Dimensions, Dialectic, Discourse. Three Political Perspectives on the Sustainability of the German Healthcare System

Abstract
1. Introduction
- Firstly, it was seen as a necessary question to elaborate further on what is meant by ‘sustainability’ when it is applied in the context of healthcare systems and health policy. This clarification was considered as especially important for the context of healthcare systems as—particularly with regard to the German social state—the notion of sustainability still faces prejudices and misunderstandings.
- Secondly, our research asked how sustainability can unfold its potential in concrete health politics (i.e., the daily struggles of a diverse set of players for power and influence). The goal was to take a deeper look into the ideological roots of the system in order to understand these struggles better.
- And thirdly, as a consequence of the analysis of the system’s roots, the question arose as to whether it is possible to design an institutional environment, a polity, which is able to enhance the potential of sustainability within the healthcare system in terms of sustainability-related factors (e.g., transparency or participation).
2. Materials and Methods
2.1. Literature Review
2.2. Grounded Theory Methodology
2.3. Design Thinking
3. Policy, Politics, Polity: Three Perspectives on the German Healthcare System
3.1. Policy: Defining Decisive Factors of Sustainability in Healthcare Systems
3.1.1. Description of the Main Outcomes
3.1.2. Scientific Context
3.2. Politics: Health Politics and Its Underlying Dialectic
3.2.1. Description of the Main Outcomes
3.2.2. Scientific Context
3.3. Polity: Designing the Discourse on Health-Related Values
3.3.1. Description of the Main Outcomes
3.3.2. Scientific Context
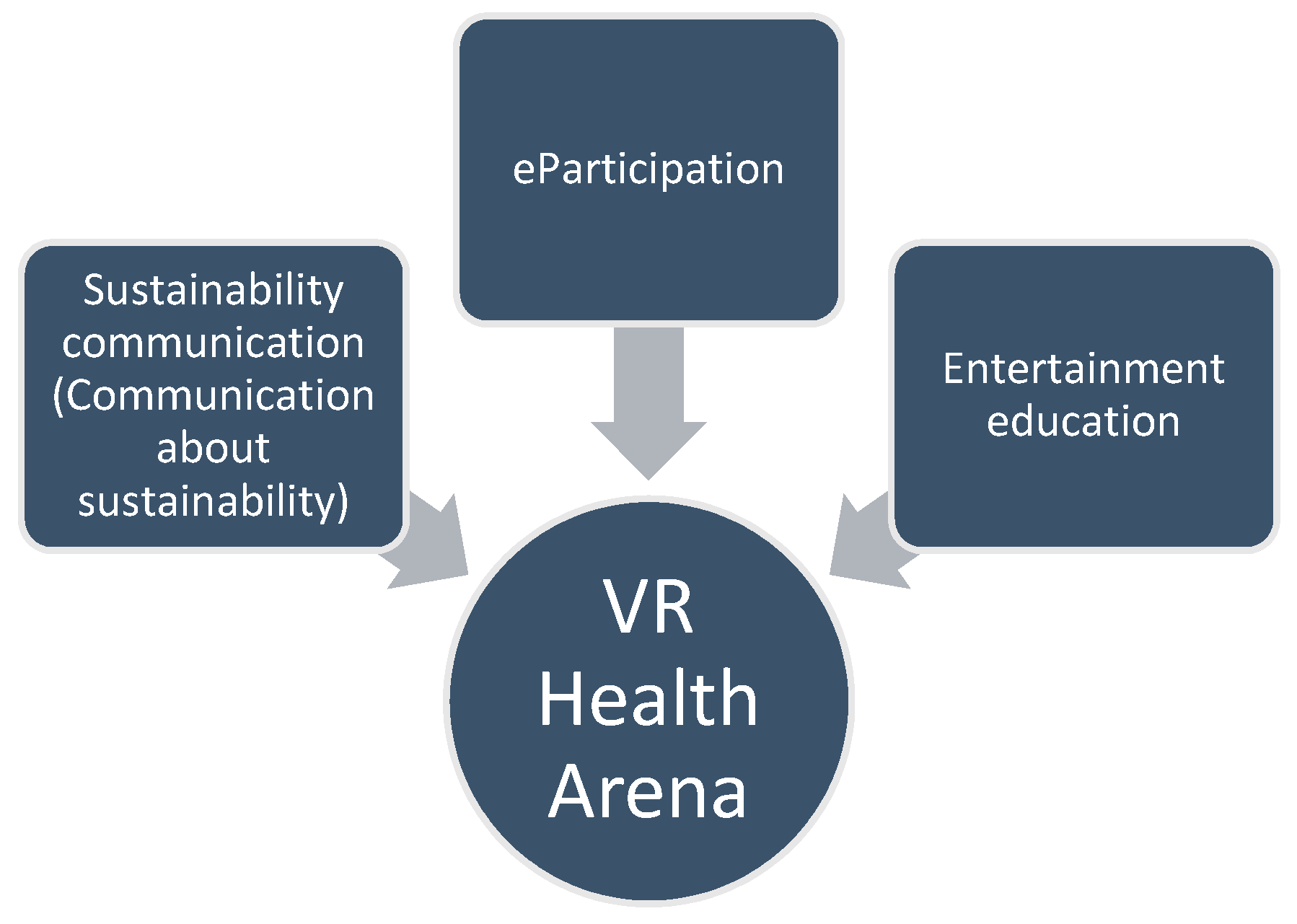
- Stimulation of interpersonal discourse instead of unidirectional ‘education’ of the audience: The approach of the VR Health Arena supports the voices of sustainability science in stressing that sustainability-related content should not be transmitted in the sense of top-down education [67]. It rather aims to confront people with different arguments, as it supposes that a non-hierarchical discourse is per se a desirable goal and a contribution to sustainable development.
