Risk Factors Contributing to Higher Mortality Rates in Elderly Patients with Acute Traumatic Subdural Hematoma Sustained in a Fall: A Cross-Sectional Analysis Using Registered Trauma Data

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
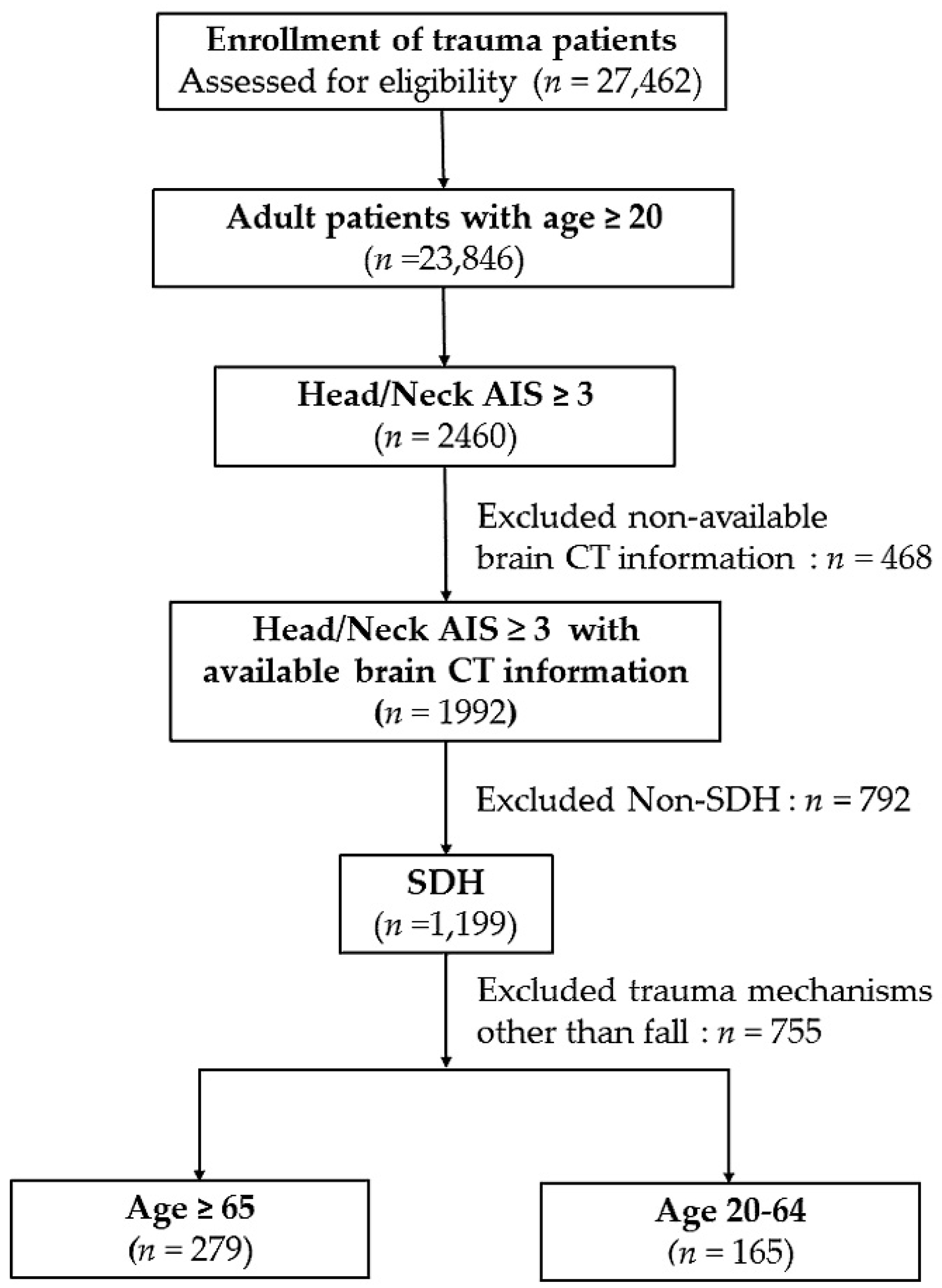
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Patient and Injury Characteristics
3.2. Patient Outcomes
3.3. Risk Factors for Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rau, C.S.; Lin, T.S.; Wu, S.C.; Yang, J.C.; Hsu, S.Y.; Cho, T.Y.; Hsieh, C.H. Geriatric hospitalizations in fall-related injuries. Scand. J. Trauma Resusc. Emerg. Med. 2014, 22, 63. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.G.; Thompson, R.E.; Temkin, N.R.; Crane, P.K.; Ellenbogen, R.G.; Elmore, J.G. Acute traumatic subdural hematoma: Current mortality and functional outcomes in adult patients at a Level I trauma center. J. Trauma Acute Care Surg. 2012, 73, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Leitgeb, J.; Mauritz, W.; Brazinova, A.; Janciak, I.; Majdan, M.; Wilbacher, I.; Rusnak, M. Outcome after severe brain trauma due to acute subdural hematoma. J. Neurosurg. 2012, 117, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Anandasivam, N.S.; Russo, G.S.; Samuel, A.M.; Grant, R.; Bohl, D.D.; Grauer, J.N. Injuries Associated with Subdural Hematoma: A Study of the National Trauma Data Bank. Conn. Med. 2017, 81, 215–222. [Google Scholar] [PubMed]
- Ledic, D.; Girotto, D.; Pal, S.; Kolbah, B. Risk factors for subdural bleeding in elderly population. Coll. Antropol. 2014, 38, 1195–1198. [Google Scholar] [PubMed]
- Shen, J.; Pan, J.W.; Fan, Z.X.; Zhou, Y.Q.; Chen, Z.; Zhan, R.Y. Surgery for contralateral acute epidural hematoma following acute subdural hematoma evacuation: Five new cases and a short literature review. Acta Neurochir. 2013, 155, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Maxeiner, H.; Wolff, M. Pure subdural hematomas: A postmortem analysis of their form and bleeding points. Neurosurgery 2002, 50, 503–508; discussion 508-9. [Google Scholar] [PubMed]
- Chisholm, K.M.; Harruff, R.C. Elderly deaths due to ground-level falls. Am. J. Forensic Med. Pathol. 2010, 31, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Murray, G.D.; Butcher, I.; McHugh, G.S.; Lu, J.; Mushkudiani, N.A.; Maas, A.I.; Marmarou, A.; Steyerberg, E.W. Multivariable prognostic analysis in traumatic brain injury: Results from the IMPACT study. J. Neurotrauma 2007, 24, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Won, S.Y.; Dubinski, D.; Bruder, M.; Cattani, A.; Seifert, V.; Konczalla, J. Acute subdural hematoma in patients on oral anticoagulant therapy: Management and outcome. Neurosurg. Focus 2017, 43, E12. [Google Scholar] [CrossRef] [PubMed]
