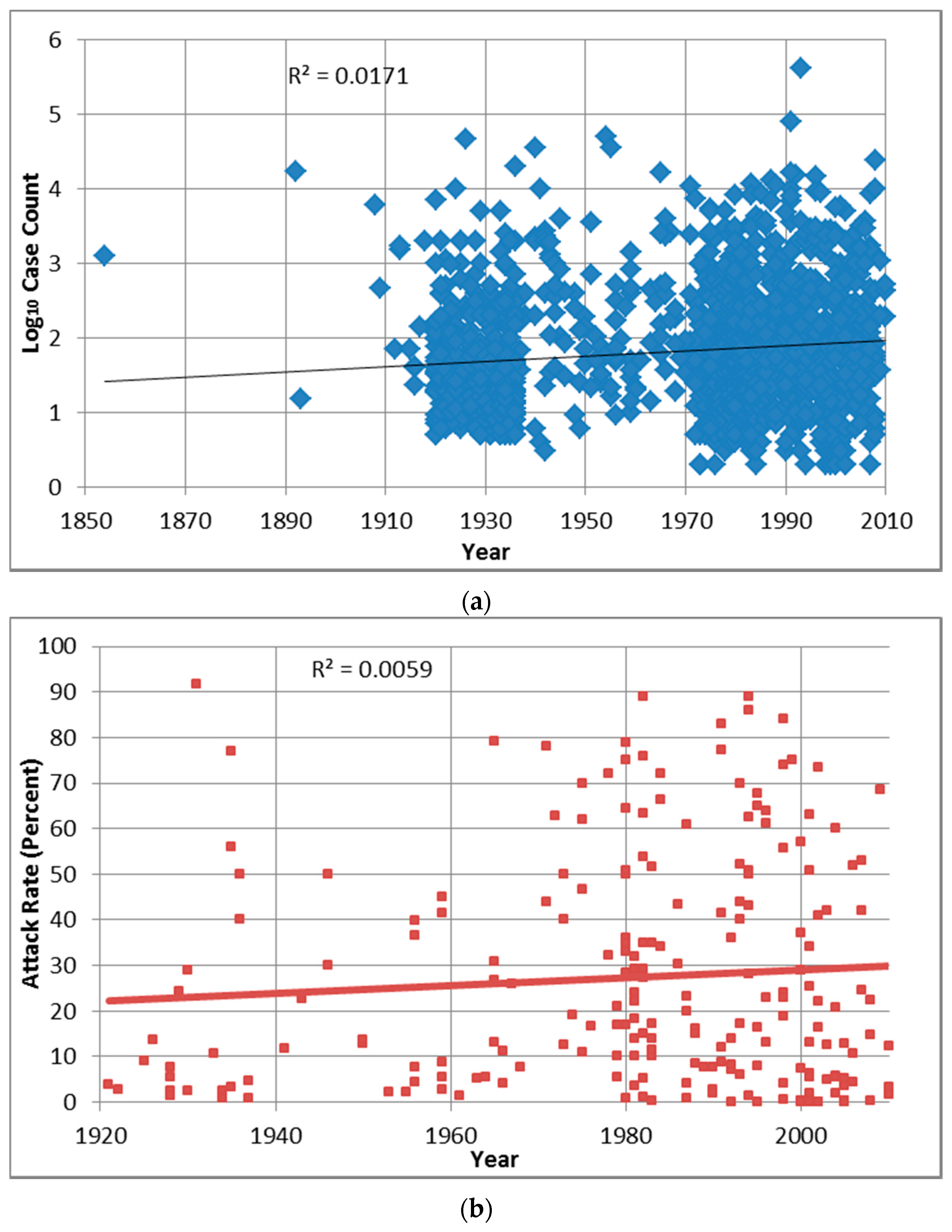
While the overall attack rate distribution does not contain mild or extreme outliers, that is not the case for the overall case count distribution, for which the removal of 228 mild or 198 extreme outliers greatly decreases the distribution’s mean, median and interquartile range lower and upper values (from 890, 49, 18 and 187 to 73–90, 35–37, 15–16 and 91–105.75, respectively). Using the adjusted distributions would decrease the influence of potentially improperly estimated case counts for many outbreaks (e.g., as described for the Milwaukee outbreak’s 403,000 cases of cryptosporidiosis in
Section 2.3). However, given the lack of consensus in judging the validity of high case count estimates (and subsequent removal of related outbreaks from statistical analysis) and of relatively low case count upper thresholds (e.g., the 440.5 and 694 values for the overall case count distribution) in the scientific literature, the outliers were retained throughout the rest of the analysis.
