The Metal Neurotoxins: An Important Role in Current Human Neural Epidemics?

Abstract
1. Introduction
2. The Major Neurotoxicants and Their Toxicity
The Neurotoxic Six Metal Elements and Their Compounds
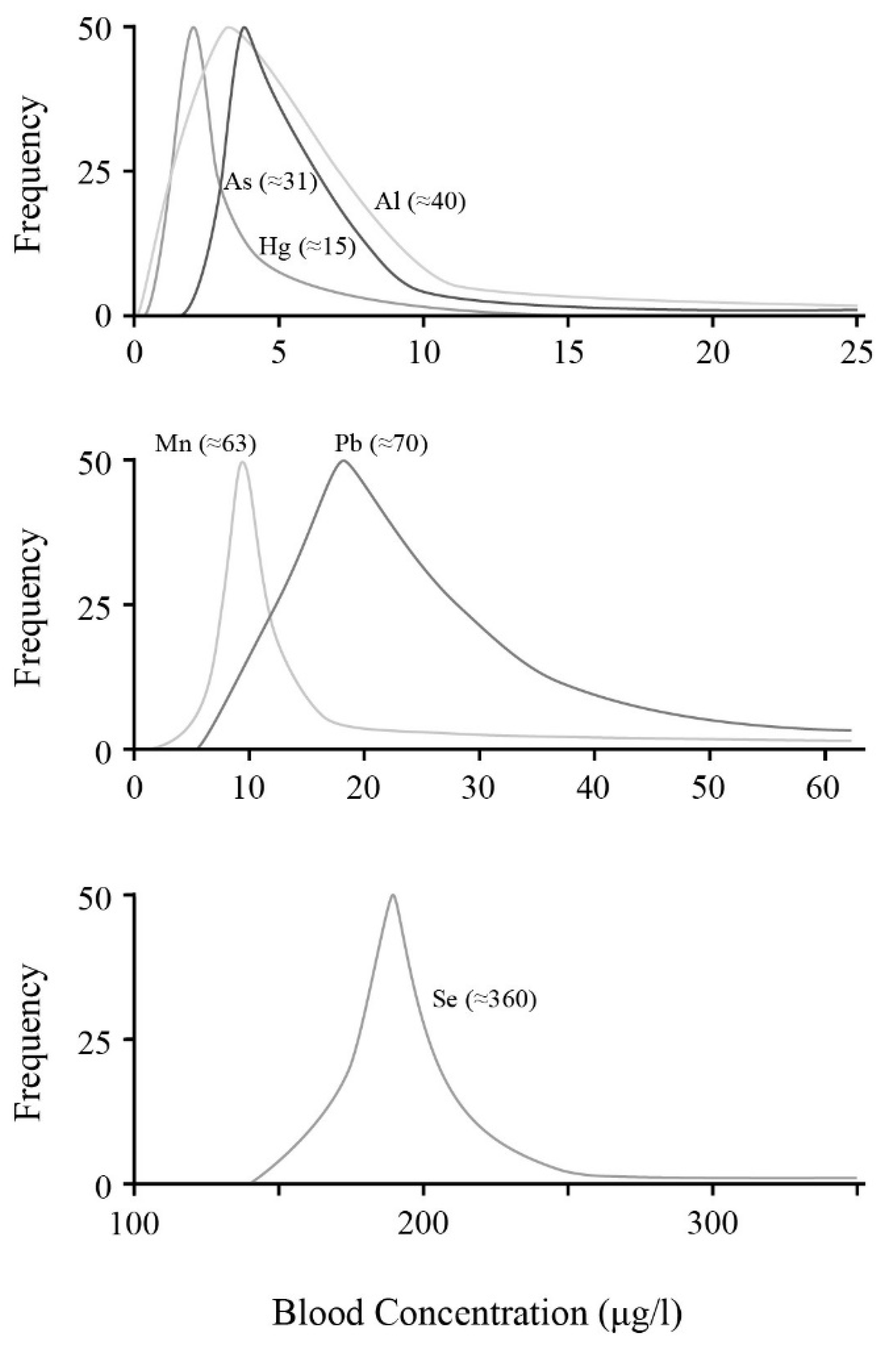
3. Blood Level Neurotoxins in the General Populace
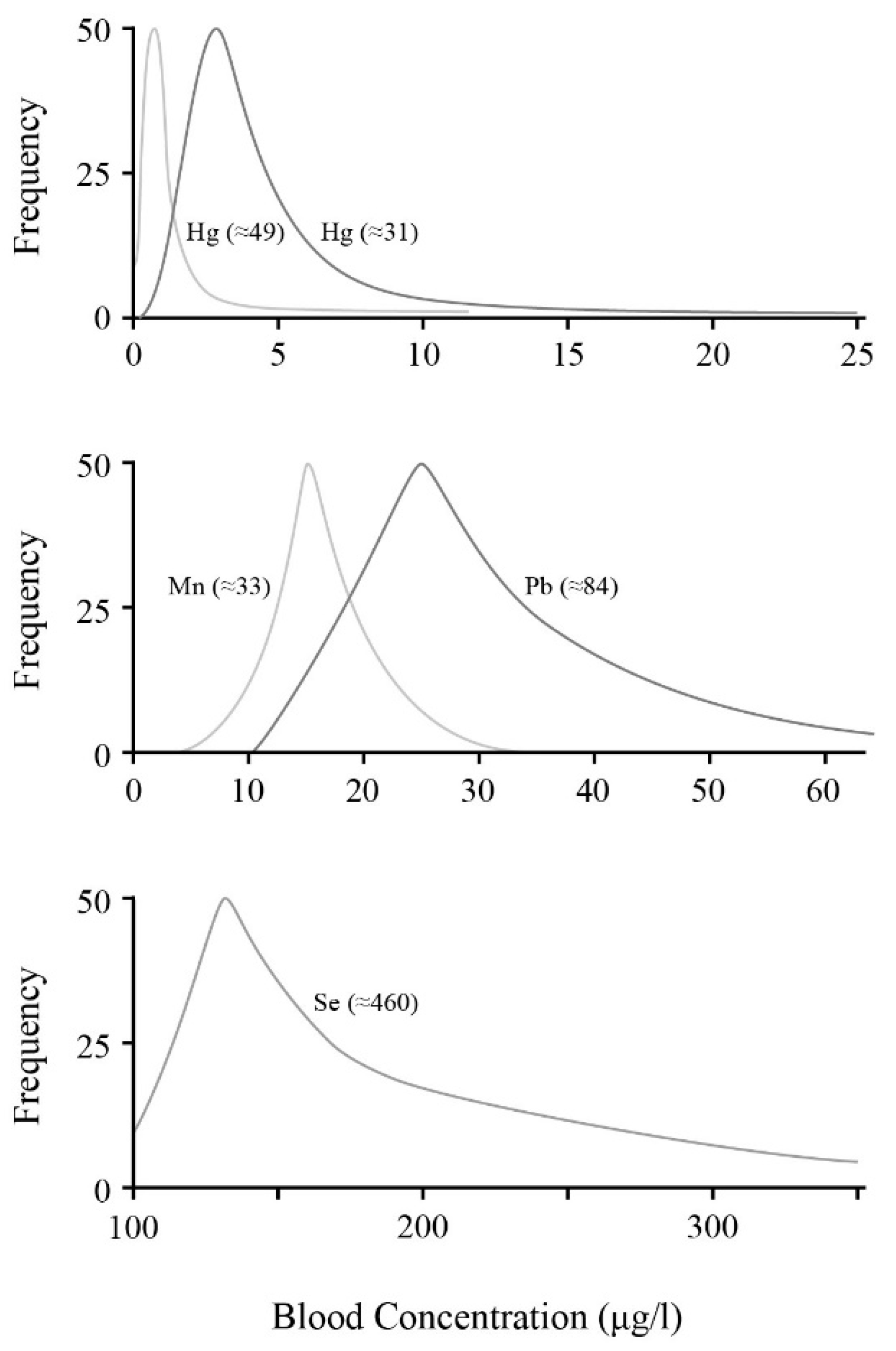
4. Blood Level Neurotoxins in Pregnant Women
5. Why Now?
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Wright, K. Our preferred poison. Discover 2005, 26, 58–65. [Google Scholar]
- O’Malley, G.F. The blood of my veins-mercury, Minamata and the soul of Japan. Clin. Toxicol. 2017, 55, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Sealey, L.A.; Hughes, B.W.; Sriskanda, A.N.; Guest, J.R.; Gibson, A.D.; Johnson-Williams, L.; Pace, D.G.; Bagasra, O. Environmental factors in the development of autism spectrum disorders. Environ. Int. 2016, 88, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Morisaki, N.; Honda, Y.; Sampei, M.; Tani, Y. Chemicals, nutrition, and autism spectrum disorder: A mini-review. Front. Neurosci. 2016, 10, 174. [Google Scholar] [CrossRef] [PubMed]
- Christensen, D.L.; Baio, J.; van Naarden Braun, K.; Bilder, D.; Charles, J.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years: Autism and developmental disabilities monitoring network, 11 sites, United States, 2012. Surveill. Summ. 2016, 65, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Kamimura-Nishimura, K.; Froehlich, T.; Chirdkiatgumchai, V.; Adams, R.; Fredstrom, B.; Manning, P. Autism spectrum disorders and their treatment with psychotropic medications in a nationally representative outpatient sample: 1994–2009. Ann. Epidemiol. 2017, 27, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Jerome, L.; Segal, A.; Habinski, L. What we know about ADHD and driving risk: A literature review, meta-analysis and critique. J. Can. Acad. Child Adolesc. Psychiatry 2006, 15, 105–125. [Google Scholar] [PubMed]
- Hickman, R.A.; Faustin, A.; Wisniewski, T. Alzheimer disease and its growing epidemic: Risk factors, biomarkers, and the urgent need for therapeutics. Neurol. Clin. 2016, 34, 941–953. [Google Scholar] [CrossRef] [PubMed]
- Brewer, G.J. Copper-2 hypothesis for causation of the current Alzheimer’s disease epidemic together with dietary changes that enhance the epidemic. Chem. Res. Toxicol. 2017, 30, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Vaz, F.N.C.; Fermino, B.L.; Haskel, M.V.L.; Wouk, J.; de Freitas, G.B.L.; Fabbri, R.; Montagna, E.; Rocha, J.B.T.; Bonini, J.S. The relationship between copper, iron, and selenium levels and Alzheimer’s disease. Biol. Trace Elem. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, P. Mercury exposure and Alzheimer’s disease in India: An imminent threat? Sci. Total Environ. 2017, 589, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Canevelli, M.; Blasimme, A.; Cesari, M. Societal and global implications of the “dementia epidemic”: The example of the London Heathrow airport. Eur. J. Epidemiol. 2017, 32, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Stromland, K.; Nordin, V.; Miller, M.; Akerstrom, B.; Gillberg, C. Autism in Thalidomide embryopathy: A population study. Dev. Med. Child Neurol. 1994, 36, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Jager, T. All individuals are not created equal: Accounting for individual variation in fitting life-history responses to toxicants. Environ. Sci. Technol. 2013, 47, 1664–1669. [Google Scholar] [CrossRef] [PubMed]
- Everts, S. Brain barrier. Chem. Eng. News 2007, 85, 33–36. [Google Scholar] [CrossRef]
- Bauer, H.-C.; Krizbai, I.A.; Bauer, H.; Traweger, A. “You shall not pass”: Tight junctions of the blood brain barrier. Front. Neurosci. 2014, 8, 392. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.T.; Harry, G.J.; Hayden, K.M.; Szabo, D.T.; Birnbaum, L. Comparison of metal levels between postmortem brain and ventricular fluid in Alzheimer’s disease and non-demented elderly controls. Toxicol. Sci. 2016, 150, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Prakash, A.; Dhaliwal, G.K.; Kumar, P.; Majeed, A.B. Brain biometals and Alzheimer’s diseases: Boon or bane? Int. J. Neurosci. 2017, 127, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Kasa, P.; Szerdahelyi, P.; Wisniewski, H.M. Lack of topographical relationship between sites of aluminum deposition and senile plaques in the Alzheimer’s disease brain. Acta Neuropathol. 1995, 90, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.R. Aluminum in hippocampal neurons from humans with Alzheimer’s disease. Neurotoxicology 2006, 27, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, S.; Zhao, Y.; Hill, J.M.; Culicchia, F.; Kruck, T.P.; Percy, M.E.; Pogue, A.I.; Walton, J.R.; Lukiw, W.J. Selective accumulation of aluminum in cerebral arteries in Alzheimer’s disease. J. Inorg. Biochem. 2013, 126, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Exley, C.; Vickers, T. Elevated brain aluminum and early onset Alzheimer’s disease in an individual occupationally exposed to aluminum: A case report. J. Med. Case Rep. 2014, 8. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. Higher levels of mercury in brain are not linked to increased risk of Alzheimer’s, study finds. Br. Med. J. 2016, 352, i611. [Google Scholar] [CrossRef] [PubMed]
