Prediction and Decomposition of Efficiency Differences in Chinese Provincial Community Health Services




Abstract
1. Introduction
2. Method and Data
2.1. Super-SBM DEA Model
2.2. GM (1,1) Grey Prediction Model
- Step 1: Given an original sequence as follows:where, is the value for the time period i (i = 1, 2, …, n).
- Step 2: A new sequence x(1) can be generated by a one-time accumulated generating operation 1-AGO) based on the original sequence x(0), which is:where, .
- Step 3: A first-order differential equation with one variable is expressed as follows:where, a, b are the developing coefficient and the grey input coefficient, respectively. These two coefficients can be determined by the least squares method as follows:where:and:
2.3. Theil Index Decomposition Method
2.4. Data
- (1)
- Input indicators included: the number of community health service centers (stations), the number of community health care technical workers, and the number of community health service beds in each region.
- (2)
- Output indicators include: the number of community health service diagnosed and treated visits, the number of community health services inpatients, as well as the bed utilization ratio of community health services in each area.
3. Results and Discussion
3.1. Measurement of Chinese Provincial Community Health Service Efficiency
3.2. Measurement and Prediction of Efficiency Differences of Chinese Provincial Health Care Services
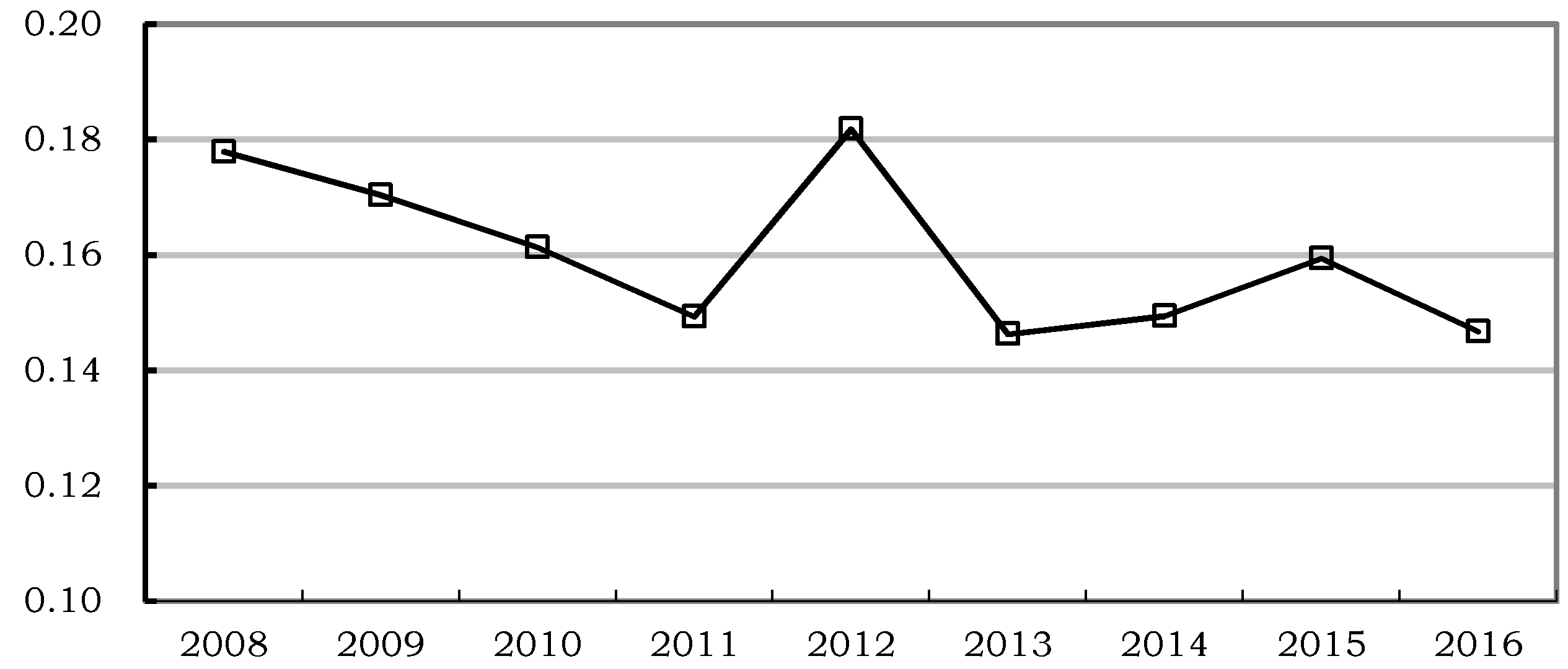
3.2.1. Measurement of Efficiency Differences of Chinese Provincial Health Service
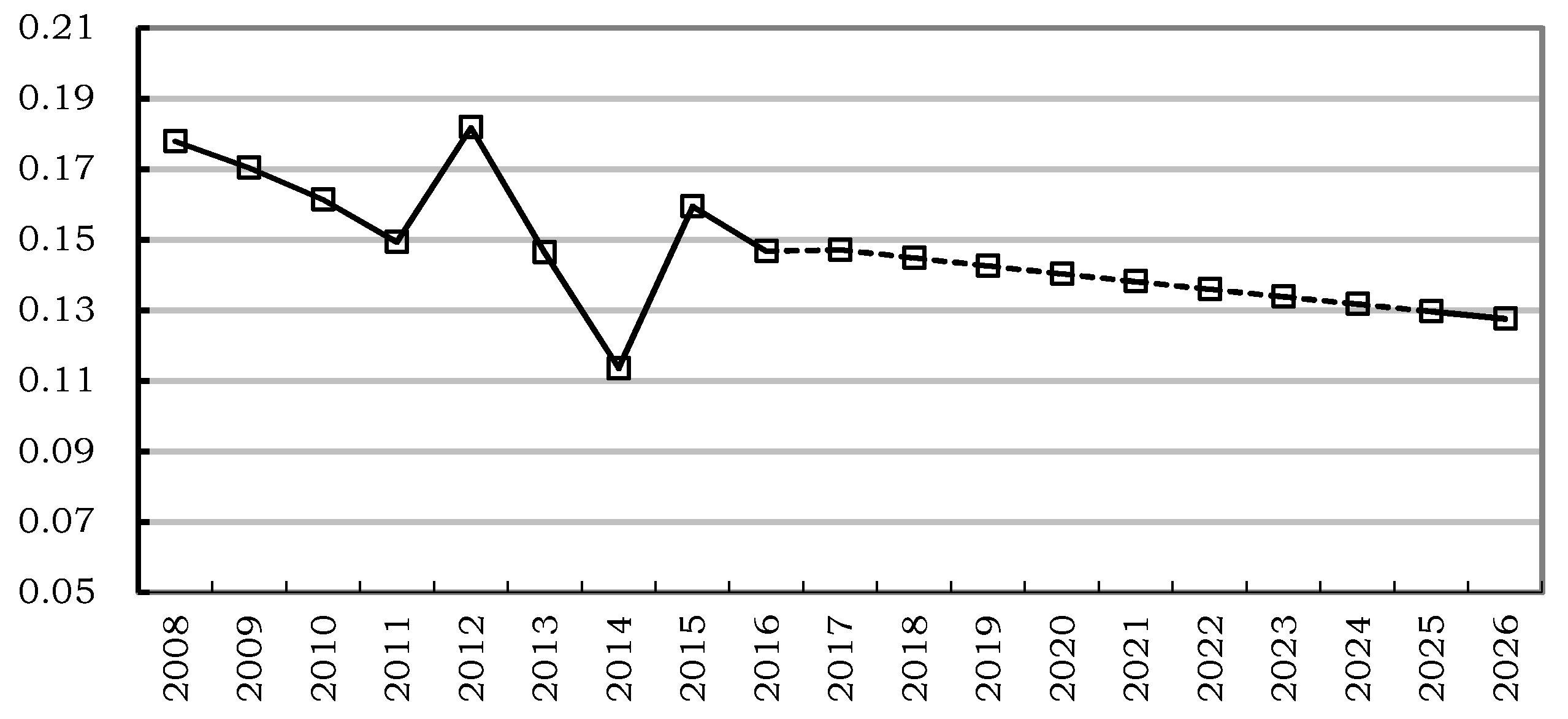
3.2.2. Prediction of Efficiency Difference of Chinese Provincial Health Service
3.3. Decomposition of the Efficiency Differences in Chinese Provincial Health Services
- (1)
- In the provincial efficiency differences of Chinese community health services, the intra-regional efficiency differences become the most important source for overall efficiency differences, and inter-regional efficiency differences among the eastern, central, and western region becomes the secondary source. In 2008, the contribution of intra-regional efficiency differences to the overall difference was 79.5%, and the contribution of inter-regional efficiency differences to the overall difference was 20.5%. Then, the contribution of intra-regional efficiency differences increased with fluctuations. In 2016, the contribution of intra-regional efficiency differences increased to 98.4%, and the contribution of inter-regional efficiency differences declined to only 1.6%.