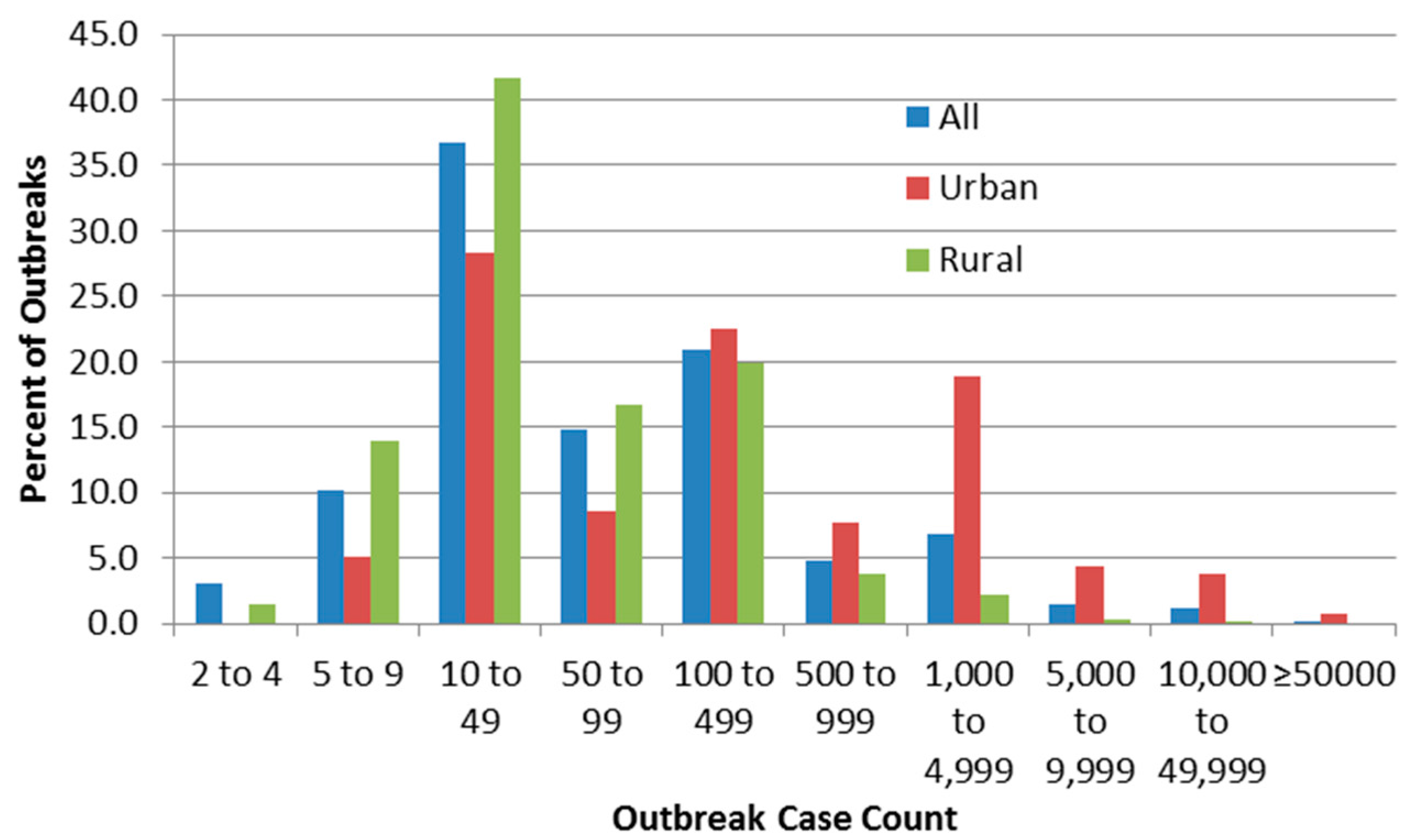
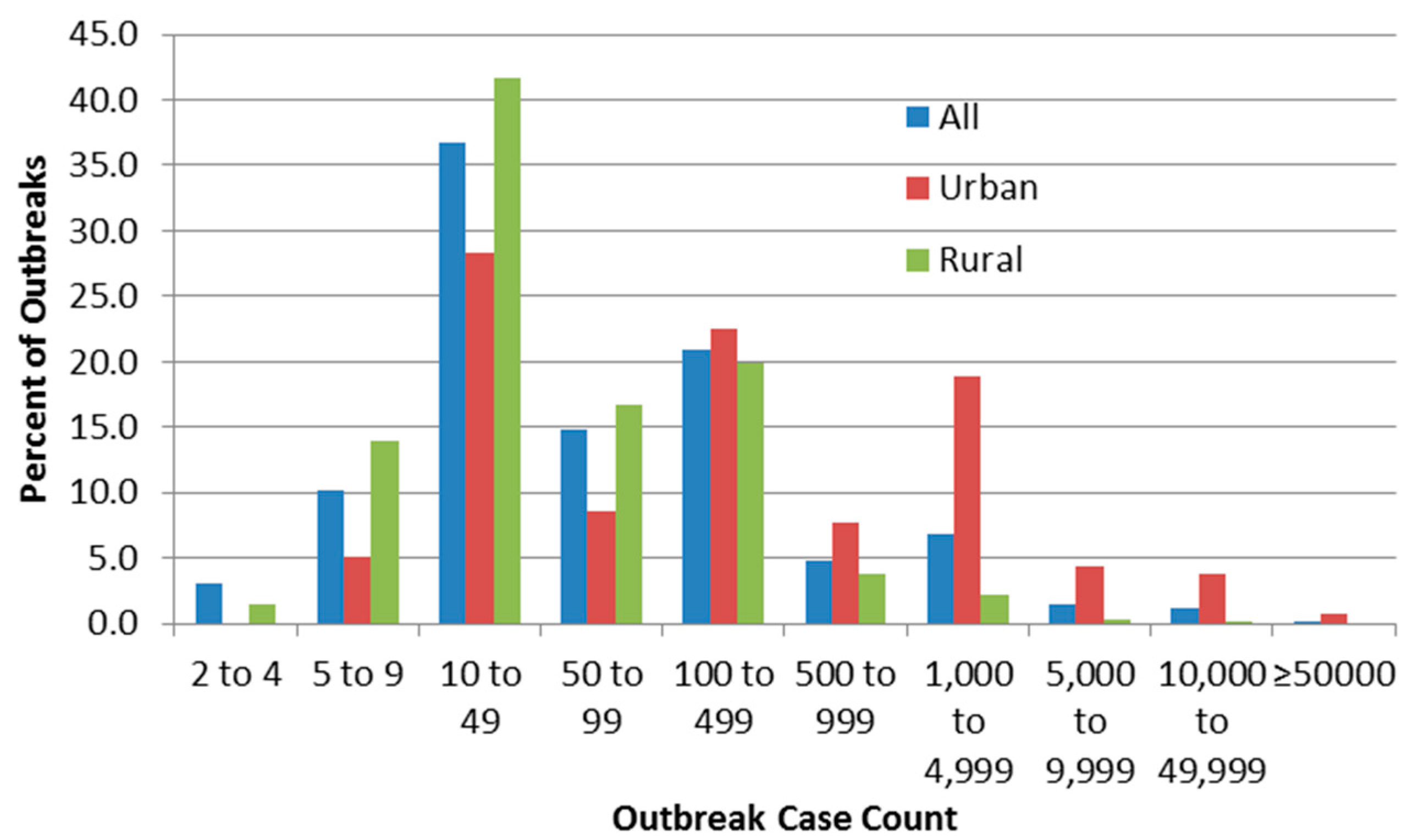
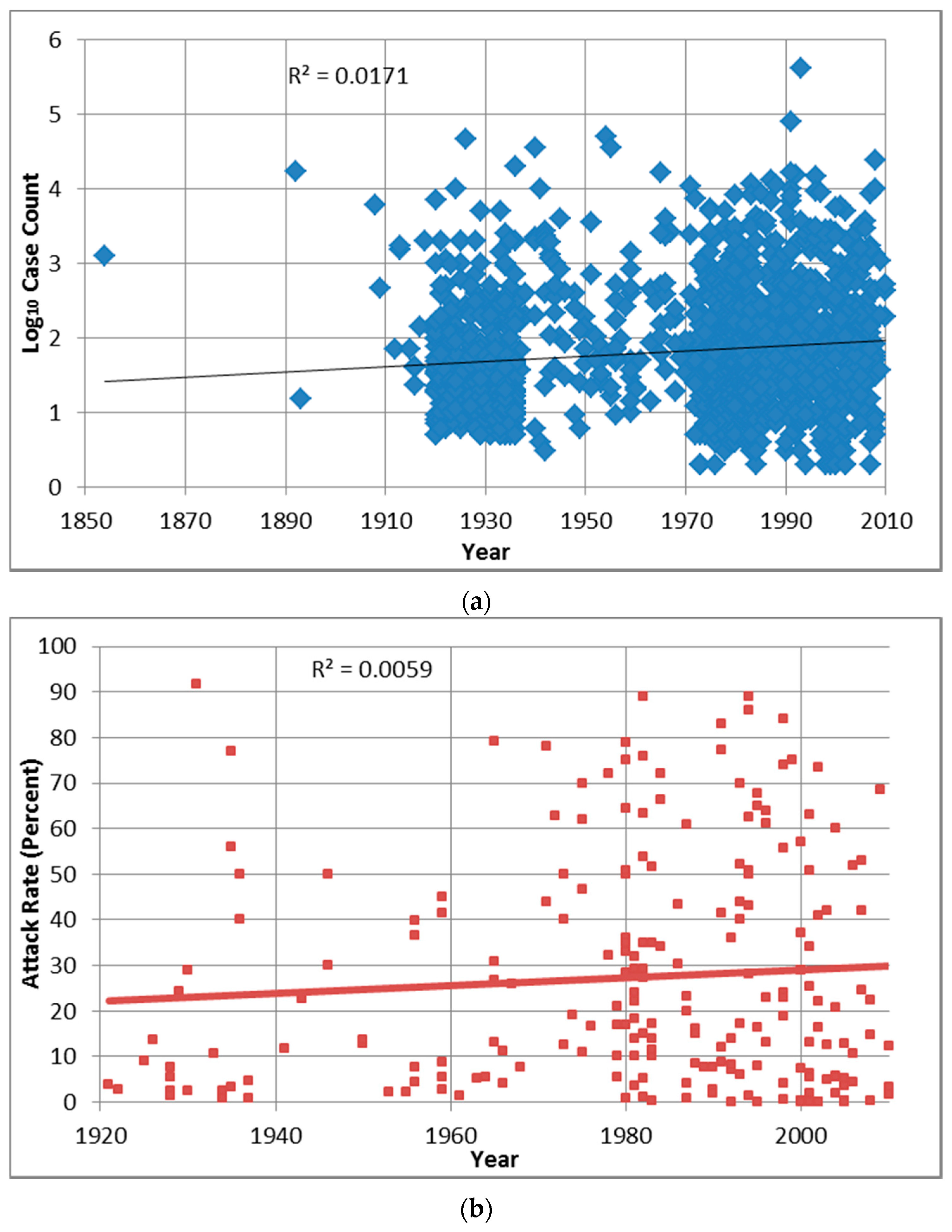
Figure 2 suggests high frequency of reporting at case counts of 10–49 and 100–499, which could be due to authors (including those of the line-listing reviews) rounding numbers of cases to 10 or 100. The figure also confirms the logical inference that rural outbreaks are associated with low case counts compared to urban ones. The very low numbers of detected outbreaks with low case counts (below 10 cases) implies that outbreak surveillance may be ineffective in detecting smaller outbreaks which in fact may be more frequent than larger ones, or that reporting systems often round up those case counts to 10. In order to compare this threshold with one described elsewhere (by Craun, who stated thatmost outbreaks are identified only if at least one percent of the community population falls ill [
24]), it would be necessary to obtain data on outbreak community population that were not present in most outbreak sources.
