The Effect of Vitamin A on Fracture Risk: A Meta-Analysis of Cohort Studies


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
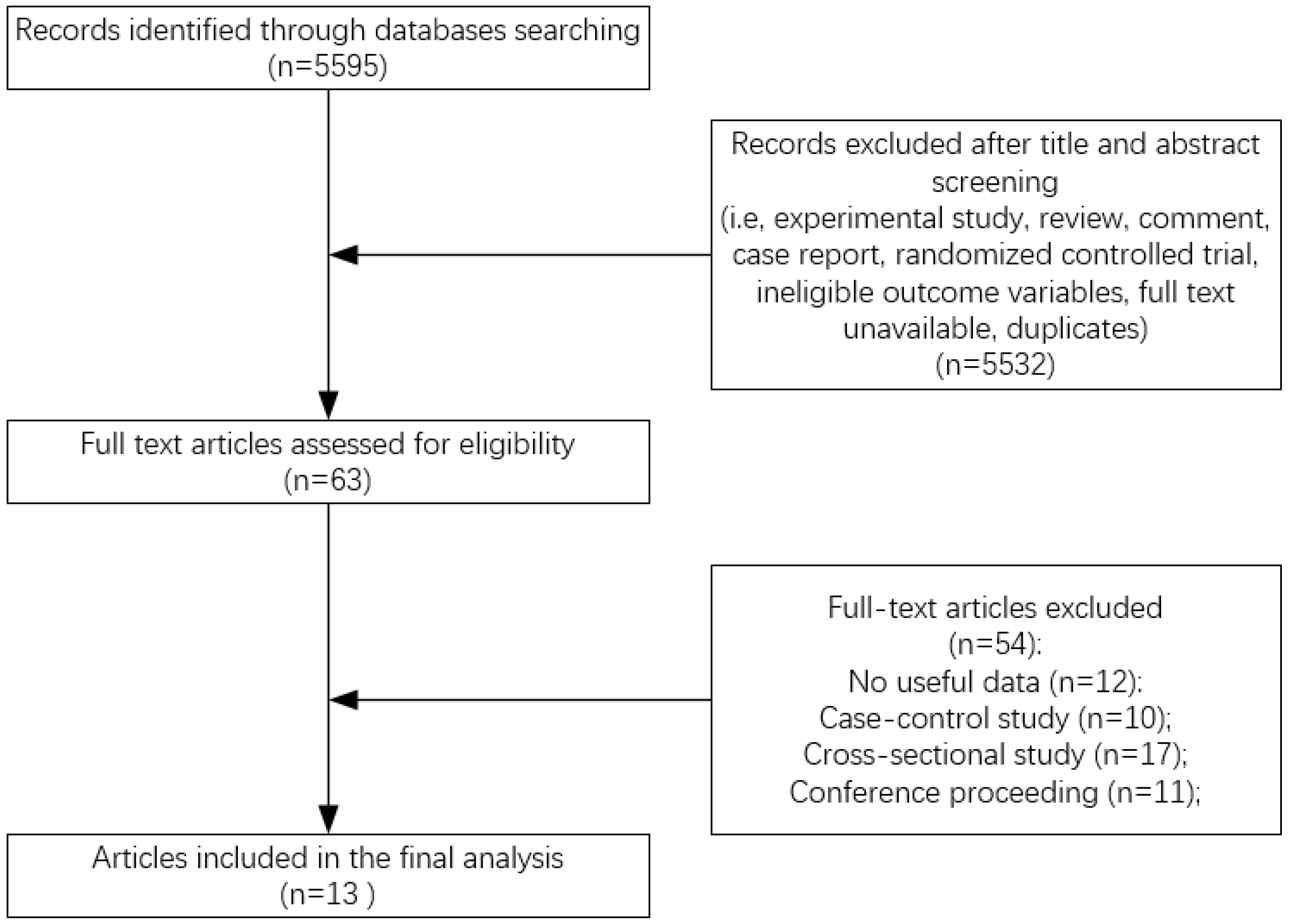
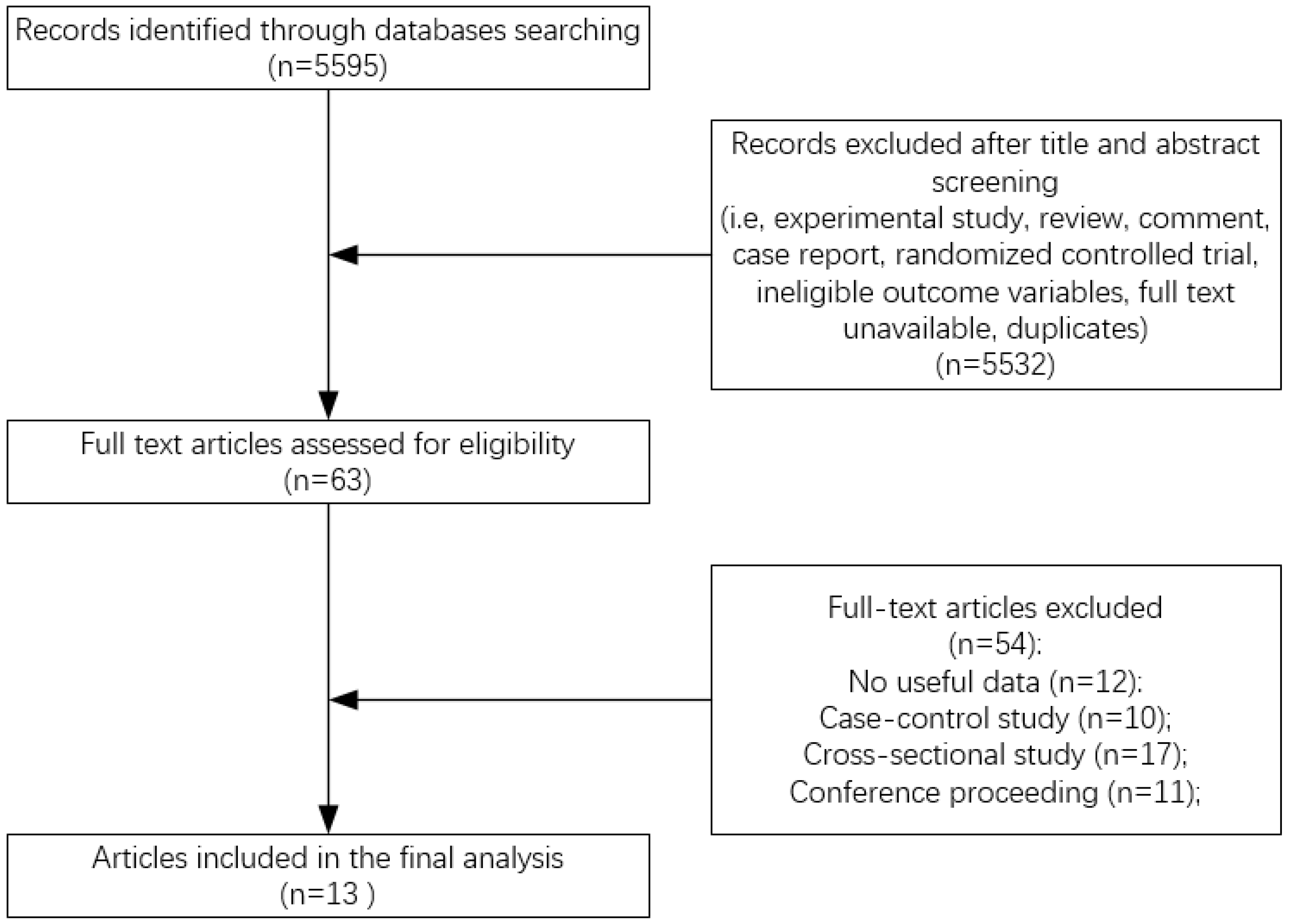
3.1. Literature Search
3.2. Study Characteristics
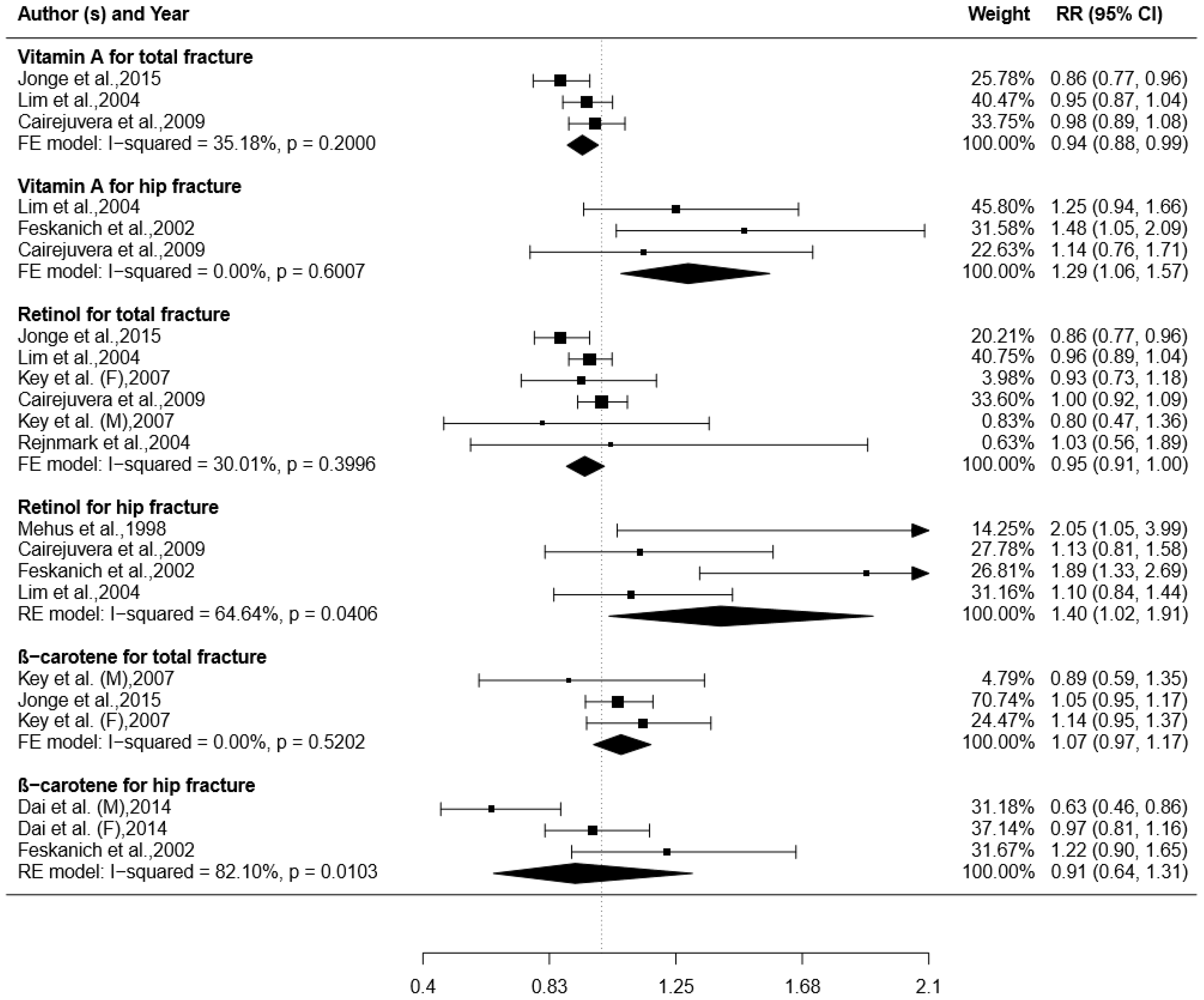
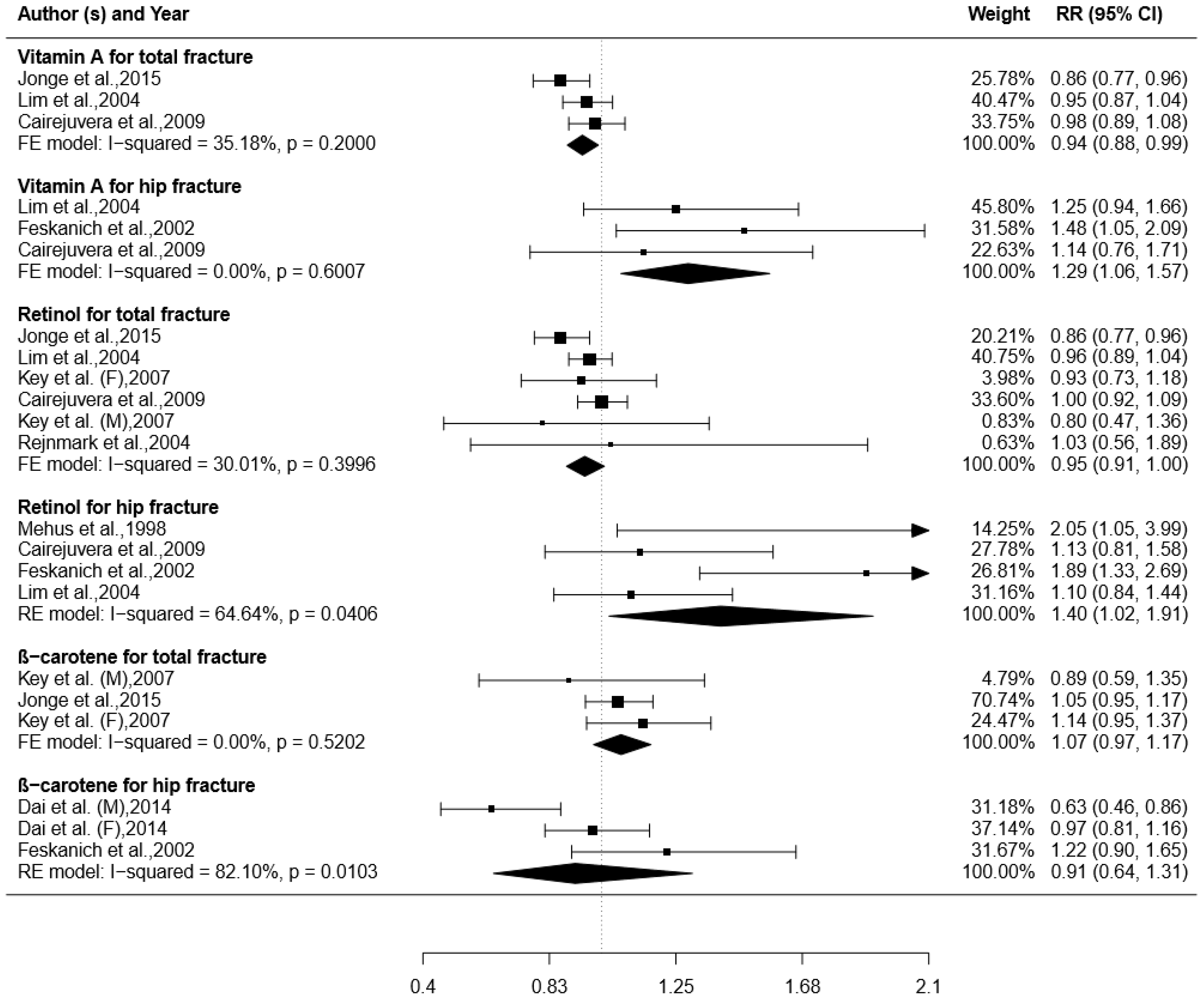
3.3. Total VA Intake and Risk of Fracture
3.4. Retinol Intake and Risk of Fracture
3.5. β-carotene Intake and Risk of Fracture
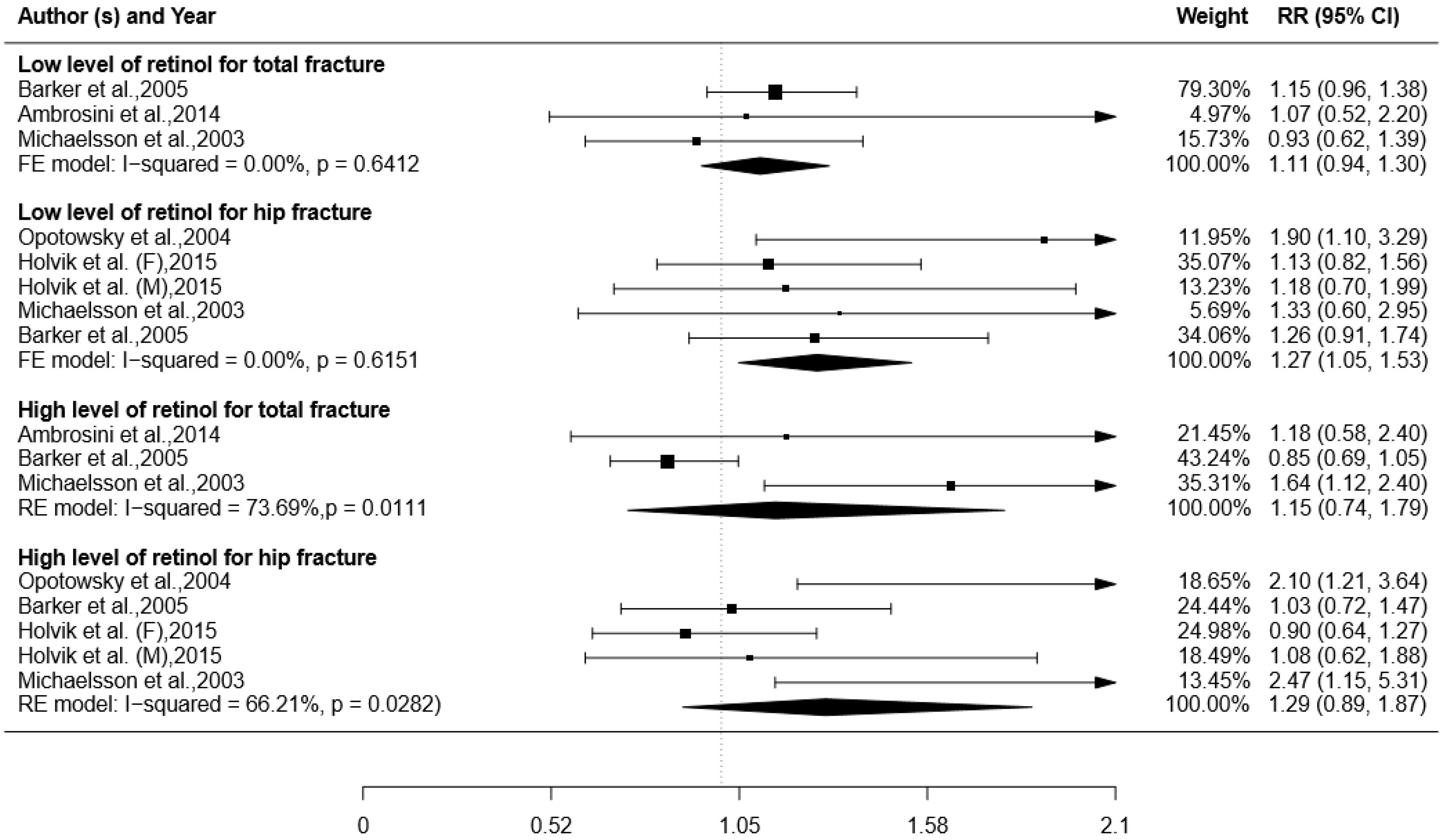
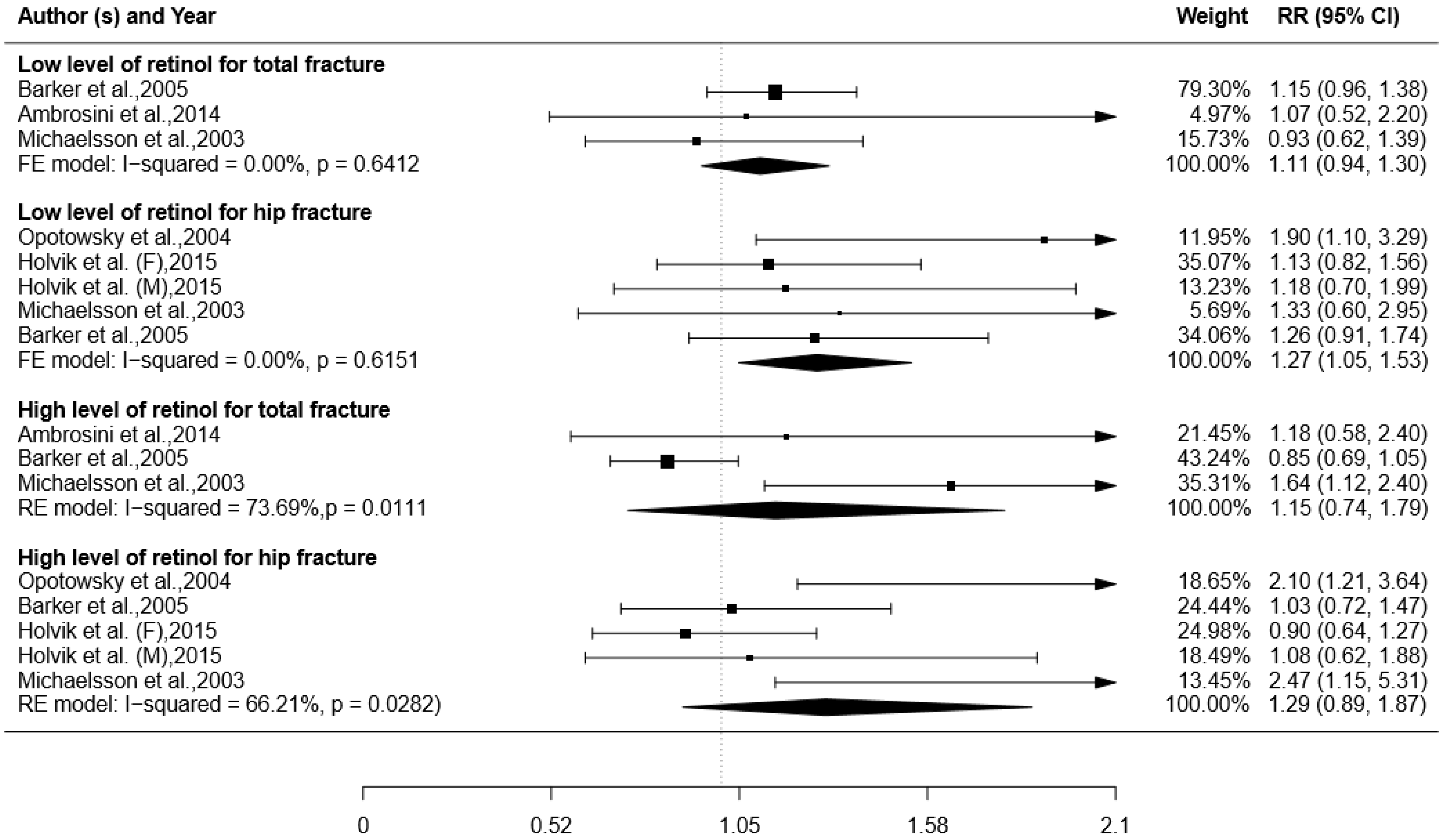
3.6. Blood Level of Retinol and Risk of Fracture
3.7. Subgroup Analysis, Sensitivity Analysis, and Publication Bias
4. Discussion
4.1. Higher Total VA or Retinol Intake may Decrease Total Fracture Risk but Increases Hip Fracture Risk
4.2. Subgroup Analysis for Retinol Intake and Total Fracture Risk
4.3. Higher β-Carotene Intake may Increase Total Fracture Risk
4.4. Lower Blood Level of Retinol may Increase Total and Hip Fracture Risk
4.5. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| FFQ | Food frequency questionnaire |
| HR | Hazard risk |
| NOS | Newcastle-Ottawa Scale |
| OR | Odds ratio |
| PSRMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RR | Relative risk |
| VA | Vitamin A |
References
- Listed, N. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Christodoulou, C.; Cooper, C. What is osteoporosis? Postgrad. Med. J. 2003, 79, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Pietschmann, P.; Rauner, M.; Sipos, W.; Kerschanschindl, K. Osteoporosis: An age-related and gender-specific disease—A mini-review. Gerontology 2009, 55, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Omsland, T.K.; Emaus, N.; Tell, G.S.; Magnus, J.H.; Ahmed, L.A.; Holvik, K.; Center, J.; Forsmo, S.; Gjesdal, C.G.; Schei, B. Mortality following the first hip fracture in Norwegian women and men (1999–2008). A NOREPOS study. Bone 2014, 63, 81. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Lourenço, Ó.; Silva, J.A.P.D. The burden of osteoporotic hip fractures in Portugal: Costs, health related quality of life and mortality. Osteoporos. Int. 2015, 26, 2623. [Google Scholar] [CrossRef] [PubMed]
- Budhia, S.; Mikyas, Y.; Tang, M.; Badamgarav, E. Osteoporotic fractures: A systematic review of U.S. healthcare costs and resource utilization. Pharmacoeconomics 2012, 30, 147. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O. The socioeconomic burden of fractures: Today and in the 21st century. Am. J. Med. 1997, 103, S20–S26. [Google Scholar] [CrossRef]
- Odén, A.; Mccloskey, E.V.; Kanis, J.A.; Harvey, N.C.; Johansson, H. Burden of high fracture probability worldwide: Secular increases 2010–2040. Osteoporos. Int. 2015, 26, 2243. [Google Scholar] [CrossRef] [PubMed]