- Cernichiari, E.; Brewer, R.; Myers, G.J.; Marsh, D.O.; Lapham, L.W.; Cox, C.; Shamlaye, C.F.; Berlin, M.; Davidson, P.W.; Clarkson, T.W. Monitoring methylmercury during pregnancy: Maternal hair predicts fetal brain exposure. Neurotoxicology 1995, 16, 705–710. [Google Scholar] [PubMed]
- Davidson, P.W.; Cory-Slechta, D.A.; Thurston, S.W.; Huang, L.S.; Shamlaye, C.F.; Gunzler, D.; Watson, G.E.; van Wijngaarden, E.; Zareba, G.; Klein, J.D.; et al. Fish consumption and prenatal methylmercury exposure: Cognitive and behavioral outcomes in the main cohort at 17 years from the Seychelles child development study. Neurotoxicology 2011, 32, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, E.; Thurston, S.W.; Myers, G.J.; Harrington, D.; Cory-Slechta, D.A.; Strain, J.J.; Watson, G.E.; Zareba, G.; Love, T.; Henderson, J.; et al. Methylmercury exposure and neurodevelopmental outcomes in the Seychelles child development study main cohort at age 22 and 24 years. Neurotoxicol. Teratol. 2017, 59, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Murata, K.; Bjerve, K.S.; Choi, A.L.; Weihe, P.; Grandjean, P. Visual evoked potentials in children prenatally exposed to methylmercury. Neurotoxicology 2013, 37, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.L.; Muckle, G.; Ayotte, P.; Dewailly, E.; Jacobson, S.W. Relation of prenatal methylmercury exposure from environmental sources to childhood IQ. Environ. Health Perspect. 2015, 123, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Debes, F.; Weihe, P.; Grandjean, P. Cognitive deficits at age 22 years associated with prenatal exposure to methylmercury. Cortex 2016, 74, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Hachiya, N.; Murata, K.-Y.; Nakanishi, I.; Kondo, T.; Yasutake, A.; Miyamoto, K.-I.; Ser, P.H.; Omi, S.; Furusawa, H.; et al. Methylmercury exposure and neurological outcomes in Taiji residents accustomed to consuming whale meat. Environ. Int. 2014, 68, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Polak-Juszczak, L. Selenium and mercury molar ratios in commercial fish from the Baltic Sea: Additional risk assessment criterion for mercury exposure. Food Control 2015, 50, 881–888. [Google Scholar] [CrossRef]
- Squadrone, S.; Benedetto, A.; Brizio, P.; Prearo, M.; Abete, M.C. Mercury and selenium in European catfish (Silurus glanis) from Northern Italian rivers: Can molar ratio be a predictive factor for mercury toxicity in a top predator? Chemosphere 2015, 119, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Ser, P.H.; Omi, S.; Shimizu-Furusawa, H.; Yasutake, A.; Sakamoto, M.; Hachiya, N.; Konishi, S.; Nakamura, M.; Watanabe, C. Differences in the responses of three plasma selenium containing proteins in relation to methylmercury exposure through consumption of fish/whales. Toxicol. Lett. 2017, 267, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Mundy, W.R.; Padilla, S.; Breier, J.M.; Crofton, K.M.; Gilbert, M.E.; Herr, D.W.; Jensen, K.F.; Radio, N.M.; Raffaele, K.C.; Schumacher, K.; et al. Expanding the test set: Chemicals with potential to disrupt mammalian brain development. Neurotoxicol. Teratol. 2015, 52, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, J.; Yonezawa, T.; Ueyama, M. Acute thallotoxicosis: Neuropathological and spectrophotometric studies on an autopsy case. J. Toxicol. Sci. 1978, 3, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Kippler, M.; Tofail, F.; Hamadani, J.D.; Gardner, R.M.; Grantham-McGregor, S.M.; Bottai, M.; Vahter, M. Early-life cadmium exposure and child development in 5-year old girls and boys: A cohort study in rural Bangladesh. Environ. Health Perspect. 2012, 120, 1462–1468. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.E.; Valentiner, E.; Maxson, P.; Miranda, M.L.; Fry, R.C. Maternal cadmium levels during pregnancy associated with lower birth weight in infants in a North Carolina cohort. PLoS ONE 2014, 9, e109661. [Google Scholar] [CrossRef] [PubMed]
- Faroon, O.; Ashizawa, A.; Wright, S.; Tucker, P.; Jenkins, K.; Ingerman, L.; Rudisill, C. Toxicological Profile for Cadmium; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2012; p. 487. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Sigel, A.; Sigel, H.; Sigel, R.K.O. (Eds.) Cadmium from Toxicity to Essentiality; Metal Ions in Life Sciences; Springer: Dordrecht, The Netherlands, 2013; Volume 11, p. 588. [Google Scholar]