4.2.1. Temporal Associations
It is likely that the attribution of 92.5% of identified outbreaks to the 1920s, 1930s, 1970s, 1980s, 1990s and 2000+ decades (with those decade groups each containing between 11.7% and 21.3% of all identified outbreaks) derives from the extensive line-listing reporting in Gorman and Wolman [
22] and the 24 U.S. CDCSs rather than any changes in outbreak occurrence. Decadal outbreak frequency statistics contrast with decadal (total) outbreak case count (
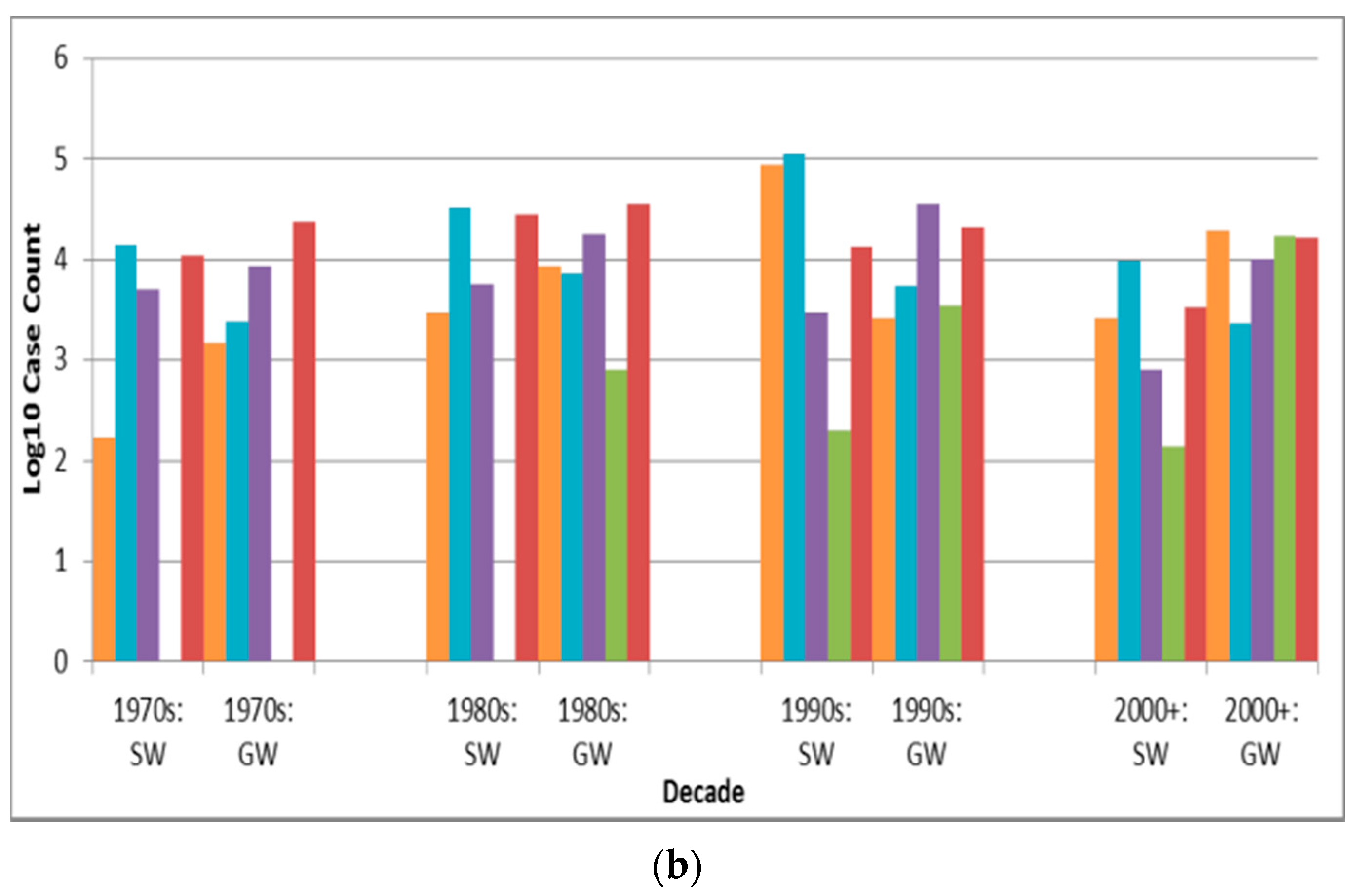
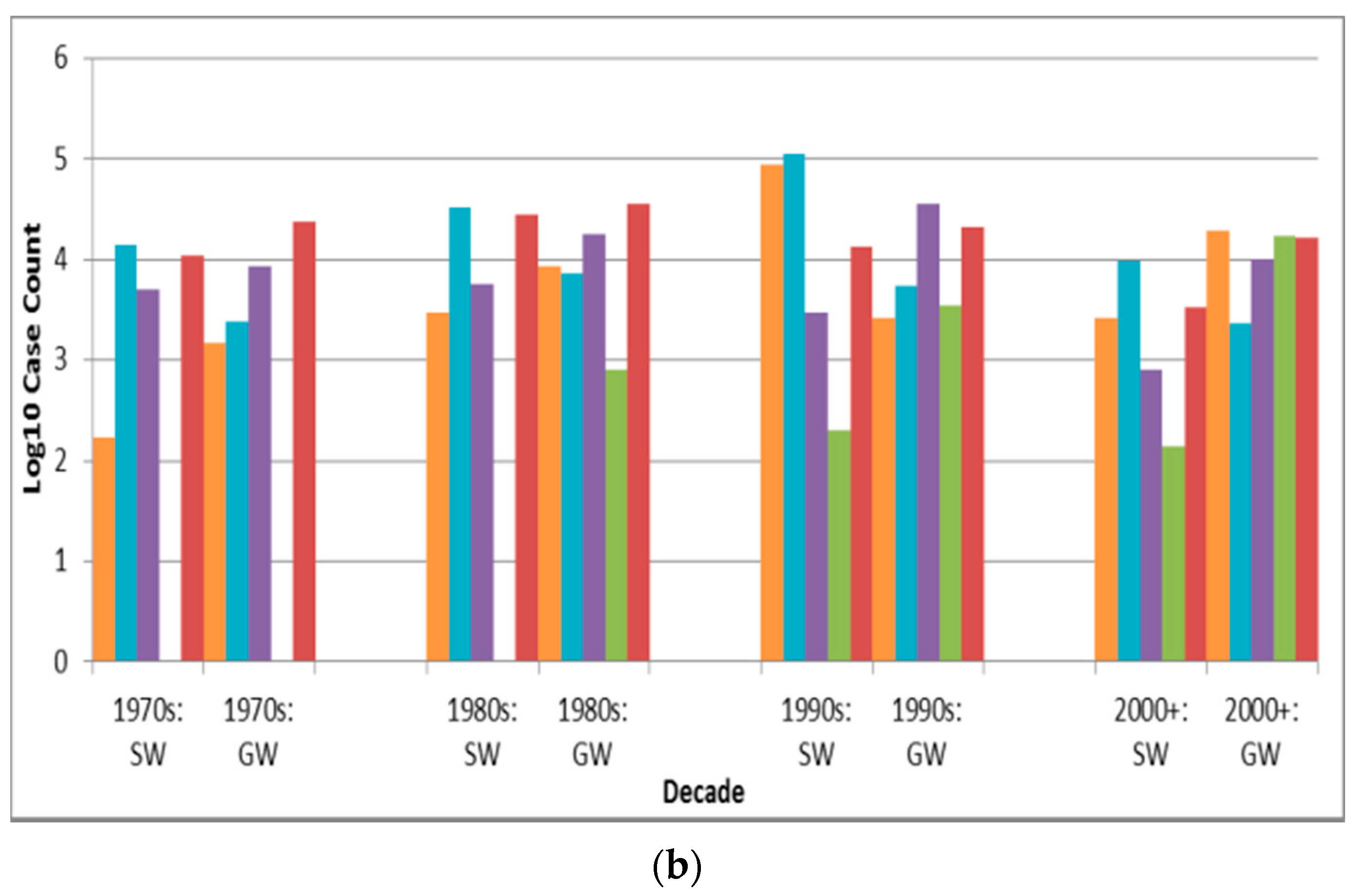
Table 2). Every decade except the 1990s contains at most 8.4% of identified cases, with the majority of the 1990s total case count of 641,243 cases (47.5% of the total) driven by the 403,000 cases in the 1993 Milwaukee Cryptosporidium (outlier) outbreak. Given how outliers can skew the total case count statistics—confirmed in the 1990s surface water protozoan, disinfection-and-filtration, and multiple deficiency realm bars (
Figure 3b,
Figure 4b and
Figure 5b), respectively—total case count (the product of outbreak mean case count and frequency) is often less conducive to insightful analysis of outbreak attribute differences than is outbreak frequency, and is therefore not included in
Table 5,
Table 6,
Table 7,
Table 8 and
Table 9.
4.2.2. Geographic Associations
While the preponderance of U.S. outbreaks is evident (70.4% of all identified outbreaks), population-weighted outbreak frequency data (
Table 3) suggest that Canada, the U.K., Sweden and Finland have similarly effective DWDO reporting systems. This is further supported by Finland and Sweden recording the highest and third-highest population-weighted total case counts among the nine countries assessed, respectively. However, although Sweden revamped its system in 1980, resulting in increased DWDO detection [
25], that source’s figure of 71 outbreaks recorded in Sweden from 1986 to 1996 contrasts with the figure of 53 reported by that country (combining their number of DWDOs and recreational water outbreaks) to the WHO for the same period [
9]. This inconsistency, potentially because Sweden’s “reporting and investigation system can be quite complex with a large number of different bodies being involved” [