- Increasing the motivational attachment of the audience by cognitive/affective-emotional stimuli and the adjustment to contemporary media consumption patterns: Instead of an exclusive focus on the presentation of the arguments in a rational manner, the VR Health Arena would try to reach the audience also on an affective-emotional level. In the best case, the play-off-based game mode of the show would lead to a continuous and intense engagement of the audience from different generations. The additional benefit of using VR technology would consist in its immersive potential, by giving the respective audience the impression of being directly part of the studio with the outlined opportunities to intervene.
- Collective learning through the imitation of role models and the possibility to practice the argumentative and reflexive competencies actively: The goal of the VR Health Arena would be to raise awareness for conflicting arguments in health–political matters, which are seen as constitutive for the healthcare system, in order to stimulate discussions among the audience. The respective teams would be coached in terms of their presentation style and develop their argumentative skills as the show proceeds. This personal development of the role models (i.e., the team members) could have a positive effect on the audience, as this could further strengthen the identification from the side of the audience. Furthermore, through the confidence of understanding the conflicting values in health-related matters better, as a result of their transparent comparison in the show setting, and by actively practicing the aspired competencies in the ‘smaller version’ of the VR Health Arena with other users, the feeling of self-efficacy among the audience could be promoted.
4. Conclusions
4.1. Central Conclusions
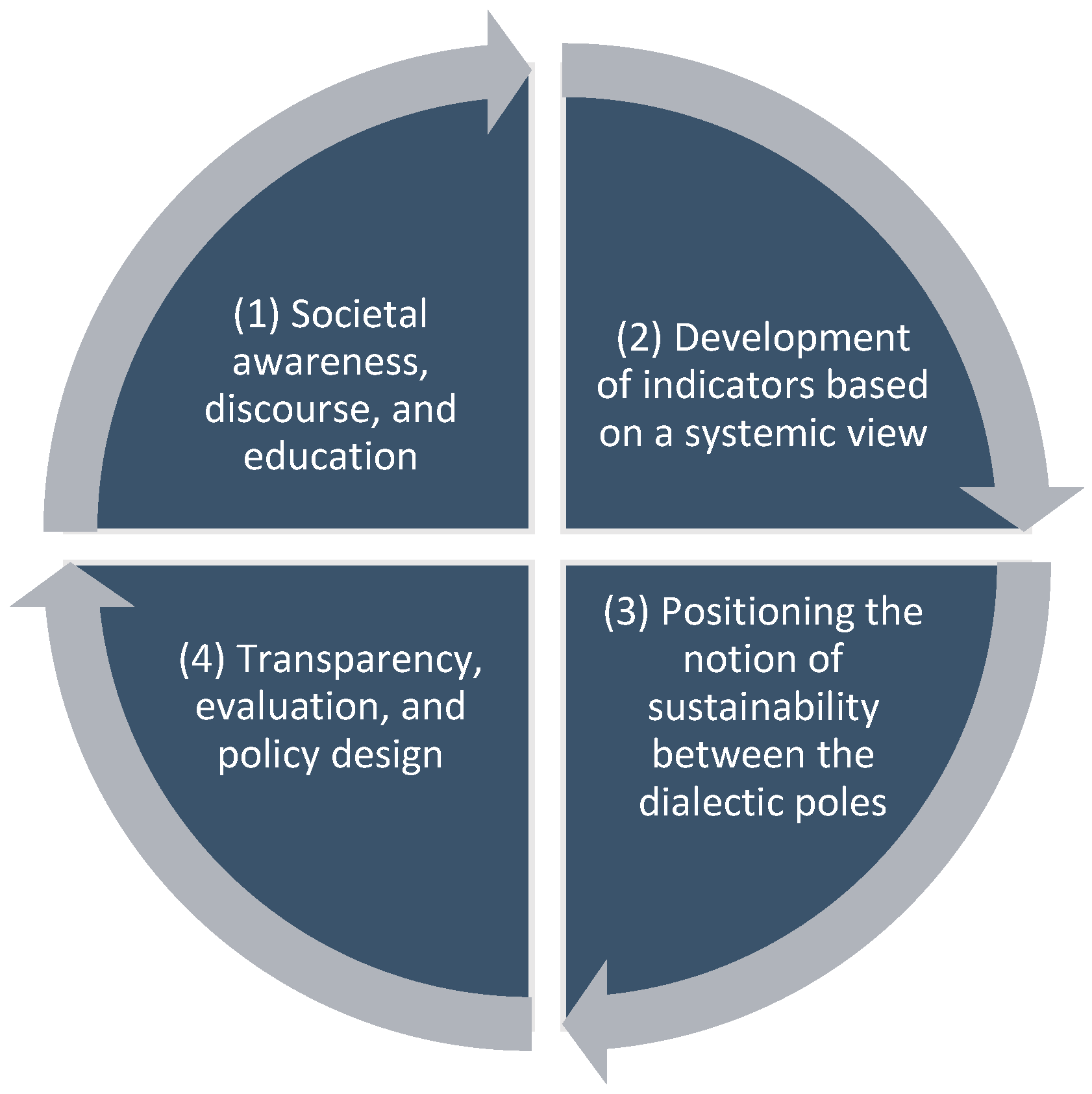
- (1) Societal Discourse, Awareness, and Education: The enhancement of sustainability in the context of healthcare systems would imply increasing public awareness among the citizenry concerning the importance of discussing the values, different options, and future directions of German health policies. A display in terms of the preferences concerning the current and future form of the healthcare system could be achieved by strengthening the possibility for a number of citizens to participate in a social discourse. Design thinking could be a useful method for developing need-based policies with a strong participatory spirit, which should go hand in hand with a profound educational strategy, regarding the competencies of the population in terms of health and the healthcare system. In order to increase the health competencies of the population regarding their argumentative and reflexive capacities, the VR Health Arena could be both an entertaining and effective component of such a strategy.