- (2)
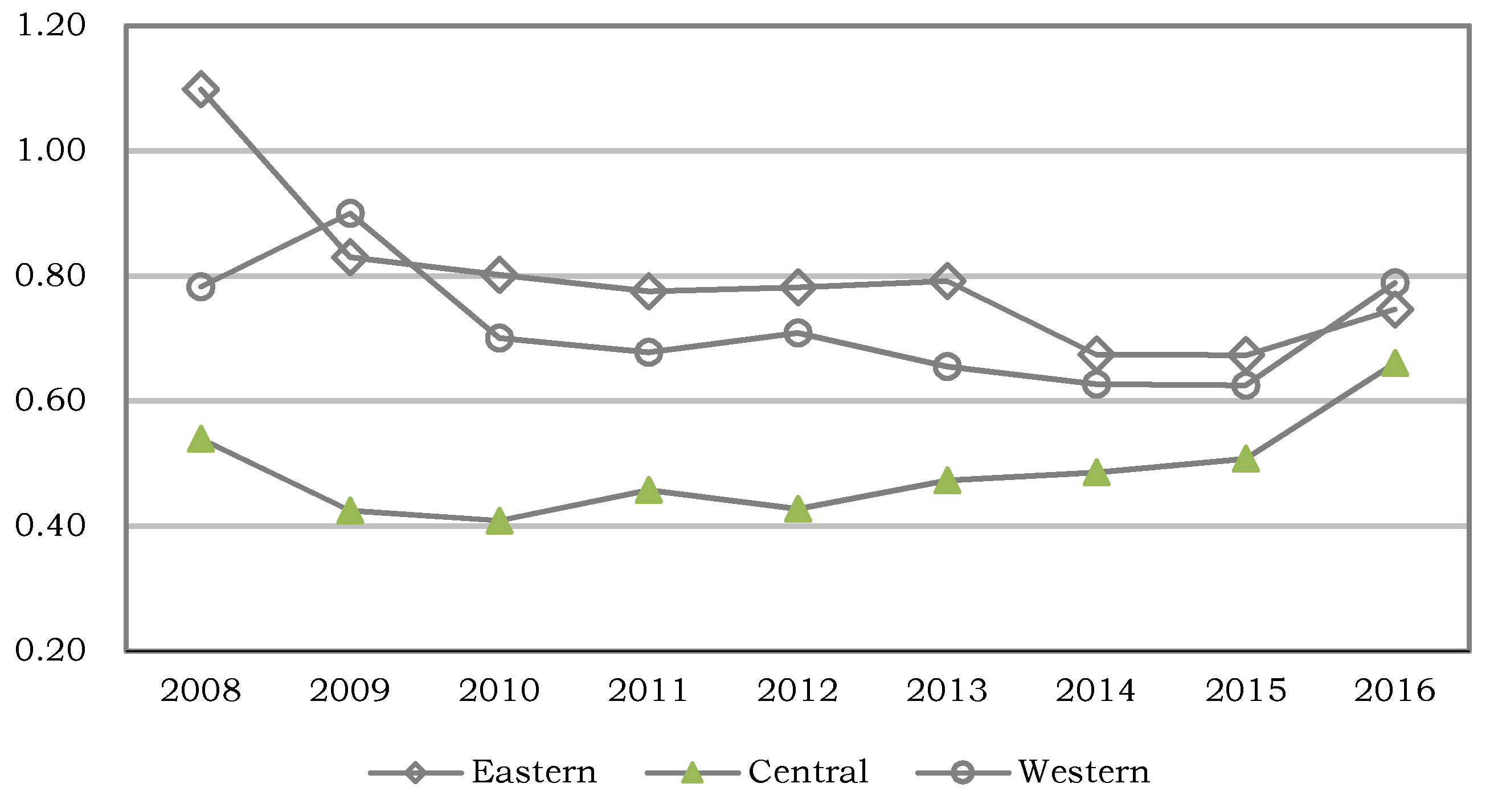
- The changing trends of contributions of intra-regional efficiency differences vary tremendously. The contribution of intra-regional efficiency differences of the eastern region declined from 51.6% in 2008 to 39.3% in 2016, which was the highest among all the regions, except for 2012. The contribution of the intra-regional efficiency differences of the western region increased from 22.6% in 2008 to 36.7% in 2016, which was the second highest among the three regions. The contribution of the intra-regional efficiency differences of the central region increased from 5.3% in 2008 to 22.4% in 2016, which was the lowest among the regions.
4. Conclusions
- (1)
- There was a fluctuating trend in the average provincial efficiency of the community health service from 2008 to 2016. The community health services in a considerable number of provinces were inefficient.
- (2)
- There were apparent provincial differences in the efficiency of Chinese community health services. The provincial differences of efficiency of Chinese community health services from 2016 to 2008 reflected by the Theil index declined at a relatively slow pace with fluctuations. Overall, although the regional gap of efficiency of the Chinese community health service declined in recent years, the gap is still apparent and it needs to be narrowed.
- (3)
- In the provincial efficiency differences of Chinese community health services, the intra-regional efficiency difference is the most important source for the overall efficiency difference, which explains the overall difference to a large extent. The inter-regional efficiency difference among the eastern, central, and western regions was the secondary source, although it should not be ignored.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chernew, M.E.; Newhouse, J.P. Health care spending growth. In Handbook of Health Economics; Pauly, M.V., McGuire, T.G., Barros, P.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Hadad, S.; Hadad, Y.; Simon-Tuval, T. Determinants of healthcare system’s efficiency in OECD countries. Eur. J. Health Econ. 2013, 14, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Lahelma, E.; Martikainen, P.; Laaksonen, M.; Aittomäki, A. Pathways between socioeconomic determinants of health. J. Epidemiol. Community Health 2004, 58, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Spinks, J.; Hollingsworth, B. Cross-country comparisons of technical efficiency of health production: A demonstration of pitfalls. Appl. Econ. 2009, 41, 417–427. [Google Scholar] [CrossRef]
