Annual Direct Medical Costs of Diabetic Foot Disease in Brazil: A Cost of Illness Study

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Site and Population
2.2. Ethics Approval
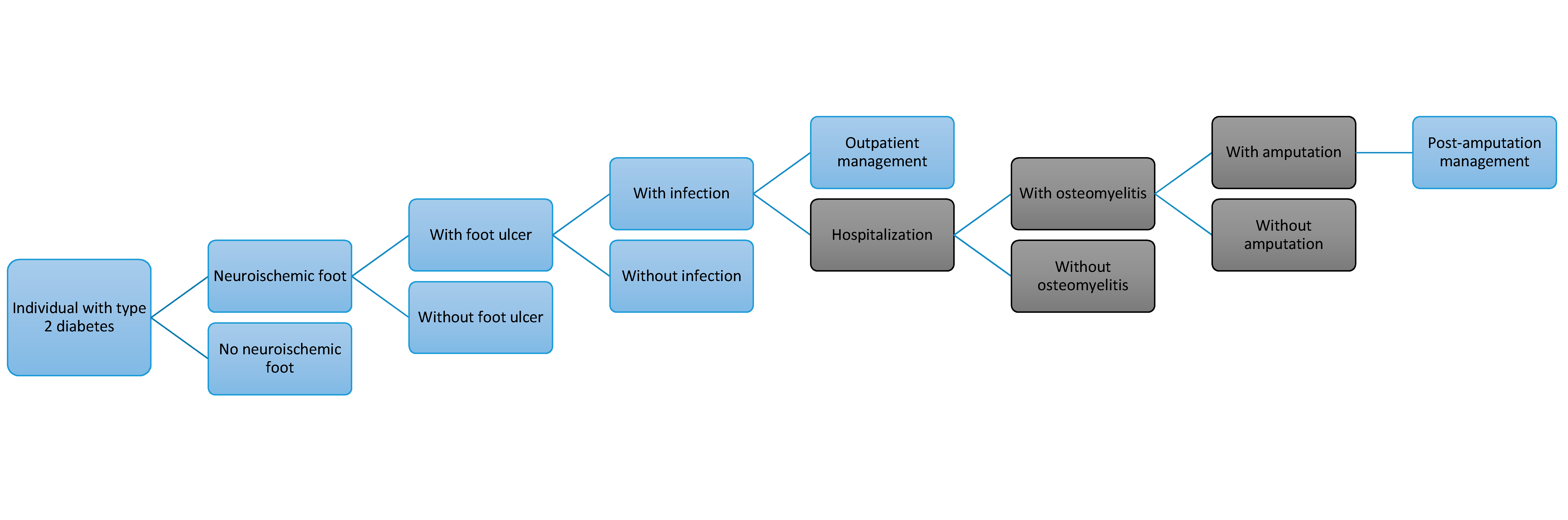
2.3. Decision Analytic Model
2.4. Model Parameters and Data Sources
2.5. Outpatient DFD Costs
2.6. Hospitalized DFD Patients and Costs
2.7. Data Analysis
2.8. Sensitivity Analysis
3. Results
3.1. Outpatient Burden and Costs
3.2. Hospitalization Burden and Costs
3.3. Overall DFD Costs
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis dagger. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. Diabetes Atlas, 7th ed. Available online: http://www.diabetesatlas.org/resources/2017-atlas.html (accessed on 11 April 2017).