- Hinds, T.S.; West, W.L.; Knight, E.M. Carotenoids and retinoids: A review of research, clinical, and public health applications. J. Clin. Pharmacol. 1997, 37, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.W.; Moore, T. Vitamin A and carotene. 11. The distribution of vitamin A in the organs of the normal and hypervitaminotic rat. Biochem. J. 1934, 28, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Krueger, D. Hypervitaminosis A and bone. Nutr. Rev. 2000, 58, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Togari, A.; Kondo, M.; Arai, M.; Matsumoto, S. Effects of retinoic acid on bone formation and resorption in cultured mouse calvaria. Gen. Pharmacol. Vasc. Syst. 1991, 22, 287–292. [Google Scholar] [CrossRef]
- Scheven, B.A.A.; Hamilton, N.J. Retinoic acid and 1,25-dihydroxyvitamin D 3 stimulate osteoclast formation by different mechanisms. Bone 1990, 11, 53–59. [Google Scholar] [CrossRef]
- Rohde, C.M.; Manatt, M.; Clagett-Dame, M.; DeLuca, H.F. Vitamin A antagonizes the action of vitamin D in rats. J. Nutr. 1999, 129, 2246–2250. [Google Scholar] [PubMed]
- White, S.C.; Atchison, K.A.; Gornbein, J.A.; Nattiv, A.; Paganini-Hill, A.; Service, S.K. Risk factors for fractures in older men and women: The Leisure World Cohort Study. Gend. Med. 2006, 3, 110–123. [Google Scholar] [CrossRef]
- Michaelsson, K.; Lithell, H.; Vessby, B.; Melhus, H. Serum retinol levels and the risk of fracture. N. Engl. J. Med. 2003, 348, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Alfonso, H.; Reid, A.; Mackerras, D.; Bremner, A.P.; Beilby, J.; Olsen, N.J.; Musk, A.W.; de Klerk, N.H. Plasma retinol and total carotenes and fracture risk after long-term supplementation with high doses of retinol. Nutrition 2014, 30, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Cairejuvera, G.; Ritenbaugh, C.; Wactawskiwende, J.; Snetselaar, L.G.; Chen, Z. Vitamin A and retinol intakes and the risk of fractures among participants of the Women’s Health Initiative Observational Study. Am. J. Clin. Nutr. 2009, 89, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Appleby, P.N.; Spencer, E.A.; Roddam, A.W.; Neale, R.E.; Allen, N.E. Calcium, diet and fracture risk: A prospective study of 1898 incident fractures among 34,696 British women and men. Public Health Nutr. 2007, 10, 1314–1320. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.S.; Harnack, L.J.; Lazovich, D.; Folsom, A.R. Vitamin A intake and the risk of hip fracture in postmenopausal women: The Iowa Women’s Health Study. Osteoporos. Int. 2004, 15, 552. [Google Scholar] [CrossRef] [PubMed]
- Jonge, E.A.L.D.; Jong, J.C.K.; Camposobando, N.; Booij, L.; Franco, O.H.; Hofman, A.; Uitterlinden, A.G.; Rivadeneira, F.; Zillikens, M.C. Dietary vitamin A intake and bone health in the elderly: The Rotterdam Study. Eur. J. Clin. Nutr. 2015, 69, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.E.; Mccloskey, E.; Saha, S.; Gossiel, F.; Charlesworth, D.; Powers, H.J.; Blumsohn, A. Serum retinoids and beta-carotene as predictors of hip and other fractures in elderly women. J. Bone Miner. Res. 2005, 20, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Yano, M. High Vitamin C Intake with High Serum β-Cryptoxanthin Associated with Lower Risk for Osteoporosis in Post-Menopausal Japanese Female Subjects: Mikkabi Cohort Study. J. Nutr. Sci. Vitaminol. 