Correlates of Sedentary Behaviour in Adults with Intellectual Disabilities—A Systematic Review

 , , , ,
, , , ,  ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection of Studies
- (a)
- Study sample with participants with ID.
- (b)
- Study sample with participants aged ≥18 years. For studies that also included individuals under 18 years, at least 80% of the total sample had to be ≥18 years.
- (c)
- In study samples with mixed developmental disabilities and data only presented for the sample as a whole, at least 50% of the sample had to have an ID. Studies were excluded if they did not report the proportion of participants with ID.
- (d)
- Sedentary behaviour was measured with objective and/or subjective methods.
- (e)
- Correlates of sedentary behaviour are reported.
- (f)
- Studies are published in English.
- (g)
- Studies are published after 1 January 1990.
- (a)
- It was a conference abstract.
- (b)
- It was a lab-based study e.g., to calibrate accelerometer cut-offs.
- (c)
- The term sedentary was used to describe a lack of physical activity e.g., <5000 steps per day.
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
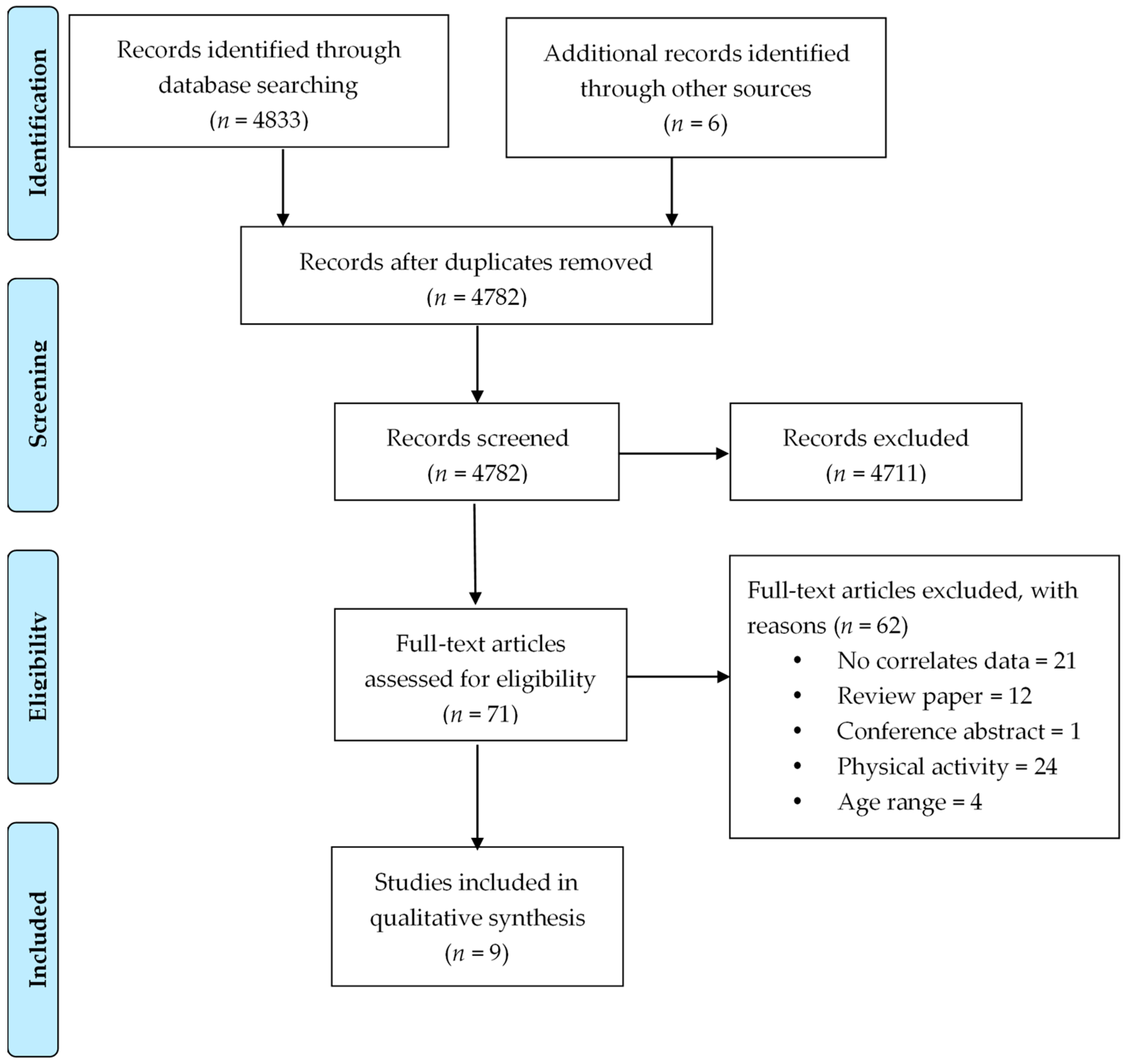
3. Results
3.1. Study Characteristics
3.2. Correlates of Sedentary Behaviour
3.3. Individual Correlates
3.4. Physical, Biological and Genetic Factors
3.5. Interpersonal and Environmental Correlates
4. Discussion
5. Strengths and Limitations
6. Future Research
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Owen, N.; Sugiyama, T.; Eakin, E.E.; Gardiner, P.A.; Tremblay, M.S.; Sallis, J.F. Adults’ sedentary behavior determinants and interventions. Am. J. Prev. Med. 2011, 41, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Loyen, A.; Verloigne, M.; Van Hecke, L.; Hendriksen, I.; Lakerveld, J.; Steene-Johannessen, J.; Koster, A.; Donnelly, A.; Ekelund, U.; Deforche, B.; et al. Variation in population levels of sedentary time in European adults according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act 2016, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Milton, K.; Gale, J.; Stamatakis, E.; Bauman, A. Trends in prolonged sitting time among European adults: 27 country analysis. Prev. Med. 2015, 77, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Participants, S.T.C.P. Sedentary behavior research network (SBRN)—Terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Vallance, J.K.; Winkler, E.A.; Gardiner, P.A.; Healy, G.N.; Lynch, B.M.; Owen, N. Associations of objectively-assessed physical activity and sedentary time with depression: NHANES (2005–2006). Prev. Med. 2011, 53, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- American Association on Intellectual and Developmental Disabilities. Definiton of Intellectual Disability. Available online: http://aaidd.org/intellectual-disability/definition (accessed on 12 July 2018).
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Polder, J.J.; Meerding, W.J.; Bonneux, L.; van der Maas, P.J. Healthcare costs of intellectual disability in the netherlands: A cost-of-illness perspective. J. Intellect. Disabil. Res. 2002, 46, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Honeycutt, A.; Dunlap, L.; Chen, H.; Al Homsi, G.; Schendel, D. Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment—United States, 2003. MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 57–59. [Google Scholar]
