
Mercury in Children: Current State on Exposure through Human Biomonitoring Studies


Abstract
:1. Background
2. Sources of Exposure
3. Biomarkers of Exposure
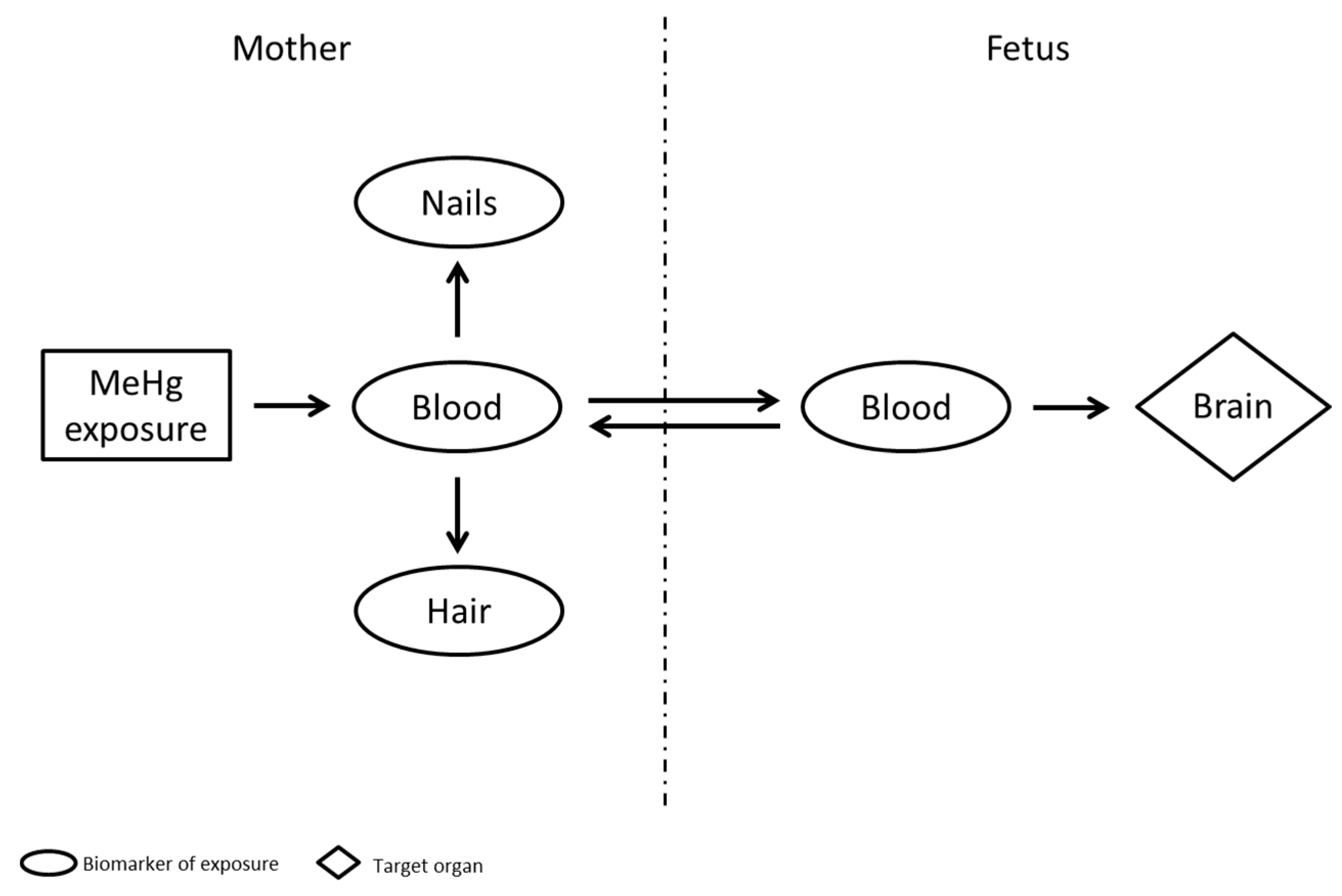
3.1. Methylmercury
3.2. Ethylmercury
3.3. Inorganic and Elemental Mercury
4. Health-Based Guidance Values for Hg
5. Cross-Sectional HBM Data
5.1. Mercury Level in Hair
5.2. Mercury Level in Blood
5.3. Mercury Level in Urine
6. Birth Cohort HBM Studies
7. Conclusions
Author Contributions
Conflicts of Interest
References
- Selevan, S.G.; Kimmel, C.A.; Mendola, P. Windows of susceptibility to environmental exposures in children. In Children’s Health and the Environment—A Global Perspective; Pronczuk-Garbino, J., Ed.; World Health Organization Press: Geneva, Switzerland, 2005; pp. 17–26. [Google Scholar]
- Bose-O’Reilly, S.; McCarty, K.M.; Steckling, N.; Lettmeier, B. Mercury Exposure and Children’s Health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 186–215. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Europe. Parma Declaration on Environment and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2010; Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/78608/E93618.pdf (accessed on 23 February 2017).
- US Department of Health and Human Services, Public Health Service, ATSDR. Toxicological Profile for Mercury; US Department of Health and Human Services: Atlanta, GA, USA, 1999; pp. 1–600. Available online: www.atsdr.cdc.gov/toxprofiles/tp46-p.pdf (accessed on 23 February 2017).
- Dórea, J.G.; Farina, M.; Rocha, J.T.B. Toxicity of ethylmercury (and Thimerosal): A comparison with methylmercury. J. Appl. Toxicol. 2013, 33, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; White, R. Neurodevelopmental disorders. In Children’s Health and Environment: A Review of Evidence; Tamburlini, G., von Ehrenstein, O.S., Bertollini, R., Eds.; WHO Regional Office for Europe: Copenhagen, Denmark, 2002; pp. 66–78. [Google Scholar]
- Rice, D.; Barone, S., Jr. Critical periods of vulnerability for the developing nervous system: Evidence from humans and animal models. Environ. Health Perspect. 2000, 108, 511–533. [Google Scholar] [CrossRef] [PubMed]
- Engleson, G.; Herner, T. Alkyl mercury poisoning. Acta Paediatr. 1952, 41, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Social Scientific Study Group on Minamata Disease (SSSGMD). In The Hope of Avoiding Repetition of Tragedy of Minamata Disease; National Institute for Minamata Disease: Minamata, Japan, 1999. Available online: http://www.nimd.go.jp/syakai/webversion/SSSGMDreport.html (accessed on 23 February 2017).