2016, 62, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. Protective effect of total carotenoid and lycopene intake on the risk of hip fracture: A 17-year follow-up from the Framingham osteoporosis study. J. Bone Miner. Res. 2009, 24, 1086. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Wang, R.; Ang, L.W.; Low, Y.L.; Yuan, J.M.; Koh, W.P. Protective effects of dietary carotenoids on risk of hip fracture in men: The Singapore Chinese Health Study. J. Bone Miner. Res. 2014, 29, 408. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Singh, V.; Willett, W.C.; Colditz, G.A. Vitamin A intake and hip fractures among postmenopausal women. JAMA 2002, 287, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Alessandro, L.; Douglas, G.A.; Jennifer, T.; Cynthia, M.; Peter, C.G.; John, P.A.; Mike, C.; Devereaux, P.J.; Jos, K.; David, M. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare intervention: Explanation and elaboration. PLoS Med. 2009, 6, e1–e34. [Google Scholar]
- Wells, G.A.; Shea, B.J.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Appl. Eng. Agric. 2014, 18, 727–734. [Google Scholar]
- Zhang, J.; Yu, K.F. What′s the Relative Risk? JAMA 1998, 280, 1690. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for systematic reviews of interventions. In Naunyn-Schmiedebergs Archiv Für Experimentelle Pathologie und Pharmakologie; John Wiley & Sons, Ltd.: Chichester, UK, 2006; p. S38. [Google Scholar]
- Dersimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Mantel, N.; Haenszel, W. Statistical Aspects of the Analysis of Data from Retrospective Studies of Disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [PubMed]
- Dersimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, A.C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed]
- Melhus, H.; Michaelsson, K.; Kindmark, A.; Bergstrom, R.; Holmberg, L.; Mallmin, H.; Wolk, A.; Ljunghall, S. Excessive dietary intake of vitamin A is associated with reduced bone mineral density and increased risk for hip fracture. Ann. Int. Med. 1998, 129, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Rejnmark, L.; Vestergaard, P.; Charles, P.; Hermann, A.P.; Brot, C.; Eiken, P.; Mosekilde, L. No effect of vitamin A intake on bone mineral density and fracture risk in perimenopausal women. Osteoporos. Int. 2004, 15, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Holvik, K.; Ahmed, L.A.; Forsmo, S.; Gjesdal, C.G.; Grimnes, G.; Samuelsen, S.O.; Schei, B.; Blomhoff, R.; Tell, G.S.; Meyer, H.E. No increase in risk of hip fracture at high serum retinol concentrations in community-dwelling older Norwegians: The Norwegian Epidemiologic Osteoporosis Studies. Am. J. Clin. Nutr. 2015, 102, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Opotowsky, A.R.; Bilezikian, J.P. Serum vitamin A concentration and the risk of hip fracture among women 50 to 74 years old in the United States: A prospective analysis of the NHANES I follow-up study. Am. J. Med. 2004, 117, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Hough, S.; Avioli, L.V.; Muir, H.; Gelderblom, D.; Jenkins, G.; Kurasi, H.; Slatopolsky, E.; Bergfeld, M.A.; Teitelbaum, S.L. Effects of hypervitaminosis A on the bone and mineral metabolism of the rat. Endocrinology 1988, 122, 2933–2939. [Google Scholar] [CrossRef] [PubMed]