- Melville, C.A.; Oppewal, A.; Schafer Elinder, L.; Freiberger, E.; Guerra-Balic, M.; Hilgenkamp, T.I.M.; Einarsson, I.; Izquierdo-Gomez, R.H.; Sansano-Nadal, O.; Rintala, P.; et al. Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual disabilities—A systematic review. Prev. Med. 2017, 97, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Evenhuis, H.M.; Hermans, H.; Hilgenkamp, T.I.; Bastiaanse, L.P.; Echteld, M.A. Frailty and disability in older adults with intellectual disabilities: Results from the healthy ageing and intellectual disability study. J. Am. Geriatr. Soc. 2012, 60, 934–938. [Google Scholar] [CrossRef] [PubMed]
- de Winter, C.F.; Bastiaanse, L.P.; Hilgenkamp, T.I.; Evenhuis, H.M.; Echteld, M.A. Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: Results of the ha-id study. Res. Dev. Disabil. 2012, 33, 1722–1731. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- O’Donoghue, G.; Perchoux, C.; Mensah, K.; Lakerveld, J.; van der Ploeg, H.; Bernaards, C.; Chastin, S.F.; Simon, C.; O’Gorman, D.; Nazare, J.A.; et al. A systematic review of correlates of sedentary behaviour in adults aged 18-65 years: A socio-ecological approach. BMC Public Health 2016, 16, 163. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Buck, C.; Freiberger, E.; Murphy, M.; Brug, J.; Cardon, G.; O’Donoghue, G.; Pigeot, I.; Oppert, J.M.; Consortium, D. Systematic literature review of determinants of sedentary behaviour in older adults: A dedipac study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, K.; Yoon, U.; Vogt, P.M. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Craniomaxillofac. Surg. 2011, 39, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, J.; Turner, A.; Granat, M.H. Measuring the actual levels and patterns of physical activity/inactivity of adults with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2011, 24, 508–517. [Google Scholar] [CrossRef]
- Hsieh, K.; Rimmer, J.H.; Heller, T. Obesity and associated factors in adults with intellectual disability. J. Intellect. Disabil. Res. 2014, 58, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Mikulovic, J.; Dieu, O.; Fardy, P.S.; Bui-Xuan, G.; Vanhelst, J. Influence of sleep timing behavior on weight status and activity patterns in adults with intellectual disabilities. Res. Dev. Disabil. 2014, 35, 3254–3259. [Google Scholar] [CrossRef] [PubMed]
- Mikulovic, J.; Vanhelst, J.; Salleron, J.; Marcellini, A.; Compte, R.; Fardy, P.S.; Bui-Xuan, G. Overweight in intellectually-disabled population: Physical, behavioral and psychological characteristics. Res. Dev. Disabil. 2014, 35, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, M.; Hansen, B.H.; Paus, B.; Kolset, S.O. Accelerometer-determined physical activity and walking capacity in persons with down syndrome, williams syndrome and prader-willi syndrome. Res. Dev. Disabil. 2013, 34, 4395–4403. [Google Scholar] [CrossRef] [PubMed]
- Oviedo, G.R.; Travier, N.; Guerra-Balic, M. Sedentary and physical activity patterns in adults with intellectual disability. Int. J. Environ. Res. Public Health 2017, 14, 1027. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.; Hilgenkamp, T.I.M.; Murthy, S.; Heller, T.; Rimmer, J.H. Low levels of physical activity and sedentary behavior in adults with intellectual disabilities. Int. J. Environ. Res. Public Health 2017, 14, 1503. [Google Scholar] [CrossRef] [PubMed]
