Enabling Factors for Sustaining Open Defecation-Free Communities in Rural Indonesia: A Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
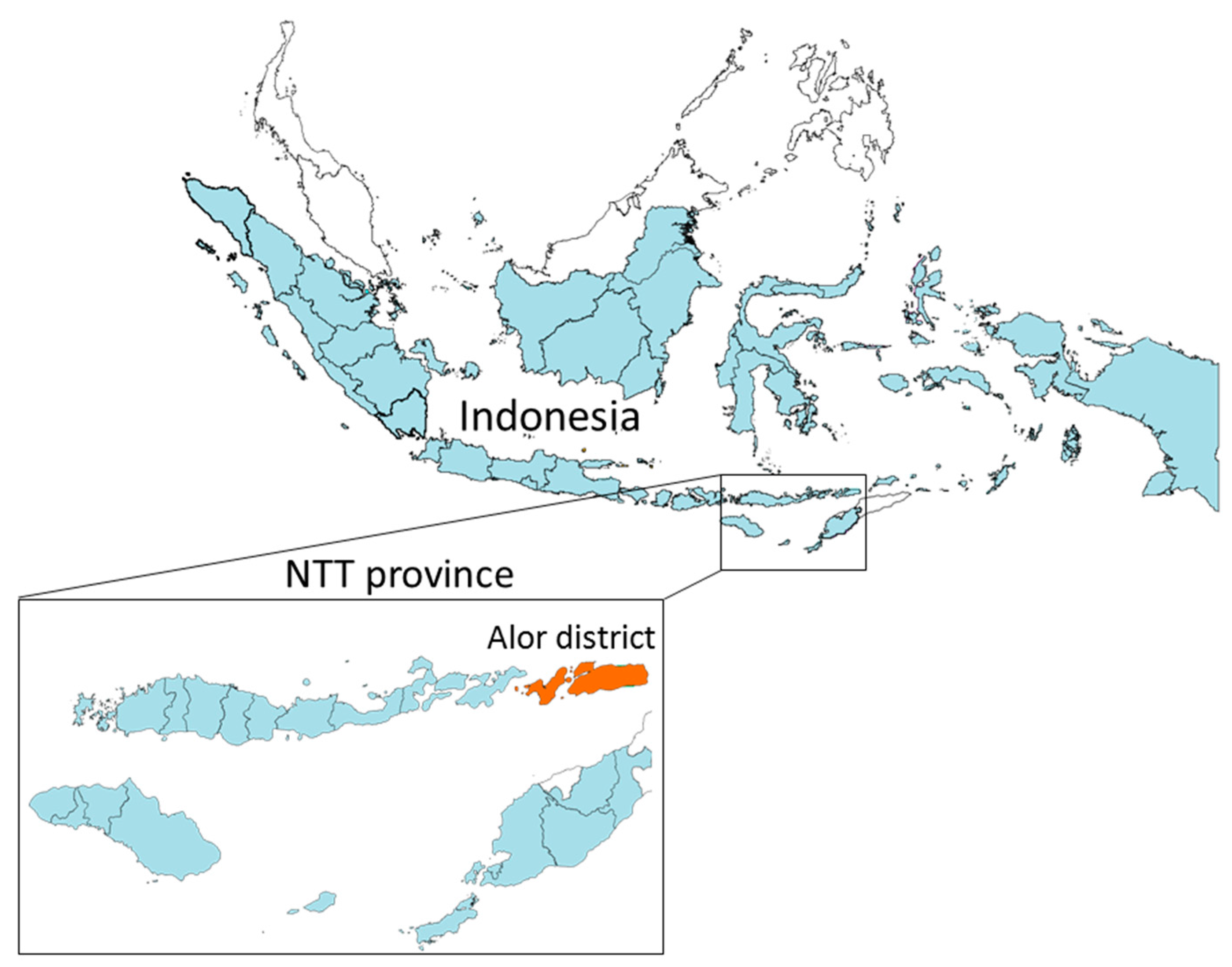
2.1. Study Area and Data Collection
2.2. Household Slippage Measurement
2.3. Social Norms Measurements
2.4. Statistical Analysis
2.5. Focus Group Discussions (FGDs)
3. Results
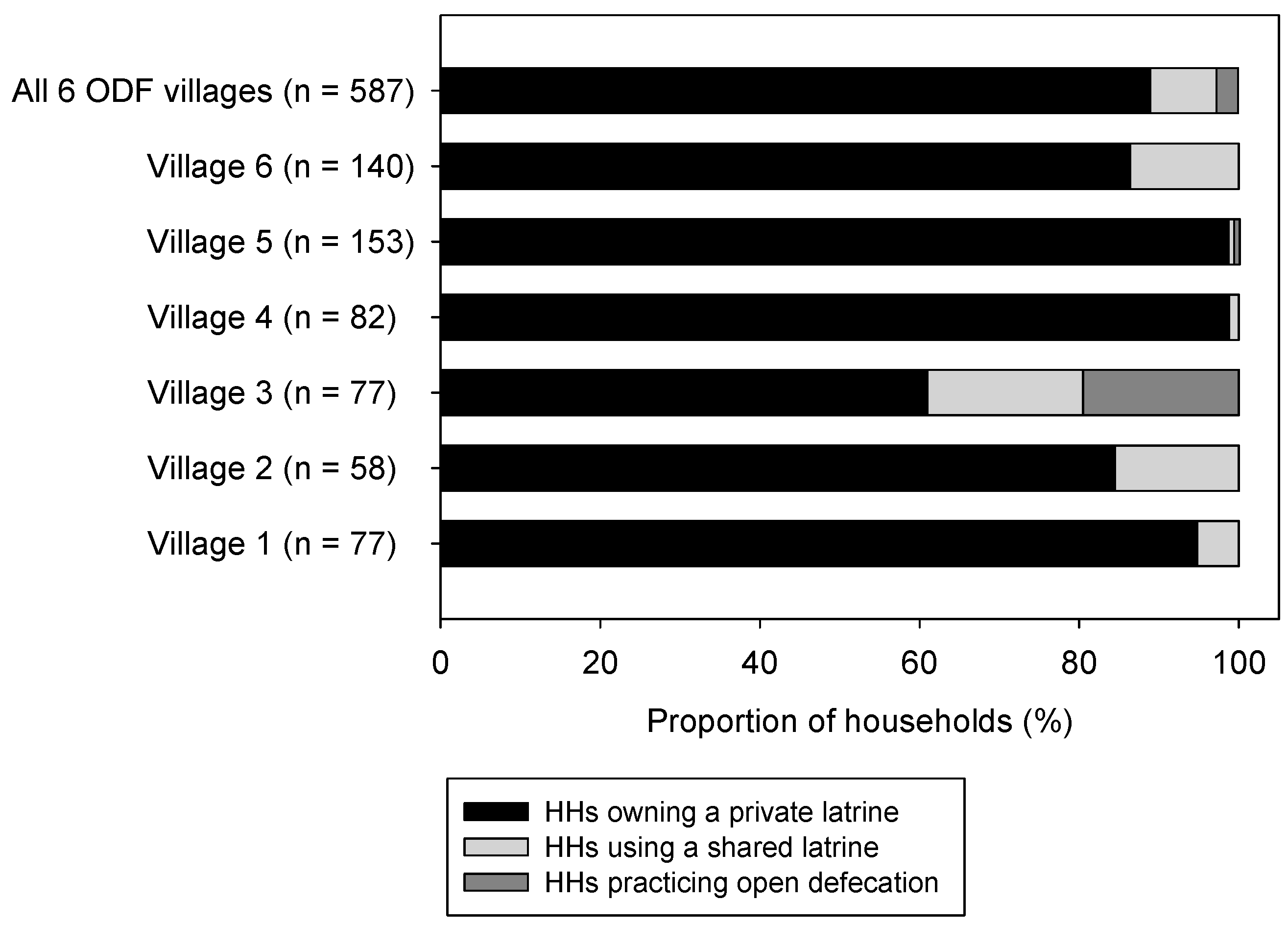
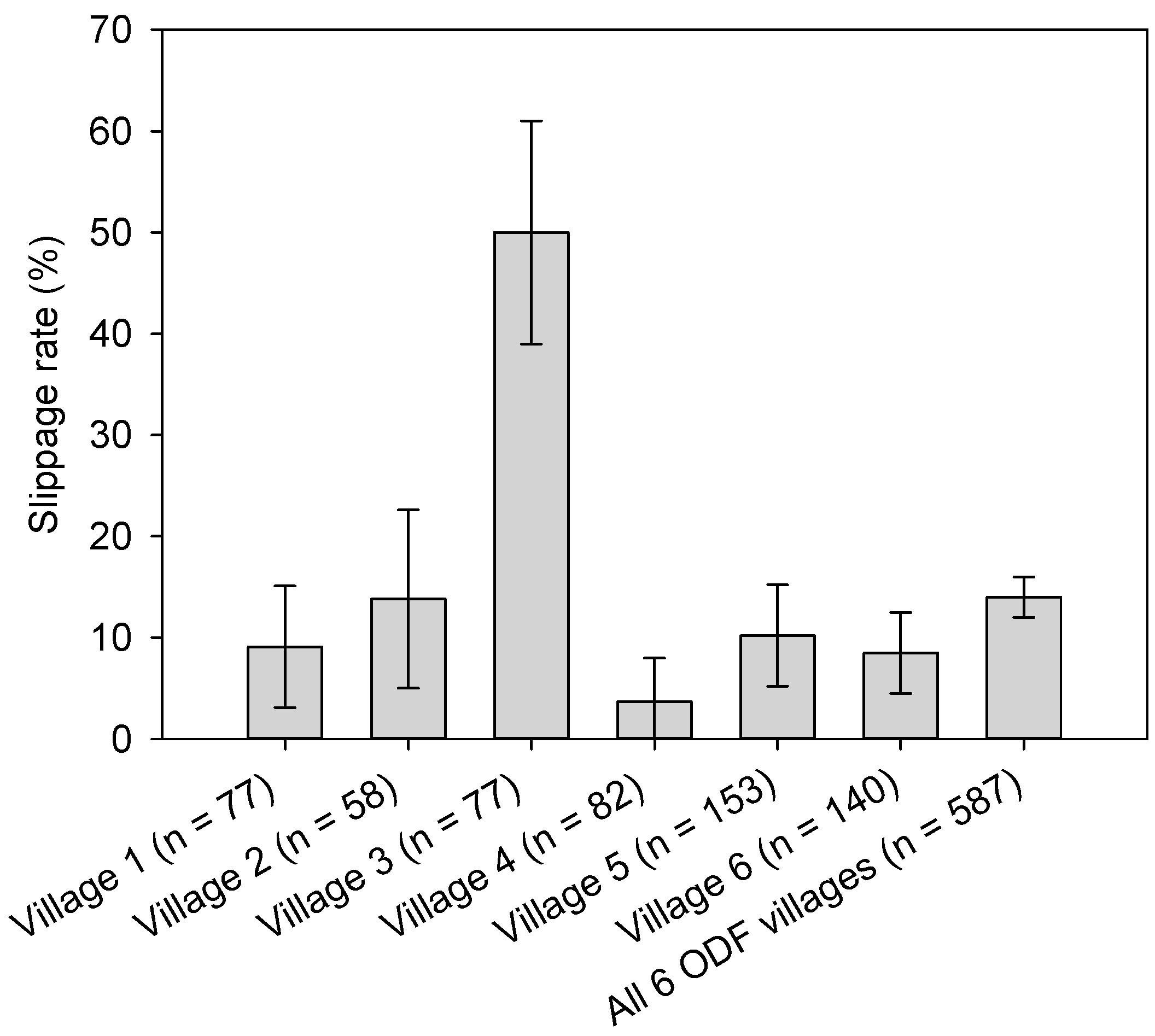
3.1. Sanitation Access and Levels of Slippage
3.2. Factors Associated with Overall Slippage (i.e., Households both Owning and Not Owning a Private Latrine) and Slippage among Households Owning a Private Latrine
3.3. Factors Associated with Private Latrine Ownership
3.4. STBM Implementation and Process Assessment via Focus Group Discussions (FGDs)
4. Discussion
4.1. ODF Sustainability, Slippage Pattern and Dynamics of Social Norms
4.2. Socio-Economic and Social Norms Related Factors Associated Overall Slippage among All Households, Slippage among Households Owning a Private Latrine, and Private Latrine Ownership
4.3. Implications in Indonesia
- At national level, a systematic monitoring mechanism for assessing the sustainability of STBM outcomes, together with the development of associated guidance with clear indicators, will help to raise awareness to key decision makers, and for more efficient targeting and resource allocation. Measuring levels of social norms could help to better understand the sustainability of ODF status in communities.
- There is a strong need for systematic approaches, including STBM, to achieve these objectives around ODF communities and improved sanitation coverage. Recent efforts in Indonesia to enhance fund flows for creating and improving sanitation access are welcome; examples are the use of zakat and wakaf (Islamic charity funds) [41], and also the Central Government instructions that the special allocation funds may be used for sanitation (known as DAK Sanitasi in Indonesia).
- For the poorest, targeted smart financing schemes by village, sub-national or national governments may help to move them up the sanitation ladder from a shared latrine to a private latrine, and from a basic latrine to an improved. However, the demand creation process and collective action commitment to the elimination of open defecation by all of the