- Bakir, F.; Damluji, S.F.; Amin-Zaki, L.; Murtadha, M.; Khalidi, A.; Al-Rawi, N.Y.; Tikriti, S.; Dahahir, H.I.; Clarkson, T.W.; Smith, J.C.; et al. Methylmercury poisoning in Iraq. Science 1973, 181, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Spyker, J.M.; Sparber, S.B.; Goldberg, A.M. Subtle consequences of methylmercury exposure: Behavioral deviations in offspring of treated mothers. Science 1972, 177, 621–623. [Google Scholar] [CrossRef] [PubMed]
- Harada, M. Congenital Minamata disease: Intrauterine methylmercury poisoning. Teratology 1978, 18, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Marsh, D.O.; Myers, G.J.; Clarkson, T.W.; Amin-Zaki, L.; Tikriti, S.; Majeed, M.A. Fetal methylmercury poisoning: Clinical and toxicological data on 29 cases. Ann. Neurol. 1980, 7, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Harada, M. Minamata disease: Methylmercury poisoning in Japan caused by environmental pollution. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Kjellström, T.; Kennedy, P.; Wallis, S.; Mantell, C. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish; Stage 1: Preliminary Tests at Age 4; Report 3080; National Swedish Environmental Protection Board: Solna, Sweden, 1986. [Google Scholar]
- Grandjean, P.; Weihe, P.; Jorgensen, P.J.; Clarkson, T.; Cernichiari, E.; Videro, T. Impact of maternal seafood diet on fetal exposure to mercury, selenium, and lead. Arch. Environ. Health 1992, 47, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sørensen, N.; Dahl, R.; Jørgensenm, P.J. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Grandjean, P.; Budtz-Jørgensen, E.; White, R.F.; Jørgensen, P.J.; Weihe, P.; Debes, F.; Keiding, N. Methylmercury exposure biomarkers as indicators of neurotoxicity in children aged 7 years. Am. J. Epidemiol. 1999, 150, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Shamlaye, C.F.; Marsh, D.O.; Myers, G.J.; Cox, C.; Davidson, P.W.; Choisy, O.; Cernichiari, E.; Choi, A.; Tanner, M.A.; Clarkson, T.W. The Seychelles child development study on neurodevelopmental outcomes in children following in utero exposure to methylmercury from a maternal fish diet: Background and demographics. Neurotoxicology 1995, 16, 597–612. [Google Scholar] [PubMed]
- Myers, G.J.; Marsh, D.O.; Davidson, P.W.; Cox, C.; Shamlaye, C.F.; Tanner, M.A.; Choi, A.; Cernichiari, E.; Choisy, E.; Clarkson, T.W. Main neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from a maternal fish diet: Outcome at six months. Neurotoxicology 1995, 16, 653–664. [Google Scholar] [PubMed]
- Myers, G.J.; Davidson, P.W.; Shamlaye, C.F.; Axtell, C.D.; Cernichiari, E.; Choisy, O.; Choi, A.; Cox, C.; Clarkson, T.W. Effects of prenatal methylmercury exposure from a high fish diet on developmental milestones in the Seychelles Child Development Study. Neurotoxicology 1997, 18, 819–829. [Google Scholar] [PubMed]
- Myers, G.J.; Davidson, P.W.; Cox, C.; Shamlaye, C.F.; Palumbo, D.; Cernichiari, E.; Sloane-Reeves, J.; Wilding, G.E.; Kost, J.; Huang, L.S.; et al. Prenatal methylmercury exposure from ocean fish consumption in the Seychelles child development study. Lancet 2003, 361, 1686–1692. [Google Scholar] [CrossRef]
- Davidson, P.W.; Myers, G.J.; Cox, C.; Shamlaye, C.F.; Marsh, D.O.; Tanner, M.A.; Berlin, M.; Sloane-Reeves, J.; Cernichiari, E.; Choisy, O. Longitudinal neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from maternal fish ingestion: Outcomes at 19 and 29 months. Neurotoxicology 1995, 16, 677–688. [Google Scholar] [PubMed]
- Davidson, P.W.; Myers, G.J.; Cox, C.; Axtell, C.; Shamlaye, C.; Sloane-Reeves, J.; Cernichiari, E.; Needham, L.; Choi, A.; Wang, Y.; et al. Effects of prenatal and postnatal methylmercury exposure from fish consumption on neurodevelopment: Outcomes at 66 months of age in the Seychelles Child Development Study. J. Am. Med. Assoc. 1998, 280, 701–707. [Google Scholar] [CrossRef]
- Davidson, P.W.; Myers, G.J.; Shamlaye, C.; Cox, C.; Gao, P.; Axtell, C.; Morris, D.; Sloane-Reeves, J.; Cernichiari, E.; Choi, A.; et al. Association between prenatal exposure to methylmercury and developmental outcomes in Seychellois children: Effect modification by social and environmental factors. Neurotoxicology 1999, 20, 833–841. [Google Scholar] [PubMed]
- Davidson, P.W.; Myers, G.J.; Weiss, B.; Shamlaye, C.F.; Cox, C. Prenatal methyl mercury exposure from fish consumption and child development: A review of evidence and perspectives from the Seychelles Child Development Study. Neurotoxicology 2006, 27, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, E.; Beck, C.; Shamlaye, C.F.; Cernichiari, E.; Davidson, P.W.; Myers, G.J.; Clarkson, T.W. Benchmark concentrations for methyl mercury obtained from the 9-year follow-up of the Seychelles Child Development Study. Neurotoxicology 2006, 27, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Marsh, D.O.; Clarkson, T.W.; Myers, G.J.; Davidson, P.W.; Cox, C.; Cernichiari, E.; Tanner, M.A.; Lednar, W.; Shamlaye, C.; Choisy, O.; et al. The Seychelles study of fetal methylmercury exposure and child development: Introduction. Neurotoxicology 1995, 16, 583–596. [Google Scholar] [PubMed]
- World Health Organization. Children’s Exposure to Mercury Compounds. 2010. Available online: http://www.who.int/ceh/publications/children_exposure/en/index.html (accessed on 23 February 2017).
- Gundacker, C.; Frohlich, S.; Graf-Rohrmeister, K.; Eibenberger, B.; Jessenig, V.; Gicic, D.; Prinz, S.; Wittmann, K.J.; Zeisler, H.; Vallant, B. Perinatal lead and mercury exposure in Austria. Sci. Total Environ. 2010, 408, 5744–5749. [Google Scholar] [CrossRef] [PubMed]
- Croes, K.; De Coster, S.; De Galan, S.; Morrens, B.; Loots, I.; Van de Mieroop, E.; Nelen, V.; Sioen, I.; Bruckers, L.; Nawrot, T.; et al. Health effects in the Flemish population in relation to low levels of mercury exposure: From organ to transcriptome level. Int. J. Hyg. Environ. Health 2014, 217, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Guldner, L.; Monfort, C.; Rouget, F.; Garlantezec, R.; Cordier, S. Maternal fish and shellfish intake and pregnancy outcomes: A prospective cohort study in Brittany, France. Environ. Health 2007, 33. [Google Scholar] [CrossRef] [PubMed]
- Miklavčič, A.; Casetta, A.; Snoj Tratnik, J.; Mazej, D.; Krsnik, M.; Mariuz, M.; Sofianou, K.; Spirić, Z.; Barbone, F.; Horvat, M. Mercury, arsenic and selenium exposure levels in relation to fish consumption in the Mediterranean area. Environ. Res. 2013, 120, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Diez, S.; Montuori, P.; Pagano, A.; Sarnacchiaro, P.; Bayona, J.M.; Triassi, M. Hair mercury levels in an urban population from southern Italy: Fish consumption as a determinant of exposure. Environ. Int. 2008, 34, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Diez, S.; Delgado, S.; Aguilera, I.; Astray, J.; Perez-Gomez, B.; Torrent, M.; Sunyer, J.; Bayona, J.M. Prenatal and early childhood exposure to mercury and methylmercury in Spain, a high-fish-consumer country. Arch. Environ. Contam. Toxicol. 2009, 56, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.R. Mercury exposure: Medical and public health issues. Trans. Am. Clin. Climatol. Assoc. 2005, 116, 127–153. [Google Scholar] [PubMed]
- Plusquellec, P.; Muckle, G.; Dewailly, E.; Ayotte, P.; Begin, G.; Desrosiers, C.; Després, C.; Saint-Amour, D.; Poitras, K. The relation of environmental contaminants exposure to behavioral indicators in Inuit preschoolers in Arctic Quebec. Neurotoxicology 2010, 31, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, M.; Kaneoka, T.; Murata, K.; Nakai, K.; Satoh, H.; Akagi, H. Correlations between mercury concentrations in umbilical cord tissue and other biomarkers of fetal exposure to methylmercury in the Japanese population. Environ. Res. 2007, 103, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Liu, J.; Ye, B.; Ren, A. Concentrations of selected heavy metals in maternal blood and associated factors in rural areas in Shanxi Province, China. Environ. Int. 2014, 66, 157–164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Europe. Human Biomonitoring: Facts and Figures; WHO Regional Office for Europe: Copenhagen, Denmark, 2015; Available online: http://www.euro.who.int/en/media-centre/events/events/2015/04/ehp-mid-term-review/publications/human-biomonitoring-facts-and-figures (accessed on 23 February 2017).