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A.; Ingelfinger, J.R. Diabetic foot ulcers and their recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Moxey, P.W.; Gogalniceanu, P.; Hinchliffe, R.J.; Loftus, I.M.; Jones, K.J.; Thompson, M.M.; Holt, P.J. Lower extremity amputations—A review of global variability in incidence. Diabet. Med. 2011, 28, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Parisi, M.C.; Moura Neto, A.; Menezes, F.H.; Gomes, M.B.; Teixeira, R.M.; de Oliveira, J.E.; Pereira, J.R.; Fonseca, R.M.; Guedes, L.B.; Costa, E.F.A.; et al. Baseline characteristics and risk factors for ulcer, amputation and severe neuropathy in diabetic foot at risk: The BRAZUPA study. Diabetol. Metab. Syndr. 2016, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Ragnarson Tennvall, G.; Apelqvist, J. Health-economic consequences of diabetic foot lesions. Clin. Infect. Dis. 2004, 39, S132–S139. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. Diabetes Atlas, 8th ed. Available online: http://www.diabetesatlas.org/ (accessed on 22 November 2017).
- Macinko, J.; Harris, M.J. Brazil’s family health strategy—Delivering community-based primary care in a universal health system. N. Engl. J. Med. 2015, 372, 2177–2181. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Beneficiary Information System. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2012/f16.def (accessed on 20 April 2017).
- Instituto Brasileiro de Geografia e Estatística (IBGE). National Health Research 2013. Access and Utilization of Health Services, Injuries and Violences: Brazil, Regions and States; Brazilian Institute of Geography and Statistics: Rio de Janeiro, Brazil, 2015.
- Instituto Brasileiro de Geografia e Estatística (IBGE). Census. Available online: http://downloads.ibge.gov.br/downloads_estatisticas.htm (accessed on 20 June 2017).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde: 2013: Percepção do Estado de Saúde, Estilos de vida e Doenças Crônicas-Brasil, Grandes Regiões e Unidades da Federação; IBGE: Rio de Janeiro, Brazil, 2014.
- Vieira-Santos, I.C.R.; Souza, W.V.; Carvalho, E.F.; Medeiros, M.C.W.C.; Nóbrega, M.G.D.L.; Lima, P.M.S. Prevalência de pé diabético e fatores associados nas unidades de saúde da família da cidade do recife, pernambuco, Brasil, em 2005. Cadernos Saúde Pública 2008, 24, 2861–2870. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Al Derwish, M.; Ouizi, S.; Youssef, A.M.; Subhani, S.N.; Ibrahim, H.M.; Alamri, B.N. Diabetic foot complications and their risk factors from a large retrospective cohort study. PLoS ONE 2015, 10, e0124446. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.C.; Silva, A.P.S.; Costa, M.T.; Frizzo, G.G.; Santin, R.A.L.; Fucs, P.M.M.B. Epidemiological aspects of foot and ankle injury in the diabetic patient. Acta Ortop. Bras. 2010, 18, 135–141. [Google Scholar] [CrossRef]
- Portal da Saúde. Informações de Saúde (Tabnet). Assistência à Saúde. Produção Hospitalar (SIH/SUS). Available online: http://www2.datasus.gov.br/DATASUS/index.php?area=0202 (accessed on 11 April 2017).
- Hopkins, R.B.; Burke, N.; Harlock, J.; Jegathisawaran, J.; Goeree, R. Economic burden of illness associated with diabetic foot ulcers in Canada. BMC Health Serv. Res. 2015, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Hurn, S.E.; Fernando, M.E.; Jen, S.D.; Kuys, S.S.; Kamp, M.C.; Reed, L.F. Prevalence of foot disease and risk factors in general inpatient populations: A systematic review and meta-analysis. BMJ Open 2015, 5, e008544. [Google Scholar] [CrossRef] [PubMed]
- Assumpção, E.C.; Pitta, G.B.; Macedo, C.L.; Mendonça, G.B.; Albuquerque, L.C.A.; Lyra, L.C.B.; Timbó, R.M.; Buarque, T.L.L. Comparação dos fatores de risco para amputações maiores e menores em pacientes diabéticos de um programa de saúde da família. J. Vasc. Bras. 2009, 8, 133–138. [Google Scholar] [CrossRef]
- Roth-Albin, I.; Mai, S.H.; Ahmed, Z.; Cheng, J.; Choong, K.; Mayer, P.V. Outcomes following advanced wound care for diabetic foot ulcers: A Canadian study. Can. J. Diabetes 2017, 41, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Peters, E.J.; Armstrong, D.G.; Wendel, C.S.; Murdoch, D.P.; Lipsky, B.A. Risk factors for developing osteomyelitis in patients with diabetic foot wounds. Diabetes Res. Clin. Pract. 2009, 83, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Caiafa, J.S.; Castro, A.A.; Fidelis, C.; Santos, V.P.; Silva, E.S.; Sitângulo Junior, C.J. Atenção Integral ao Portador de pé Diabético; Sociedade Brasileira de Angiologia e de Cirurgia Vascular: São Paulo, Brasil, 2011; p. 36. [Google Scholar]
- Ministério da Saúde. Caderno de Atenção Básica—Diabetes Mellitus; Secretaria de Atenção à Saúde, Departamento de Atenção Básica, Ed.; Ministério da Saúde: Brasilía, Brasil, 2006; Volume 16.