- Seiford, L.M. Data envelopment analysis: The evolution of the state of the art (1978–1995). J. Prod. Anal. 1996, 7, 99–138. [Google Scholar] [CrossRef]
- Gattoufi, S.; Oral, M.; Reisman, A. Data envelopment analysis literature: A bibliography update. Socio-Econ. Plan. Sci. 2004, 38, 159–229. [Google Scholar] [CrossRef]
- Kazley, A.S.; Ozcan, Y.A. Electronic medical record use and efficiency: A DEA and windows analysis of hospitals. Socio-Econ. Plan. Sci. 2009, 43, 209–216. [Google Scholar] [CrossRef]
- Liu, J.S.; Lu, Y.Y.; Lu, W.M. Research fronts in data envelopment analysis. Omega 2016, 58, 33–45. [Google Scholar] [CrossRef]
- Jia, T.; Yuan, H. The application of DEA (data envelopment analysis) window analysis in the assessment of influence on operational efficiencies after the establishment of branched hospitals. BMC Health Serv. Res. 2017, 17, 265. [Google Scholar] [CrossRef] [PubMed]
- Sapienza, F.; Matranga, D. Evaluating the Reform of the Healthcare System in Sicily, variations of efficiency and appropriateness between 2008 and 2010. Epidemiol. Biostat. Public Health 2018, 15, 125931–1259310. [Google Scholar]
- Stefko, R.; Gavurova, B.; Kocisova, K. Healthcare efficiency assessment using DEA analysis in the Slovak Republic. Health Econ. Rev. 2018, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Halkos, G.E.; Tzeremes, N.G. A conditional nonparametric analysis for measuring the efficiency of regional public healthcare delivery: An application to Greek prefectures. Health Policy 2011, 103, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, T.; Huang, S. Analysis on the Operation Efficiency of Community Health Service System Based on Ultra-efficient DEA Model in Hunan Province. Chin. Health Econ. 2013, 32, 74–77. [Google Scholar]
- Zhang, C.; Liu, H. Research on Input-output Technical Efficiency Evaluation of China’s Regional Health Economy System. Chin. Health Econ 2009, 28, 11–13. [Google Scholar]
- Luo, L.; Hu, M. An Analysis on the Productive Efficiency of China’s Regional Health and Care Services. Stat. Inf. Forum 2008, 23, 47–51. [Google Scholar]
- Guo, Q.; Wang, X.; Wang, S.; Ma, H.; Li, X.; Xu, L. Main problems and countermeasures of resource allocation in community health service. Chin. Health Serv. Manag. 2006, 23, 317–319. [Google Scholar]
- Zhang, X.; Zhou, Y.; Fang, P. Comparative analysis of resource allocation in Chinese health service center. Chin. Health Econ. 2008, 27, 29–32. [Google Scholar]
- Zhang, Y.; Tang, G.; Wang, W.; Liu, L.; Zhao, Z.; Guo, B.; Wu, Y.; Yi, D. Application of Gini Coefficient and Theil Index in Study on Equity of Health Resources Distribution. Chin. J. Health Stat. 2008, 25, 243–246. [Google Scholar]