- Lygre, G.B.; Haug, K.; Skjaerven, R.; Björkman, L. Prenatal exposure to dental amalgam and pregnancy outcome. Community Dent. Oral Epidemiol. 2016, 44, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Björnberg, K.A.; Vahter, M.; Petersson-Grawé, K.; Glynn, A.; Cnattingius, S.; Darnerud, P.O.; Atuma, S.; Aune, M.; Becker, W.; Berglund, M. Methyl mercury and inorganic mercury in Swedish pregnant women and in cord blood: Influence of fish consumption. Environ. Health Perspect. 2003, 111, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Agency for Toxic Substances and Disease Registry, ATSDR. Health Consultation: Mercury Exposure Investigation Using Serial Urine Testing and Medical Records Review, Kiddie Kollege. 2007. Available online: https://www.atsdr.cdc.gov/HAC/pha/KiddieKollege/KiddieKollegeHC061307.pdf (accessed on 23 February 2017).
- Ronchetti, R.; Zuurbier, M.; Jesenak, M.; Koppe, J.G.; Ahmed, U.F.; Ceccatelli, S.; Villa, M.P. Children’s health and mercury exposure. Acta Paediatr. Suppl. 2006, 95, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Murata, K.; Budtz-Jørgensen, E.; Weihe, P. Cardiac autonomic activity in methylmercury neurotoxicity: 14-year follow-up of a Faroes birth cohort. J. Pediatr. 2004, 144, 169–176. [Google Scholar] [CrossRef] [PubMed]
- National Research Council, NRC. Toxicological Effects of Methylmercury; National Academy Press: Washington, DC, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK225778/pdf/Bookshelf_NBK225778.pdf (accessed on 23 February 2017).
- Sakamoto, M.; Kubota, M.; Liu, X.J.; Murata, K.; Nakai, K.; Satoh, H. Maternal and fetal mercury and n-3 polyunsaturated fatty acids as a risk and benefit of fish consumption to fetus. Environ. Sci. Technol. 2004, 38, 3860–3863. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.H.; Smith, A.E. An assessment of the cord blood: Maternal blood methylmercury ratio: Implications for risk assessment. Environ. Health Perspect. 2003, 111, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Lederman, S.A.; Jones, R.L.; Caldwell, K.L.; Rauh, V.; Sheets, S.E.; Tang, D.; Viswanathan, S.; Becker, M.; Stein, J.L.; Wang, R.Y.; et al. Relation between cord blood mercury levels and early child development in a World Trade Center cohort. Environ. Health Perspect. 2008, 116, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Budtz-Jørgensen, E.; Jørgensen, P.J.; Weihe, P. Umbilical cord mercury concentration as biomarker of prenatal exposure to methylmercury. Environ. Health Perspect. 2005, 113, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Budtz-Jørgensen, E. Total Imprecision of Exposure Biomarkers: Implications for Calculating Exposure Limits. Am. J. Ind. Med. 2007, 50, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Jørgensen, P.J.; Weihe, P. Validity of mercury exposure biomarkers. In Biomarkers of Environmentally Associated Disease; Wilson, S.H., Suk, W.A., Eds.; CRC Press: Boca Raton, FL, USA, 2002; pp. 235–247. [Google Scholar]
- Wickre, J.B.; Folt, C.L.; Sturup, S.; Karagas, M.R. Environmental exposure and fingernail analysis of arsenic and mercury in children and adults in a Nicaraguan gold mining community. Arch. Environ. Health 2004, 59, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.R.; Sturup, S.; Chen, C.; Folt, C.; Karagas, M.R. Toenail mercury and dietary fish consumption. J. Expo. Sci. Environ. Epid. 2007, 17, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, M.; Chan, H.M.; Domingo, J.L.; Oliveira, R.B.; Kawakami, S.; Murata, K. Significance of fingernail and toenail mercury concentrations as biomarkers for prenatal methylmercury exposure in relation to segmental hair mercury concentrations. Environ. Res. 2015, 136, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, A.; Schültz, A.; Skerfving, S.; Hallén, I.P.; Ohlin, B.; Lagerkvist, B.J. Total and inorganic mercury in breast milk and blood in relation to fish consumption and amalgam fillings in lactating women. Arch. Environ. Health 1996, 51, 234–241. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency (EPA). Water Quality Criterion for the Protection of Human Health: Methylmercury; Chapter 4: Risk Assessment for Methylmercury; Office of Sciences and Technology, Office of Water: Washington, DC, USA, 2001. Available online: https://nepis.epa.gov/Exe/ZyPDF.cgi/20003UU4.PDF?Dockey=20003UU4.PDF (accessed on 23 February 2017).