- McClaskey, E.M.; Michalets, E.L. Subdural hematoma after a fall in an elderly patient taking high-dose omega-3 fatty acids with warfarin and aspirin: Case report and review of the literature. Pharmacotherapy 2007, 27, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Wilberger, J.E., Jr.; Harris, M.; Diamond, D.L. Acute subdural hematoma: Morbidity, mortality, and operative timing. J. Neurosurg. 1991, 74, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Prasad, G.L.; Anmol, N.; Menon, G.R. Outcome of Traumatic Brain Injury in the Elderly Population: A Tertiary Center Experience in a Developing Country. World Neurosurg. 2018, 111, e228–e234. [Google Scholar] [CrossRef] [PubMed]
- Perel, P.; Roberts, I.; Bouamra, O.; Woodford, M.; Mooney, J.; Lecky, F. Intracranial bleeding in patients with traumatic brain injury: A prognostic study. BMC Emerg. Med. 2009, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Khormi, Y.H.; Gosadi, I.; Campbell, S.; Senthilselvan, A.; O’Kelly, C.; Zygun, D. Adherence to Brain Trauma Foundation Guidelines for Management of Traumatic Brain Injury Patients and Its Effect on Outcomes: Systematic Review. J. Neurotrauma 2018, 35, 1407–1418. [Google Scholar] [CrossRef] [PubMed]
- Hukkelhoven, C.W.; Steyerberg, E.W.; Habbema, J.D.; Farace, E.; Marmarou, A.; Murray, G.D.; Marshall, L.F.; Maas, A.I. Predicting outcome after traumatic brain injury: Development and validation of a prognostic score based on admission characteristics. J. Neurotrauma 2005, 22, 1025–1039. [Google Scholar] [CrossRef] [PubMed]
- Bartek, J., Jr.; Laugesen, C.; Mirza, S.; Forsse, A.; Petersen, M.A.; Corell, A.; Dyhrfort, P.W.; Redebrandt, H.N.; Reen, L.; Zolfaghari, S.; et al. Scandinavian Multicenter Acute Subdural Hematoma (SMASH) Study: Study Protocol for a Multinational Population-Based Consecutive Cohort. Neurosurgery 2018. [Google Scholar] [CrossRef] [PubMed]
- El-Fiki, M. Acute traumatic subdural hematoma outcome in patients older than 65 years. World Neurosurg. 2012, 78, 228–230. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.G.; Singh, D.; Khandelwal, N.; Sharma, S.K. Dating of Early Subdural Haematoma: A Correlative Clinico-Radiological Study. J. Clin. Diagn. Res. 2016, 10, HC01–HC05. [Google Scholar] [CrossRef] [PubMed]
- Seddighi, A.S.; Motiei-Langroudi, R.; Sadeghian, H.; Moudi, M.; Zali, A.; Asheghi, E.; Alereza-Amiri, R.; Seddighi, A. Factors predicting early deterioration in mild brain trauma: A prospective study. Brain Inj. 2013, 27, 1666–1670. [Google Scholar] [CrossRef] [PubMed]