- (2) Development of Indicators based on a Systemic View: Based on the discourse and the insights with regard to the population’s preferences, research on the sustainability of healthcare systems should still aim to define measurable factors of healthcare sustainability. These approaches would include a public discourse in which political, economic, scientific, and civil societal actors could participate. Such indexes of healthcare sustainability could also build upon previous attempts on the European and on the international level, with their strong interest of measuring the performance of healthcare system with relevant data (e.g., [75]).
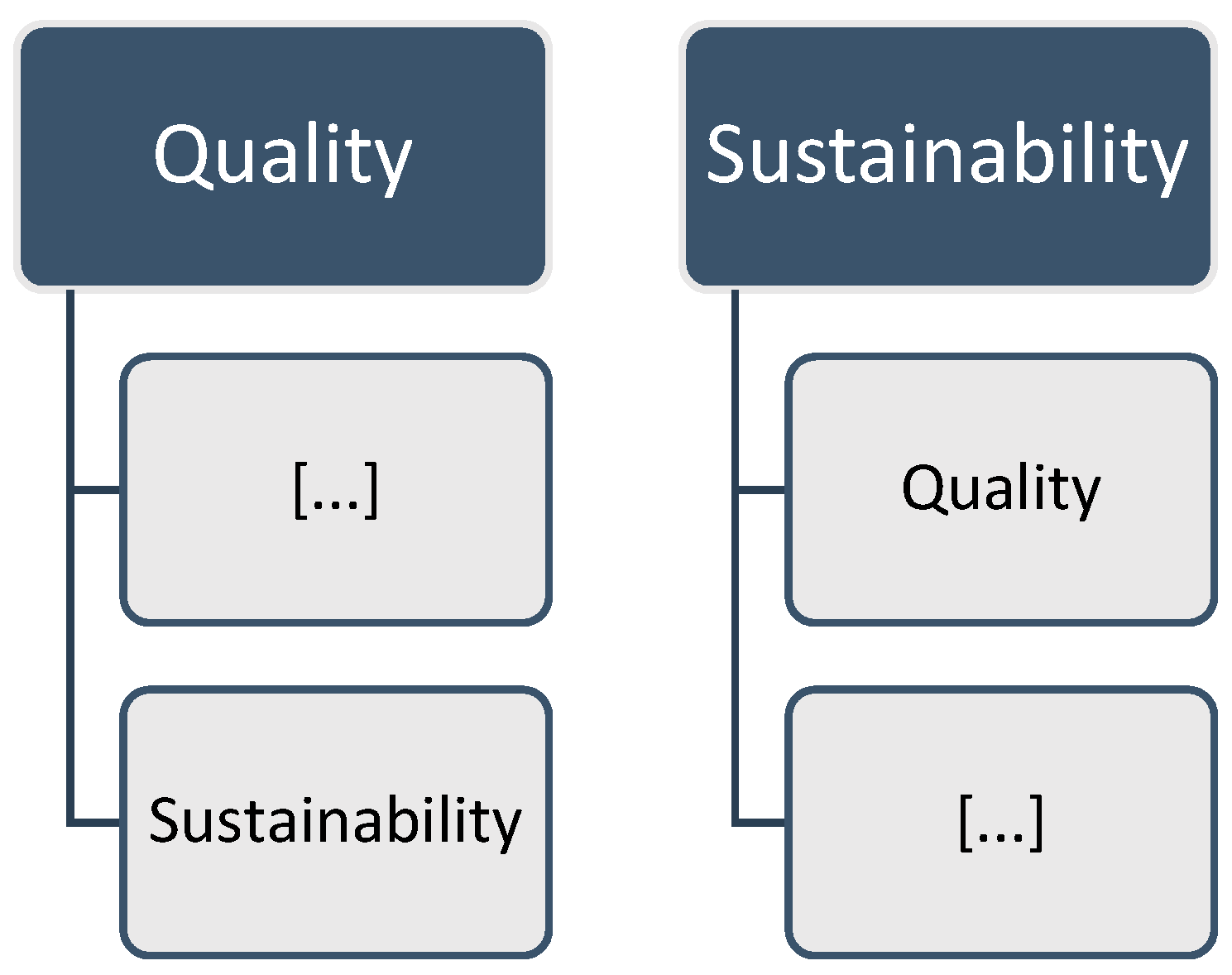
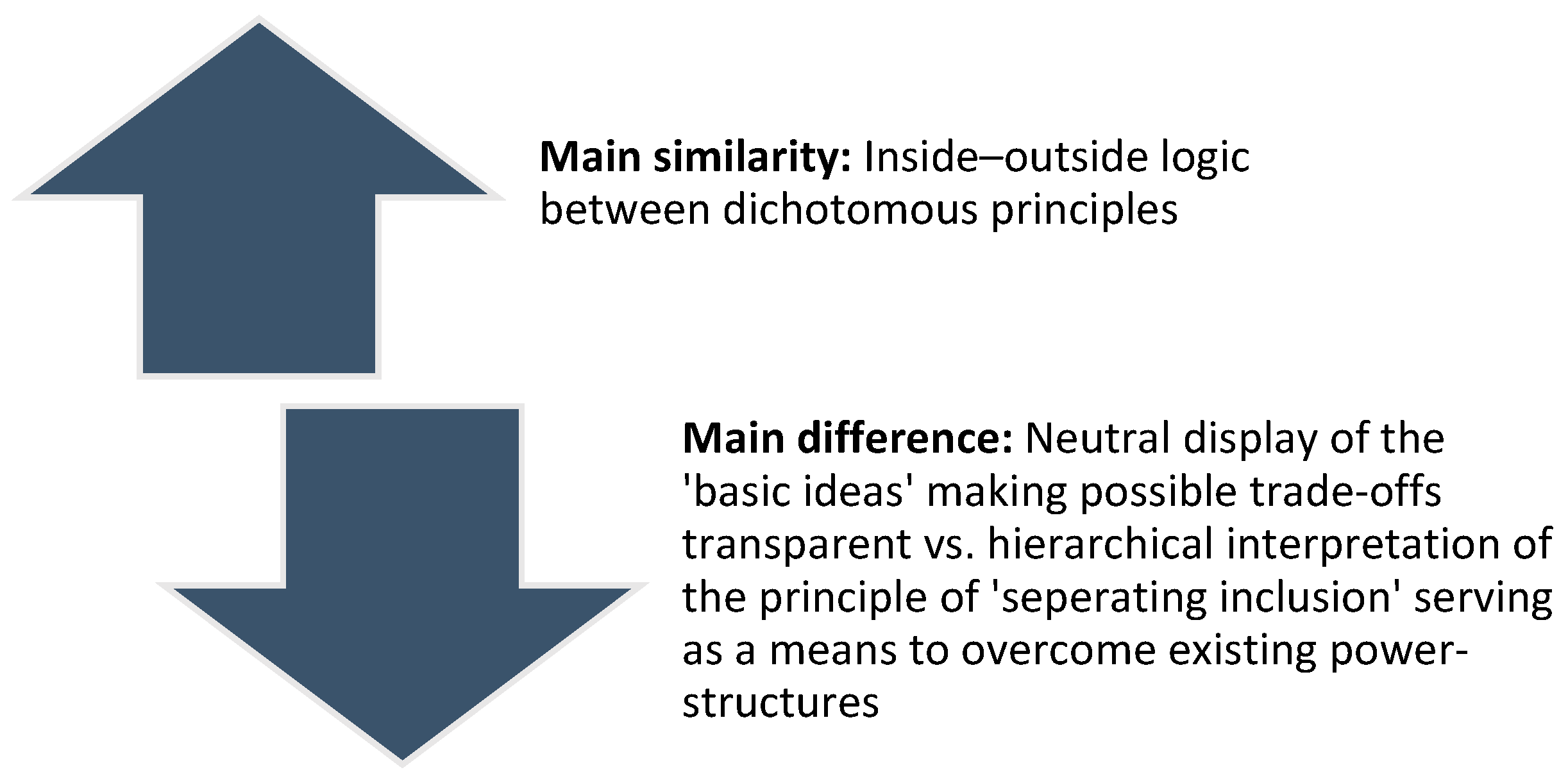
- (3) Positioning the Notion of Sustainability between the Dialectic Poles: The results of our research would make it possible to come to a more conscious decision, as each reference to sustainability in the public discourse could be positioned within the range of a health-related understanding of sustainability: As was discussed in the article by Fischer [9], the notion of sustainability may implicitly assume a more exclusive or inclusive understanding in terms of the dialectic basic ideas. Thus, the application of sustainability could be specified in terms of the extent to which a more exclusive or more inclusive understanding of the notion is applied within the range of the dialectic poles.