25] (p. 116) and thus might be conducive to conflicting reporting by differing agencies, which signals the need for enhanced reporting that likely applies to many other countries with non- or under-standardized systems.
The finding that India outbreak case counts are significantly higher than those of U.S., U.K. and Canada outbreaks (p < 0.0001 for all three comparisons), while India outbreak attack rates are lower than the attack rates of those three countries’ outbreaks (significance not tested due to n < 30 for India), is consistent with the nature of the significant differences between developing and developed country outbreak case counts (p < 0.0001) and attack rates (p = 0.0006). This could reflect how outbreak surveillance and reporting systems are likely stronger in the usually higher-resource developed country settings and are thus more able to detect and publish findings of (smaller) outbreaks outside major cities. The much more urban nature of the developing country outbreaks (57 out of 88, or 66%) compared to developed country ones (360 out of 1431, or 25%) implies that the former are likelier to have greater supplied populations potentially affected by the outbreaks, driving down attack rates.
Given that 42% of the world’s population (disproportionately located in developing countries) lacks piped-on-premises water and relies on supply types like public taps, unprotected dug wells and manually-collected surface water [
26] that are less-represented in peer-reviewed DWDO literature, it is not surprising that only 5.8% of identified outbreaks are attributed to such countries. This underreporting is also likely to be associated with developing countries’ aforementioned likely weaker NWDOS systems (relative to those in developed countries), reasoning parallel to that in a review of waterborne disease on ships which concluded that “the number of reported outbreaks...is likely to be a small fraction of the total” (p. 437) due to lack of scientific literature publication and reporting to relevant authorities [
27]. Combined with the likelihood of low probability of detection of low case count outbreaks, these factors imply that, for much of the world, collated drinking water disease data greatly underestimate the actual incidence of outbreak and endemic waterborne disease, even in actively-reporting countries [
9].