- Koc, R.K.; Akdemir, H.; Oktem, I.S.; Meral, M.; Menku, A. Acute subdural hematoma: Outcome and outcome prediction. Neurosurg. Rev. 1997, 20, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Feliciano, C.E.; De Jesus, O. Conservative management outcomes of traumatic acute subdural hematomas. Puerto Rico Health Sci. J. 2008, 27, 220–223. [Google Scholar]
- Benedetto, N.; Gambacciani, C.; Montemurro, N.; Morganti, R.; Perrini, P. Surgical management of acute subdural haematomas in elderly: Report of a single center experience. Br. J. Neurosurg. 2017, 31, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Valadka, A.B.; Sprunt, J.M. Craniotomy for acute subdural hematoma in the elderly: Not as bad as you thought. World Neurosurg. 2012, 78, 231–232. [Google Scholar] [CrossRef] [PubMed]
- De Bonis, P.; Trevisi, G.; de Waure, C.; Sferrazza, A.; Volpe, M.; Pompucci, A.; Anile, C.; Mangiola, A. Antiplatelet/anticoagulant agents and chronic subdural hematoma in the elderly. PLoS ONE 2013, 8, e68732. [Google Scholar] [CrossRef] [PubMed]
- Aspegren, O.P.; Astrand, R.; Lundgren, M.I.; Romner, B. Anticoagulation therapy a risk factor for the development of chronic subdural hematoma. Clin. Neurol. Neurosurg. 2013, 115, 981–984. [Google Scholar] [CrossRef] [PubMed]
- Bershad, E.M.; Farhadi, S.; Suri, M.F.; Feen, E.S.; Hernandez, O.H.; Selman, W.R.; Suarez, J.I. Coagulopathy and inhospital deaths in patients with acute subdural hematoma. J. Neurosurg. 2008, 109, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Raj, R.; Mikkonen, E.D.; Kivisaari, R.; Skrifvars, M.B.; Korja, M.; Siironen, J. Mortality in Elderly Patients Operated for an Acute Subdural Hematoma: A Surgical Case Series. World Neurosurg. 2016, 88, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Connolly, B.J.; Pearce, L.A.; Kurth, T.; Kase, C.S.; Hart, R.G. Aspirin therapy and risk of subdural hematoma: Meta-analysis of randomized clinical trials. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2013, 22, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Bakheet, M.F.; Pearce, L.A.; Hart, R.G. Effect of addition of clopidogrel to aspirin on subdural hematoma: Meta-analysis of randomized clinical trials. Int. J. Stroke off. J. Int. Stroke Soc. 2015, 10, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.K.; Lin, C.L.; Wu, Y.Y.; Kuo, H.L.; Lin, S.Y.; Chang, C.T.; Yen, T.H.; Chuang, F.R.; Cheng, Y.K.; Huang, C.C.; et al. Subdural hematoma in patients with end-stage renal disease receiving hemodialysis. Eur. J. Neurol. 