- Melville, C.A.; McGarty, A.; Harris, L.; Hughes-McCormack, L.; Baltzer, M.; McArthur, L.A.; Morrison, J.; Allan, L.; Cooper, S.A. A population-based, cross-sectional study of the prevalence and correlates of sedentary behaviour of adults with intellectual disabilities. J. Intellect. Disabil. Res. 2018, 62, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; McGarty, A.M.; Hilgenkamp, T.; Mitchell, F.; Melville, C.A. Correlates of objectively measured sedentary time in adults with intellectual disabilities. Prev. Med. Rep. 2018, 9, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004. [Google Scholar]
- Einarsson, I.O.; Olafsson, A.; Hinriksdottir, G.; Johannsson, E.; Daly, D.; Arngrimsson, S.A. Differences in physical activity among youth with and without intellectual disability. Med. Sci. Sports Exerc. 2015, 47, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Lobenius-Palmer, K.; Sjoqvist, B.; Hurtig-Wennlof, A.; Lundqvist, L.O. Accelerometer-assessed physical activity and sedentary time in youth with disabilities. Adapt. Phys. Activ. Q. 2017, 35, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Hancox, R.J.; Milne, B.J.; Poulton, R. Association between child and adolescent television viewing and adult health: A longitudinal birth cohort study. Lancet 2004, 364, 257–262. [Google Scholar] [CrossRef]
- Malina, R.M. Physical activity and fitness: Pathways from childhood to adulthood. Am. J. Hum. Biol. 2001, 13, 162–172. [Google Scholar] [CrossRef]
- Harris, L.; Melville, C.; Murray, H.; Hankey, C. The effects of multi-component weight management interventions on weight loss in adults with intellectual disabilities and obesity: A systematic review and meta-analysis of randomised controlled trials. Res. Dev. Disabil. 2018, 72, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.A.; Foley, J.T.; Lloyd, M. Body mass index of adults with intellectual disability participating in special olympics by world region. J. Intellect. Disabil. Res. 2014, 58, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Sparling, P.B.; Howard, B.J.; Dunstan, D.W.; Owen, N. Recommendations for physical activity in older adults. BMJ 2015, 350, h100. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.D.I.; Brosnan, B.J.; Chu, A.K.Y.; Skeaff, C.M.; Rehrer, N.J.; Perry, T.L.; Peddie, M.C. Sedentary behavior and body weight and composition in adults: A systematic review and meta-analysis of prospective studies. Sports Med. 2018, 48, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, J.; Jackson, A.; Cooper, S.; Morrison, J.; Melville, C.; Smiley, E.; Allan, L.; Mantry, D. Understanding predictors of low physical activity in adults with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2009, 22, 236–247. [Google Scholar] [CrossRef]
- Bruhn, K.; Kronisch, S.; Waltz, S.; Stephani, U. Screen sensitivity in photosensitive children and adolescents: Patient-dependant and stimulus-dependant factors. Epileptic Disord. 2007, 9, 57–64. [Google Scholar] [PubMed]