Among U.S. states, Colorado and Oregon have the highest population-weighted outbreak frequency and total case count, respectively. This illustrates how outbreak data are related to both DWDO reporting system effectiveness—an association seen in Colorado, which received federal funding for reporting during 1980–1983 and saw an increase in outbreaks reported per year from 2.0 for the period 1971–1979 to 4.5 per year over those four years [
28]—and underlying outbreak occurrence (greatly influenced by outlier events like the 1954–1955 Oregon outbreak with 50,000 estimated cases of giardiasis and the 1993 Milwaukee outbreak with 403,000 estimated cases of cryptosporidiosis). This strength in DWDO reporting for Colorado is also reflected in the low case counts for their outbreaks (likely arising from superior detection of small outbreaks) relative to those of outbreaks for other top-recording states (albeit with almost significantly greater case counts based on Bonferroni-adjusted
p of 0.0014). The significantly lower case counts for Florida outbreaks relative to those of other states (e.g., for Colorado, Pennsylvania and Indiana,
p = 0.0001, < 0.0001 and 0.0005, respectively) also imply the strength in DWDO reporting for Florida. This is further suggested by the case of the Florida Department of Health which has developed a Food and Waterborne Disease Program task force to assist county health departments and since 1997 has published annual outbreak reports linked to an online database [