- Williams, M.; Todd, G.D.; Roney, N.; Crawford, J.; Coles, C.; McClure, P.R.; Garey, J.D.; Zaccaria, K.; Citra, M. Toxicological Profile for Manganese; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2012; p. 556. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Fordyce, F. Selenium geochemistry and health. AMBIO 2007, 36, 94–97. [Google Scholar] [CrossRef]
- Desta, B.; Maldonado, G.; Reid, H.; Puschner, B.; Maxwell, J.; Agasan, A.; Humphreys, L.; Holt, T. Acute selenium toxicosis in polo ponies. J. Vet. Diagn. Investig. 2011, 23, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Nishijo, M.; Pham, T.T.; Nguyen, A.T.; Tran, N.N.; Nakagawa, H.; Hoang, L.V.; Tran, A.H.; Morikawa, Y.; Ho, M.D.; Kido, T.; et al. 2,3,7,8-Tetrachlorodibenzo-p-dioxin in breast milk increases autistic traits of 3-year-old children in Vietnam. Mol. Psychiatry 2014, 19, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Long, M.H.; Knudsen, A.-K.S.; Pedersen, H.S.; Bonefeld-Jorgensen, E.C. Food intake and serum persistent organic pollutants in the Greenlandic pregnant women: The ACCEPT sub-study. Sci. Total Environ. 2015, 529, 198–212. [Google Scholar] [CrossRef] [PubMed]
- Ostrea, E.M., Jr.; Mantaring, J.B., III; Silvestre, M.A. Drugs that affect the fetus and newborn infant via the placenta or breast milk. Pediatr. Clin. N. Am. 2004, 51, 539–579. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Jurewicz, J.; Hanke, W. Review of current evidence on the impact of pesticides, polychlorinated biphenyls and selected metals on attention deficit/hyperactivity disorder in children. Int. J. Occup. Med. Environ. Health 2013, 26, 16–38. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, C.; Sasaki, S.; Saijo, Y.; Okada, E.; Kobayashi, S.; Baba, T.; Kajiwara, J.; Todaka, T.; Iwasaki, Y.; Nakazawa, H.; et al. Demographic, behavioral, dietary, and socioeconomic characteristics related to persistent organic pollutants and mercury levels in pregnant women in Japan. Chemosphere 2015, 133, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Yokel, R.A.; Lasley, S.M.; Dorman, D.C. The speciation of metals in mammals influences their toxicokinetics and toxicodynamics and therefore human health risk assessment. Toxicol. Environ. Health B Crit. Rev. 2006, 9, 63–85. [Google Scholar] [CrossRef] [PubMed]
- Dopp, E.; Kligerman, A.D.; Diaz-Bone, R.A. Organoarsenicals: Uptake, metabolism and toxicity. In Metal Ions in Life Sciences: Volume 7. Organometallics in Environment and Toxicology; Sigel, A., Sigel, H., Sigel, R.K.O., Eds.; Royal Society of Chemistry: London, UK, 2010; Chapter 7; pp. 231–265. [Google Scholar]
- Ceccatelli, S.; Dare, E.; Moors, M. Methylmercury-induced neurotoxicity and apoptosis. Chem. Biol. Interact. 2010, 188, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Hooker, B.; Kern, J.; Geier, D.; Haley, B.; Sykes, L.; King, P.; Geier, M. Methodological issues and evidence of malfeasance in research purporting to show Thimerosal in vaccines is safe. BioMed Res. Int. 2014, 8, 247218. [Google Scholar] [CrossRef] [PubMed]
- Geier, D.A.; Kern, J.K.; Geier, M.R. Increased risk for an atypical autism diagnosis following Thimerosal-containing vaccine exposure in the United States: A prospective longitudinal case-control study in the vaccine safety datalink. J. Trace Elem. Med. Biol. 2017, 42, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G. Low-dose Thimerosal in pediatric vaccines: Adverse effects in perspective. Environ. Res. 2017, 152, 280–293. [Google Scholar] [CrossRef] [PubMed]
- Keith, S.; Jones, D.; Rosemond, Z.; Ingerman, L.; Chappell, L. Toxicological Profile for Aluminum; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2008; p. 357. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Krewski, D.; Yokel, R.A.; Nieboer, E.; Borchelt, D.; Cohen, J.; Harry, J.; Kacew, S.; Lindsay, J.; Mahfouz, A.M.; Rondeau, V. Human health risk assessment for aluminum, aluminum oxide and aluminum hydroxide. J. Toxicol. Environ. Health B 2007, 10, 1–269. [Google Scholar] [CrossRef] [PubMed]
- Tomljenovic, L.; Shaw, C.A. Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J. Inorg. Biochem. 2011, 105, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Tomljenovic, L. Aluminum and Alzheimer’s disease: After a century of controversy, is there a plausible link? J. Alzheimer’s Dis. 2011, 23, 567–598. [Google Scholar] [CrossRef]
- Yokel, R.A. Brain uptake, retention, and efflux of aluminum and manganese. Environ. Health Perspect. 2002, 110 (Suppl. 5), 699–704. [Google Scholar] [CrossRef] [PubMed]
- Yumoto, S.; Nagai, H.; Matsuzaki, H.; Matsumura, H.; Tada, W.; Nagatsuma, E.; Kobayashi, K. Aluminum incorporation into the brain of rat fetuses and sucklings. Brain Res. Bull. 2001, 55, 229–234. [Google Scholar] [CrossRef]