community together should not be undermined, as per the principles of CATS/CLTS. Such systematic approaches may include regular monitoring and oversight from primary health centers (PUSKESMAS) and District Health Office (DHO), as well as all stakeholders working on a shared community action plan over a 3 to 5 year timeline, with key milestones agreed and owned by all.
- Water access provision may be coupled with ODF achievements for sustaining latrine use behaviour. National and sub-national government may incentivize communities to achieve ODF as prerequisite for water provision.
- This paper may inform monitoring and preventive measures to sustain ODF status. It is important for STBM to first focus on the achievement of ODF communities, and to then continue beyond ODF (i.e., to cover all five pillars of STBM). This requires continual support and demand generation efforts with all of the support of the entire community, especially to move open defecators onto the sanitation ladder, and to move those with basic or shared sanitation up to a higher level of WASH service provision and other community-based health interventions (e.g., reduction of stunting), and possibly in a phased fashion over a multi-year period. This will support communities to continuously improve their public health and child survival status by building on the new social capital and norms created via the achievement of an ODF community.
4.4. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO/UNICEF Joint Monitoring Programme. Progress on Sanitation and Drinking Water—2017 Update and SDG Baseline; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Boisson, S.; Engels, D.; Gordon, B.A.; Medlicott, K.O.; Neira, M.P.; Montresor, A.; Solomon, A.W.; Velleman, Y. Water, sanitation and hygiene for accelerating and sustaining progress on neglected tropical diseases: A new global strategy 2015–20. Int. Health 2016, 8 (Suppl. 1), i19–i21. [Google Scholar] [CrossRef] [PubMed]
- Mara, D.; Lane, J.; Scott, B.; Trouba, D. Sanitation and health. PLoS Med. 2010, 7, e1000363. [Google Scholar] [CrossRef] [PubMed]
- Strunz, E.C.; Addiss, D.G.; Stocks, M.E.; Ogden, S.; Utzinger, J.; Freeman, M.C. Water, sanitation, hygiene, and soil-transmitted helminth infection: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001620. [Google Scholar] [CrossRef] [PubMed]