- Frankel, T.L.; Seshadri, M.S.; Mcdowall, D.B.; Cornish, C.J. Hypervitaminosis A and calcium-regulating hormones in the rat. J. Nutr. 1986, 116, 578–587. [Google Scholar] [PubMed]
- Karamati, M.; Yousefian-Sanni, M.; Shariati-Bafghi, S.E.; Rashidkhani, B. Major Nutrient Patterns and Bone Mineral Density among Postmenopausal Iranian Women. Calcif. Tissue Int. 2014, 94, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Maggio, D.; Barabani, M.; Pierandrei, M.; Polidori, M.C.; Catani, M.; Mecocci, P.; Senin, U.; Pacifici, R.; Cherubini, A. Marked decrease in plasma antioxidants in aged osteoporotic women: Results of a cross-sectional study. J. Clin. Endocrinol. Metab. 2003, 88, 1523–1527. [Google Scholar] [CrossRef] [PubMed]
- Lind, P.M.; Larsson, S.; Johansson, S.; Melhus, H.; Wikström, M.; Lindhe, O.; Orberg, J. Bone tissue composition, dimensions and strength in female rats given an increased dietary level of vitamin A or exposed to 3,3′,4,4′,5-pentachlorobiphenyl (PCB126) alone or in combination with vitamin, C. Toxicology 2000, 151, 11–23. [Google Scholar] [CrossRef]
- Houtkooper, L.B.; Ritenbaugh, C.; Aickin, M.; Lohman, T.G.; Going, S.B.; Weber, J.L.; Greaves, K.A.; Boyden, T.W.; Pamenter, R.W.; Hall, M.C. Nutrients, body composition and exercise are related to change in bone mineral density in premenopausal women. J. Nutr. 1995, 125, 1229–1237. [Google Scholar] [PubMed]
- Green, A.C.; Martin, T.J.; Purton, L.E. The role of vitamin A and retinoic acid receptor signaling in post-natal maintenance of bone. J. Steroid Biochem. Mol. Biol. 2016, 155, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Promislow, J.H.; Goodman-Gruen, D.; Slymen, D.J.; Barrett-Connor, E. Retinol Intake and Bone Mineral Density in the Elderly: The Rancho Bernardo Study. Am. J. Epidemiol. 2002, 17, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M.; Huang, C.Q.; Lin, Z.K.; Tian, N.F.; Ni, W.F.; Wang, X.Y.; Xu, H.Z.; Chi, Y.L. The relationship between vitamin A and risk of fracture: meta-analysis of prospective studies. J. Bone Miner. Res. 2014, 29, 2032. [Google Scholar] [CrossRef] [PubMed]
- Schlecht, S.H.; Bigelow, E.M.R.; Jepsen, K.J. How Does Bone Strength Compare Across Sex, Site, and Ethnicity? Clin. Orthop. Relat. Res. 2015, 473, 2540–2547. [Google Scholar] [CrossRef] [PubMed]
- Oyster, N. Sex differences in cancellous and cortical bone strength, bone mineral content and bone density. Age Ageing 1992, 21, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Fotopoulos, A.; Georgiou, A.; Xourgia, X.; Papadopoulos, A.; Kalefezra, J.A. Age at menarche, age at menopause and duration of fertility as risk factors for osteoporosis. Climacteric 2010, 13, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Bush, T.L.; Miller, S.R.; Golden, A.L.; Hale, W.E. Self-report and medical record report agreement of selected medical co. Am. J. Public Health 2011, 79, 1554. [Google Scholar] [CrossRef]