- Crump, K.S.; Van Landingham, C.; Shamlaye, C.; Cox, C.; Davidson, P.W.; Myers, G.J.; Clarkson, T.W. Benchmark concentrations for methylmercury obtained from the Seychelles Child Development Study. Environ. Health Perspect. 2000, 18, 257–263. [Google Scholar] [CrossRef]
- Budtz-Jorgensen, E.; Grandjean, P.; Keiding, N.; White, R.F.; Weihe, P. Bench-mark dose calculations of methylmercury-associated neurobehavioural deficits. Toxicol. Lett. 2000, 112, 193–199. [Google Scholar] [CrossRef]
- Axelrad, D.A.; Bellinger, D.C.; Ryan, L.M.; Woodruff, T.J. Dose—Response relationship of prenatal mercury exposure and IQ: An integrative analysis of epidemiologic data. Environ. Health Perspect. 2007, 115, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Bellanger, M.; Pichery, C.; Aerts, D.; Berglund, M.; Castaño, A.; Cejchanová, M.; Crettaz, P.; Davidson, F.; Esteban, M.; Fischer, M.E.; et al. Economic benefits of methylmercury exposure control in Europe: Monetary value of neurotoxicity prevention. Environ. Health 2013, 3. [Google Scholar] [CrossRef]
- Guallar, E.; Sanz-Gallardo, M.I.; van’t Veer, P.; Bode, P.; Aro, A.; Gomez-Aracena, J.; Kark, J.D.; Riemersma, R.A.; Martín-Moreno, J.M.M.; Kok, J.F.; Heavy Metals and Myocardial Infarction Study Group. Mercury fish oils, and the risk of myocardial infarction. N. Engl. J. Med. 2002, 347, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Björkman, L.; Lundekvam, B.F.; Lægreid, T.; Bertelsen, B.I.; Morild, I.; Lilleng, P.; Lind, B.; Palm, B.; Vahter, M. Mercury in human brain, blood, muscle and toenails in relation to exposure: An autopsy study. Environ. Health 2007, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Perera, F.; Jankowski, J.; Rauh, V.; Flak, E.; Caldwell, K.L.; Jones, R.L.; Pac, A.; Lisowska-Miszczyk, I. Fish consumption in pregnancy, cord blood mercury level and cognitive and psychomotor development of infants followed over the first three years of life Krakow epidemiologic study. Environ. Int. 2007, 33, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Akagi, H.; Grandjean, P.; Takizawa, Y.; Weihe, P. Methylmercury dose estimation from umbilical cord concentrations in patients with Minamata disease. Environ. Res. 1998, 77, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F. Milestone development in infants exposed to methylmercury from human milk. Neurotoxicology 1995, 16, 27–33. [Google Scholar] [PubMed]
- Pichichero, M.E.; Gentile, A.; Giglio, N.; Umido, V.; Clarkson, T.; Cernichiari, E.; Zareba, G.; Gotelli, C.; Gotelli, M.; Yan, L.; et al. Mercury levels in newborns and infants after receipt of thimerosal-containing vaccines. Pediatrics 2008, 121, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G. Exposure to Mercury and Aluminum in Early Life: Developmental Vulnerability as a Modifying Factor in Neurologic and Immunologic Effects. Int. J. Environ. Res. Public Health 2015, 12, 1295–1313. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Dórea, J.G.; Fonseca, M.F.; Bastos, W.R.; Malm, O. Hair mercury in breast-fed infants exposed to thimerosal-preserved vaccines. Eur. J. Ped. 2007, 166, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.D.; Wimer, W.; Marques, R.C.; Shade, C. Automated Speciation of Mercury in the Hair of Breastfed Infants Exposed to Ethylmercury from Thimerosal-Containing Vaccines. Biol. Trace Elem. Res. 2011, 140, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-D.; Zheng, W. Human Exposure and Health Effects of Inorganic and Elemental Mercury. J. Prev. Med. Public Health 2012, 45, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Goldman, L.R.; Shannon, M.W. Technical report: Mercury in the environment: Implications for pediatricians. Pediatrics 2001, 108, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Eide, R.; Wesenberg, G.R. Mercury contents of indicator and target organs in rats after long-term, low-level mercury vapour exposure. Environ. Res. 1993, 61, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Lochner, F.; Appleton, J.; Keenan, F.; Cooke, M. Multi-element profiling of human deciduous teeth by laser ablation-inductively coupled plasma-mass spectrometry. Anal. Chim. Acta 1999, 401, 299–306. [Google Scholar] [CrossRef]
- Aylward, L.L.; Kirman, C.R.; Schoeny, R.; Portier, C.J.; Hays, S.M. Evaluation of Biomonitoring Data from the CDC National Exposure Report in a Risk Assessment Context: Perspectives across Chemicals. Environ. Health Perspect. 2013, 121, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Wilhelm, M.; Heudorf, U.; Kolossa-Gehring, M. Update of the reference and HBM values derived by the German Human Biomonitoring Commission. Int. J. Hyg. Environ. Health 2011, 215, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Joint FAO/WHO Expert Committee on Food Additives (JECFA), Methylmercury. Summary and Conclusions of the 67th Joint FAO/WHO Expert Committee on Food Additives; International Programme on Chemical Safety; WHO Technical Report Series 940; World Health Organization: Geneva, Switzerland, 2006; Available online: http://www.who.int/ipcs/publications/jecfa/reports/trs940.pdf (accessed on 23 February 2017).
- United Nations Environment Programme, UNEP. Global Mercury Assessment; UNEP Chemicals: Geneva, Switzerland, 2002; p. 258. Available online: http://www.unep.org/gc/gc22/Document/UNEP-GC22-INF3.pdf (accessed on 23 February 2017).
- Oken, E.; Osterdal, M.L.; Gillman, M.W.; Knudsen, V.K.; Halldorsson, T.I.; Strom, M.; Bellinger, D.C.; Hadders-Algra, M.; Michaelsen, K.F.; Olsen, S.F. Associations of maternal fish intake during pregnancy and breastfeeding duration with attainment of developmental milestones in early childhood: A study from the Danish National Birth Cohort. Am. J. Clin. Nutr. 2008, 88, 789–796. [Google Scholar] [PubMed]
- Suzuki, K.; Nakai, K.; Sugawara, T.; Nakamura, T.; Ohba, T.; Shimada, M.; Hosokawa, T.; Okamura, K.; Sakai, T.; Kurokawa, N. Neurobehavioral effects of prenatal exposure to methylmercury and PCBs, and seafood intake: Neonatal behavioral assessment scale results of Tohoku study of child development. Environ. Res. 2010, 110, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Batáriová, A.; Spěváčková, V.; Beneš, B.; Čejchanová, M.; Šmíd, J.; Černá, M. Blood and urine levels of Pb, Cd and Hg in the general population of the Czech Republic and proposed reference values. Int. J. Hyg. Environ. Health 2006, 209, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Puklová, V.; Krsková, A.; Černá, M.; Čejchanová, M.; Řehůřková, I.; Ruprich, J.; Kratzer, K.; Kubínová, R.; Zimová, M. The mercury burden of the Czech population: An integrated approach. Int. J. Hyg. Environ. Health 2010, 213, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Conrad, A.; Becker, K.; Kolossa-Gehring, M.; Seiwert, M.; Seifert, B. Twenty years of the German Environmental Survey (GerES): Human biomonitoring—Temporal and spatial (West Germany/East Germany) differences in population exposure. Int. J. Hyg. Environ. Health 2007, 210, 271–297. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Angerer, J.; Ewers, U.; Heudorf, U.; Wilhelm, M.; Human Biomonitoring Commission of the German Federal Environment Agency. Revised and new reference values for environmental pollutants in urine or blood of children in Germany derived from the German environmental survey on children 2003–2006 (GerES IV). Int. J. Hyg. Environ. Health 2009, 212, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Schoeters, G.; Colles, A.; Den Hond, E.; Croes, K.; Vrijens, J.; Baeyens, W.; Nelen, V.; Van De Mieroop, E.; Covaci, A.; Bruckers, L.; et al. The Flemish Environment and Health Study (FLEHS)—Second Survey (2007–2011): Establishing Reference Values for Biomarkers of Exposure in the Flemish Population. In Biomarkers and Human Biomonitoring; Knudsen, E., Merlo, D.F., Eds.; Royal Society of Chemistry: London, UK, 2012; Volume 1, pp. 135–165. [Google Scholar]