- Jin, Q.; Lu, Y.; Feng, Y.; Xu, C. Analysis on the Equity of Health Resource Configuration in Hangzhou. Zhejiang J. Prev. Med. 2012, 24, 4–7. [Google Scholar]
- He, M.; Wang, L.; He, J.; Wei, Y. Studying on the status and equity of health services resources allocation in China. Chin. Health Serv. Manag. 2013, 30, 197–199. [Google Scholar]
- Hollingsworth, B. Non-Parametric and Parametric Applications Measuring Efficiency in Health Care. Health Care Manag. Sci. 2003, 6, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Charnes, A.; Cooper, W.; Rhodes, E. Measuring the efficiency of decision making units. Eur. J. Oper. Res. 1978, 2, 429–444. [Google Scholar] [CrossRef]
- Hollingsworth, B. The Measurement of Efficiency and Productivity of Health Care Delivery. Health Econ. 2008, 17, 1107–1128. [Google Scholar] [CrossRef] [PubMed]
- Worthington, A.C. Frontier Efficiency Measurement in Health Care, A Review of Empirical Techniques and Selected Applications. Med. Care Res. Rev. 2004, 61, 35–70. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, L.; Rauner, M.; Heidenberger, K.; Kraus, M. A Cross-National Comparison and Taxonomy of DEA-Based Hospital Efficiency Studies. Socio-Econ. Plan. Sci. 2008, 42, 158–189. [Google Scholar] [CrossRef]
- Kontodimopoulos, N.; Nanos, P.; Niakas, D. Balancing efficiency of health services and equity of access in remote areas in Greece. Health Policy 2006, 76, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Nedelea, I.C.; Fannin, J.M. Analyzing cost efficiency of critical access hospitals. J. Policy Model. 2013, 35, 183–195. [Google Scholar] [CrossRef]
- Hernandez, A.R.; Sebastián, M.S. Assessing the technical efficiency of health posts in rural Guatemala: A data envelopment analysis. Glob. Health Action 2014, 7, 23190. [Google Scholar] [CrossRef] [PubMed]
- Czypionka, T.; Kraus, M.; Mayer, S.; Röhrling, G. Efficiency, ownership, and financing of hospitals, the case of Austria. Health Care Manag. Sci. 2014, 17, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Cai, M.; Tao, H.; He, Z.; Lin, X.; Lin, H.; Zuo, Y. Efficiency and productivity measurement of rural township hospitals in China: A bootstrapping data envelopment analysis. BMJ Open 2016, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tone, K. A Slacks-Based Measure of Efficiency in Data Envelopment Analysis. Eur. J. Oper. Res. 2001, 130, 498–509. [Google Scholar] [CrossRef]
- Avkiran, N.K.; Tone, K.; Tsutsui, M. Bridging Radial and Non-Radial Measures of Efficiency in DEA. Ann. Oper. Res. 2008, 164, 127–138. [Google Scholar] [CrossRef]