- Ministério da Saúde. System of Management of the Table of Procedures, Medications and OPM from SUS. Available online: http://sigtap.datasus.gov.br/tabela-unificada/app/sec/inicio.jsp (accessed on 18 April 2017).
- Portal da Saúde. Bases Anuais Compiladas. Banco de Preços em Saúde. Available online: http://portalsaude.saude.gov.br/index.php/cidadao/principal/banco-de-precos-em-saude?layout=edit&id=8667 (accessed on 11 April 2017).
- Ministério da Saúde. Datasus. Ministry of Health. File Transfer Service. Available online: http://www2.datasus.gov.br/DATASUS/index.php?area=0901&item=1&acao=25 (accessed on 20 June 2017).
- World Health Organization. International Classification of Diseases (ICD) 10. Available online: http://apps.who.int/classifications/icd10/browse/2016/en-/XVI (accessed on 20 June 2017).
- Donnan, P.T.; Leese, G.P.; Morris, A.D.; Audit, D. Hospitalizations for people with type 1 and type 2 diabetes compared with the nondiabetic population of Tayside, Scotland: A retrospective cohort study of resource use. Diabetes Care 2000, 23, 1774–1779. [Google Scholar] [CrossRef] [PubMed]
- Al-Mayahi, M.; Cian, A.; Kressmann, B.; de Kalbermatten, B.; Rohner, P.; Egloff, M.; Jafaar, J.; Malacarne, S.; Miozzari, H.H.; Uckay, I. Associations of diabetes mellitus with orthopaedic infections. Infect. Dis. 2016, 48, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, F.L.; Maggini, M.; De Bellis, A.; Seghieri, G.; Anichini, R. Lower extremity amputations in persons with and without diabetes in Italy: 2001–2010. PLoS ONE 2014, 9, e86405. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.I.; Hoffmann, J.F.; de Fatima Sander Diniz, M.; Lotufo, P.A.; Griep, R.H.; Bensenor, I.M.; Mill, J.G.; Barreto, S.M.; Aquino, E.M.; Duncan, B.B. High prevalence of diabetes and intermediate hyperglycemia—The Brazilian longitudinal study of adult health (ELSA-Brasil). Diabetol. Metab. Syndr. 2014, 6, 123. [Google Scholar] [CrossRef] [PubMed]
- Malerbi, D.A.; Franco, L.J. Multicenter study of the prevalence of diabetes mellitus and impaired glucose tolerance in the urban Brazilian population aged 30–69 years. The Brazilian cooperative group on the study of diabetes prevalence. Diabetes Care 1992, 15, 1509–1516. [Google Scholar] [CrossRef] [PubMed]
- World Bank. PPP Conversion Factor, GDP (LCU per International $). Available online: http://data.worldbank.org/indicator/PA.NUS.PPP?locations=BR> (accessed on 25 June 2017).