- Fréry, N.; Vandentorren, S.; Etchevers, A.; Fillol, C. Highlights of recent studies and future plans for the French human biomonitoring (HBM) programme. Int. J. Hyg. Environ. Health 2012, 215, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Pino, A.; Amato, A.; Alimonti, A.; Mattei, D.; Bocca, B. Human biomonitoring for metals in Italian urban adolescents: Data from Latium Region. Int. J. Hygiene Environ. Health 2012, 215, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Valent, F.; Mariuz, M.; Bin, M.; Little, D.A.; Mazej, D.; Tognin, V.; Tratnik, J.; McAfee, A.J.; Mulhern, M.S.; Parpinel, M.; et al. Associations of Prenatal Mercury Exposure from Maternal Fish Consumption and Polyunsaturated Fatty Acids with Child Neurodevelopment: A Prospective Cohort Study in Italy. J. Epidemiol. 2013, 23, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Hohenblum, P.; Steinbichl, P.; Raffesberg, W.; Weiss, S.; Moche, W.; Vallant, B.; Scharf, S.; Haluza, D.; Moshammer, H.; Kundi, M.; et al. Pollution gets personal! A first population-based human biomonitoring study in Austria. Int. J. Hygiene Environ. Health 2012, 215, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Gibicar, D.; Horvat, M.; Nakou, S.; Sarafidou, J.; Yager, J. Pilot study of intrauterine exposure to methylmercury in Eastern Aegean islands, Greece. Sci. Total Environ. 2006, 367, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Tratnik, J.S.; Mazej, D.; Miklavčič, A.; Krsnik, M.; Kobal, A.B.; Osredkar, J.; Briški, A.S.; Horvat, M. Biomonitoring of selected trace elements in women, men and children from Slovenia. In Proceedings of the 16th International Conference on Heavy Metals in the Environment—E3S Web of Conferences, Rome, Italy, 23–27 September 2012. [Google Scholar]
- Bárány, E.; Bergdahl, I.A.; Bratteby, L.E.; Lundh, T.; Samuelson, G.; Schütz, A.; Skerfving, S.; Oskarsson, A. Trace element levels in whole blood and serum from Swedish adolescents. Sci. Total Environ. 2002, 286, 129–141. [Google Scholar] [CrossRef]
- Vahter, M.; Åkesson, A.; Lind, B.; Björs, U.; Schütz, A.; Berglund, M. Longitudinal study of methylmercury and inorganic mercury in blood and urine of pregnant and lactating women, as well as in umbilical cord blood. Environ. Res. 2000, 84, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Ramón, R.; Murcia, M.; Aguinagalde, X.; Amurrio, A.; Llop, S.; Ibarluzea, J.; Lertxundi, A.; Alvarez-Pedrerol, M.; Casas, M.; Vioque, J.; et al. Prenatal mercury exposure in a multicenter cohort study in Spain. Environ. Int. 2011, 37, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Smolders, R.; Den Hond, E.; Koppen, G.; Govarts, E.; Willems, H.; Casteleyn, L.; Kolossa-Gehring, M.; Fiddicke, U.; Castaño, A.; Koch, H.M.; et al. Interpreting biomarker data from the COPHES/DEMOCOPHES twin projects: Using external exposure data to understand biomarker differences among countries. Environ. Res. 2015, 141, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Fourth National Report on Human Exposure to Environmental Chemicals, Updated Tables, February 2015. Centers for Disease Control and Prevention, Department of Health and Human Services: Atlanta, GA, USA, 2015. Available online: https://www.cdc.gov/biomonitoring/pdf/fourthreport_updatedtables_feb2015.pdf (accessed on 23 February 2017).
- Lye, E.; Legrand, M.; Clarke, J.; Probert, A. Blood total mercury concentrations in the Canadian population: Canadian Health Measures Survey cycle 1, 2007–2009. Can. J. Public Health 2013, 104, 246–251. [Google Scholar] [CrossRef]
- Muckle, G.; Ayotte, P.; Dewailly, E.E.; Jacobson, S.W.; Jacobson, J.L. Prenatal exposure of the Northern Quebec Inuit infants to environmental contaminants. Environ. Health Perspect. 2001, 109, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, P.; Hansen, J.C. Organochlorines and heavy metals in pregnant women from the Disco Bay area in Greenland. Sci. Total Environ. 2000, 245, 195–202. [Google Scholar] [CrossRef]
- Ha, M.; Kwon, H.J.; Leem, J.H.; Kim, H.C.; Lee, K.J.; Park, I.; Lim, Y.W.; Lee, J.H.; Kim, Y.; Seo, J.H.; et al. Korean Environmental Health Survey in Children and Adolescents (KorEHS-C): Survey design and pilot study results on selected exposure biomarkers. Int. J. Hyg. Environ. Health 2014, 217, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Steuerwald, U.; Weihe, P.; Jørgensen, P.J.; Bjerve, K.; Brock, J.; Heinzow, B.; Budtz-Jørgensen, E.; Grandjean, P. Maternal seafood diet, methyl-mercury exposure and neonatal neurological function. J. Pediatr. 2000, 136, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Fok, T.F.; Lam, H.S.; Ng, P.C.; Yip, A.S.; Sin, N.C.; Chan, I.H.S.; Gua, G.J.S.; So, H.K.; Wong, E.M.C.; Lam, C.W.K. Fetal methylmercury exposure as measured by cord blood mercury concentrations in a mother–infant cohort in Hong Kong. Environ. Int. 2007, 33, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.S.; Liu, P.L.; Chien, L.C.; Chou, S.Y.; Han, B.C. Mercury concentration and fish consumption in Taiwanese pregnant women. BJOG 2007, 114, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Dewailly, E.; Suhas, E.; Mou, Y.; Dallaire, R.; Chateau-Degat, L.; Chansin, R. High fish consumption in French Polynesia and prenatal exposure to metals and nutrients. Asia Pac. J. Clin. Nutr. 2008, 17, 461–470. [Google Scholar] [PubMed]
- United Nations Environment Programme and World Health Organization. Guidance for Identifying Populations at Risk from Mercury Exposure; World Health Organization: Geneva, Switzerland, 2008; Available online: http://www.who.int/foodsafety/publications/chem/mercuryexposure.pdf (accessed on 23 February 2017).
- Višnjevec, A.M.; Kocman, D.; Horvat, M. Human mercury exposure and effects in Europe. Environ. Toxicol. Chem. 2014, 33, 1259–1270. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Health and Environmental Risks, SCHER. Opinion on Mercury in Certain Energy-Saving Light Bulbs; European Commission Health & Consumer Protection Directorate-General Brussels Belgium: Brussels, Belgium, 2012; Available online: https://ec.europa.eu/health/scientific_committees/environmental_risks/docs/scher_o_159.pdf (accessed on 23 February 2017).
- European Commission-DG Environment (DG ENV). Study on the Potential for Reducing Mercury Pollution from Dental Amalgam and Batteries; Final Report; European Commission: Brussels, Belgium, 2012; Available online: http://ec.europa.eu/environment/chemicals/mercury/pdf/final_report_110712.pdf (accessed on 23 February 2017).