- Torgersen, A.M.; Førsund, F.R.; Kittelsen, S.A. Slack-Adjusted Efficiency Measures and Ranking of Efficient Units. J. Prod. Anal. 1996, 7, 379–398. [Google Scholar] [CrossRef]
- Yang, T.; Chen, W.; Zhou, K.; Ren, M. Regional energy efficiency evaluation in China: A super efficiency slack-based measure model with undesirable outputs. J. Clean. Prod. 2018, 198, 859–866. [Google Scholar] [CrossRef]
- Zhou, C.; Shi, C.; Wang, S.; Zhang, G. Estimation of eco-efficiency and its influencing factors in Guangdong province based on Super-SBM and panel regression models. Ecol. Indic. 2018, 86, 67–80. [Google Scholar] [CrossRef]
- Tone, K. A slacks-based measure of super-efficiency in data envelopment analysis. Eur. J. Oper. Res. 2002, 143, 32–41. [Google Scholar] [CrossRef]
- Deng, J. Control problems of grey systems. Syst. Control Lett. 1982, 1, 288–294. [Google Scholar]
- Deng, J. Introduction to grey system theory. J. Grey Syst. 1989, 1, 1–24. [Google Scholar]
- Hsu, L.C. Applying the Grey prediction model to the global integrated circuit industry. Technol. Forecast. Soc. Chang. 2003, 70, 563–574. [Google Scholar] [CrossRef]
- Dang, H.S.; Huang, Y.F.; Wang, C.N.; Nguyen, T.M.T. An application of the short-term forecasting with limited data in the healthcare traveling industry. Sustainability 2016, 8, 1037. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, F.; Sun, C.; Li, Q. The research of improved grey GM (1,1) model to predict the postprandial glucose in type 2 diabetes. Biomed Res. Int. 2016, 2016, 6837052. [Google Scholar] [PubMed]
- Mahmod, W.E.; Watanabe, K. Modified Grey Model and its application to groundwater flow analysis with limited hydrogeological data: A case study of the Nubian Sandstone, Kharga Oasis, Egypt. Environ. Monit. Assess. 2014, 186, 1063–1081. [Google Scholar] [CrossRef] [PubMed]
- Theil, H. Economics and Information Theory; North-Holland: Amsterdam, The Netherlands, 1967. [Google Scholar]
- Gustafsson, B.; Shi, L. Income inequality within and across counties in rural China 1988 and 1995. J. Dev. Econ. 2002, 69, 179–204. [Google Scholar] [CrossRef]
- Alcantara, V.; Duro, J.A. Inequality of energy intensities across OECD countries: A note. Energy Policy 2004, 32, 1257–1260. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Prov. | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | Avg |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Beijing | 1.053 | 0.243 | 0.384 | 0.377 | 0.368 | 0.366 | 0.295 | 0.164 | 0.252 | 0.389 |
| 2 | Tianjin | 0.253 | 0.196 | 0.262 | 0.350 | 1.013 | 1.009 | 1.000 | 0.576 | 0.235 | 0.544 |