2014, 21, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Lukasiewicz, A.M.; Grant, R.A.; Basques, B.A.; Webb, M.L.; Samuel, A.M.; Grauer, J.N. Patient factors associated with 30-day morbidity, mortality, and length of stay after surgery for subdural hematoma: A study of the American College of Surgeons National Surgical Quality Improvement Program. J. Neurosurg. 2016, 124, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Pruitt, P.; Ornam, J.V.; Borczuk, P. A Decision Instrument to Identify Isolated Traumatic Subdural Hematomas at Low Risk of Neurologic Deterioration, Surgical Intervention, or Radiographic Worsening. Acad. Emerg. Med. 2017, 24, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Savitsky, B.; Givon, A.; Rozenfeld, M.; Radomislensky, I.; Peleg, K. Traumatic brain injury: It is all about definition. Brain Inj. 2016, 30, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Parr, J.D.; Zhang, B.; Nilsson, M.E.; Wright, A.; Balboni, T.; Duthie, E.; Paulk, E.; Prigerson, H.G. The influence of age on the likelihood of receiving end-of-life care consistent with patient treatment preferences. J. Palliat. Med. 2010, 13, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Yadav, Y.R.; Basoor, A.; Jain, G.; Nelson, A. Expanding traumatic intracerebral contusion/hematoma. Neurol. India 2006, 54, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Oertel, M.; Kelly, D.F.; McArthur, D.; Boscardin, W.J.; Glenn, T.C.; Lee, J.H.; Gravori, T.; Obukhov, D.; McBride, D.Q.; Martin, N.A. Progressive hemorrhage after head trauma: Predictors and consequences of the evolving injury. J. Neurosurg. 2002, 96, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Allison, R.Z.; Nakagawa, K.; Hayashi, M.; Donovan, D.J.; Koenig, M.A. Derivation of a Predictive Score for Hemorrhagic Progression of Cerebral Contusions in Moderate and Severe Traumatic Brain Injury. Neurocrit. Care 2017, 26, 80–86. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Elderly (n = 279) | Young Adults (n = 165) | p |
|---|---|---|---|
| Age (years) | 77.5 ± 7.7 | 49.3 ± 11.2 | <0.001 |
| Gender | <0.001 | ||
| Male, n (%) | 149(53.4) | 137(83.0) | |
| Female, n (%) | 130(46.6) | 28(17.0) | |
| Comorbidities | |||
| DM, n (%) | 91(32.6) | 29(17.6) | 0.001 |
| HTN, n (%) | 180(64.5) | 42(25.5) | <0.001 |
| CAD, n (%) | 31(11.1) | 8(4.8) | 0.024 |
| CHF, n (%) | 4(1.4) | 2(1.2) | 0.845 |
| CVA, n (%) | 45(16.1) | 6(3.6) | <0.001 |
| ESRD, n (%) | 26(9.3) | 5(3.0) | 0.012 |
| GCS (median, IQR) | 15(11–15) | 14(8–15) | 0.079 |
| 1–8 | 54(19.4) | 45(27.3) | 0.053 |
| 9–12 | 36(12.9) | 19(11.5) | 0.668 |
| 13–15 | 189(67.7) | 101(61.2) | 0.162 |
| Coagulopathy, n (%) | 20(7.2) | 13(7.9) | 0.852 |
| ISS (median, IQR) | 16(16–20) | 16(16–24) | 0.434 |
| Hematoma volume (mL) | 39.0 ± 35.7 | 34.7 ± 30.8 | 0.199 |