- Mbuya, M.N.; Humphrey, J.H. Preventing environmental enteric dysfunction through improved water, sanitation and hygiene: An opportunity for stunting reduction in developing countries. Matern. Child Nutr. 2016, 12 (Suppl. 1), 106–120. [Google Scholar] [CrossRef] [PubMed]
- Kar, K.; Chambers, R. Handbook on Community-Led Total Sanitation; Plan UK & Institute of Development Studies at the University of Sussex: London, UK, 2008. [Google Scholar]
- UNICEF. Community-Led Total Sanitation in East Asia and Pacific: Progress, Lessons and Directions; East Asia and Pacific Regional Office, UNICEF: Bangkok, Thailand, 2013. [Google Scholar]
- UNICEF. Second Review of Community-Led Total Sanitation in the East Asia and Pacific Region Regional Report; East Asia and Pacific Regional Office, UNICEF: Bangkok, Thailand, 2015. [Google Scholar]
- Bicchieri, C. The Grammar of Society: The Nature and Dynamics of Social Norms; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Robinson, A.; Gnilo, E.M. Beyond ODF: A phased approach to rural sanitation development. In Sustainable Sanitation for All: Experiences, Challenges, and Innovations; Practical Action Publishing: Rugby, UK, 2016; pp. 153–166. [Google Scholar]
- UNICEF. Evaluation of the WASH Sector Strategy ‘Community Approaches to Total Sanitation’ (CATS); UNICEF: New York, NY, USA, 2014. [Google Scholar]
- Pickering, A.J.; Djebbari, H.; Lopez, C.; Coulibaly, M.; Alzua, M.L. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: A cluster-randomised controlled trial. Lancet Glob. Health 2015, 3, e701–e711. [Google Scholar] [CrossRef]
- Crocker, J.; Saywell, D.; Bartram, J. Sustainability of community-led total sanitation outcomes: Evidence from Ethiopia and Ghana. Int. J. Hyg. Environ. Health 2017, 220, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Garn, J.V.; Sclar, G.D.; Freeman, M.C.; Penakalapati, G.; Alexander, K.T.; Brooks, P.; Rehfuess, E.A.; Boisson, S.; Medlicott, K.O.; Clasen, T.F. The impact of sanitation interventions on latrine coverage and latrine use: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2017, 220, 329–340. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics Indonesia (BPS). Susenas (National Socio-Economic Survey); National Bureau of Statistics Indonesia: Jakarta, Indonesia, 2016.