- (4) Transparency, Evaluation, and Policy Design: Apart from analyzing the respective understanding of sustainability, it would be considered as equally important to be transparent and to communicate the results of the analysis to the public. This would not only meet one of the basic values of sustainability on a general level (i.e., transparency; see [6]), but as well close the circle and afford the opportunity to feed the respective expertise and experience back to the efforts concerning education and awareness-raising. Furthermore, the development of the indicators should be observed and evaluated in terms of their potential to contribute to a more sustainable development of the healthcare system, which might also result in adjustments of concrete health policies. For organizing these adjustments in a participatory manner, design thinking could again be considered a useful tool.
4.2. Limitations and Perspectives for Further Research
4.3. Practical Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Simon, M. Das Gesundheitssystem in Deutschland. Eine Einführung in Struktur und Funktionsweise; Huber: Bern, Switzerland, 2013. (In German) [Google Scholar]
- Dietrich, C.F.; Riemer-Hommel, P. Challenges for the German health care system. Zeitschrift für Gastroenterologie 2012, 50, 557–572. [Google Scholar] [CrossRef] [PubMed]
- Giamo, S. Germany: Modernizing social health insurance to meet new challenges. In Reforming Health Care in the United States, Germany, and South Africa; Giamo, S., Ed.; Palgrave Macmillan: New York, NY, USA, 2016; pp. 95–142. [Google Scholar]
- Straub, C.; Repschläger, U.; Rumke, R.; Weineck, S. Aktuelle Herausforderungen in der Gesundheitspolitik. In Gesundheitswesen Aktuell 2017; Repschläger, U., Schulte, C., Osterkamp, N., Eds.; Barmer: Wuppertal, Germany, 2017; pp. 14–31. (In German) [Google Scholar]
- Coiera, E.; Hovenga, E.J.S. Building a sustainable health system. IMIA Yearb. Med. Inf. 2007, 2, 11–18. [Google Scholar]
- Fischer, M. Fit for the future? A new approach in the debate about what makes healthcare systems really sustainable. Sustainablity 2015, 7, 294–312. [Google Scholar] [CrossRef]
- World Commission on Environment and Development (WCED). Our Common Future. Report of the World Commission on Environment and Development; Oxford University Press: Oxford, UK, 1987. [Google Scholar]
- Größler, A. Policies, politics and polity: Comment on the paper by Bianchi. Syst. Res. Behav. Sci. 2010, 27, 385–389. [Google Scholar] [CrossRef]
- Fischer, M. Welfare with or without Growth? Potential Lessons from the German Healthcare System. Sustainability 2016, 8, 1088. [Google Scholar] [CrossRef]
- Fischer, M. The growth-welfare dialectic: What might Hegel say? Gaia 2016, 25, 80–83. [Google Scholar] [CrossRef]
- Fischer, M. Design it! Solving sustainability problems by applying design thinking. Gaia 2015, 24, 174–178. [Google Scholar] [CrossRef]
- Fischer, M. The future of health debates? A design thinking sketch of the VR Health Arena. Health Technol. 2018, 1–10. [Google Scholar] [CrossRef]
- Fischer, M. Decoding sustainability in the healthcare system. Teaching students how to problematize complex concepts. RISUS. J. Innov. Sustain. 2018. submitted. [Google Scholar]
- Dick, B. Grounded Theory: A Thumbnail Sketch. Available online: http://www.aral.com.au/resources/grounded.html (accessed on 16 June 2018).
- Charmaz, K. Grounded theory as an emergent method. In Handbook of Emergent Methods; Hesse-Bieber, S.N., Leavy, P., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 155–170. [Google Scholar]
- Breuer, F. Reflexive Grounded Theory. Eine Einführung für die Forschungspraxis; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2009. (In German) [Google Scholar]
- Glaser, B.G. Theoretical Sensitivity; Sociology Press: Mill Valley, CA, USA, 1978. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research, 11th ed.; Aldine: New York, NY, USA, 1980. [Google Scholar]
- Plattner, H.; Meinel, C.; Weinberg, U. Design Thinking. Innovation Lernen—Ideenwelten öffnen; Mi-wirtschaftsbuch: Munich, Germany, 2009. (In German) [Google Scholar]
- Coughlan, P.; Suri, J.F.; Canales, K. Prototypes as (design) tools for behavioral and organizational change: A design-based approach to help organizations change work behaviors. J. Appl. Behav. Sci. 2007, 43, 122–134. [Google Scholar] [CrossRef]
- Meierjürgen, R.; Becker, S.; Warnke, A. Die Entwicklung der Präventionsgesetzgebung in Deutschland. Prävention und Gesundheitsförderung 2016, 11, 206–213. (In German) [Google Scholar] [CrossRef]
- Rotar, A.M.; Van den Berg, M.J.; Kringos, D.S.; Klazinga, N.S. Reporting and use of the OECD Health Care Quality Indicators at national and regional level in 15 countries. Int. J. Qual. Health Care 2016, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Reference List of 100 Core Health Indicators. 2015. Available online: www.who.int/healthinfo/indicators/2015/en/ (accessed on 21 April 2018).