- Dairo, Y.M.; Collett, J.; Dawes, H.; Oskrochi, G.R. Physical activity levels in adults with intellectual disabilities: A systematic review. Prev. Med. Rep. 2016, 4, 209–219. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Setting and Target Population | Study Design | Study Aim | Participants | Sedentary Behaviour Measure: Outcome | Potential Correlates Investigated | Quality Score (0–1.0) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Mean Age (SD a, Range) | Sex (% F b) | Level of ID c | Causes of ID | |||||||
| Finlayson et al. (2011) [20] | Scotland, adults with mild-moderate ID, living in the community | cross sectional, convenience sample | Collect pilot data on habitual physical activity and inactivity, and compare activity monitor data with self-report data | n = 62 | 37.1 (12.8, 18–66) | 56.5% | N/A | 9.7% DS d | Total sedentary time by AcvtivPal (sedentary cut-off N/A): 18.71 h/day (SD 1.88, range 14.88–22.19) | Sex | 0.82 |
| Hsieh et al. (2014) [21] | USA, adults with all levels of ID, known to specialist organisations | cross sectional, population-based sample | Examine the relationship between nonmodifiable and modifiable risk factors and obesity | n = 1619 | 37.1 (14.1, 18–86) | 44.8% | 13.3% borderline, 31.6% mild, 23.7% moderate, 8.6% severe/profound, 22.8% unknown | 24.9% DS | Hours of TV e watching (Proxy rater question): Mean sedentary time not reported | Weight status | 0.95 |
| Mikulovic et al. (2014) [22] | France, adults with ID, living in institutions | cross sectional, administrative sample | Explore the relationship between sleep habits and overweight/obesity, physical activity and sedentary behaviour | n = 691 | 38.1 (10.3, 19–59) | 41% | N/A | N/A | Total hours TV and computer/week (Questionnaire adapted from French Federation Adapted Sports-proxy rater): group 1 20.25 (SD 12.25), group 2 17.75 (SD 12.76), group 3 23.82 (SD 14.89), group 4 27.20 (SD 17.46) | Sleep habits | 1.0 |
| Mikulovic et al. (2014) [23] | France, adults with ID, living in institutions | cross sectional, administrative sample | Asess the prevalence of overweight/obesity, and lifestyle, food habits, physical activities and self-awareness about body and health, and assess associations with overweigh/obesity | n = 691 | N/A | N/A | N/A | N/A | Total hours TV and computer/week (Questionnaire adapted from French Federation Adapted Sports-proxy rater): 18 (12–28) | Weight status | 1.0 |
| Nordstrom et al. (2013) [24] | Norway, adults with DS, WS f and PWS g living all over Norway | cross sectional, convenience sample | Describe levels of physical activity and sedentary behaviour, and study physical activity and walking capacity in relation to BMI | n = 96 | 28.5 (7.5) | 62.1% | N/A | 41.7% DS, 29.2% WS, 29.3% PWS | Total sedentary time by ActiGraph GT3X+ accelerometer (sedentary cut-off < 100 cpm): 522 min/day (SD 80.3) | Sex, genetic syndrome (DS, WS and PWS), BMI h, living situation (supported community setting vs with parents) | 0.90 |
| Oviedo et al. (2017) [25] | Spain, adults with ID | cross sectional, convenience sample | Assess the temporal patterning of sedentary behaviour and physical activity levels throughout the week, and analyze age and sex differences | n = 92 | 45.0 (12) | 41.7% | 32.6% mild, 37.0% moderate, 30.4% severe | 14.1% DS, 2.2% West syndrome, 2.2% Cerebral Palsy, 2.2% Cornelia Lange syndrome, 1.1% microcephaly | Total sedentary time by ActiGraph GT3X+ accelerometer (sedentary cut-off < 100 cpm): 612.9 min/day (SD 80.1) | Age, sex, center time, BMI | 0.64 |