- Torlesse, H.; Cronin, A.A.; Sebayang, S.K.; Nandy, R. Determinants of stunting in Indonesian children: Evidence from a cross-sectional survey indicate a prominent role for the water, sanitation and hygiene sector in stunting reduction. BMC Public Health 2016, 16, 669. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Road Map Nasional Percepatan Program STBM 2013–2015; Ministry of Health: Jakarta, Indonesia, 2013.
- Ministry of Health. STBM SMS-Based Monitoring Data in Indonesia. Available online: http://stbm-indonesia.org/monev/ (accessed on 1 September 2017).
- National Bureau of Statistics Indonesia (BPS). Alor Dalam Angka; National Bureau of Statistics Indonesia: Jakarta, Indonesia, 2016.
- Ministry of Health. STBM Verification Pocket Book; Ministry of Health: Jakarta, Indonesia, 2013.
- Hirai, M.; Kelsey, A.; Mattson, K.; Cronin, A.A.; Mukerji, S.; Graham, P.J. Determinants of toilet ownership among rural households in six eastern districts of Indonesia. J. Water Sanit. Hyg. Dev. 2017. under review. [Google Scholar]
- Jenkins, M.W.; Freeman, M.C.; Routray, P. Measuring the safety of excreta disposal behavior in India with the new safe san index: Reliability, validity and utility. Int. J. Environ. Res. Public Health 2014, 11, 8319–8346. [Google Scholar] [CrossRef] [PubMed]
- Routray, P.; Schmidt, W.P.; Boisson, S.; Clasen, T.; Jenkins, M.W. Socio-cultural and behavioural factors constraining latrine adoption in rural coastal Odisha: An exploratory qualitative study. BMC Public Health 2015, 15, 880. [Google Scholar] [CrossRef] [PubMed]
- Cameron, L.A.; Olivia, S.; Shah, M. Initial Conditions Matter: Social Capital and Participatory Development. IZA Discussion Paper No. 9653. 2015. Available online: https://pdfs.semanticscholar.org/81d9/cd20840728e392bfc65b2a6cca66b0072b23.pdf (accessed on 1 September 2017).
- Tyndale-Biscoe, P.; Bond, M.; Kidd, R. Plan International ODF Sustainability Study. Available online: www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/Plan_International_ODF_Sustainability_Study.pdf (accessed on 1 September 2017).
- Crocker, J.; Abodoo, E.; Asamani, D.; Domapielle, W.; Gyapong, B.; Bartram, J. Impact evaluation of training natural leaders during a community-led total sanitation intervention: A cluster-randomized field trial in Ghana. Environ. Sci. Technol. 2016, 50, 8867–8875. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Documentation of Good Wash Practice around STBM in Aceh Timur, Aech Province, Indonesia; UNICEF: Jakarta, Indonesia, 2015. [Google Scholar]
- Shakya, H.B.; Christakis, N.A.; Fowler, J.H. Association between social network communities and health behavior: An observational sociocentric network study of latrine ownership in rural India. Am. J. Public Health 2014, 104, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Hulland, K. What Factors Affect Sustained Adoption of Safe Water, Hygiene and Sanitation Technologies? A Systematic Review of Literature; EPPI—Centre, Social Science Research Unit, UCL Institute of Education, University College London: London, UK, 2015. [Google Scholar]
- Cronin, A.A.; Gnilo, M.E.; Odagiri, M.; Wijesekera, S. Equity implications for sanitation from recent health and nutrition evidence. Int. J. Equity Health 2017, 16, 211. [Google Scholar] [CrossRef] [PubMed]
- Dooley, T.; Maule, L.; Gnilo, E.M. Using social norms theory to strengthen cats impact and sustainability. In Sustainable Sanitation for All: Experiences, Challenges, and Innovations; Practical Action Publishing: Rugby, UK, 2016; pp. 299–314. [Google Scholar]
- Bicchieri, C.; Xiao, E. Do the right thing: But only if others do so. J. Behav. Decis. Mak. 2009, 22, 191–208. [Google Scholar] [CrossRef]
- Fuller, J.A.; Villamor, E.; Cevallos, W.; Trostle, J.; Eisenberg, J.N. I get height with a little help from my friends: Herd protection from sanitation on child growth in rural Ecuador. Int. J. Epidemiol. 2016, 45, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Alzua, M.L.; Osbert, N.; Pickering, A. Community-level sanitation coverage more strongly associated with child growth and household drinking water quality than access to a private toilet in rural Mali. Environ. Sci. Technol. 2017, 51, 7219–7227. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.T.; Lou, W.; Cheng, Y.L. Exposure-response relationship of neighbourhood sanitation and children’s diarrhoea. Trop. Med. Int. Health 2017, 22, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.A.; Grisham, T.; Slawsky, E.; Narine, L. An individual-level meta-analysis assessing the impact of community-level sanitation access on child stunting, anemia, and diarrhea: Evidence from DHS and MICS surveys. PLoS Negl. Trop. Dis. 2017, 11, e0005591. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, J.J.; Yeboah-Antwi, K.; Biemba, G.; Ram, P.K.; Osbert, N.; Sabin, L.L.; Hamer, D.H. Beliefs, behaviors, and perceptions of community-led total sanitation and their relation to improved sanitation in rural Zambia. Am. J. Trop. Med. Hyg. 2016, 94, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Aiemjoy, K.; Stoller, N.E.; Gebresillasie, S.; Shiferaw, A.; Tadesse, Z.; Sewent, T.; Ayele, B.; Chanyalew, M.; Aragie, S.; Callahan, K.; et al. Is using a latrine “strange thing to do”? A mixed-methods study of sanitation preference and behaviors in rural Ethiopia. Am. J. Trop. Med. Hyg. 2017, 96, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Nagel, C.L.; Schmidt, W.P.; Torondel, B.; Boisson, S.; Routray, P.; Clasen, T.F. Assessing patterns and determinants of latrine use in rural settings: A longitudinal study in Odisha, India. Int. J. Hyg. Environ. Health 2017, 220, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Barnard, S.; Routray, P.; Majorin, F.; Peletz, R.; Boisson, S.; Sinha, A.; Clasen, T. Impact of Indian Total Sanitation Campaign on latrine coverage and use: A cross-sectional study in Orissa three years following programme implementation. PLoS ONE 2013, 8, e71438. [Google Scholar] [CrossRef] [PubMed]
- Prabowo, H.; Huda, M.; Trimaya, L.; Cronin, A.A. 2016 Hygiene and Environmental Health in Islam; Majelis Ulama Indonesia (Indonesia Council of Islamic Scholars): Jakarta, Indonesia, 2016; p. 168. ISBN 978-602-99475-5-7. (In Indonesian) [Google Scholar]
- Sinha, A.; Nagel, C.L.; Thomas, E.; Schmidt, W.P.; Torondel, B.; Boisson, S.; Clasen, T.F. Assessing latrine use in rural India: A cross-sectional study comparing reported use and passive latrine use monitors. Am. J. Trop. Med. Hyg. 2016, 95, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, W.P. The elusive effect of water and sanitation on the global burden of disease. Trop. Med. Int. Health 2014, 19, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Cavill, S.; Chambers, R.; Vernon, N. 2015 Sustainability and CLTS: Taking stock. In Frontiers of CLTS: Innovations and Insights 4; CLTS Knowledge Hub, Institute of Development Studies, University of Sussex: Brighton, UK, 2015. [Google Scholar]
- Alzua, M.L.; Cardenas, J.; Djebbari, H. 2014 Community Mobilization Around Social Dilemmas: Evidence from Lab Experiments in Rural Mali. Documento de Trabajo, No. 160. Available online: https://www.econstor.eu/bitstream/10419/127679/1/cedlas-wp-160.pdf (accessed on 1 September 2017).
- Crocker, J.; Geremew, A.; Atalie, F.; Yetie, M.; Bartram, J. Teachers and sanitation promotion: An assessment of community-led total sanitation in Ethiopia. Environ. Sci. Technol. 2016, 50, 6517–6525. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Proportions (%) | |||||
|---|---|---|---|---|---|---|
| Village 1 | Village 2 | Village 3 | Village 4 | Village 5 | Village 6 | |
| (n = 77) | (n = 58) | (n = 77) | (n = 82) | (n = 153) | (n = 140) | |
| Age of respondents | ||||||
| 18–37 | 48.1 | 20.3 | 30.9 | 32.9 | 32.0 | 29.6 |
| 38–50 | 26.0 | 27.1 | 38.3 | 50.0 | 32.7 | 27.5 |
| >51 | 26.0 | 52.5 | 30.9 | 17.1 | 35.4 | 43.0 |
| Sex of respondents | ||||||
| Male | 32.9 | 74.6 | 65.4 | 68.3 | 79.6 | 70.4 |
| Female | 67.1 | 25.4 | 34.6 | 31.7 | 20.4 | 29.6 |
| Education level of respondents | ||||||
| Not complete Primary | 9.1 | 31.0 | 17.5 | 3.7 | 29.4 | 15.5 |
| Primary | 44.2 | 39.7 | 48.8 | 40.2 | 19.6 | 22.5 |
| Pre-secondary | 23.4 | 22.4 | 17.5 | 23.2 | 24.8 | 19.7 |
| Secondary or higher | 23.4 | 6.9 | 16.2 | 32.9 | 26.1 | 42.3 |
| Size of households | ||||||
| 1–3 | 20.0 | 25.4 | 29.6 | 13.4 | 25.2 | 32.4 |
| 4–6 | 62.7 | 40.7 | 45.7 | 53.7 | 49.0 | 51.4 |
| 7 or more | 17.3 | 33.9 | 24.7 | 32.9 | 25.8 | 16.2 |
| Year-round water access for household use | 98.7 | 94.8 | 42.9 | 100 | 73.2 | 100 |
| Access to improved sanitation | 96.1 | 86.2 | 55.8 | 98.8 | 92.8 | 86.4 |
| Wealth quintile | ||||||
| Richest | 37.7 | 1.7 | 2.5 | 47.6 | 6.4 | 32.4 |
| Richer | 24.7 | 11.9 | 8.6 | 29.3 | 14 | 25.4 |
| Middle | 16.9 | 22 | 18.5 | 22.0 | 18.5 | 23.9 |
| Poorer | 19.5 | 37.3 | 30.9 | 0 | 14.6 | 16.9 |
| Poorest | 1.3 | 27.1 | 39.5 | 1.2 | 46.5 | 1.4 |
| Questions/Statements | Type of Expectations/Beliefs | Proportions of Households in Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| Village 1 (n = 77) | Village 2 (n = 58) | Village 3 (n = 77) | Village 4 (n = 82) | Village 5 (n = 153) | Village 6 (n = 140) | All 6 ODF Villages (n = 587) | ||
| Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people, how many do you think said that the members of their household always use a latrine? (More than or equal to 8) | Empirical expectations | 90.7 | 76.3 | 34.6 | 100 | 93.4 | 39.0 | 71.4 |
| Think about the people in your village, such as your family, friends, and neighbours. Out of 10 people, how many do you think said that people should use a latrine because it is the right thing to do? (More than or equal to 8) | Normative expectations | 90.7 | 76.3 | 67.9 | 100 | 94 | 33.1 * | 74.8 |
| If someone in your village was observed defecating in the open, would any sanction happen to the person (Yes) | Not applicable | 36 | 91.5 | 30.4 | 70.4 | 17.5 | 5 | 33.3 |
| Most people in this community do not have a toilet. (Strongly agree/agree) | Empirical expectations | 2.6 | 11.9 | 28.4 * | 0 | 0.6 | 3.5 | 6.4 |
| People in your village should use a toilet. (Strongly agree/agree) | Normative belief | 97.4 | 93.2 | 92.6 | 98.8 | 96.1 | 93.7 | 95.3 |
| A lot of people think it is too expensive to have a toilet in their house. (Strongly agree/agree) | Factual belief | 13 | 18.6 | 32.5 | 1.2 | 3.9 | 37.3 | 18 |
| In this community, it is acceptable to defecate in the open. (Strongly agree/agree) | Factual belief | 0 | 5.1 | 2.5 | 1.2 | 6.5 | 2.1 | 3.2 |
| It is embarrassing when people can see others defecating in the open. (Strongly agree/agree) | Normative belief | 92.2 | 81.4 | 70.4 | 70.7 | 80 | 85.2 | 80.4 |
| Most people feel ashamed to not have a toilet in their house. (Strongly agree/agree) | Factual belief | 85.7 | 89.8 | 76.5 | 74.4 | 79.4 | 70.4 | 78 |
| It is not a problem defecating on the beach, or in a river. (Strongly agree/agree) | Factual belief | 5.2 | 0 | 4.9 | 1.2 | 0.7 | 2.8 | 2.4 |
| Any household member participated in a meeting about sanitation or has any government staff visited your home to talk about sanitation. (Yes) | Not applicable | 85.7 | 96.6 | 33.3* | 69.5 | 71.6 | 63.1 | 68.4 |
| I know that this community was verified as an ODF. (Yes) | Not applicable | 93.5 | 100 | 30.9* | 73 | 90.3 | 81 | 78.6 |
| Factors | Slippage in all Households | Slippage in Households Owning a Private Latrine | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Slippage Rate (%) | Adjusted OR | 95% CI | p-Value | N | Slippage Rate (%) | Adjusted OR | 95% CI | p-Value | |
| Gender | ||||||||||
| Male | 402 | 13 | 0.61 | (0.31–1.21) | 0.159 | 357 | 8 | 0.50 | (0.27–0.92) | 0.025 |
| Female | 193 | 18 | Ref | 165 | 15 | Ref | ||||
| Age (years) | ||||||||||
| 18–37 | 189 | 19 | 1.16 | (0.77–1.75) | 0.464 | 158 | 13 | 1.17 | (0.50–2.75) | 0.722 |
| 38–50 | 195 | 10 | 0.48 | (0.36–0.63) | <0.001 | 172 | 7 | 0.47 | (0.25–0.88) | 0.018 |
| >51 | 202 | 15 | Ref | 182 | 13 | Ref | ||||
| Education | ||||||||||
| Not complete Primary | 109 | 16 | 1.11 | (0.39–3.19) | 0.846 | 93 | 12 | 0.91 | (0.41–2.02) | 0.820 |
| Primary | 191 | 18 | 1.12 | (0.54–2.30) | 0.762 | 159 | 12 | 1.18 | (0.79–1.77) | 0.417 |
| Pre-secondary | 128 | 13 | 0.94 | (0.36–2.47) | 0.907 | 116 | 10 | 1.12 | (0.43–2.93) | 0.819 |
| Secondary or higher | 162 | 11 | Ref | 149 | 9 | Ref | ||||
| Size of households | ||||||||||
| 1–3 | 149 | 13 | 0.72 | (0.39–1.32) | 0.288 | 129 | 9 | 0.31 | (0.15–0.64) | 0.002 |
| 4–6 | 298 | 15 | 0.98 | (0.79–1.23) | 0.880 | 261 | 10 | 0.52 | (0.29–0.91) | 0.023 |
| 7 or more | 141 | 15 | Ref | 124 | 13 | Ref | ||||
| Presence of a child under 5 years old | ||||||||||
| Yes | 290 | 15 | 0.96 | (0.69–1.33) | 0.793 | 243 | 9 | 1.24 | (0.83–1.85) | 0.288 |
| No | 306 | 14 | Ref | 279 | 11 | Ref | ||||
| Wealth quintile | ||||||||||
| Poorest | 124 | 23 | 2.36 | (1.05–5.27) | 0.037 | 101 | 14 | 3.85 | (1.90–7.81) | <0.001 |
| Poorer | 109 | 19 | 2.26 | (1.04–4.90) | 0.039 | 84 | 13 | 3.33 | (0.95–11.70) | 0.061 |
| Middle | 122 | 11 | 1.37 | (0.73–2.57) | 0.324 | 109 | 9 | 2.08 | (1.12–3.87) | 0.020 |
| Richer | 115 | 16 | 2.68 | (1.01–7.11) | 0.048 | 108 | 14 | 4.46 | (1.20–16.62) | 0.026 |
| Richest | 127 | 5 | Ref | 120 | 4 | |||||
| All year round water access for household needs | ||||||||||
| Yes | 498 | 11 | 0.60 | (0.39–0.93) | 0.021 | 450 | 10 | 0.49 | (0.41–0.58) | <0.001 |
| No | 91 | 34 | Ref | 65 | 18 | Ref | ||||
| Most people do not have a toilet. | ||||||||||
| No | 556 | 12 | 0.36 | (0.19–0.67) | 0.001 | 500 | 10 | 0.21 | (0.05–0.90) | 0.036 |
| Strongly agree/agree | 38 | 50 | Ref | 21 | 33 | Ref | ||||
| It is not problem defecating on the beach or in a river. | ||||||||||