- American Diabetes Association. Economic costs of diabetes in the US in 2012. Diabetes Care 2013, 36, 1033–1046. [Google Scholar]
- Cardenas, M.K.; Mirelman, A.J.; Galvin, C.J.; Lazo-Porras, M.; Pinto, M.; Miranda, J.J.; Gilman, R.H. The cost of illness attributable to diabetic foot and cost-effectiveness of secondary prevention in Peru. BMC Health Serv. Res. 2015, 15, 483. [Google Scholar] [CrossRef] [PubMed]
- Cawich, S.O.; Islam, S.; Hariharan, S.; Harnarayan, P.; Budhooram, S.; Ramsewak, S.; Naraynsingh, V. The economic impact of hospitalization for diabetic foot infections in a Caribbean nation. Perm. J. 2014, 18, e101–e104. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.; Attinger, C.; Abbas, Z.; Bal, A.; Rojas, N.; Xu, Z.R. Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab. Res. Rev. 2012, 28, 107–111. [Google Scholar] [CrossRef] [PubMed]
- World Bank. International Comparison Program Database. GDP, PPP (Current International $). Available online: https://data.worldbank.org/indicator/NY.GDP.MKTP.PP.CD?locations=BR&year_high_desc=true (accessed on 19 December 2017).
- World Health Organization. Countries. Brazil. Available online: http://www.who.int/countries/bra/en/ (accessed on 19 December 2017).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Conta-Satélite de Saúde: Brasil: 2010–2015; Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, Brasil, 2017.
- Ministério da Saúde. DATASUS. Tabulações Avançadas Sobre os Arquivos rd. Available online: http://datasus.saude.gov.br/ (accessed on 19 December 2017).
- Rezende, K.F.; Ferraz, M.B.; Malerbi, D.A.; Melo, N.H.; Nunes, M.P.; Pedrosa, H.C.; Chacra, A.R. Direct costs and outcomes for inpatientes with diabetes mellitus and foot ulcers in a developing country: The experience of the public health system of Brazil. Diabetes Metab. Syndr. Clin. Res. Rev. 2009, 3, 228–232. [Google Scholar] [CrossRef]
- Rezende, K.F.; Ferraz, M.B.; Malerbi, D.A.; Melo, N.H.; Nunes, M.P.; Pedrosa, H.C.; Chacra, A.R. Predicted annual costs for inpatients with diabetes and foot ulcers in a developing country—A simulation of the current situation in Brazil. Diabet. Med. 2010, 27, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M.C.L.; Bortoletto, M.S.S.; Silva, R.S. Amputação de membros inferiores de portadores de diabetes mellitus: Análise dos custos da internação em hospital público. Ciência Cuidado Saúde 2010, 9, 107–113. [Google Scholar] [CrossRef]
- Oliveira, A.F.; De Marchi, A.C.B.; Leguisamo, C.P.; Baldo, G.V.; Wawginiak, T.A. Estimativa do custo de tratar o pé diabético, como prevenir e economizar recursos. Ciência Saúde Coletiva 2014, 19, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Milman, M.H.S.A.; Leme, C.B.M.; Borelli, D.T.; Kater, F.R.; Baccili, E.C.D.C.; Rocha, R.C.M.; Senger, M.-H. Pé diabético: Avaliação da evolução e custo hospitalar de pacientes internados no conjunto hospitalar de sorocaba. Arq. Bras. Endocrinol. Metabol. 2001, 45, 447–451. [Google Scholar] [CrossRef]