- Zhang, J.; Munger, R.G.; West, N.A.; Cutler, D.R.; Wengreen, H.J.; Corcoran, C.D. Antioxidant intake and risk of osteoporotic hip fracture in Utah: An effect modified by smoking status. Am. J. Epidemiol. 2006, 163, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.E.; Cho, S.H.; Park, H.M.; Chang, Y.K. Relationship between bone mineral density and dietary intake of β-carotene, vitamin C, zinc and vegetables in postmenopausal Korean women: A cross-sectional study. J. Int. Med. Res. 2016, 44, 1103–1114. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.L.; Cauley, J.A.; Pettinger, M.; Jackson, R.; Lacroix, A.; Leboff, M.S.; Lewis, C.E.; Nevitt, M.C.; Simon, J.A.; Stone, K.L. Lack of a relation between vitamin and mineral antioxidants and bone mineral density: Results from the Women’s Health Initiative. Am. J. Clin. Nutr. 2005, 82, 581. [Google Scholar] [PubMed]
- Melhus, H.; Michaëlsson, K.; Holmberg, L.; Wolk, A.; Ljunghall, S. Smoking, Antioxidant Vitamins, and the Risk of Hip Fracture. J. Bone Miner. Res. 1999, 14, 129. [Google Scholar] [CrossRef] [PubMed]
- Andersson, E.; Vahlquist, A.; Rosdahl, I. Beta-carotene uptake and bioconversion to retinol differ between human melanocytes and keratinocytes. Nutr. Cancer 2001, 39, 300. [Google Scholar] [CrossRef] [PubMed]
- Hickenbottom, S.J.; Follett, J.R.; Lin, Y.; Dueker, S.R.; Burri, B.J.; Neidlinger, T.R.; Clifford, A.J. Variability in conversion of beta-carotene to vitamin A in men as measured by using a double-tracer study design. Am. J. Clin. Nutr. 2002, 75, 900–907. [Google Scholar] [PubMed]
- Tadaishi, M.; Nishide, Y.; Tousen, Y.; Kruger, M.C.; Ishimi, Y. Cooperative effects of soy isoflavones and carotenoids on osteoclast formation. J. Clin. Biochem. Nutr. 2014, 54, 109. [Google Scholar] [CrossRef] [PubMed]
- Haider, C.; Ferk, F.; Bojaxhi, E.; Martano, G.; Stutz, H.; Bresgen, N.; Knasmüller, S.; Alija, A.; Eckl, P.M. Effects of β-Carotene and Its Cleavage Products in Primary Pneumocyte Type II Cells. Antioxidants 2017, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Navia, J.M.; Harris, S.S. Vitamin A influence on calcium metabolism and calcification. Ann. N. Y. Acad. Sci. 1980, 355, 45. [Google Scholar] [CrossRef] [PubMed]
- Bedo, G.; Santisteban, P.; Aranda, A. Retinoic acid regulates growth hormone gene expression. Nature 1989, 339, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.D.; Rose, A.; Craft, N.; Seidel, K.E.; Smith, J.C., Jr. Concentrations of carotenoids, retinol, and tocopherol in plasma, in response to ingestion of a meal. Clin. Chem. 1989, 35, 310–312. [Google Scholar] [PubMed]
- Stephensen, C.B.; Gildengorin, G. Serum retinol, the acute phase response, and the apparent misclassification of vitamin A status in the third National Health and Nutrition Examination Survey. Am. J. Clin. Nutr. 2000, 72, 1170–1178. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author Year [ref.] | Country Period | Male/Female Age Case | Range of Exposure | Exposure Assessment | Case Ascertainment | Adjusted Variables | Quality Score |
|---|---|---|---|---|---|---|---|