| No | 577 | 13 | 0.44 | (0.21–0.92) | 0.030 | |||||
| Strongly agree/agree | 14 | 23 | Ref | |||||||
| Satisfaction with a latrine | ||||||||||
| Satisfied | 461 | 10 | 0.32 | (0.09–1.08) | 0.066 | |||||
| Dissatisfied | 34 | 26 | Ref | |||||||
| Cleaner and healthier living in our home | ||||||||||
| Yes | 389 | 8 | 0.50 | (0.30–0.81) | 0.006 | |||||
| No | 133 | 17 | Ref | |||||||
| To avoid sharing with others | ||||||||||
| Yes | 35 | 29 | 15.41 | (1.99–119.25) | 0.009 | |||||
| No | 487 | 9 | Ref | |||||||
| Factors | Private latrine Ownership | ||||
|---|---|---|---|---|---|
| N | Latrine Ownership (%) | Adjusted OR | 95% CI | p-Value | |
| Gender | |||||
| Female | 191 | 89 | Ref | ||
| Male | 403 | 86 | 0.70 | (0.33–1.48) | 0.349 |
| Age (years) | |||||
| 18–37 | 189 | 84 | 0.45 | (0.24–0.84) | 0.012 |
| 38–50 | 195 | 88 | 0.41 | (0.22–0.76) | 0.004 |
| >51 | 201 | 91 | Ref | ||
| Education | |||||
| Not complete Primary | 108 | 86 | 0.78 | (0.22–2.78) | 0.702 |
| Primary | 190 | 84 | 0.50 | (0.26–0.99) | 0.048 |
| Pre–secondary | 129 | 91 | 1.11 | (0.84–1.49) | 0.461 |
| Secondary or higher | 162 | 92 | Ref | ||
| Size of households | |||||
| 1–3 | 149 | 87 | 0.42 | (0.16–1.13) | 0.087 |
| 4–6 | 297 | 88 | 0.95 | (0.48–1.91) | 0.895 |
| 7 or more | 141 | 88 | Ref | ||
| Presence of a child under 5 years old | |||||
| Yes | 290 | 84 | 3.31 | (2.03–5.41) | <0.001 |
| No | 306 | 92 | Ref | ||
| Wealth quintile | |||||
| Poorest | 125 | 81 | 0.15 | (0.04–0.59) | 0.007 |
| Poorer | 106 | 80 | 0.22 | (0.05–0.88) | 0.033 |
| Middle | 122 | 89 | 0.41 | (0.25–0.66) | <0.001 |
| Richer | 115 | 94 | 0.86 | (0.30–2.49) | 0.785 |
| Richest | 127 | 94 | |||
| All year round water access for household needs | |||||
| Yes | 498 | 91 | 1.76 | (0.96–3.23) | 0.067 |
| No | 90 | 72 | Ref | ||
| Most people do not have a toilet. | |||||
| Strongly agree/agree | 38 | 55 | 2.40 | (1.41–4.09) | 0.001 |
| No | 556 | 90 | Ref | ||
| A lot of people think it is too expensive to have toilet in their house. | |||||
| Strongly agree/agree | 107 | 68 | Ref | ||
| No | 486 | 92 | 3.25 | (1.16–9.13) | 0.025 |
| It is embarrassing when people can see others defecating in the open. | |||||
| Strongly agree/agree | 477 | 90 | Ref | ||
| No | 117 | 80 | 0.47 | (0.20–1.08) | 0.076 |
| It is not problem defecating on the beach or in a river. | |||||
| Strongly agree/agree | 14 | 36 | Ref | ||
| No | 577 | 89 | 23.28 | (7.70–70.34) | <0.001 |
| How many do you think said that the members of their household always use a latrine (Scale: 0 to 10) | |||||
| 1.32 | (1.19–1.46) | <0.001 | |||
| Theme | Village 1 | Village 2 |
| STBM triggering | Facilitated by Puskesmas. | Facilitated by Puskesmas |
| Key message dissemination mechanisms after triggering to become ODF | The STBM team actively visited each household. Further sanitation promotion message was disseminated through church, mosque and community meetings. | The STBM team actively visited each household. Further message dissemination was done from church. |
| Presence of community support mechanisms to build and/or improve a latrine | Local support revolving fund (Arisan) & village government support to poorest household with some non-local materials. | Households were responsible to build a latrine with support from neighbors using “gotong royong” modality. |
| Key message dissemination mechanisms after ODF verification | Religious leaders and a local women’s group kept disseminating sanitation and other hygiene messages to motivate households. | Religious leaders kept disseminating messages. A local women’s group and cadres regularly visited households for hygiene promotion. |
| Community challenges to become ODF | Economic conditions of households affect latrine adoption. However, everyone support each other through Arisan and Gotong royong. The village government also provided financial/in-kind support. | Most people work as a farmer, and spend most their time in their fields, being unable to find time to build a latrine. Access to water is challenging during dry season. |
| Social norms creation | A local women’s group member said, “I believe that all people use a latrine. A few families still use a shared latrine, but I don’t see anyone defecating in the open. People in this village will feel ashamed to defecate in the open.” | All people in the community would say other think that all people should use a latrine to protect community health. People also feel comfortable using a latrine as it meets people’s privacy. |
| Theme | Village 3 | Village 4 |