- Rezende, K.F.; Nunes, M.A.; Melo, N.H.; Malerbi, D.; Chacra, A.R.; Ferraz, M.B. In hospital care for diabetic foot: A comparison between the estimated cost and the SUS reimbursement. Arq. Bras. Endocrinol. Metabol. 2008, 52, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A. IDF clinical practice recommendation on the diabetic foot: A guide for healthcare professionals. Diabetes Res. Clin. Pract. 2017, 127, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, H.C.; Leme, L.A.; Novaes, C.; Saigg, M.; Sena, F.; Gomes, E.B.; Mayer Coutinho, A.; Boulton, A.J.M. The diabetic foot in South America: Progress with the Brazilian save the diabetic foot project. Int. Diabetes Monit. 2004, 16, 17–23. [Google Scholar]


{kind=link}
| Model Parameters | Base Case | Sensitivity Analysis | ||||
|---|---|---|---|---|---|---|
| Value | Reference | Lower | Reference | Upper | Reference | |
| Total adult population, 2014 | 148,696,000 | [12] | ||||
| Prevalence of self-reported diabetes (%) | 6.2 | [13] | ||||
| Prevalence of neuroischemic foot among DM # patients (%) | 9 | [14] | 3.3 | [15] | 10.6 | [14] |
| Proportion of DM # patients with ulcers (%) | 5.27 | [13] | 1.24 | [15] | 30 | [16] |
| Ulcers managed as outpatients * (%) | 98.31 | [17] | 65.2 | [18] | 99.7 | [19] |
| Non-infected foot ulcer (%) | 50 | [20] | 88 | [21] | 44.5 | [22]] |
| Infected foot ulcer (%) | 50 | [20] | 12 | [21] | 55.5 | [22] |
| Ulcers managed as inpatients | 1.69 | [17] | 34.8 | [18] | 0.3 | [19] |
| Amputation (%) | 1.36 | [13] | 1.1 | [15] | 13.7 | [6] |
| Diabetes Mellitus * | |||
| E10 | Insulin-dependent diabetes mellitus | ||
| E11 | Non-insulin-dependent diabetes mellitus | ||
| E13 | Other specified diabetes mellitus | ||
| E14 | Unspecified diabetes mellitus | ||
| Complications Related to Diabetic Foot Disease | Relative Risk | Ref. | |
| G57 | Mononeuropathies of lower limb | 1.97 | [29] |
| G59 | Mononeuropathy in diseases classified elsewhere | 1.97 | [29] |
| G63 | Polyneuropathy in diseases classified elsewhere | 1.97 | [29] |
| L97 | Non-pressure chronic ulcer of lower limb, not elsewhere classified | 1.97 | [29] |
| M86 | Osteomyelitis | 5.8 | [30] |
| M87.3 | Other secondary osteonecrosis | 5.8 | [30] |
| M87.8 | Other osteonecrosis | 5.8 | [30] |
| M87.9 | Unspecified osteonecrosis | 5.8 | [30] |
| R02 | Gangrene, not elsewhere classified | 10.9 | [31] |
| S88 | Traumatic amputation of lower leg | 6.4 | [31] |
| S98 | Traumatic amputation of ankle and foot | 19.4 | [31] |
| DFD Condition | Number of Individuals | ||
|---|---|---|---|
| Base Case | Sensitivity Analysis | ||
| Individuals with diabetes mellitus | 9,219,152 | Lower | Upper |
| DM patients with neuroischemic foot | 829,724 | 304,232 | 977,230 |
| DM patients with ulcers | 43,727 | 3773 | 293,169 |
| Patients with ulcers managed as outpatients | 42,984 | 2460 | 292,290 |
| Non-infected foot ulcer | 21,492 | 2165 | 130,069 |
| Infected foot ulcer | 21,492 | 295 | 162,221 |
| Patients amputated requiring follow up | 11,284 | 3347 | 133,880 |
| DFD Condition | Value in Int$ | ||
|---|---|---|---|
| Base Case | Sensitivity Analysis | ||
| Lower | Upper | ||
| Neuroischemic foot without ulcer | 285,197,635 | 104,572,466 | 335,899,436 |