- Arah, O.A.; Westert, G.P.; Hurst, J.; Klazinga, N.S. A conceptual framework for the OECD health care quality indicators project. Int. J. Qual. Health Care 2006, 18 (Suppl. 1), 5–13. [Google Scholar] [CrossRef] [PubMed]
- Arah, O.A.; Westert, G.P.; Delnoij, D.M.; Klazinga, N.S. Health system outcomes and determinants amenable to public health in industrialized countries: A pooled, cross-sectional time series analysis. BMC Public Health 2005, 5, 81. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, H.; Laws, N. “Sustainability State” in the Making? Institutionalization of Sustainability in German Federal Policy Making. Sustainability 2014, 6, 2623–2641. [Google Scholar] [CrossRef]
- Faezipour, M.; Ferreira, S. Applying systems thinking to assess sustainability in healthcare system of systems. IJSSE 2006, 2, 290–308. [Google Scholar] [CrossRef]
- Braithwaite, J.; Matsuyama, Y.; Johnson, J. Healthcare Reform, Quality and Safety: Perspectives, Participants, Partnerships and Prospects in 30 Countries; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Henke, K.D.; Schreyögg, J. Towards Sustainable Health Care Systems: Strategies in Health Insurance Schemes in France, Germany, Japan and The Netherlands; International Social Security Association: Geneva, Switzerland, 2005. (In German) [Google Scholar]
- Bourdieu, P. The social space and the genesis of groups. Theory Soc. 1985, 14, 723–744. [Google Scholar] [CrossRef]
- Bourdieu, P. Ökonomisches Kapital, kulturelles Kapital, soziales Kapital. In Handbuch Bildungs-und Erziehungssoziologie; Bauer, U., Bittlingmayer, U.H., Scherr, A., Eds.; Springer: Wiesbaden, Germany, 2012; pp. 229–242. (In German) [Google Scholar]
- Hofbauer, J.; Striedinger, A. Gender Equality Politik: Überlegungen und Befunde zu institutionellen Logiken und symbolischer Gewalt am Beispiel von Hochschulen. In Neo-Institutionalismus-Revisited; Funder, M., Ed.; Nomos: Baden-Baden, Germany, 2017; pp. 499–524. (In German) [Google Scholar]
- Bourdieu, P. Social space and symbolic power. Sociol. Theory 1989, 7, 14–25. [Google Scholar] [CrossRef]
- Bourdieu, P.; Passeron, J.C. Grundlagen einer Theorie der Symbolischen Gewalt; Suhrkamp: Frankfurt, Germany, 1973. (In German) [Google Scholar]
- Okun, A.M. Equality and Efficiency. The Big Tradeoff; Brookings Institution: Washington, DC, USA, 1975. [Google Scholar]
- Lehmbruch, G. Konkordanzdemokratie. In Lexikon der Politik 3; Nohle, D., Ed.; Beck: Munich, Germany, 1992; pp. 206–211. (In German) [Google Scholar]
- Lehmbruch, G. Parteienwettbewerb im Bundesstaat. Regelsysteme und Spannungslagen im politischen System der Bundesrepublik Deutschland; Westdeutscher: Wiesbaden, Germany, 2000. [Google Scholar]
- Grunwald, A.; Kopfmüller, J. Nachhaltigkeit; Campus: Frankfurt am Main, Germany, 2006. (In German) [Google Scholar]
- Khan, M.A. Putting ‘Good Society’ Ahead of the Economy: Overcoming Neoliberalism’s Growth Trap and its Costly Consequences. Sustain. Dev. 2015, 23, 55–63. [Google Scholar] [CrossRef]
- Jackson, T. Live better by consuming less? Is there a “double dividend” in sustainable consumption? J. Ind. Ecol. 2005, 9, 19–36. [Google Scholar] [CrossRef]
- Paech, N. Liberation from Excess: The Road to a Post-Growth Economy; Oekom: Munich, Germany, 2012. [Google Scholar]
- Jakob, M.; Edenhofer, O. Green growth, degrowth, and the commons. Oxf. Rev. Econ. Policy 2014, 30, 447–468. [Google Scholar] [CrossRef]
- Ott, K. The case for strong sustainability. In Greifwald’s Environmental Ethics; Ott, K., Thapa, P.T., Eds.; Steinbecker: Greifswald, Germany, 2003; pp. 59–64. [Google Scholar]
- Ott, K. Institutionalizing strong sustainability: A Rawlsian perspective. Sustainability 2014, 6, 894–912. [Google Scholar] [CrossRef]
- Ayres, R.; Van den Bergh, J.; Gowdy, J. Strong versus weak sustainability: Economics, natural sciences, and consilience. Environ. Ethics 2001, 23, 155–168. [Google Scholar] [CrossRef]
- Hediger, W. Weak and strong sustainability, environmental conservation and economic growth. Nat. Resour. Model. 2006, 19, 359–394. [Google Scholar] [CrossRef]