| Feskanich et al., 2002 [26] | U.S. 1980–1998 | 0/72,337 34–77 Hip: 603 | Total VA μg RE/day | FFQ | Self-report | 1, 2, 3, 4, 9, 10, 11, 12, 14, 15, 17, 18, 23 | 8 |
| <1250; 1250–1699; 1700–2249; 2250–2999; ≥3000 | |||||||
| Retinol μg/day | |||||||
| <500; 500–849; 850–1299; 1300–1999; ≥2000 | |||||||
| β-carotene μg/day | |||||||
| <2550; 2550–3549; 3550–4669; 4650–6299; ≥6300 | |||||||
| Melhus et al., 1998 [35] | SE 1987–1990 | 0/1120 40–76 Hip: 247 | Retinol μg/day | FFQ | Medical records | 2, 5, 8, 9, 11, 12, 16, 17, 20, 32 | 7 |
| ≤500; 500–1000; 1000–1500; >1500 | |||||||
| Lim et al., 2004 [21] | US 1985–1997 | 0/34,703 55–69 Total: 6502 Hip: 525 | Total VA IU | FFQ | Self-report | 1, 2, 7, 8, 10, 17, 19, 20, 24 | 6 |
| 221–7055; 7056–10484; 10,485–14,209; 14,210–19,892; 19,893–23,6991 | |||||||
| Retinol IU | |||||||
| 28–1405; 1406–2952; 2953–4655; 4656–7001; 7002–211,051 | |||||||
| Key et al., 2007 [20] | UK 1993–2005 | 7947/26,749 20–89 Total: 1898 | Retinol μg/day | FFQ | Self-report | 1, 2, 3, 4, 8, 9, 10, 11, 14, 22, 25, 26, 27, women for 21 and 12 | 8 |
| <200; 200–299; 300–499; 450–999; ≥1000 | |||||||
| β-carotene μg/day | |||||||
| <2000; 2000–2999; 3000–3999; 4000–4499; ≥5000 | |||||||
| Dai et al., 2014 [25] | SG 1993–2010 | 27,959/35,298 45–74 Hip: 1630 | β-carotene 1000 kcal/day | FFQ | Medical records | 1, 2, 4, 7, 8, 9,11, 12, 13, 20, 29, 30, 31, 32 | 8 |
| <850.4; 580.4–1235.4; 1235.4–1772.4; ≥1772.4 | |||||||
| Cairejuvera et al., 2009 [19] | U.S. 1993–2005 | 0/93676 50–79 Total: 10,405 Hip: 588 | Total VA μg RE/day | FFQ | Self-report for total; Medical records for hip | 1, 2, 3, 4, 8, 9, 10, 11, 12, 14, 15, 18, 28, 31 | 8 |
| <5055; 5055–5824; 5825–6550; 6551–7507; ≥7508 | |||||||
| Retinol μg/day | |||||||
| <474; 474–764; 765–1092; 1093–1425; ≥1426 | |||||||
| Rejnmark et al., 2004 [36] | DK 5 years | 0/2016 45–58 Total: 163 | Retinol μg/day | FFQ | Medical records | 1, 3, 4, 5, 6, 8, 9, 10, 11, 16, 17, 33, 34, 35, 36 | 8 |
| <500; 500–1500; >1500 | |||||||
| Jonge et al., 2015 [16] | NED 1989–2007 | 2172/3116 ≥ 50 | Total VA μg RE/day | FFQ | Medical records | 1, 2, 4, 5, 7, 9, 10, 11, 12, 37, 38, 39 | 7 |
| 568–793; 867–1052; 1050–1257; 1263–1551; 1712–2485 | |||||||
| Retinol μg/day | |||||||
| 135–289; 173–384; 212–523; 272–734; 594–1518 | |||||||
| β-carotene μg/day | |||||||
| 1845–2909; 2942–3964; 3336–4575; 3586–5461; 3771–6586 |
| Author Year [ref.] | Country Period | Population/Age Case | Category of Blood Retinol (μmol/L) | Exposure Assessment | Case Ascertainment | Adjusted Variables | Quality Score |
|---|---|---|---|---|---|---|---|
| Michaelsson et al., 2003 [17] | SE 1970–2001 | 2322/49–51 Total: 266 Hip: 84 | The lowest: <1.95 The highest: >2.64 | High-performance liquid chromatography | Medical records | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12 | 9 |
| Ambrosini et al., 2014 [18] | AU 1990–2007 | 998/39–62 Total: 123 | The lowest: ≤2.80 The highest: ≥19.3 | High-performance liquid chromatography | Self-reported | 1, 8, 13,14, 15 | 6 |