29].
The case counts of urban outbreaks are significantly (p < 0.0001) higher than the case counts of rural outbreaks. This is logical in that urban water systems typically serve greater populations and thus have greater potential for high case counts. However, while urban outbreak case counts are significantly higher than rural outbreak case counts, the opposite is true for their outbreak attack rates (with the difference significant, p < 0.0001).
4.2.3. Associated Pathogens
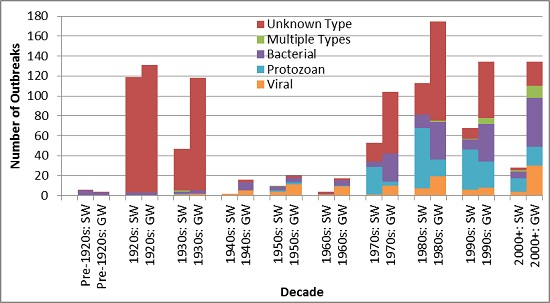
Source authors attributed dozens of outbreaks to pathogens not normally associated with DWDOs, e.g., Clostridium perfringens and other indicator-type pathogens. With the aim of following the original text as closely as possible, such pathogen attributions were retained. Similarly, reported causative pathogen attributions were also retained for outbreaks lacking microbiological detection of pathogens in water or affected cases. Such outbreaks might also have been erroneously noted as single-pathogen rather than multiple-pathogen, especially in the case of sewage contamination-associated outbreaks, in which the fecal loadings likely contained a variety of fecal-oral pathogens. These types of pathogen attributions have less validity than those in sources in which the authors conservatively declared the pathogen as suspected or unknown types.
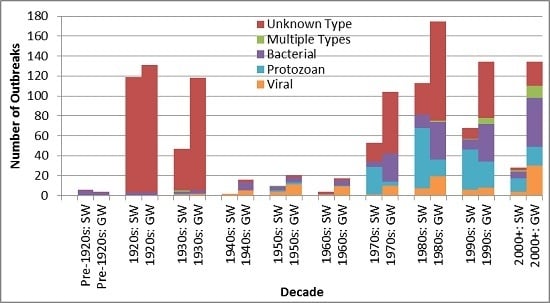
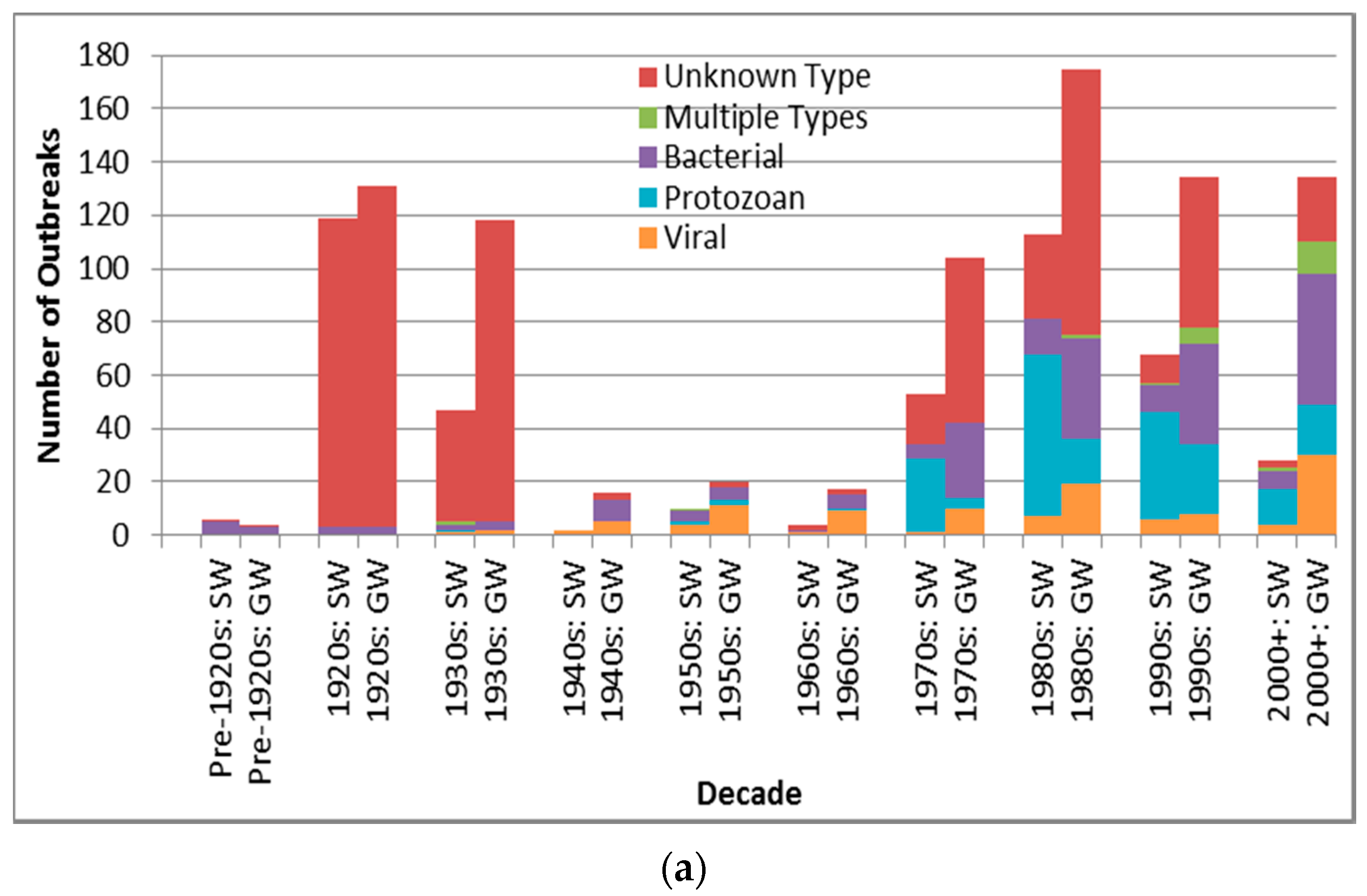