- Biesecker, A.; Von Winterfeld, U. Extern?: Weshalb und Inwiefern Moderne Gesellschaften Externalisierung Brauchen und Erzeugen; Working Paper 2/2014; DFG-ForscherInnengruppe Postwachstumsgesellschaften: Jena, Germany, 2014. (In German) [Google Scholar]
- Mankiw, N.G.; Taylor, M.P. Economics; Cengage Learning: Hampshire, UK, 2014. [Google Scholar]
- Pressel, H. Der Gesundheitsfonds. Entstehung–Einführung–Weiterentwicklung–Folgen; Springer: Wiesbaden, Germany, 2012. (In German) [Google Scholar]
- Heck, R. Zur Diskussion um das Gesundheitswesen—Vorschlag für einen Ausweg. Sozialer Fortschritt 2005, 54, 172–174. (In German) [Google Scholar]
- Rürup, B. Nun ist die Politik gefordert. Die Empfehlungen der Kommission für die Nachhaltigkeit in der Finanzierung der Sozialen Sicherungssysteme. Soziale Sicherheit 2003, 8, 256–267. (In German) [Google Scholar]
- Brown, T.; Wyatt, J. Design thinking for social innovation. Dev. Outreach 2010, 12, 29–43. [Google Scholar] [CrossRef]
- Owen, C. Design thinking: Notes on its nature and use. Des. Res. Q. 2007, 2, 16–27. [Google Scholar]
- Korte, K.-R. Das politische System der Bundesrepublik Deutschland. In Politikwissenschaft: Eine Einführung; Lauth, H.-J., Wagner, C., Eds.; Schöningh: Paderborn, Germany, 2016; pp. 63–97. (In German) [Google Scholar]
- Habermas, J. Between Facts and Norms: Contributions to a Discourse Theory of Law and Democracy; MIT Press: Cambridge, MA, USA, 1996. [Google Scholar]
- Renn, O. Participatory processes for designing environmental policies. Land Use Policy 2006, 23, 34–43. [Google Scholar] [CrossRef]
- Medaglia, R. eParticipation research: Moving characterization forward (2006–2011). Gov. Inf. Q. 2012, 29, 346–360. [Google Scholar] [CrossRef]
- Newig, J.; Schulz, D.; Fischer, D.; Hetze, K.; Laws, N.; Lüdecke, G.; Rieckmann, M. Communication Regarding Sustainability: Conceptual Perspectives and Exploration of Societal Subsystems. Sustainability 2013, 5, 2976–2990. [Google Scholar] [CrossRef]
- Fischer, D.; Lüdecke, G.; Godemann, J.; Michelsen, G.; Newig, J.; Rieckmann, M.; Schulz, D. Sustainability communication. In Sustainability Science. An Introduction; Heinrichs, H., Martens, P., Michelsen, G., Wiek, A., Eds.; Springer: Dordrecht, The Netherlands, 2016; pp. 139–148. [Google Scholar]
- Fuchs, C. The implications of new information and communication technologies for sustainability. Environ. Dev. Sustain. 2008, 10, 291–309. [Google Scholar] [CrossRef]
- Vaughan, P.W.; Rogers, E.M.; Singhal, A.; Swalehe, R.M. Entertainment-education and HIV/AIDS prevention: A field experiment in Tanzania. J. Health Commun. 2000, 5 (Suppl. 1), 81–100. [Google Scholar] [PubMed]
- Wang, H.; Singhal, A. Entertainment-education through digital games. In Serious Games Mechanisms and Effects; Ritterfeld, U., Cody, M.J., Vorderer, P., Eds.; Routledge: New York, NY, USA, 2009; pp. 271–292. [Google Scholar]
- Lampert, C. Gesundheitsförderung durch Unterhaltung? Zum Potenzial des Entertainment-Education-Ansatzes für die Förderung des Gesundheitsbewusstseins. Medien Kommunikationswissenschaft 2003, 51, 461–477. (In German) [Google Scholar] [CrossRef]
- Papa, M.J.; Singhal, A.; Law, S.; Pant, S.; Sood, S.; Rogers, E.M.; Shefner-Rogers, C.L. Entertainment-education and social change: An analysis of parasocial interaction, social learning, collective efficacy, and paradoxical communication. J. Commun. 2000, 50, 31–55. [Google Scholar] [CrossRef]
- Singhal, A.; Rogers, E. Entertainment-Education: A Communication Strategy for Social Change; Routledge: Milton Park, UK, 2012. [Google Scholar]
- Reinermann, J.-L.; Lubjuhn, S.; Bouman, M.; Singhal, A. Entertainment-education: Storytelling for the greater, greener good. Int. J. Sustain. Dev. 2014, 17, 176–191. [Google Scholar] [CrossRef]
- Barth, M. Social learning instead of educating the other. Gaia 2012, 20, 232–235. [Google Scholar] [CrossRef]
- Luckmann, T. Zum Verhältnis von Alltagswissen und Wissenschaft. In Wissenschaftstransfer in der Weiterbildung: Der Beitrag der Wissenssoziologie; Rebel, K., Ed.; Beltz: Weinheim, Germany, 1989; pp. 28–35. (In German) [Google Scholar]