| STBM triggering | Facilitated by Puskesmas | Facilitated by Puskesmas |
| Key message dissemination mechanisms after triggering to become ODF | Cadres continued to motivate the community. The head of village strongly encouraged community members to build a latrine. | Sanitation promotion messages were disseminated from mosques to improve latrines. |
| Presence of community support mechanisms to build and/or improve a latrine | No mechanism to support households to build or improve latrine was mentioned. | The poorest families received financial support from the District Government (~$40 USD) for improving a latrine. |
| Key message dissemination mechanisms to become ODF after triggering | No specific dissemination mechanisms were mentioned. | Religious leaders kept disseminating sanitation/hygiene promotion messages through mosques and churches |
| Community challenges to become ODF | The most challenging barrier is economic conditions of households who cannot afford to build an improved latrine. Water access during dry seasons is also a big barrier. | Most peoples in this village are farmers and working in the filed for a whole day. It is challenging to allocate their time to build a toilet. |
| Social norms creation | “A new family will build a latrine when building a house as all people in the community would feel ashamed if they did not have a latrine.” | “A new family will build a latrine when building a house as all people in the community would feel ashamed if they did not have a latrine.” |
| Theme | Village 5 | Village 6 |
| STBM triggering | Facilitated by Puskesmas | Facilitated by Puskesmas |
| Key message dissemination mechanisms after triggering to become ODF | Religious leaders promoted sanitation adoption and use through sermon. Community leaders and a local women’s group regularly visited households. | Sanitation promotion messages were disseminated from mosques. Cadres disseminated hygiene message to mothers. |
| Presence of community support mechanisms to build and/or improve a latrine | Households improved their toilet with Arisan and Gotong royong mechanisms. | Gotong royong was the main social capital for acceleration of sanitation promotion. For the poorest, financial support from the village was provided to buy cement for building a latrine |
| Key message dissemination mechanisms to become ODF after triggering | Community leaders and a local women’s group members kept disseminating sanitation/hygiene promotion messages. | Religious leaders kept disseminating sanitation promotion messages. Cadres also disseminated the hygiene practice messages to mothers. |
| Community challenges to become ODF | According to the village leader. “it is challenging for people to build an improve latrine because of lack of locally available materials. However, through Arisan and Gotong royong, people can overcome this.” | The poorest households are slow to build latrine. The village government provides in-kind support such as cements for latrine construction. |
| Social norms creation | A local women’s group member said, “We would feel ashamed and guilty if a guest saw a poor quality of a latrine. Having an improved latrine is a pride.” | All people in the community use a latrine because there is strong feeling of shame defecating in the open, pride of families owning an improved toilet as part of faith. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odagiri, M.; Muhammad, Z.; Cronin, A.A.; Gnilo, M.E.; Mardikanto, A.K.; Umam, K.; Asamou, Y.T. Enabling Factors for Sustaining Open Defecation-Free Communities in Rural Indonesia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 1572. https://doi.org/10.3390/ijerph14121572
Odagiri M, Muhammad Z, Cronin AA, Gnilo ME, Mardikanto AK, Umam K, Asamou YT. Enabling Factors for Sustaining Open Defecation-Free Communities in Rural Indonesia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2017; 14(12):1572. https://doi.org/10.3390/ijerph14121572
Chicago/Turabian StyleOdagiri, Mitsunori, Zainal Muhammad, Aidan A. Cronin, Michael E. Gnilo, Aldy K. Mardikanto, Khaerul Umam, and Yameha T. Asamou. 2017. "Enabling Factors for Sustaining Open Defecation-Free Communities in Rural Indonesia: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 14, no. 12: 1572. https://doi.org/10.3390/ijerph14121572
APA StyleOdagiri, M., Muhammad, Z., Cronin, A. A., Gnilo, M. E., Mardikanto, A. K., Umam, K., & Asamou, Y. T. (2017). Enabling Factors for Sustaining Open Defecation-Free Communities in Rural Indonesia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 14(12), 1572. https://doi.org/10.3390/ijerph14121572