the UK. Arch. Dis. Child. 1995, 73, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Department for Communities and Local Government. The English Indices of Deprivation 2010; Communities and Local Government Publications: Wetherby, UK, 2010.
- The NHS Information Centre. National Child Measurement Programme: England, 2006/07 School Year; Department of Health: London, UK, 2007.
- The NHS Information Centre. National Child Measurement Programme: England, 2007/08 School Year; Department of Health: London, UK, 2008.
- The NHS Information Centre. National Child Measurement Programme: England, 2008/09 School Year; Department of Health: London, UK, 2009.
- The NHS Information Centre. National Child Measurement Programme: England, 2009/10 School Year; Department of Health: London, UK, 2010.
- The NHS Information Centre. National Child Measurement Programme: England, 2010/11 School Year; Department of Health: London, UK, 2011.
- The NHS Information Centre. National Child Measurement Programme: England, 2011/12 School Year; Department of Health: London, UK, 2012.
- Noonan, R.J. The effect of childhood deprivation on weight status and mental health in childhood and adolescence: Longitudinal findings from the Millennium Cohort Study. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Vizard, P.; Obolenskaya, P. Labour’s Record on Health 1997–2010; London School of Economics and Political Science: London, UK, 2013. [Google Scholar]
- Defra. Food Statistics Pocket Book: In Year Update; Defra: London, UK, 2014. [Google Scholar]
- Lambie-Mumford, H.; Green, M.A. Austerity, welfare reform and the rising use of food banks by children in England and Wales. Area 2017, 49, 273–279. [Google Scholar] [CrossRef]
- Loopstra, R.; Reeves, A.; Taylor-Robinson, D.; Barr, B.; McKee, M. Austerity, sanctions, and the rise of food banks in the UK. BMJ 2015, 350, h1775. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, F.; Ward, M. Poverty in the Liverpool City Region; House of Commons: London, UK, 2017.
- Backholer, K.; Beauchamp, A.; Ball, K.; Turrell, G.; Martin, J.; Woods, J.; Peeters, A. A framework for evaluating the impact of obesity prevention strategies on socioeconomic inequalities in weight. Am. J. Public Health 2014, 104, e43–e50. [Google Scholar] [CrossRef] [PubMed]
- Olstad, D.L.; Teychenne, M.; Minaker, L.M. Can policy ameliorate socioeconomic inequities in obesity and obesity-related behaviours? A systematic review of the impact of universal policies on adults and children. Obes. Rev. 2016, 17, 1198–1217. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Change4Life. Available online: https://campaignresources.phe.gov.uk/resources/campaigns/17-change4life/overview (accessed on 21 November 2018).
- Taylor-Robinson, D.C. Bigger Cuts to Sure Start Children’s Centres in More Disadvantaged Areas. Available online: https://www.bmj.com/content/359/bmj.j5332/rr (accessed on 21 November 2018).
- MRC Epidemiology Unit. Food Environment Assessment Tool (Feat). Available online: http://www.feat-tool.org.uk/ (accessed on 21 November 2018).
- Sweeting, H.N. Measurement and Definitions of Obesity in Childhood and Adolescence: A field guide for the uninitiated. Nutr. J. 2007, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: A systematic review and meta-analysis. Pediatr. Obes. 2015, 34, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Freeman, J.V.; Preece, M.A. British 1990 growth reference centiles for weight, height, body mass index and head circumference fitted by maximum penalized likelihood. Stat. Med. 1998, 17, 407–429. [Google Scholar] [CrossRef]
- Freeman, J.V.; Cole, T.J.; Chinn, S.; Jones, P.R.M.; White, E.M.; Preece, M.A. Cross sectional stature and weight reference curves for the UK, 1990. Arch. Dis. Child. 1995, 73, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.; Webb-Phillips, S.; Bray, I. Changes in objectively measured BMI in children aged 4–11 years: Data from the National Child Measurement Programme. J. Public Health 2015, 38, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Primatesta, P.; Chinn, S.; Falascheti, E. Overweight and obesity trends from 1974 to 2003 in English children: What is the role of socioeconomic factors? Arch. Dis. Child. 2005, 90, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Casanova, I.; Sarmiento, O.L.; Gazmararian, J.A.; Cunningham, S.A.; Martorell, R.; Pratt, M.; Stein, A.D. Comparing three body mass index classification systems to assess overweight and obesity in children and adolescents. Revista Panamericana de Salud Pública 2013, 33, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.A.; Kipping, R.R.; Jago, R.; Lawlor, D.A. Variation in childhood and adolescent obesity prevalence defined by international and country-specific criteria in England and the United States. Eur. J. Clin. Nutr. 2011, 65, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Falconer, C.L.; Park, M.H.; Croker, H.; Kessel, A.S.; Saxena, S.; Viner, R.M.; Kinra, S. Can the relationship between ethnicity and obesity-related behaviours among school-aged children be explained by deprivation? A cross-sectional study. BMJ Open 2014, 4, e003949. [Google Scholar] [CrossRef] [PubMed]
- Liverpool City Council. Ethnicity in Liverpool: 2011 Census. Available online: https://liverpool.gov.uk/media/9899/ethnicity-and-migration.pdf (accessed on 21 November 2018).
- HM Government. Childhood Obesity: A Plan for Action, Chapter 2; HM Government: London, UK, 2016.



© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noonan, R.J. Prevalence of Childhood Overweight and Obesity in Liverpool between 2006 and 2012: Evidence of Widening Socioeconomic Inequalities. Int. J. Environ. Res. Public Health 2018, 15, 2612. https://doi.org/10.3390/ijerph15122612
Noonan RJ. Prevalence of Childhood Overweight and Obesity in Liverpool between 2006 and 2012: Evidence of Widening Socioeconomic Inequalities. International Journal of Environmental Research and Public Health. 2018; 15(12):2612. https://doi.org/10.3390/ijerph15122612
Chicago/Turabian StyleNoonan, Robert J. 2018. "Prevalence of Childhood Overweight and Obesity in Liverpool between 2006 and 2012: Evidence of Widening Socioeconomic Inequalities" International Journal of Environmental Research and Public Health 15, no. 12: 2612. https://doi.org/10.3390/ijerph15122612
APA StyleNoonan, R. J. (2018). Prevalence of Childhood Overweight and Obesity in Liverpool between 2006 and 2012: Evidence of Widening Socioeconomic Inequalities. International Journal of Environmental Research and Public Health, 15(12), 2612. https://doi.org/10.3390/ijerph15122612