- Woods, J.S.; Martin, M.D.; Leroux, B.G.; DeRouen, T.A.; Leitão, J.G.; Bernardo, M.F.; Luis, H.S.; Simmonds, P.L.; Kushleika, J.V.; Huang, Y. The contribution of dental amalgam to urinary mercury excretion in children. Environ. Health Perspect. 2007, 115, 1527–1531. [Google Scholar] [CrossRef] [PubMed]
- Maserejian, N.N.; Trachtenberg, F.L.; Assmann, S.F.; Barregard, L. Dental amalgam exposure and urinary mercury levels in children: The New England Children’s Amalgam Trial. Environ. Health Perspect. 2008, 116, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Baek, H.J.; Kim, E.K.; Lee, S.G.; Jeong, S.H.; Sakong, J.; Merchant, A.T.; Im, S.U.; Song, K.B.; Choi, Y.H. Dental amalgam exposure can elevate urinary mercury concentrations in children. Int. Dental J. 2016, 66, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Martinez, A.C.; Orta-Garcia, S.T.; Rico-Escobar, E.M.; Carrizales-Yañez, L.; Martin Del Campo, J.D.; Pruneda-Alvarez, L.G.; Ruiz-Vera, T.; Gonzalez-Palomo, A.K.; Piña-Lopez, I.G.; Torres-Dosal, A.; et al. Exposure Assessment to Environmental Chemicals in Children from Ciudad Juarez, Chihuahua, Mexico. Arch. Environ. Contam. Toxicol. 2016, 70, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Schwartz, S.; Dijak, M.; Weber, J.-P.; Tardif, R.; Rouah, F. Childhood urine mercury excretion: Dental amalgam and fish consumption as exposure factors. Environ. Res. 2004, 94, 283–290. [Google Scholar] [CrossRef] [PubMed]
- De Burbure, C.; Buchet, J.-P.; Leroyer, A.; Nisse, C.; Haguenoer, J.-M.; Mutti, A.; Smerhovský, Z.; Cikrt, M.; Trzcinka-Ochocka, M.; Rezniewska, G.; et al. Renal and neurologic effects of cadmium, lead, mercury, and arsenic in chilly effects and multiple interactions at environmental exposure levels. Environ. Health Perspect. 2006, 114, 585–590. [Google Scholar]
- Vandentorren, S.; Bois, C.; Pirus, C.; Sarter, H.; Salines, G.; Leridon, H. Rationales, design and recruitment for the ELFE longitudinal study. BMC Pediatr. 2009, 58. [Google Scholar] [CrossRef]
- Golding, J.; Steer, C.D.; Hibbeln, J.R.; Emmett, P.M.; Lowery, T.; Jones, R. Dietary predictors of maternal prenatal blood mercury levels in the ALSPAC birth cohort study. Environ. Health Perspect. 2013, 121, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Olsén, J.; Melbye, M.; Olsen, S.F.; Sorensen, T.I.; Aaby, P.; Andersen, A.M.; Taxbøl, D.; Hansen, K.D.; Juhl, M.; Schow, T.B.; et al. The Danish National Birth Cohort—Its background, structure and aim. Scand. J. Public Health 2001, 29, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Vejrup, K.; Brantsæter, A.L.; Knutsen, H.K.; Magnus, P.; Alexander, J.; Kvalem, H.E.; Meltzer, H.M.; Haugen, M. Prenatal mercury exposure and infant birth weight in the Norwegian Mother and Child Cohort Study. Public. Health Nutr. 2014, 17, 2071–2080. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M.; Wittsiepe, J.; Lemm, F.; Ranft, U.; Krämer, U.; Fürst, P.; Röseler, S.C.; Greshake, M.; Imöhl, M.; Eberwein, G.; et al. The Duisburg birth cohort study: Influence of the prenatal exposure to PCDD/Fs and dioxin-like PCBs on thyroid hormone status in newborns and neurodevelopment of infants until the age of 24 months. Mutat. Res. 2008, 659, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Hanke, W.; Jurewicz, J.; Sobala, W.; Madsen, C.; Nafstad, P.; Magnus, P. Polish mother and child cohort study (REPRO_PL)—Methodology of follow-up of the children. Int. J. Occup. Med. Environ. Health 2011, 24, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Sonneborn, D.; Park, H.Y.; Petrik, J.; Kocan, A.; Palkovicova, L.; Trnovec, T.; Nguyen, D.; Hertz-Picciotto, I. Prenatal polychlorinated biphenyl exposures in Eastern Slovakia modify effects of social factors on birth weight. Paediatr. Perinat. Epidemiol. 2008, 22, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Leino, O.; Kiviranta, H.; Karjalainen, A.K.; Kronberg-Kippilä, C.; Sinkko, H.; Larsen, E.H.; Virtanen, S.; Tuomisto, J.T. Pollutant concentrations in placenta. Food Chem. Toxicol. 2013, 54, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.; Patelarou, E.; Chatzi, L.; Vrijheid, M.; Koutis, A.; Fthenou, E.; Grander, M.; Palm, B.; Kogevinas, M.; Vahter, M. Determinants of Blood Cadmium, Lead, Arsenic, Uranium, Mercury and Molybdenum Levels among Pregnant Women in Crete, Greece. In Proceedings of the International Society for Environmental Epidemiology ISEE 21st Annual Conference Abstracts Supplement, Dublin, Ireland, 25–29 August 2009. [Google Scholar]
- Valent, F.; Horvat, M.; Sofianou-Katsoulis, A.; Spiric, Z.; Mazej, D.; Little, D.; Prasouli, A.; Mariuz, M.; Tamburlini, G.; Nakou, S.; et al. Neurodevelopmental effects of low-level prenatal mercury exposure from maternal fish consumption in a Mediterranean cohort: Study rationale and design. J. Epidemiol. 2013, 23, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Casas, M.; Bergström, A.; Carmichael, A.; Cordier, S.; Eggesbø, M.; Eller, E.; Fantini, M.P.; Fernández, M.F.; Fernández-Somoano, A.; et al. European Birth Cohorts for Environmental Health Research. Environ. Health Perspect. 2010, 120, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Snoj Tratnik, J.; Falnoga, I.; Trdin, A.; Mazej, D.; Fajon, V.; Miklavčič, A.; Kobal, A.B.; Osredkar, J.; Sešek Briški, A.; Krsnik, M.; et al. Prenatal mercury exposure, neurodevelopment and apolipoprotein E genetic polymorphism. Environ. Res. 2017, 152, 375–385. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year | Event | References |
|---|---|---|
| 1952 | First report on developmental MeHg neurotoxicity in infants | [8] |
| 1956 | Discovery of a seafood-related disease in Minamata Bay in Japan | [9] |
| 1968 | Acknowledgment of MeHg as cause of Minamata disease | [9] |
| 1972 | Experimental study on delayed effects of developmental neurotoxicity in rats | [11] |
| 1973 | Report on a dose-dependence of poisoning from methylmercury-derived fungicide by using Iraq data | [10] |
| 1986 | First epidemiology report on adverse effects in children related to maternal fish intake during pregnancy in New Zealand | [15] |
| 1997 | Confirmation from prospective study in the Faroe Islands on adverse effects in children from maternal fish intake during pregnancy | [17] |
| 1995 | The Seychelles Child Development Study was launched for evaluating prenatal methylmercury exposure resulting solely from ocean fish consumption | [19] |