| Holvik et al., 2015 [37] | NO 1994–2008 | 2487/65–79 Hip: 1154 | The lowest: ≤2.12 The highest: >3.63 | High-performance liquid chromatography | Medical records | 1, 2, 16, 17 | 8 |
| Barker et al., 2005 [22] | UK 1996–2002 | 2606/≥75 Total: 312 Hip: 192 | The lowest: ≤1.66 The highest: ≥2.42 | High-performance liquid chromatography | Medical records | Total: 1, 18 Hip: 1, 3, 18 | 8 |
| Opotowsky et al., 2004 [38] | U.S. 1971–1992 | 0/3571 50–74 Hip: 172 | The lowest: ≤1.61 The highest: ≥2.56 | - | Medical records | 1, 3, 7, 11, 12, 14, 15, 19, 20 | 8 |
| Exposure | Subgroup | Number of Studies | RR (95% CI) | Q | p-Q | I2 (%) |
|---|---|---|---|---|---|---|
| Sex | Men | 1 | 0.80 (0.47, 1.36) | 0.00 | 1.00 | - |
| Women | 4 | 0.98 (0.92, 1.03) | 0.69 | 0.88 | 0.00% | |
| All | 1 | 0.86 (0.77, 0.96) | 0.00 | 1.00 | - | |
| Region | USA | 2 | 0.98 (0.92, 1.03) | 0.50 | 0.48 | 0.00% |
| Europe | 4 | 0.87 (0.79, 0.96) | 0.70 | 0.87 | 0.00% | |
| Case ascertainment | Self-report | 4 | 0.97 (0.92, 1.03) | 1.19 | 0.76 | 0.00% |
| Medical record | 2 | 0.87 (0.78, 0.96) | 0.32 | 0.57 | 0.00% | |
| Education level | Adjusted | 2 | 0.93 (0.90, 0.97) | 2.55 | 0.11 | 60.83% |
| Unadjusted | 4 | 0.99 (0.91, 1.07) | 0.94 | 0.82 | 0.00% | |
| Age at menopause | Adjusted | 2 | 0.87 (0.78, 0.96) | 0.32 | 0.57 | 0.00% |
| Unadjusted | 4 | 0.97 (0.92, 1.03) | 1.19 | 0.76 | 0.00% | |
| Vitamin D intake | Adjusted | 3 | 0.95 (0.87, 1.02) | 4.63 | 0.099 | 58.31% |
| Unadjusted | 3 | 0.92 (0.75, 1.13) | 0.40 | 0.82 | 0.00% |
| Group | Omitted Study | RR (95% CI) | Q | p-Q | I2 (%) | Z-Egger | p-Egger |
|---|---|---|---|---|---|---|---|
| Total VA intake for total fracture | Cairejuvera et al., [19] | 0.93 (0.86, 1.00) | 3.03 | 0.08 | 67.01% | −1.3982 | 0.16 |
| Lim et al., [21] | 0.96 (0.90, 1.03) | 0.22 | 0.64 | 0.00% | |||
| Feskanich et al., [26] | 0.91 (0.85, 0.98) | 1.89 | 0.17 | 47.11% | |||
| Total VA for hip fracture | Jonge et al., [16] | 1.34 (1.08, 1.67) | 0.55 | 0.46 | 0.00% | −0.1893 | 0.85 |
| Cairejuvera et al., [19] | 1.21 (0.96, 1.53) | 0.13 | 0.72 | 0.00% | |||
| Lim et al., [21] | 1.33 (1.02, 1.72) | 0.93 | 0.34 | 0.00% | |||
| Retinol intake for total fracture | Jonge et al., [16] | 0.95 (0.90, 1.00) | 5.07 | 0.28 | 36.04% | 0.6236 | 0.53 |
| Cairejuvera et al., [19] | 0.95 (0.91, 1.00) | 5.10 | 0.28 | 39.45% | |||
| Key et al. (M), [20] | 0.95 (0.91, 1.00) | 4.73 | 0.32 | 34.86% | |||
| Key et al. (F), [20] | 0.93 (0.87, 0.98) | 2.96 | 0.56 | 20.26% | |||
| Lim et al., [21] | 0.97 (0.92, 1.03) | 1.22 | 0.87 | 0.00% | |||
| Rejnmark et al., [36] | 0.94 (0.89, 1.00) | 5.02 | 0.29 | 37.52% | |||
| Retinol intake for hip fracture | Cairejuvera et al., [19] | 1.54 (1.02, 2.33) | 7.13 | 0.028 | 69.57% | 1.3639 | 0.17 |
| Lim et al., [21] | 1.57 (1.06, 2.31) | 5.29 | 0.07 | 60.93% | |||
| Feskanich et al., [26] | 1.17 (0.96, 1.43) | 2.96 | 0.23 | 0.01% | |||
| Melhus et al., [35] | 1.31 (0.94, 1.84) | 6.48 | 0.039 | 70.25% | |||
| β-carotene intake for total fracture | Jonge et al., [16] | 1.04 (0.94, 1.16) | 0.61 | 0.44 | 0.00% | −0.4368 | 0.66 |