- Bishop, N.J.; Morley, R.; Day, J.P.; Lucas, A. Aluminum neurotoxicity in preterm infants receiving intravenous-feeding solutions. N. Engl. J. Med. 1997, 336, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Burrell, S.A.; Exley, C. There is (still) too much aluminum in infant formulas. BMC Pediatr. 2010, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G.; Marques, R.C. Infants’ exposure to aluminum from vaccines and breast milk during the first 6 months. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Maya, S.; Prakash, T.; Madhu, K.D.; Goli, D. Multifaceted effects of aluminum in neurodegenerative diseases: A review. Biomed. Pharmacother. 2016, 83, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.P.; Mold, M.; Mery, L.; Cottier, M.; Exley, C. Aluminum content of human semen: Implications for semen quality. Reprod. Toxicol. 2014, 50, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Abadin, H.; Ashizawa, A.; Stevens, Y.W.; Llados, F.; Diamond, G.; Sage, G.; Citra, M.; Quinones, A.; Bosch, S.J.; Swarts, S.G. Toxicological Profile for Lead; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2007; p. 582. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Final Review of Scientific Information on Lead; United Nations Environment Program: Nairobi, Kenya, 2010; p. 332. Available online: http://www.unep.org (accessed on 29 November 2017).
- Vorvolakos, T.; Arseniou, S.; Samakouri, M. There is no safe threshold for lead exposure: A literature review. Psychiatriki 2016, 27, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Reuben, A.; Caspi, A.; Belsky, D.W.; Broadbent, J.; Harrington, H.; Sugden, K.; Houts, R.M.; Ramrakha, S.; Poulton, R.; Moffitt, T.E. Association of childhood blood lead levels with cognitive function and socioeconomic mobility between childhood and adulthood. J. Am. Med. Assoc. 2017, 317, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Fatmi, Z.; Sahito, A.; Ikegami, A.; Mizuno, A.; Cui, X.; Mise, N.; Takagi, M.; Kobayashi, Y.; Kayama, F. Lead exposure assessment among pregnant women. Newborns and children: Case study from Karachi, Pakistan. Int. J. Environ. Res. Public Health 2017, 14, 413. [Google Scholar] [CrossRef] [PubMed]
- McDaniels, J.; Chouinard, R.; Veiga, M.M. Appraising the global mercury project: An adaptive management approach to combating mercury pollution in small-scale gold mining. Int. J. Environ. Pollut. 2010, 41 (Suppl. 3–4), 242–258. [Google Scholar] [CrossRef]
- Risher, J. Toxicological Profile for Mercury; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 1999; p. 676. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Syversen, T.; Kaur, P. The toxicology of mercury and its compounds. J. Trace Elem. Med. Biol. 2012, 26, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Burbacher, T.M.; Shen, D.D.; Liberato, N.; Grant, K.S.; Cernichiari, E.; Clarkson, T. Comparison of blood and brain levels in infant monkeys exposed to methylmercury or vaccines containing thimerosal. Environ. Health Perspect. 2005, 113, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G.; Farina, M.; Rocha, J.B.T. Toxicity of ethylmercury (and Thimerosal): A comparison with methylmercury. J. Appl. Toxicol. 2013, 33, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Dock, L.; Rissanen, R.-L.; Vahter, M. Demethylation and placental transfer of methyl mercury in the pregnant hamster. Toxicology 1994, 94, 131–142. [Google Scholar] [CrossRef]
- Atsdr, U. Toxicological Profile for Arsenic; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2007; p. 559. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- World Health Organization. Trace Elements in Human Nutrition and Health; World Health Organization: Geneva, Switzerland, 1996; p. 360. [Google Scholar]
- Shakoor, M.B.; Nawaz, R.; Hussain, F.; Raza, M.; Ali, S.; Rizwan, M.; Oh, S.-E.; Ahmad, S. Human health implications, risk assessment and remediation of arsenic-contaminated water: A critical review. Sci. Total Environ. 2017, 601–602, 756–769. [Google Scholar] [CrossRef] [PubMed]
- Ciminelli, V.S.T.; Gasparon, M.; Ng, J.C.; Silva, G.C.; Caldeira, C.L. Dietary arsenic exposure in Brazil: The contribution of rice and beans. Chemosphere 2017, 168, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Yokel, R.A. Manganese flux across the blood-brain barrier. Neuromol. Med. 2009, 11, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.; Strazielle, N.; Richaud, P.; Bouron, A.; Ghersi-Egea, J.F. Active transport at the blood-CSF barrier contributes to manganese influx into the brain. J. Neurochem. 2011, 117, 747–756. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (Ed.) Concise International Chemical Assessment Document 63. In Manganese and Its Compounds: Environmental Aspects; World Health Organization: Geneva, Switzerland, 2004; p. 65. Available online: http://www.inchem.org/pages/cicads (accessed on 29 November 2017).