| Organic Mercury | Elemental Mercury (Hg0) | Inorganic Mercury (Mercurous Hg+; Mercuric Hg2+) |
|---|---|---|
| Source of exposure | ||
| - MeHg: diet (fish, rice) - EtHg: a topical antiseptic and antifungal agent in vaccines | - Hg vapours released from maternal dental amalgam (50% is Hg0) [41] - Accidental exposure (from broken thermometers and other devices used in school laboratories) - Specific products (e.g., mercury-containing paints) | Use of cosmetics containing salts (skin creams, soaps, medications); vaccines; breast milk for infants |
| Absorption | ||
| - Oral: MeHg from GI tract (95%) [4,29] - Transdermal: EtHg from vaccines (100%) [5] - Inhalation: only from vapours of MeHg | - Oral: metallic Hg in GI tract is converted to mercuric sulfide [4] - Dermal: absorption of Hg0 through children’s skin - Inhalation: from Hg vapours (70–85%) [2] | - Oral: absorption through the GI from breast milk (infants) or from water (children) - Dermal: absorption through children’s skin - Inhalation: aerosol from Hg salts |
| Distribution | ||
| - MeHg from the GI tract is distributed to the blood; in the body it is present as hydrophilic complexes attached to the sulfur atom of thiol ligands [46] - MeHg crosses the blood-brain or placental barrier via a MeHg-l-cysteine complex transported by neutral amino acid carrier [29,46] - After thimerosal injection, the EtHg–cysteine complex is exported from muscle cells by thiol-containing proteins. Then, it exchanges with generic plasma thiol proteins, like albumin [5] | After absorption it crosses the lungs and, thus, into the bloodstream, where, due to its high lipophilicity, is distributed throughout the body, including the blood-brain and the placenta barrier [7] | - From the GI tract it is distributed to the blood and organs. Mercuric Hg has affinity for sulfhydryl groups in the RBCs and plasma [4,47] - Due to its ionic charge it does not cross the blood-brain or the placenta barrier |
| Biotransformation (metabolism) | ||
| - MeHg is stable in the body, but intestinal flora, tissue macrophages, and fetal liver are site of demethylation to inorganic Hg [4] - EtHg is much more less stable; it is rapidly degraded to mercuric Hg | Elemental Hg is oxidized to mercuric Hg in the RBCs by catalase and hydrogen peroxide [4] | Mercuric Hg is unstable in vivo; it is converted to elemental Hg (rat study); only intestinal flora is site of methylation [46] |
| Excretion | ||
| - MeHg is secreted in bile and excreted in feces (~90% in feces occurs as inorganic Hg after demethylation) [46] - MeHg is excreted also in breast milk [2] - Approximately 1% of the human body burden of MeHg is excreted daily [2,46] - MeHg half-life elimination has been estimated at 45–90 days [4,46] - EtHg is excreted mainly by feces - From infant blood the EtHg excretion resulted more rapid than MeHg due to its rapid conversion to mercuric Hg (half-life 3–7 days) [5] | - Hg vapour is excreted via sweat and saliva, or as mercuric Hg via feces and urine - Approximately more than 1% of the human body burden is excreted daily [46] - Half-life elimination has been estimated at 58 days [4,46] | - Inorganic Hg is excreted mainly in urine; saliva, bile, sweat, exhalation, and breast milk are other routes of excretion - Half-life has been estimated at 49–96 days [4,46] |
| Target organs | ||
| MeHg and EtHg have the same target: fetal brain, CNS, other system (cardiovascular, reproductive, immune, etc.) | CNS, kidney, lungs, skin | Since mercuric Hg induces metallothionein production in the kidneys, the highest concentration is in this organ, however also CNS and skin are critical sites |
| Biomarker | Exposure | Pros | Cons |
|---|---|---|---|
| Maternal blood | Short-term exposure | Total Hg is suitable for estimating internal exposure to MeHg (mother with regular fish consumption) [4] Total Hg in RBCs is a more accurate measure of MeHg exposure (procedure is more time-consuming) [47] | Invasive sampling Storage and transportation is more complicated Total Hg does not provide clear information about magnitude and timing of exposure [46] |
| Cord blood | Middle-term exposure | Total Hg reflects the MeHg concentrations in the target organ (i.e., fetal brain) [46] Total Hg represents fetal exposure over longer time than maternal blood [48] | Total Hg does not provide information on exposure variability during gestation [46] Storage and transportation is more complicated |
| Hair | Long-term exposure | Non-invasive sampling Easy to preserve Total Hg estimates internal mehg exposure at all exposure levels (fish consumer population) [46] Total Hg provides information about magnitude and timing of exposure [29] | Quality assurance/quality control systems are required for accurate results (presence of external contamination) [29] Uncertainties on the hair-growth rate [47,52] |
| Nails (finger- and toenails) | Long-term exposure | Simple and non-invasive sampling Easy to preserve Capable to reveal chronic exposure [53,54] | Quality assurance/quality control systems are required for accurate results [29,55] Fingernails are sometimes contaminated [54,55] |
| Umbilical cord tissue | Middle term exposure | Simple and non-invasive sampling Total Hg represents exposure during the third trimester [29] | Not capable to identify sensitive short-term variation [50] A dry weight-based total Hg concentration is more accurate (procedure is more time-consuming) [50] |
| Breast milk | Long-term exposure | Total Hg is suitable for estimating past maternal exposure Total Hg is suitable to predict the potential exposure for breast-feeding in infants [56] | MeHg-specific analysis may be required [56] |
| Reference Population | HBM-I [77] | HBM-II [77] | NRC, [46] | JECFA, [78] | Bellanger et al. [61] | |
|---|---|---|---|---|---|---|
| Total Hg in urine | children and women of child-bearing age | 7 µg/L (5 µ/g creat.) | 25 µg/L (20 µ/g creat.) | |||
| Total Hg in blood | children and women of child-bearing age | 5 µg/L | 15 µg/L | |||
| MeHg in hair a | children and women of child-bearing age | 1 µg/g | 2.3 µg/g | 0.58 µg/g | ||
| Total Hg cord blood | - | 5.8 µg/L | ||||
| Total Hg maternal blood | pregnant women | 3.5 µg/L |
| MeHg | Total Hg | |||||||
|---|---|---|---|---|---|---|---|---|
| Country | Study Period | Reference Population | Hair (µg/g) | Hair (µg/g) | Blood (µg/L) | Urine (µg/L) | Cord Blood (µg/L) | References |
| Czech Republic | Cz-HBM 2001–2003 | Children (8–10 yo) | 0.43 (1.44) n = 333 | 0.45 (4.18) a n = 619 | [82] | |||