| Key et al. (F), [20] | 1.08 (0.98, 1.18) | 0.54 | 0.46 | 0.00% | |||
| Key et al. (M), [20] | 1.09 (0.93, 1.29) | 1.16 | 0.28 | 14.10% | |||
| β-carotene intake for hip fracture | Dai et al. (M), [25] | 0.88 (0.46, 1.68) | 8.76 | 0.03 | 88.59% | −0.2493 | 0.80 |
| Dai et al. (F), [25] | 1.05 (0.85, 1.30) | 1.62 | 0.20 | 38.10% | |||
| Feskanich et al., [26] | 0.80 (0.52, 1.22) | 5.45 | 0.02 | 81.64% | |||
| High level of blood retinol for total fracture | Michaelsson et al., [17] | 0.87 (0.71, 1.07) | 0.75 | 0.39 | 0.00% | 0.4619 | 0.64 |
| Ambrosini et al., [18] | 1.16 (0.61, 2.20) | 8.78 | 0.003 | 88.61% | |||
| Barker et al., [22] | 1.52 (1.09, 2.13) | 0.64 | 0.42 | 0.00% | |||
| High level of blood retinol for hip fracture | Michaelsson et al., [17] | 1.15 (0.82, 1.61) | 6.78 | 0.079 | 57.69% | 2.7952 | 0.005 |
| Barker et al., [22] | 1.41 (0.87, 2.29) | 10.27 | 0.016 | 70.12% | |||
| Holvik et al. (M), [37] | 1.37 (0.85, 2.21) | 10.79 | 0.013 | 76.05% | |||
| Holvik et al. (F), [37] | 1.46 (0.95, 2.24) | 7.67 | 0.053 | 61.11% | |||
| Opotowsky et al., [38] | 1.08 (0.84, 1.40) | 5.62 | 0.13 | 23.13% | |||
| Low level of blood retinol for total fracture | Michaelsson et al., [17] | 1.15 (0.96, 1.36) | 0.04 | 0.85 | 0.00% | −0.6384 | 0.52 |
| Ambrosini et al., [18] | 1.11 (0.94, 1.31) | 0.88 | 0.35 | 0.00% | |||
| Barker et al., [22] | 0.96 (0.68, 1.37) | 0.11 | 0.74 | 0.00% | |||
| Low level of blood retinol for hip fracture | Michaelsson et al., [17] | 1.26 (1.04, 1.54) | 2.65 | 0.45 | 0.00% | 0.8156 | 0.41 |
| Barker et al., [22] | 1.27 (1.01, 1.60) | 2.66 | 0.45 | 0.00% | |||
| Holvik et al. (F), [37] | 1.35 (1.06, 1.71) | 1.92 | 0.59 | 0.00% | |||
| Holvik et al. (M), [37] | 1.28 (1.04, 1.57) | 2.58 | 0.46 | 0.00% | |||
| Opotowsky et al., [38] | 1.20 (0.98, 1.47) | 0.29 | 0.96 | 0.00% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Zhang, R.; Moore, J.B.; Wang, Y.; Yan, H.; Wu, Y.; Tan, A.; Fu, J.; Shen, Z.; Qin, G.; et al. The Effect of Vitamin A on Fracture Risk: A Meta-Analysis of Cohort Studies. Int. J. Environ. Res. Public Health 2017, 14, 1043. https://doi.org/10.3390/ijerph14091043
Zhang X, Zhang R, Moore JB, Wang Y, Yan H, Wu Y, Tan A, Fu J, Shen Z, Qin G, et al. The Effect of Vitamin A on Fracture Risk: A Meta-Analysis of Cohort Studies. International Journal of Environmental Research and Public Health. 2017; 14(9):1043. https://doi.org/10.3390/ijerph14091043
Chicago/Turabian StyleZhang, Xinge, Rui Zhang, Justin B. Moore, Yueqiao Wang, Hanyi Yan, Yingru Wu, Anran Tan, Jialin Fu, Ziqiong Shen, Guiyu Qin, and et al. 2017. "The Effect of Vitamin A on Fracture Risk: A Meta-Analysis of Cohort Studies" International Journal of Environmental Research and Public Health 14, no. 9: 1043. https://doi.org/10.3390/ijerph14091043
APA StyleZhang, X., Zhang, R., Moore, J. B., Wang, Y., Yan, H., Wu, Y., Tan, A., Fu, J., Shen, Z., Qin, G., Li, R., & Chen, G. (2017). The Effect of Vitamin A on Fracture Risk: A Meta-Analysis of Cohort Studies. International Journal of Environmental Research and Public Health, 14(9), 1043. https://doi.org/10.3390/ijerph14091043