- Simms, J.A. Dark side of manganese. Chem. Eng. News 2011, 89, 4. [Google Scholar]
- Ritter, S.K. Study fuels toxicity debate. Chem. Eng. News 2014, 92, 40–41. [Google Scholar]
- Bouchard, M.F.; Sauve, S.; Barbeau, B.; Legrand, M.; Brodeur, M.-E.; Bouffard, T.; Limoges, E.; Bellinger, D.C.; Mergler, D. Intellectual impairment in school-age children exposed to manganese from drinking water. Environ. Health Perspect. 2011, 119, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Al Saggaf, S.M.; Abdel-Hamid, G.A.; Hagras, M.; Saleh, H.A. Does selenium ameliorate toxic effects of prenatal aluminum on brain of full term rat fetuses? J. Anim. Vet. Adv. 2012, 11, 3588–3592. [Google Scholar]
- Lakshmi, B.V.S.; Sudhakar, M.; Prakash, K.S. Protective effect of selenium against aluminum chloride-induced Alzheimer’s disease: Behavioral and biochemical alterations in rats. Biol. Trace Elem. Res. 2015, 165, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Gailer, J. Arsenic-selenium and mercury-selenium bonds in biology. Coord. Chem. Rev. 2007, 251, 234–254. [Google Scholar] [CrossRef]
- Wang, M.; Fu, H.; Xiao, Y.; Ai, B.; Wei, Q.; Wang, S.; Liu, T.; Ye, L.; Hu, Q. Effects of low-level organic selenium on lead-induced alterations in neural cell adhesion molecules. Brain Res. 2013, 1530, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Bao, Y.-X.; Fu, H.-H.; Li, L.-L.; Ren, T.-H.; Yu, X.-D. Selenium protects neonates against neurotoxicity from prenatal exposure to manganese. PLoS ONE 2014, 9, e86611. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.L.; Budtz-Jorgensen, E.; Jorgensen, P.J.; Steuerwald, U.; Debes, F.; Weihe, P.; Grandjean, P. Selenium as a protective factor against mercury developmental neurotoxicity. Environ. Res. 2008, 107, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, M.; Yasutake, A.; Kakita, A.; Ryufuku, M.; Chan, H.M.; Yamamoto, M.; Oumi, S.; Kobayashi, S.; Watanabe, C. Selenomethionine protects against neuronal degeneration by methylmercury in the developing rat cerebrum. Environ. Sci. Technol. 2013, 47, 2862–2868. [Google Scholar] [CrossRef] [PubMed]
- Schrauzer, G.N.; Surai, P.F. Selenium in human and animal nutrition: Resolved and unresolved issues. A partly historical treatise in commemoration of the 50th anniversary of the discovery of the biological essentiality of selenium, dedicated to the memory of Klaus Schwartz (1914–1978) on the occasion of the 30th anniversary of his death. Crit. Rev. Biotechnol. 2009, 29, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Risher, J. Toxicological Profile for Selenium; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2003; p. 457. Available online: http://www.atsdr.cdc.gov/ (accessed on 29 November 2017).
- Cesbron, A.; Saussereau, E.; Mahieu, L.; Couland, I.; Guerbet, M.; Goulle, J.-P. Metallic profile of whole blood and plasma in a series of 106 healthy volunteers. J. Anal. Toxicol. 2013, 37, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Curren, M.S.; Liang, C.L.; Davis, K.; Kandola, K.; Brewster, J.; Potyrala, M.; Chan, H.M. Assessing determinants of maternal blood concentrations for persistent organic pollutants and metals in the Eastern and Western Canadian Arctic. Sci. Total Environ. 2015, 527, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Tomljenovic, L.; Shaw, C.A. Aluminum vaccine adjuvants: Are they safe? Curr. Med. Chem. 2011, 18, 2630–2637. [Google Scholar] [CrossRef] [PubMed]
- Exley, C. What is the risk of aluminum as a neurotoxin? Expert Rev. Neurother. 2014, 14, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Akay, C.; Kalman, S.; Dundaroz, R.; Sayal, A.; Aydin, A.; Ozkan, Y.; Gul, H. Serum aluminum levels in glue-sniffer adolescent and in glue containers. Basic Clin. Pharmacol. Toxicol. 2008, 102, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Bank, M.S.; Spengler, J.D. Assessing metal exposures in a community near a cement plant in the northeast U.S. Int. J. Environ. Res. Public Health 2015, 12, 952–969. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.; Hyun, W.; Ro, Y.; Lee, H.; Song, K. A study on blood lipid profiles, aluminum and mercury levels in college students. Nutr. Res. Pract. 2016, 10, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Nisse, C.; Tagne-Fotso, R.; Howsam, M.; Richeval, C.; Labat, L.; Leroyer, A. Blood and urinary levels of metals and metalloids in the general adult population of Northern France: The IMEPOGE study, 2008–2010. Int. J. Hyg. Environ. Health 2017, 220, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Birgisdottir, B.E.; Knutsen, H.K.; Haugen, M.; Gjelstad, I.M.; Jenssen, M.T.S.; Ellingsen, D.G.; Thomassen, Y.; Alexander, J.; Meltzer, H.M.; Brantsaeter, A.L. Essential and toxic element concentrations in blood and urine and their association with diet: Results from a Norwegian population study including high-consumers of seafood and game. Sci. Total Environ. 2013, 463/464, 836–844. [Google Scholar] [CrossRef] [PubMed]
- George, C.M.; Gamble, M.; Slavkovich, V.; Levy, D.; Ahmed, A.; Ahsan, H.; Graziano, J. A cross-sectional study of the impact of blood selenium on blood and urinary arsenic concentrations in Bangladesh. Environ. Health 2013, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Freire, C.; Koifman, R.J.; Fujimoto, D.; de Oliveira Souza, V.C.; Barbosa, F.B., Jr.; Koifman, S. Reference values of cadmium, arsenic and manganese in blood and factors associated with exposure levels among adult population of Rio Branco, Acre, Brazil. Chemosphere 2015, 128, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Abass, K.; Koiranen, M.; Mazej, D.; Tratnik, J.S.; Horvat, M.; Hakkola, J.; Jarvelin, M.-R.; Rautio, A. Arsenic, cadmium, lead and mercury levels in blood of Finnish adults and their relation to diet, lifestyle habits and sociodemographic variations. Environ. Sci. Pollut. Res. 2017, 24, 1347–1362. [Google Scholar] [CrossRef] [PubMed]
- Kuno, R.; Roquetti, M.H.; Becker, K.; Seiwert, M.; Gouveia, N. Reference values for lead, cadmium and mercury in the blood of adults from the metropolitan area of Sao Paulo, Brazil. Int. J. Hyg. Environ. Health 2013, 216, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Obiri, S.; Yeboah, P.O.; Osae, S.; Adu-Kumi, S. Levels of arsenic, mercury, cadmium, copper, lead, zinc and manganese in serum and whole blood of resident adults from mining and non-mining communities in Ghana. Environ. Sci. Pollut. Res. 2016, 23, 16589–16597. [Google Scholar] [CrossRef] [PubMed]
- Santos-Burgoa, C.; Rios, C.; Mercado, L.A.; Arechiga-Serrano, R.; Cano-Valle, F.; Eden-Wynter, R.A.; Texcalac-Sangrador, J.L.; Villa-Barragan, J.P.; Rodriguez-Agudelo, Y.; Montes, S. Exposure to manganese: Health effects on the general population, a pilot study in Central Mexico. Environ. Res. A 2001, 85, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Bocca, B.; Madeddu, R.; Asara, Y.; Tolu, P.; Marchal, J.A.; Forte, G. Assessment of reference ranges for blood Cu, Mn, Se, and Zn in a selected Italian population. J. Trace Elem. Med. Biol. 2011, 25, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Oulhote, Y.; Mergler, D.; Bouchard, M.F. Sex and age differences in blood manganese levels in the U.S. general population: National health and nutrition examination survey, 2011–2012. Environ. Health 2014, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, W.; Gwynn, R.C.; Jeffery, N.; Kass, D.; Thorpe, L.E.; Garg, R.K.; Palmer, C.D.; Parsons, P.J. A biomonitoring study of lead, cadmium, and mercury in the blood of New York City Adults. Environ. Health Perspect. 2007, 115, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.B.; Choi, Y.S. Normal reference ranges for and variability in the levels of blood manganese and selenium by gender, age and race/ethnicity for general U.S. population. J. Trace Elem. Med. Biol. 2015, 30, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Angerer, J.; Ewers, U.; Heudorf, U.; Wilhelm, M. Revised and new reference values for environmental pollutants in urine or blood of children in Germany derived from the German Environmental Survey on Children, 2003–2006 (GerES IV). Int. J. Hyg. Environ. Health 2009, 212, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Interpretive Handbook—Mayo Medical Laboratories. 2015. Available online: https://www.mayomedicallaboratories.com/test-catalog/print-catalog.html?classification=interpretive (accessed on 29 November 2017).