| Surgery, n (%) | 69(24.7) | 55(33.3) | 0.063 |
| Reoperation, n (%) | 19(6.8) | 16(9.7) | 0.362 |
| LOS in hospital (days) | 12.4 ± 13.0 | 13.7 ± 13.5 | 0.321 |
| ICU, n (%) | 228(81.7) | 129(78.2) | 0.364 |
| Mortality, n (%) | 49(17.6) | 19(11.5) | 0.087 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Gender (male) | 0.9(0.55–1.61) | 0.825 | — | — |
| Comorbidities | ||||
| DM | 0.8(0.44–1.47) | 0.481 | — | — |
| HTN | 0.7(0.42–1.19) | 0.189 | — | — |
| CAD | 2.4(1.13–5.09) | 0.023 | 3.2(1.09–9.69) | 0.035 |
| CHF | — | 0.999 | — | — |
| CVA | 0.6(0.22–1.49) | 0.251 | — | — |
| ESRD | 2.9(1.31–6.50) | 0.009 | 4.6(1.48–14.13) | 0.008 |
| Not an isolated SDH | 1.1(0.65–1.85) | 0.735 | — | |
| Hematoma volume (mL) | 1.4(1.26–1.49) | <0.001 | 1.2(1.11–1.36) | <0.001 |
| ISS | 1.4(1.31–1.52) | <0.001 | 1.3(1.23–1.46) | <0.001 |
| Coagulopathy | 5.6(2.68–11.84) | <0.001 | 4.0(1.47–11.05) | 0.007 |
| Surgery | 1.2(0.68–2.08) | 0.555 | — | |
| Reoperation | 0.9(0.34–2.45) | 0.860 | — | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, C.-H.; Rau, C.-S.; Wu, S.-C.; Liu, H.-T.; Huang, C.-Y.; Hsu, S.-Y.; Hsieh, H.-Y. Risk Factors Contributing to Higher Mortality Rates in Elderly Patients with Acute Traumatic Subdural Hematoma Sustained in a Fall: A Cross-Sectional Analysis Using Registered Trauma Data. Int. J. Environ. Res. Public Health 2018, 15, 2426. https://doi.org/10.3390/ijerph15112426
Hsieh C-H, Rau C-S, Wu S-C, Liu H-T, Huang C-Y, Hsu S-Y, Hsieh H-Y. Risk Factors Contributing to Higher Mortality Rates in Elderly Patients with Acute Traumatic Subdural Hematoma Sustained in a Fall: A Cross-Sectional Analysis Using Registered Trauma Data. International Journal of Environmental Research and Public Health. 2018; 15(11):2426. https://doi.org/10.3390/ijerph15112426
Chicago/Turabian StyleHsieh, Ching-Hua, Cheng-Shyuan Rau, Shao-Chun Wu, Hang-Tsung Liu, Chun-Ying Huang, Shiun-Yuan Hsu, and Hsiao-Yun Hsieh. 2018. "Risk Factors Contributing to Higher Mortality Rates in Elderly Patients with Acute Traumatic Subdural Hematoma Sustained in a Fall: A Cross-Sectional Analysis Using Registered Trauma Data" International Journal of Environmental Research and Public Health 15, no. 11: 2426. https://doi.org/10.3390/ijerph15112426
APA StyleHsieh, C.-H., Rau, C.-S., Wu, S.-C., Liu, H.-T., Huang, C.-Y., Hsu, S.-Y., & Hsieh, H.-Y. (2018). Risk Factors Contributing to Higher Mortality Rates in Elderly Patients with Acute Traumatic Subdural Hematoma Sustained in a Fall: A Cross-Sectional Analysis Using Registered Trauma Data. International Journal of Environmental Research and Public Health, 15(11), 2426. https://doi.org/10.3390/ijerph15112426