| 2008 | Children (8–10 yo) | 0.18 (0.61) n = 316 | 0.45 (1.39) n = 382 | 0.26 (2.19) a n = 364 | [83] | |||
| Germany | GerES II 1990–1992 | Children (6–17 yo) | 0.33 (1.4) n = 812 | 0.54 (3.99) n = 812 | [84] | |||
| GerES IV 2003–2006 | Children (3–14 yo) | 0.23 (0.89) n = 1790 | <0.1 (0.4) n = 1790 | [85] | ||||
| Belgium (Flanders) | FLEHS II 2007–2011 | Mothers (20–40 yo) | 0.26 (0.5) b n = 242 | 0.35 (0.60) b n = 242 | [86] | |||
| Adolescents (14–15 yo) | 0.12 (0.35) b n = 206 | 0.19 (0.47) b n = 206 | ||||||
| France | ENNS 2006–2007 | Children (3–17 yo) | 0.37 (1.2) n = 1364 | [87] | ||||
| Italy | PROBE 2008–2010 | Adolescents (13–15 yo) | 0.84 (3.55) n = 252 | [88] | ||||
| 2007–2009 | Pregnant women | 1.38 c (1.85) e n = 220 | 0.78 c (1.28) e n = 604 | 0.0023 c (0.0039) e n = 606 | [89] | |||
| Austria | 2008–2010 | Children (6–11 yo) | 0.006 c n = 50 | [90] | ||||
| Greece | Pregnant women (17–46 yo) | 1.07 n = 246 | 1.36 n = 246 | [91] | ||||
| Slovenia | Not available | women in childbearing age (20–35 yo) | 0.24 n = 127 | 1.04 n = 127 | 0.73 a n = 127 | [92] | ||
| Children (6–11 yo) | 0.18 n = 174 | 0.77 n = 174 | 0.73 a n = 174 | |||||
| Sweden | 1993–1994 | Adolescent (15 yo) | 1.1 c (2.7) n = 335 | [93] | ||||
| 1996–1999 | Pregnant women (20–40 yo) | 0.35 c (0.81) b n = 127 | MeHg: 1.3 c (2.7) b In-Hg: 0.15 c (0.32) b n = 130 | [42] | ||||
| 1994–1996 | Pregnant women (20–40 yo) | MeHg: 0.94 c (2.5) In-Hg: 0.37 c (1.4) n = 148 | 1.6 c (4.6) n = 226 | [94] | ||||
| Newborns | MeHg: 1.4 c (3.8) In-Hg: 0.34 c (0.75) n = 98 | |||||||
| Spain | 2008 | Newborns and infants (0–4 yo) | 0.97 n = 218 | 1.41 n = 218 | [35] | |||
| 2004–2008 | Mother and child pairs | 8.2 n = 1883 | [95] | |||||
| Poland | 2001–2003 | Mother and child pairs | 1.09 n = 233 | 0.8 n = 233 | [64] | |||
| 17 EU countries | DEMOCHOPES 2010–2012 | Children (6–11 yo) | 0.15 (0.80) b n = 120 | [96] | ||||
| Mothers (<45 yo) | 0.23 (1.20) b n = 120 | |||||||
| USA—NHANES | 2003–2004 | Infant (1–5 yo) | 0.33 (1.8) n = 911 | [97] | ||||
| 2003–2004 | Children (6–11 yo) | 0.42 (1.95) n = 856 | 0.30 (1.87) d n = 398 | |||||
| 2003–2004 | Adolescent (12–19 yo) | 0.49 (2.60) n = 2081 | 0.36 (1.82) d n = 375 | |||||
| 2009–2010 | Adolescent (12–19 yo) | 0.53 (3.01) n = 1183 | ||||||
| 2011–2012 | Infant (1–5 yo) | 0.26 (0.99) n = 713 | ||||||
| 2011–2012 | Children (6–11 yo) | 0.33 (1.40) n = 1048 | 0.24 (1.37) n = 401 | |||||
| MeHg: 0.21 (1.34) n = 1044 | ||||||||
| 2011–2012 | Adolescent (12–19 yo) | 0.41 (2.25) n = 1129 | 0.26 (1.31) n = 390 | |||||
| MeHg: 0.27 (2.15) n = 1121 | ||||||||
| Canada | CHMS 2009–2011 | Infant (1–5 yo) | 0.27 (3.0) n = 495 | [98] | ||||
| CHMS 2009–2011 | Children (6–11 yo) | 0.28 (2.0) n = 961 | ||||||
| CHMS 2009–2011 | Adolescent (12–19 yo) | 0.27 (2.4) n = 997 | ||||||
| Inuit popluation 1995–2001 | Pregnant women (14–40 yo) | 3.7 n = 130 | 10.4 n = 130 | 18.5 n = 130 | [99] | |||
| Greenland | 1994–1996 | Pregnant women | 12.8 n = 180 | 25.3 n = 178 | [100] | |||
| South Korea | KorEHS-C 2011–2012 | Children and adolescent (6–19 yo) | 1.73 (3.20) n = 351 | [101] | ||||
| Faeroe Island | 1994–1995 | Mothers (20–35 yo) | 4.08 n = 144 | [102] | ||||
| Hong Kong | 2000–2001 | Mother and child pairs | 1.2 c n = 1057 | 8.8 c n = 1057 | [103] | |||
| Taiwan | 2004–2005 | Pregnant women (16–42 yo) | 9.2 n = 65 | [104] | ||||
| Japan | 1996 | Pregnant women (19–41 yo) | 1.62 (2.19) e n = 116 | 5.18 (7.34) e n = 116 | 9.8 (13.6) e n = 116 | [38] | ||
| Polynesia | 2005–2006 | Pregnant women (15–44 yo) | 10.5 (11.5) n = 242 | [105] | ||||
| Country | Birth Cohort | Metals | Enrollment Period | No. of Children at Birth | References |
|---|---|---|---|---|---|
| Faroe Islands | Faroes: Children’s Health and the Environment in the Faroes | Hg, Pb, Se | 1986–2009 | 2351 | [17,45] |
| United Kingdom | ALSPAC—The Avon Longitudinal Study of Parents and Children | As, Cd, Hg, Mn, Pb, Se | 1991–1992 | 14,062 | [117] |
| Denmark | DNBC—Danish National Birth Cohort | Hg | 1996–2002 | 96,986 | [118] |
| Spain | INMA—Environment and Childhood | Hg, Pb, TMS | 1997–2008 | 3757 | [95] |
| Norway | MoBa—Norwegian Mother and Child Cohort Study | Hg | 1999–2008 | 100,000 | [119] |
| Germany | Duisburg cohort | Cd, Hg, Pb, Se | 2000–2003 | 234 | [120] |
| Poland | Kraków cohort | Cd, Hg, Pb | 2000–2003 | 505 | [64] |
| REPRO_PL—Polish Mother and Child Cohort | Cd, Hg, Pb, Se, Zn, Cu | 2007–2011 | 1800 | [121] | |
| Slovakia | PCB cohort—Early Childhood Development and PCB exposures in Slovakia | Hg, Pb | 2001–2003 | 1134 | [122] |
| Finland | LUKAS cohort: Finnish cohort | As, Cd, Hg, Pb, Se | 2002–2005 | 442 | [123] |
| France | PÉLAGIE—Endocrine disruptors: longitudinal study on pregnancy abnormalities, infertility, and childhood | Hg | 2002–2006 | 3421 | [32] |
| ELFE: French longitudinal study of children | Al, As, Cd, Hg, Pb | 2011–2012 | 20,000 | [116] | |
| Italy | Trieste Cohort: Trieste child development cohort | Hg, Pb, Se, Zn | 2007–2009 | 900 | [89] |
| Greece | RHEA—Mother Child Cohort in Crete | As, Cd, Hg, Mn, Pb | 2007–2008 | 1500 | [124] |
| Italy, Greece, Slovenia, and Croatia | NACII—Mediterranean cohort study, (within PHIME project) | Cd, Hg, Pb, Mn, Se, Zn | 2006–2011 | 1700 | [125] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruggieri, F.; Majorani, C.; Domanico, F.; Alimonti, A. Mercury in Children: Current State on Exposure through Human Biomonitoring Studies. Int. J. Environ. Res. Public Health 2017, 14, 519. https://doi.org/10.3390/ijerph14050519
Ruggieri F, Majorani C, Domanico F, Alimonti A. Mercury in Children: Current State on Exposure through Human Biomonitoring Studies. International Journal of Environmental Research and Public Health. 2017; 14(5):519. https://doi.org/10.3390/ijerph14050519
Chicago/Turabian StyleRuggieri, Flavia, Costanza Majorani, Francesco Domanico, and Alessandro Alimonti. 2017. "Mercury in Children: Current State on Exposure through Human Biomonitoring Studies" International Journal of Environmental Research and Public Health 14, no. 5: 519. https://doi.org/10.3390/ijerph14050519
APA StyleRuggieri, F., Majorani, C., Domanico, F., & Alimonti, A. (2017). Mercury in Children: Current State on Exposure through Human Biomonitoring Studies. International Journal of Environmental Research and Public Health, 14(5), 519. https://doi.org/10.3390/ijerph14050519