- Environmental and Clinical Laboratory/Micro Trace Minerals Laboratory. Mineral Analysis: Whole Blood; Micro Trace Minerals: Boulder, CO, USA, 2012. [Google Scholar]
- Edwards, M. Fetal death and reduced birth rates associated with exposure to lead-contaminated drinking water. Environ. Sci. Technol. 2014, 48, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Prokopowicz, A.; Pawlas, N.; Ochota, P.; Szula, M.; Sobczak, A.; Pawlas, K. Blood levels of lead, cadmium and mercury in healthy women in their 50s in an urban area of Poland: A pilot study. Pol. J. Environ. Stud. 2014, 23, 167–175. [Google Scholar]
- Hightower, J.M.; Moore, D. Mercury levels in high-end consumers of fish. Environ. Health Perspect. 2003, 111, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Callan, A.C.; Hinwood, A.L.; Ramalingam, M.; Boyce, M.; Heyworth, J.; McCafferty, P.; Odland, J.O. Maternal exposure to metals: Concentrations and predictors of exposure. Environ. Res. 2013, 126, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, M.H.; Samms-Vaughan, M.; Dickerson, A.S.; Hessabi, M.; Bressler, J.; Desai, C.C.; Shakespeare-Pellington, S.; Reece, J.-A.; Morgan, R.; Loveland, K.A.; et al. Concentration of lead, mercury, cadmium, aluminum, arsenic and manganese in umbilical cord blood of Jamaican newborns. Int. J. Environ. Res. Public Health 2015, 12, 4481–4501. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.P.; Flood, K.; Chiang, S.; Herring, A.H.; Wolf, L.; Fry, R.C. Towards prenatal biomonitoring in North Carolina: Assessing arsenic, cadmium, mercury and lead levels in pregnant women. PLoS ONE 2012, 7, e31354. [Google Scholar] [CrossRef] [PubMed]
- Miklavcic, A.; Casetta, A.; Tratnik, J.S.; Mazej, D.; Krsnik, M.; Mariuz, M.; Sofianou, K.; Spiric, Z.; Barbone, F.; Horvat, M. Mercury, arsenic and selenium exposure levels in relation to fish consumption in the Mediterranean area. Environ. Res. 2013, 120, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Baeyens, W.; Vrijens, J.; Gao, Y.; Croes, K.; Schoeters, G.; Hond, E.D.; Sioen, I.; Bruckers, L.; Nawrot, T.; Nelen, V.; et al. Trace metals in blood and urine of newborn/mother pairs, adolescents and adults of the Flemish population (2007–2011). Int. J. Hyg. Environ. Health 2014, 217, 878–890. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Shinwari, N.; Mashhour, A.; Rabah, A. Birth outcome measures and maternal exposure to heavy metals (lead, cadmium and mercury) in Saudi Arabian population. Int. J. Hyg. Environ. Health 2014, 217, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Chen, W.; Wang, D.; Jin, Y.; Chen, X.; Xu, Y. The effects of prenatal exposure to low-level cadmium, lead and selenium on birth outcomes. Chemosphere 2014, 108, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, A.S.; Roy, A.; Amarasiriwardena, C.J.; Smith, D.; Lupoli, N.; Mercado-Garcia, A.; Lamadrid-Figueroa, H.; Tellez-Rojo, M.M.; Hu, H.; Hernandez-Avila, M. Maternal blood, plasma, and breast milk: Lactational transfer and contribution to infant exposure. Environ. Health Perspect. 2014, 122, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-M.; Chung, J.-Y.; An, H.S.; Park, S.Y.; Kim, B.-G.; Bae, J.W.; Han, M.; Cho, Y.J.; Hong, Y.-S. Biomonitoring of lead, cadmium, total mercury and methylmercury levels in maternal blood and in umbilical cord blood at birth in South Korea. Int. J. Environ. Res. Public Health 2015, 12, 13482–13493. [Google Scholar] [CrossRef] [PubMed]
- Gunier, R.B.; Mora, A.M.; Smith, D.; Arora, M.; Austin, C.; Eskenazi, B.; Bradman, A. Biomarkers of manganese exposure in pregnant women and children living in an agricultural community in California. Environ. Sci. Technol. 2014, 48, 14695–14702. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Ding, G.; Gao, Y.; Wang, P.; Shi, R.; Huang, H.; Tian, Y. Manganese concentrations in maternal-infant blood and birth weight. Environ. Sci. Pollut. Res. 2014, 21, 6170–6175. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, T.E.; Liang, C.L.; Morisset, A.-S.; Fisher, M.; Weiler, H.; Cirtiu, C.M.; Legrand, M.; Davis, K.; Ettinger, A.S.; Fraser, W.D. Maternal and fetal exposure to cadmium, lead, manganese and mercury: The MIREC study. Chemosphere 2016, 163, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Kozikowska, I.; Binkowski, L.J.; Szczepanska, K.; Slawska, H.; Miszczuk, K.; Sliwinska, M.; Laciak, T.; Stawarz, R. Mercury concentrations in human placenta, umbilical cord, cord blood and amniotic fluid and their relations with body parameters of newborns. Environ. Pollut. 2013, 182, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Basu, N.; Tutino, R.; Zhang, Z.; Cantonwine, D.E.; Goodrich, J.M.; Somers, E.C.; Rodriguez, L.; Schnaas, L.; Solano, M.; Mercado, A.; et al. Mercury levels in pregnant women, children and seafood from Mexico City. Environ. Res. 2014, 135, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Abduljabber, M.; Al-Rouqi, R.; Eltabache, C.; Al-Rajudi, T.; Elkhatib, R.; Nester, M. The extent of mercury (Hg) exposure among Saudi mothers and their respective infants. Environ. Monit. Assess. 2015, 187, 29. [Google Scholar] [CrossRef] [PubMed]
- Lemire, M.; Kwan, M.; Laouan-Sidi, A.E.; Muckle, G.; Pirkle, C.; Ayotte, P.; Dewailly, E. Local country food sources of methylmercury, selenium and omega-3 fatty acids in Nunavik, Northern Quebec. Sci. Total Environ. 2015, 509–510, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.M.; Golding, J.; Emond, A.M. Lead, cadmium and mercury levels in pregnancy: The need for international consensus on levels of concern. J. Dev. Origins Health Dis. 2014, 5, 16–30. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, C.; Frohlich, S.; Graf-Rohrmeister, K.; Eibenberger, B.; Jessenig, V.; Gicic, D.; Prinz, S.; Wittmann, K.J.; Zeisler, H.; Vallant, B.; et al. Perinatal lead and mercury exposure in Austria. Sci. Total Environ. 2010, 408, 5744–5749. [Google Scholar] [CrossRef] [PubMed]
- Aylward, L.L.; Hays, S.M.; Kirman, C.R.; Marchitti, S.A.; Kenneke, J.F.; English, C.; Mattison, D.R.; Becker, R.A. Relationships of chemical concentrations in maternal and cord blood: A review of available data. J. Toxicol. Environ. Health B 2014, 17, 175–203. [Google Scholar] [CrossRef] [PubMed]
- Yokel, R.A. Toxicity of gestational aluminum exposure to the maternal rabbit and offspring. Toxicol. Appl. Pharmacol. 1985, 79, 121–133. [Google Scholar] [CrossRef]