| 3 | Hebei | 0.448 | 0.384 | 0.413 | 0.368 | 0.328 | 0.344 | 0.313 | 0.304 | 1.057 | 0.440 |
| 4 | Shanxi | 0.409 | 0.309 | 0.322 | 0.284 | 0.287 | 0.286 | 0.260 | 0.218 | 0.461 | 0.315 |
| 5 | Inner Mongolia | 0.331 | 0.294 | 0.247 | 0.258 | 0.236 | 0.244 | 0.225 | 0.228 | 0.453 | 0.280 |
| 6 | Liaoning | 0.483 | 0.390 | 0.372 | 0.342 | 0.329 | 0.413 | 0.421 | 0.336 | 0.492 | 0.398 |
| 7 | Jilin | 1.034 | 0.187 | 0.203 | 0.277 | 0.265 | 0.231 | 0.260 | 0.241 | 0.193 | 0.321 |
| 8 | Heilongjiang | 0.387 | 0.234 | 0.280 | 0.274 | 0.213 | 0.235 | 0.273 | 0.305 | 0.241 | 0.271 |
| 9 | Shanghai | 1.889 | 1.510 | 1.412 | 1.376 | 1.278 | 1.268 | 1.000 | 1.339 | 1.060 | 1.348 |
| 10 | Jiangsu | 1.091 | 1.093 | 1.170 | 1.118 | 1.102 | 1.106 | 1.000 | 1.118 | 1.083 | 1.098 |
| 11 | Zhejiang | 1.129 | 1.002 | 0.483 | 0.503 | 0.495 | 0.407 | 0.413 | 0.391 | 0.179 | 0.556 |
| 12 | Anhui | 0.536 | 0.495 | 0.369 | 0.333 | 0.339 | 0.401 | 0.414 | 0.381 | 1.063 | 0.481 |
| 13 | Fujian | 1.421 | 1.158 | 1.063 | 0.750 | 0.622 | 0.588 | 0.575 | 0.466 | 0.525 | 0.797 |
| 14 | Jiangxi | 0.458 | 0.456 | 0.341 | 0.354 | 0.318 | 0.410 | 0.388 | 0.415 | 0.574 | 0.413 |
| 15 | Shandong | 0.435 | 0.461 | 0.386 | 0.534 | 0.433 | 0.422 | 0.397 | 0.383 | 1.011 | 0.496 |
| 16 | Henan | 0.466 | 0.457 | 0.469 | 0.454 | 0.424 | 0.450 | 0.480 | 0.471 | 0.808 | 0.498 |
| 17 | Hubei | 0.551 | 0.727 | 0.776 | 1.067 | 1.057 | 1.043 | 1.000 | 1.023 | 1.156 | 0.933 |
| 18 | Hunan | 0.477 | 0.532 | 0.507 | 0.619 | 0.513 | 0.726 | 0.810 | 1.004 | 0.792 | 0.664 |
| 19 | Guangdong | 1.196 | 1.334 | 1.425 | 1.334 | 1.278 | 1.285 | 1.000 | 1.095 | 1.232 | 1.242 |
| 20 | Guangxi | 0.322 | 1.077 | 0.655 | 0.572 | 0.560 | 0.609 | 0.716 | 0.584 | 0.568 | 0.629 |
| 21 | Hainan | 2.683 | 1.355 | 1.451 | 1.478 | 1.352 | 1.501 | 1.000 | 1.231 | 1.075 | 1.458 |
| 22 | Chongqing | 1.155 | 1.042 | 1.100 | 1.104 | 1.159 | 1.168 | 1.000 | 1.161 | 1.194 | 1.120 |
| 23 | Sichuan | 1.211 | 1.129 | 1.114 | 1.043 | 1.022 | 0.842 | 0.696 | 0.648 | 0.716 | 0.936 |
| 24 | Guizhou | 0.788 | 1.038 | 1.037 | 1.039 | 0.640 | 0.671 | 0.550 | 0.540 | 0.736 | 0.782 |
| 25 | Yunnan | 0.704 | 1.025 | 0.719 | 0.616 | 0.599 | 0.560 | 0.547 | 0.646 | 0.687 | 0.678 |
| 26 | Shaanxi | 0.338 | 0.394 | 0.327 | 0.350 | 0.386 | 0.381 | 0.376 | 0.324 | 0.467 | 0.371 |
| 27 | Gansu | 0.531 | 0.468 | 0.382 | 0.398 | 0.315 | 0.348 | 0.379 | 0.361 | 0.573 | 0.417 |
| 28 | Qinghai | 1.190 | 1.134 | 0.625 | 0.647 | 0.542 | 1.000 | 1.000 | 1.029 | 0.602 | 0.863 |
| 29 | Ningxia | 1.363 | 1.726 | 1.000 | 1.000 | 1.911 | 1.000 | 1.000 | 1.000 | 2.147 | 1.350 |