- Luhmann, N. The autopoiesis of social systems. In Sociocybernetic Paradoxes. Observation, Control and Evolution of Self-Steering Systems; Geyer, F., van der Zouven, J., Eds.; Sage: Beverly Hills, CA, USA, 1986; pp. 172–192. [Google Scholar]
- Nowotny, H.; Scott, P.; Gibbons, M. Re-Thinking Science. Knowledge and the Public in an Age of Uncertainty; Polity Press: Oxford, UK, 2004. [Google Scholar]
- Majchrzak, A.; Markus, M.L.; Wareham, J. Designing for digital transformation: Lessons for information systems research from the study of ICT and societal challenges. MIS Q. 2016, 40, 267–277. [Google Scholar] [CrossRef]
- Junginger, S. Design and innovation in the public sector: Matters of design in policy-making and policy implementation. Ann. Rev. Policy Des. 2013, 1, 1–11. [Google Scholar]
- Junginger, S. Transforming Public Services by Design: Reorienting Policies, Organizations and Services around People; Routledge: Milton Park, UK, 2017. [Google Scholar]
- Gießelmann, K. Gesundheitskompetenz: Aktionsplan mit viel Spielraum. Deutsches Ärzteblatt 2018, 115, A-317/B-271/C-271. (In German) [Google Scholar]
- Cacace, M.; Ettelt, S.; Mays, N.; Nolte, E. Assessing quality in cross-country comparisons of health systems and policies: Towards a set of generic quality criteria. Health Policy 2013, 112, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Marmor, T.; Wendt, C. Conceptual frameworks for comparing healthcare politics and policy. Health Policy 2012, 107, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.G.; Ostheim, T.; Siegel, N.A.; Zohlnhöfer, R. Der Wohlfahrtsstaat: Eine Einführung in den Historischen und Internationalen Vergleich; Springer: Wiesbaden, Germany, 2008. (In German) [Google Scholar]
- Pinzone, M.; Guerci, M.; Lettieri, E.; Redman, T. Progressing in the change journey towards sustainability in healthcare: The role of ‘Green’HRM. J. Clean. Prod. 2016, 122, 201–211. [Google Scholar] [CrossRef]
- Höhl, R. Ökonomischer Zugzwang: Neutrale Beschwerdestelle muss her! Ärzte Zeitung Online 15 April 2018. Available online: https://www.aerztezeitung.de/politik_gesellschaft/berufspolitik/article/961635/thema-dgim-oekonomischer-zugzwang-neutrale-beschwerdestelle-muss-her.html?sh=2&h=-1000585904 (accessed on 21 April 2018). (In German).
- CDU/CSU & SPD. Ein neuer Aufbruch für Europa. Eine neue Dynamik für Deutschland. Ein neuer Zusammenhalt für unser Land; Koalitionsvertrag zwischen CDU, CSU und SPD. 19; Legislaturperiode: Berlin, Germany, 2018. (In German) [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Narrative Bracket: The Three Dimensions of the Political Term | ||||
|---|---|---|---|---|
| Policy | Politics | Polity | ||
| Second narrative bracket: Increasing methodological innovativeness | Literature review | [6] | ||
| Grounded theory methodology | [9,10] | |||
| Design Thinking | [11,12,13] | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischer, M.; Heinrichs, H. Dimensions, Dialectic, Discourse. Three Political Perspectives on the Sustainability of the German Healthcare System. Int. J. Environ. Res. Public Health 2018, 15, 1526. https://doi.org/10.3390/ijerph15071526
Fischer M, Heinrichs H. Dimensions, Dialectic, Discourse. Three Political Perspectives on the Sustainability of the German Healthcare System. International Journal of Environmental Research and Public Health. 2018; 15(7):1526. https://doi.org/10.3390/ijerph15071526
Chicago/Turabian StyleFischer, Matthias, and Harald Heinrichs. 2018. "Dimensions, Dialectic, Discourse. Three Political Perspectives on the Sustainability of the German Healthcare System" International Journal of Environmental Research and Public Health 15, no. 7: 1526. https://doi.org/10.3390/ijerph15071526
APA StyleFischer, M., & Heinrichs, H. (2018). Dimensions, Dialectic, Discourse. Three Political Perspectives on the Sustainability of the German Healthcare System. International Journal of Environmental Research and Public Health, 15(7), 1526. https://doi.org/10.3390/ijerph15071526