- Kruger, P.C.; Schell, L.M.; Stark, A.D.; Parsons, P.J. A study of the distribution of aluminum in human placental tissues based on alkaline solubilization with determination by electrothermal atomic absorption spectrometry. Metallomics 2010, 2, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.A.; Austin, D.W. Maternal transfer of mercury to the developing embryo/fetus: Is there a safe level? Toxicol. Environ. Chem. 2012, 94, 1610–1627. [Google Scholar] [CrossRef]
- Ollson, C.J.; Smith, E.; Herde, P.; Juhasz, A.L. Influence of co-contaminant exposure on the absorption of arsenic, cadmium and lead. Chemosphere 2017, 168, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Cobbina, S.J.; Chen, Y.; Zhou, Z.-X.; Wu, X.; Feng, W.; Wang, W.; Mao, G.; Xu, H.; Zhang, Z.; Wu, X.; et al. Low concentration toxic metal mixture interactions: Effects on essential and non-essential metals in brain, liver, and kidneys of mice on sub-chronic exposure. Chemosphere 2015, 132, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Andrade, V.; Mateus, M.L.; Batoreu, M.C.; Aschner, M.; dos Santos, A.P.M. Urinary delta-ALA: A potential biomarker of exposure and neurotoxic effect in rats co-treated with a mixture of lead, arsenic and manganese. Neurotoxicology 2013, 38, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Karri, V.; Schuhmacher, M.; Kumar, V. Heavy metals (Pb, Cd, As and MeHg) as risk factors for cognitive dysfunction: A general review of metal mixture mechanism in brain. Environ. Toxicol. Pharmacol. 2016, 48, 203–213. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, S.M.; Horgan, K.A.; Murphy, R.A. Chemical form of selenium differentially influences DNA repair pathways following exposure to lead nitrate. J. Trace Elem. Med. Biol. 2015, 29, 151–169. [Google Scholar] [CrossRef] [PubMed]
- Folven, K.I.; Glover, C.N.; Malde, M.K.; Lundebye, A.-K. Does selenium modify neurobehavioral impacts of developmental methylmercury exposure in mice? Environ. Toxicol. Pharmacol. 2009, 28, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Raymond, L.J.; Ralston, N.V.C. Selenium prevents and reverses methylmercury toxicity. Neurotoxicology 2006, 27, 1172–1173. [Google Scholar]
- Ralston, N.V.C.; Ralston, C.R.; Raymond, L.J. Selenium health benefit values: Updated criteria for mercury risk assessments. Biol. Trace Elem. Res. 2016, 171, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Cusack, L.K.; Eagles-Smith, C.; Harding, A.K.; Kile, M.; Stone, D. Selenium: Mercury molar ratios in freshwater fish in the Columbia River basin: Potential applications for specific fish consumption advisories. Biol. Trace Elem. Res. 2017, 178, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Meplan, C. Selenium and chronic diseases: A nutritional genomics. Nutrients 2015, 7, 3621–3651. [Google Scholar] [CrossRef] [PubMed]
- Dominiak, A.; Wilkaniec, A.; Wrocynski, P.; Adamczyk, A. Selenium in the therapy of neurological diseases. Where is it going? Curr. Neuropharmacol. 2016, 14, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Pieczynska, J.; Grajeta, H. The role of selenium in human conception and pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, B.R.; Bandeira, V.S.; Jacob-Filho, W.; Cozzolino, S.M.F. Selenium status in elderly: Relation to cognitive decline. J. Trace Elem. Med. Biol. 2014, 28, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Alexander, J.; Aaseth, J. Supplementation with selenium and co-enzyme Q10 reduces cardiovascular mortality in elderly with low selenium status. A secondary analysis of a randomized clinical trial. PLoS ONE 2016, 11, e0157541. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Johansson, P.; Aaseth, J.; Alexander, J.; Wagsater, D. Significant changes in circulating microRNA by dietary supplementation of selenium and co-enzyme Q10 in healthy elderly males. A subgroup analysis of a prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. PLoS ONE 2017, 12, e174880. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Roberts, B.R.; Bush, A.I.; Hare, D.J. Selenium, selenoproteins and neurodegenerative diseases. Metallomics 2015, 7, 1213–1228. [Google Scholar] [CrossRef] [PubMed]
- Solovyev, N.D. Importance of selenium and selenoprotein for brain function: From antioxidant protection to neuronal signaling. J. Inorg. Biochem. 2015, 153, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Du, X.-B.; Wang, C.; Liu, Q. Potential roles of selenium and selenoproteins in the prevention of Alzheimer’s disease. Curr. Top. Med. Chem. 2016, 16, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, B.R.; Hare, D.J.; Lind, M.; McLean, C.A.; Volitakis, I.; Laws, S.M.; Masters, C.L.; Bush, A.I.; Roberts, B.R. The APOE epsilon 4 allene is associated with lower selenium levels in the brain: Implications for Alzheimer’s disease. Am. Chem. Soc. Chem. Neurosci. 2017, 8, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Naziroglu, M.; Muhamad, S.; Pecze, L. Nanoparticles as potential clinical therapeutic agents in Alzheimer’s disease: Focus on selenium nanoparticles. Exp. Rev. Clin. Pharmacol. 2017, 10, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Bjorklund, G.; Aaseth, J.; Ajsuvakova, O.P.; Nikonorov, A.A.; Skainy, A.V.; Skainaya, M.G.; Tinkov, A.A. Molecular interaction between mercury and selenium in neurotoxicity. Coord. Chem. Rev. 2017, 332, 30–37. [Google Scholar] [CrossRef]
- Schofield, K. Autism, chemicals, probable cause and mitigation: A new examination. Autism Open Access 2016, 6, 27. [Google Scholar] [CrossRef]
- Thakur, J.S.; Prinja, S.; Singh, D.; Rajwanshi, A.; Prasad, R.; Parwana, H.K.; Kumar, R. Adverse reproductive and child health outcomes among people living near highly toxic waste water drains in Punjab, India. J. Epidemiol. Community Health 2010, 64, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.; Kim, M.H.; Lim, S. Increased risk of spontaneous abortion and menstrual aberrations in female workers in semiconductor industry, South Korea. Occup. Environ. Med. 2014, 71 (Suppl. 1), A15. [Google Scholar] [CrossRef]
- Passini, R.P., Jr.; Cecatti, J.G.; Lajos, G.J.; Tedesco, R.P.; Nomura, M.L.; Dias, T.Z.; Haddad, S.M.; Rehder, P.M.; Pacagnella, R.C.; Costa, M.L.; et al. Brazilian multicenter study on preterm birth: Prevalence and factors associated with spontaneous preterm birth. PLoS ONE 2014, 9, e109069. [Google Scholar] [CrossRef] [PubMed]