| 30 | Xinjiang | 0.673 | 0.574 | 0.502 | 0.429 | 0.424 | 0.379 | 0.402 | 0.351 | 0.533 | 0.474 |
| - | Avg | 0.834 | 0.747 | 0.660 | 0.655 | 0.660 | 0.656 | 0.606 | 0.611 | 0.739 | 0.685 |
| Year | Predicted Theil | Year | Predicted Theil |
|---|---|---|---|
| 2017 | 0.1471 | 2022 | 0.1359 |
| 2018 | 0.1448 | 2023 | 0.1338 |
| 2019 | 0.1426 | 2024 | 0.1317 |
| 2020 | 0.1403 | 2025 | 0.1296 |
| 2021 | 0.1381 | 2026 | 0.1276 |
| Region | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | Average |
|---|---|---|---|---|---|---|---|---|---|---|
| Eastern | 1.098 | 0.830 | 0.802 | 0.775 | 0.782 | 0.792 | 0.674 | 0.673 | 0.746 | 0.797 |
| Central | 0.540 | 0.425 | 0.408 | 0.458 | 0.427 | 0.473 | 0.486 | 0.507 | 0.661 | 0.487 |
| Western | 0.782 | 0.900 | 0.701 | 0.678 | 0.709 | 0.655 | 0.626 | 0.625 | 0.789 | 0.718 |
| Year | Intra-Regional | Inter-Regional | Total | Theil Index | |||
|---|---|---|---|---|---|---|---|
| Eastern | Central | Western | Sum | ||||
| 2008 | 51.6% | 5.3% | 22.6% | 79.5% | 20.5% | 100.0% | 0.1779 |
| 2009 | 42.8% | 6.9% | 27.5% | 77.2% | 22.8% | 100.0% | 0.1704 |
| 2010 | 48.8% | 7.8% | 24.2% | 80.7% | 19.3% | 100.0% | 0.1614 |
| 2011 | 45.3% | 16.1% | 25.4% | 86.9% | 13.1% | 100.0% | 0.1493 |
| 2012 | 32.4% | 13.6% | 39.8% | 85.8% | 14.2% | 100.0% | 0.1818 |
| 2013 | 43.2% | 18.0% | 25.9% | 87.1% | 12.9% | 100.0% | 0.1463 |
| 2014 | 46.7% | 18.3% | 24.4% | 89.4% | 10.6% | 100.0% | 0.1494 |
| 2015 | 46.8% | 22.5% | 26.9% | 96.2% | 3.8% | 100.0% | 0.1594 |
| 2016 | 39.3% | 22.4% | 36.7% | 98.4% | 1.6% | 100.0% | 0.1468 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Q.; Li, B.; Mohiuddin, M. Prediction and Decomposition of Efficiency Differences in Chinese Provincial Community Health Services. Int. J. Environ. Res. Public Health 2018, 15, 2265. https://doi.org/10.3390/ijerph15102265
Liu Q, Li B, Mohiuddin M. Prediction and Decomposition of Efficiency Differences in Chinese Provincial Community Health Services. International Journal of Environmental Research and Public Health. 2018; 15(10):2265. https://doi.org/10.3390/ijerph15102265
Chicago/Turabian StyleLiu, Qian, Bo Li, and Muhammad Mohiuddin. 2018. "Prediction and Decomposition of Efficiency Differences in Chinese Provincial Community Health Services" International Journal of Environmental Research and Public Health 15, no. 10: 2265. https://doi.org/10.3390/ijerph15102265
APA StyleLiu, Q., Li, B., & Mohiuddin, M. (2018). Prediction and Decomposition of Efficiency Differences in Chinese Provincial Community Health Services. International Journal of Environmental Research and Public Health, 15(10), 2265. https://doi.org/10.3390/ijerph15102265