| Non-infected foot ulcer | 8,771,482 | 833,410 | 53,085,829 |
| Infected foot ulcer | 34,752,923 | 477,287 | 262,319,121 |
| Patients amputated requiring follow up | 6,767,704 | 2,007,089 | 80,294,609 |
| Total outpatient DFD costs | 335,489,743 | 107,940,251 | 731,598,996 |
| Diabetes Mellitus (E10, E11, E13, E14) * | Number (n) | Average Hospitalization Cost (Int$) | Total Hospitalization Cost (Int$) | |
| Diabetic foot treatment | 12,994 | 306.1 | 3,976,997 | |
| Amputation/disarticulation of lower limbs | 3318 | 1097.5 | 3,641,671 | |
| Amputation/disarticulation of foot/tarsus | 1820 | 354.3 | 644,869 | |
| Surgical revision of lower limb amputation stump | 209 | 388.8 | 81,266 | |
| Amputation/disarticulation of toe | 3817 | 400.3 | 141,688,219 | |
| Surgical revision of toe amputation stump | 86 | 224.5 | 19,310 | |
| Sub-Total | 22,244 | 444.7 | 9,892,152 | |
| Complications related to Diabetic Foot Disease | ||||
| Ulcer | L97—Non-pressure chronic ulcer of lower limb, not elsewhere classified | 3545 | 527.5 | 1,870,290 |
| R02—Gangrene, not elsewhere classified | 15,419 | 668.9 | 10,313,991 | |
| Neuropathy | G57—Mononeuropathies of lower limb | 29 | 498.7 | 14,404 |
| G59.0—Mononeuropathy in diseases classified elsewhere | 5 | 163.6 | 817 | |
| G63—Polyneuropathy in diseases classified elsewhere | 276 | 382.3 | 105,460 | |
| Osteomyelitis | M86—Osteomyelitis | 5849 | 554.1 | 3,240,765 |
| M87.3—Other secondary osteonecrosis | 177 | 2710.2 | 480,326 | |
| M87.8—Other osteonecrosis | 125 | 2530.9 | 315,405 | |
| M87.9—Unspecified osteonecrosis | 168 | 1346.5 | 226,575 | |
| Amputation | S88—Traumatic amputation of lower leg | 439 | 1055.6 | 463,567 |
| S98—Traumatic amputation of ankle and foot | 2100 | 378.3 | 794,283 | |
| Sub-Total | 28,133 | 983.3 | 17,825,887 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toscano, C.M.; Sugita, T.H.; Rosa, M.Q.M.; Pedrosa, H.C.; Rosa, R.D.S.; Bahia, L.R. Annual Direct Medical Costs of Diabetic Foot Disease in Brazil: A Cost of Illness Study. Int. J. Environ. Res. Public Health 2018, 15, 89. https://doi.org/10.3390/ijerph15010089
Toscano CM, Sugita TH, Rosa MQM, Pedrosa HC, Rosa RDS, Bahia LR. Annual Direct Medical Costs of Diabetic Foot Disease in Brazil: A Cost of Illness Study. International Journal of Environmental Research and Public Health. 2018; 15(1):89. https://doi.org/10.3390/ijerph15010089
Chicago/Turabian StyleToscano, Cristiana M., Tatiana H. Sugita, Michelle Q. M. Rosa, Hermelinda C. Pedrosa, Roger Dos S. Rosa, and Luciana R. Bahia. 2018. "Annual Direct Medical Costs of Diabetic Foot Disease in Brazil: A Cost of Illness Study" International Journal of Environmental Research and Public Health 15, no. 1: 89. https://doi.org/10.3390/ijerph15010089
APA StyleToscano, C. M., Sugita, T. H., Rosa, M. Q. M., Pedrosa, H. C., Rosa, R. D. S., & Bahia, L. R. (2018). Annual Direct Medical Costs of Diabetic Foot Disease in Brazil: A Cost of Illness Study. International Journal of Environmental Research and Public Health, 15(1), 89. https://doi.org/10.3390/ijerph15010089