- Amadi, C.N.; Igweze, Z.N.; Orisakwe, O.E. Heavy metals in miscarriages and stillbirths in developing nations. Middle East Fertil. Soc. J. 2017, 22, 91–100. [Google Scholar] [CrossRef]
- Klemm, L.; Scialli, A.R. The transport of chemicals in semen. Birth Defects Res. B Dev. Reprod. Toxicol. 2005, 74, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.; Banerjee, R.; Nath, S.; Das, S.; Banerjee, S. Metals and female reproductive toxicity. Hum. Exp. Toxicol. 2015, 34, 679–697. [Google Scholar] [CrossRef] [PubMed]
- Nenkova, G.; Petrov, L.; Alexandrova, A. Role of trace elements for oxidative status and quality of human sperm. Balk. Med. J. 2017, 34, 343–348. [Google Scholar] [CrossRef] [PubMed]
- DeLong, G. A positive association found between autism prevalence and childhood vaccination uptake across the US population. J. Toxicol. Environ. Health A 2011, 74, 903–916. [Google Scholar] [CrossRef] [PubMed]
- Goldman, G.S. Comparison of the vaccine adverse event reporting system (VAERS) fetal-loss reports during three consecutive influenza seasons: Was there a synergistic fetal toxicity associated with the two-vaccine 2009/2010 season? Hum. Exp. Toxicol. 2013, 32, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Bjermo, H.; Sand, S.; Nalsen, C.; Lundh, T.; Barbieri, H.E.; Pearson, M.; Lindroos, A.K.; Jonsson, B.A.G.; Barregard, L.; Darnerud, P.O. Lead, mercury and cadmium in blood and their relation to diet among Swedish adults. Food Chem. Toxicol. 2013, 57, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Laks, D.R. Mercury rising: Response to the EPA assessment of mercury exposure. Biometals 2014, 27, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Gaskin, J.; Rennie, C.; Coyle, D. Reducing periconceptual methylmercury exposure: Cost-utility for a proposed screening program for women planning a pregnancy in Ontario, Canada. Environ. Health Perspect. 2015, 123, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; O’Leary, K.; Rainis, H.; Gibb, H.J. Country specific estimates of the incidence of intellectual disability associated with prenatal exposure to methylmercury. Environ. Res. 2016, 147, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Starling, P.; Charlton, K.; McMahon, A.T.; Lucas, C. Fish intake during pregnancy and foetal neurodevelopment: A systematic review of the evidence. Nutrients 2015, 7, 2001–2014. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.M.; Golding, J.; Emond, A.M. Blood mercury levels and fish consumption in pregnancy: Risks and benefits for birth outcomes in a prospective observational birth cohort. Int. J. Hyg. Environ. Health 2016, 219, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.C.; de Paiva, E.L.; Milani, R.F.; Bearzoti, E.; Morgano, M.A.; Quintaes, K.D. Risk estimation to human health caused by the mercury content of Sushi and Sashimi sold in Japanese restaurants in Brazil. J. Environ. Sci. Health B 2017, 52, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Rose, M.; Baxter, M.; Brereton, N.; Baskaran, C. Dietary exposure to metals and other elements in the 2006 UK total diet study and some trends over the last 30 years. Food Addit. Contam. 2010, 27, 1380–1404. [Google Scholar] [CrossRef] [PubMed]
- Rescue, G. Autism and Vaccines around the World: Vaccine Schedules, Autism Rates and under 5 Mortality; Special Report; Generation Rescue, Inc.: Los Angeles, CA, USA, 2009; p. 4. [Google Scholar]
- Branco, V.; Caito, S.; Farina, M.; da Rocha, J.T.; Aschner, M.; Carvalho, C. Biomarkers of mercury toxicity: Past, present and future trends. J. Toxicol. Environ. Health B Crit. Rev. 2017, 20, 119–154. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| MRL | Average (Maximum Value), Country | |||||
|---|---|---|---|---|---|---|
| Al * | <6 | 37 [100] Turkey | 4.6 (≤17) [101] USA | 7.1 [102] Korea | 4.3 (≤11.8) [103] France | |
| As | <12 | 1.9 (≤7.1) [96] France | 5.9 (≤41) [104] Norway | 7.0 (≤56) [105] Bangladesh | 4.1 (≤31) [106] Brazil | 0.8 (≤18) [107] Finland |
| Pb | 50–70 | 2.7 (≤131) [108] Brazil | 25 (≤65) [104] Norway | 2.4 (≤245) [109] Ghana | 23 (≤54) [103] France | 17 (≤146) [107] Finland |
| Mn | <18 | 18 (≤88) [110] Mexico | 8.9 (<17) [111] Italy | 9.9 (≤62) [112] USA | 13 (≤119) [106] Brazil | 1.5 (≤42) [109] Ghana |
| Hg | <5.8 | 2.7 (≤36) [113] USA | 1.7 (≤5.1) [96] France | 4.0 (≤13) [104] Norway | 1.4 (≤12) [108] Brazil | 2.5 (≤15) [107] Finland |
| Se | 70–130 | 110 (≤142) [96] France | 95 (≤153) [104] Norway | 123 (≤222) [105] Bangladesh | 190 (≤253) [114] USA | 104 (≤245) [107] Finland |
| MRL | Average (Maximum Value), Country | |||||
|---|---|---|---|---|---|---|
| Al * | <6 | 65 (≤860) [121] Australia | 11 (≤28) [122] Jamaica | |||
| As | <12 | 0.4 (≤8.6) [123] USA | 1.9 (≤16) [121] Australia | 2.1 (≤37) [124] Croatia | 1.2 (≤33) [124] Italy | 0.6 (≤5.8) [125] Belgium |
| Pb | <50 | 8.9 (≤77) [123] USA | 29 (≤260) [126] Saudi Arabia | 45 (≤137) [127] China | 77 (≤287) [128] Mexico | 10 (≤22) [129] South Korea |
| Mn | <18 | 9.1 (≤50) [121] Australia | 15 (≤33) [130] USA | 12 (≤40) [125] Belgium | 66 (≤304) [131] China | 13 (≤34) [132] Canada |
| Hg | <3.5 | 8.0 (≤16) [133] Poland | 2.4 (≤40) [124] Italy | 3.7 (≤31) [134] Mexico | 0.9 (≤49) [135] Saudi Arabia | 11 (≤241) [136] North Canada |
| Se | 70–130 | 102 (≤374) [121] Australia | 117 (≤229) [124] Italy | 90 (≤182) [124] Croatia | 157 (≤456) [127] China | 271 (≤357) [136] North Canada |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schofield, K. The Metal Neurotoxins: An Important Role in Current Human Neural Epidemics? Int. J. Environ. Res. Public Health 2017, 14, 1511. https://doi.org/10.3390/ijerph14121511
Schofield K. The Metal Neurotoxins: An Important Role in Current Human Neural Epidemics? International Journal of Environmental Research and Public Health. 2017; 14(12):1511. https://doi.org/10.3390/ijerph14121511
Chicago/Turabian StyleSchofield, Keith. 2017. "The Metal Neurotoxins: An Important Role in Current Human Neural Epidemics?" International Journal of Environmental Research and Public Health 14, no. 12: 1511. https://doi.org/10.3390/ijerph14121511
APA StyleSchofield, K. (2017). The Metal Neurotoxins: An Important Role in Current Human Neural Epidemics? International Journal of Environmental Research and Public Health, 14(12), 1511. https://doi.org/10.3390/ijerph14121511