| Hsieh et al. (2017) [26] | USA, adults with all levels of ID, known to specialist organisations | cross sectional, population- based sample | Assess the prevalence of low levels of physical activity and sedentary behaviour, and identify associated factors | n = 1619 | 37.7 (14.4, 18–86) | 44.8% | 12.4% borderline, 52.4% mild or moderate, 8.2% severe/profound, 27% unknown | 25% DS, 12.2% autism, 12.7% cerebral palsy | Hours of TV watching (Proxy rater question): 3.42 (SD 2.13) | Age, sex, ethnicity, level of ID, ID-related conditions, general health status, days with activity limitation, chronic health conditions, obesity, depression, psychotropic medication use, epilepsy/seizure disorder, urinary incontinence, falls, mobility limitations, day/educational program or employment participation, residential type, social participation, special Olympics participation, low levels of PA | 1.0 |
| Melville et al. (2018) [27] | Scotland, adults with ID living in community | cross sectional, population- based sample | Assess the prevalence and correlates of screen time | n = 727 | 43.6 (NA, 18–90) | 45% | mild 35.6%, moderate 26.5%, severe 17.9%, profound 20.0% | 13.4% DS | Hours of screen time = watching TV, DVDs, videos or on the PC (C21st Health Check questionnaire- self and proxy report): 8.6% none, 2.8% 1–3 h/month, 14.3% <2 h/day, 23.3% 2–3 h/day, 28.1% 4–5 h/day, 22.8% 6 h/day | Sex, age, accommodation type, neighbourhood deprivation category, level of ID, Down syndrome, obesity, hearing impairment, visual impairment, mobility problems, mental ill health, problem behaviours, meets PA recommendation | 1.0 |
| Harris et al. (2018) [28] | Scotland, adults with ID living in the community | Secondary analysis of baseline data from two RCTs i | Study correlates of objectively measured sedentary behaviour | n = 152 | Mean age = N/A; 38.6% < 45 years, 61.4% ≥ 45 years | 51.7% | 48.3% mild, 35.7% moderate, 12.6% severe, 2.8% profound | N/A | Total sedentary time by ActiGraph GT3X+ accelerometer sedentary cut-off < 100 cpm): median 467.5 min/day (IQR j 411.0–542.2) | Age, sex, level of ID, physical health problems, mental health problems, problem behaviours obesity, accommodation type, neighbourhood deprivation | 1.0 |
| Level | Category | Correlate | Association with SB a (Direction of Association) | No Association with SB |
|---|---|---|---|---|
| Individual | Physical, biological and genetic | Age | Oviedo et al., 2017 [25]; Hsieh et al., 2017 [26]; Harris et al., 2018 [28]; Melville et al., 2018 [27] | |
| Sex | Finlayson et al., 2011 [20] (women more sedentary); Hsieh et al., 2017 [26] (men more sedentary); Melville et al., 2018 [27] (men more sedentary) | Oviedo et al., 2017 [25]; Harris et al., 2018 [28] | ||
| Ethnicity | Hsieh et al., 2017 [26] | |||
| Genetic syndromes | Nordstrom et al., 2013 [24] (DS b −) | Hsieh et al., 2017 [26]; Melville et al., 2018 [27] | ||
| Weight status | Nordstrom et al., 2013 [24] (−); Oviedo et al., 2017 (+) [25]; Hsieh et al., 2017 [26] (+); Melville et al., 2018 [27] (+) | Mikulovic et al., 2014 [23] Harris et al., 2018 [28] Hsieh et al., 2014 [21] | ||
| Epilepsy | Hsieh et al., 2017 [26] (−); Melville et al., 2018 [27] (−) | |||
| Physical health | Harris et al., 2018 [28] (+) | Hsieh et al., 2017 [26] | ||
| Psychotropic medication use | Hsieh et al., 2017 [26] | |||
| Urinary incontinence | Hsieh et al., 2017 [26] | |||
| Sleep habits | Mikulovic et al., 2014 [22] (+) | |||
| Mobility | Melville et al., 2018 [27] (+) | Hsieh et al., 2017 [26] | ||
| Visual impairment | Melville et al., 2018 [27] | |||
| Hearing impairment | Melville et al., 2018 [27] (−) | |||
| Falls | Hsieh et al., 2017 [26] | |||
| Level of ID c | Hsieh et al., 2017 [26] (−); Melville et al., 2018 [27] (−) | Harris et al., 2018 [28] | ||
| Mental health | Harris et al., 2018 [28] (+) | Hsieh et al., 2017 [26]; Melville et al., 2018 [27] | ||
| Problem behaviours | Harris et al., 2018 [28]; Melville et al., 2018 [27] | |||
| Functional limitation in past 30 days | Hsieh et al., 2017 [26] | |||
| Behavioural | Physical activity | Hsieh et al., 2017 [26]; Melville et al., 2018 [27] | ||
| Special Olympics participation | Hsieh et al., 2017 [26] | |||
| Socioeconomic status | Deprivation category | Harris et al., 2018 [28]; Melville et al., 2018 [27] | ||
| Employment | Hsieh et al., 2017 [26] | |||
| Interpersonal | Living arrangements | Hsieh et al., 2017 [26] (family home +; foster home −) | Nordstrom et al., 2013 [24]; Harris et al., 2018 [28]; Melville et al., 2018 [27] | |
| Social participation | Hsieh et al., 2017 [26] | |||
| Environmental | Residential location (urban/rural) | Hsieh et al., 2017 [26] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oppewal, A.; Hilgenkamp, T.I.M.; Schäfer Elinder, L.; Freiberger, E.; Rintala, P.; Guerra-Balic, M.; Giné-Garriga, M.; Cuesta-Vargas, A.; Oviedo, G.R.; Sansano-Nadal, O.; et al. Correlates of Sedentary Behaviour in Adults with Intellectual Disabilities—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2274. https://doi.org/10.3390/ijerph15102274
Oppewal A, Hilgenkamp TIM, Schäfer Elinder L, Freiberger E, Rintala P, Guerra-Balic M, Giné-Garriga M, Cuesta-Vargas A, Oviedo GR, Sansano-Nadal O, et al. Correlates of Sedentary Behaviour in Adults with Intellectual Disabilities—A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(10):2274. https://doi.org/10.3390/ijerph15102274
Chicago/Turabian StyleOppewal, Alyt, Thessa I. M. Hilgenkamp, Liselotte Schäfer Elinder, Ellen Freiberger, Pauli Rintala, Myriam Guerra-Balic, Maria Giné-Garriga, Antonio Cuesta-Vargas, Guillermo R. Oviedo, Oriol Sansano-Nadal, and et al. 2018. "Correlates of Sedentary Behaviour in Adults with Intellectual Disabilities—A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 10: 2274. https://doi.org/10.3390/ijerph15102274
APA StyleOppewal, A., Hilgenkamp, T. I. M., Schäfer Elinder, L., Freiberger, E., Rintala, P., Guerra-Balic, M., Giné-Garriga, M., Cuesta-Vargas, A., Oviedo, G. R., Sansano-Nadal, O., Izquierdo-Gómez, R., Einarsson, I., Teittinen, A., & Melville, C. A. (2018). Correlates of Sedentary Behaviour in Adults with Intellectual Disabilities—A Systematic Review. International Journal of Environmental Research and Public Health, 15(10), 2274. https://doi.org/10.3390/ijerph15102274