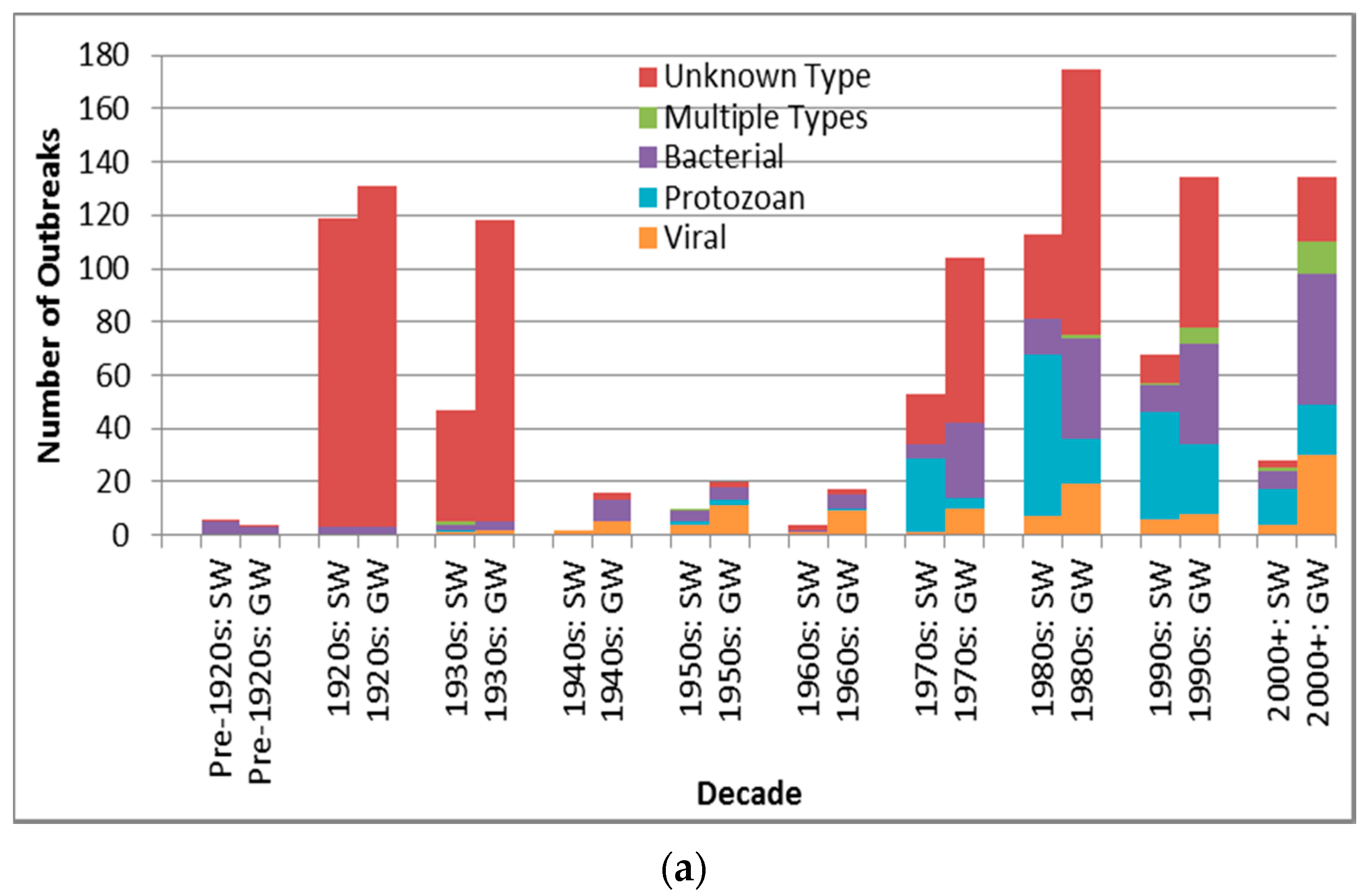
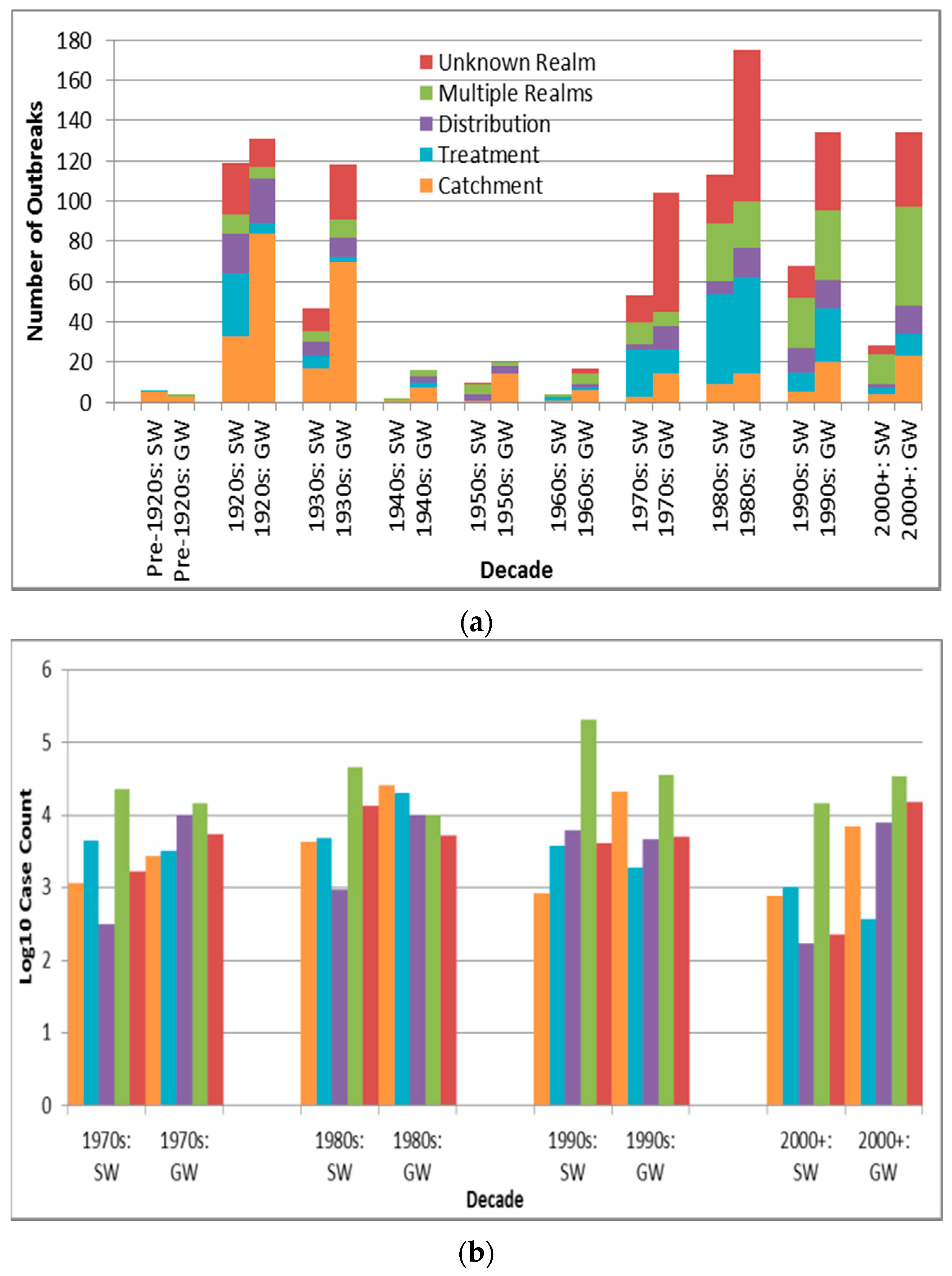
Figure 3a suggests a marked decline in unknown type etiology attribution (for the countries implicated in identified outbreaks) since the 1920s–1930s continuing through the 1980s to the 2000s, likely due to increasing ability to diagnose pathogens, for example, with the development of methods for Norovirus starting in the 1970s [
30] and advent of Polymerase Chain Reaction testing. The relatively high overall unknown etiology proportion (53.3% of all identified outbreaks) corresponds well with the 54.9% proportion found in another recent multi-country DWDO review (of U.S. and Canada small system DWDOs from 1970 to 2014) [
12], and contrasts the proportion found in a third multi-country review of DWDOs [
11] in four Nordic countries (from 1998 to 2012). The relatively low unknown etiology proportion (29.7%) of the latter review is logical in that its authors attributed this to “improvements over time in methods and routines for microbiological analysis” (p. 8) that would better facilitate pathogen attribution during the review’s relatively recent time period of analysis. The potential strength and depth in reporting of NWDOS for those Nordic countries (relative to the voluntary, line-listing reporting-based US system) could also facilitate greater outbreak pathogen diagnosis and documentation, further supporting that low unknown etiology proportion.
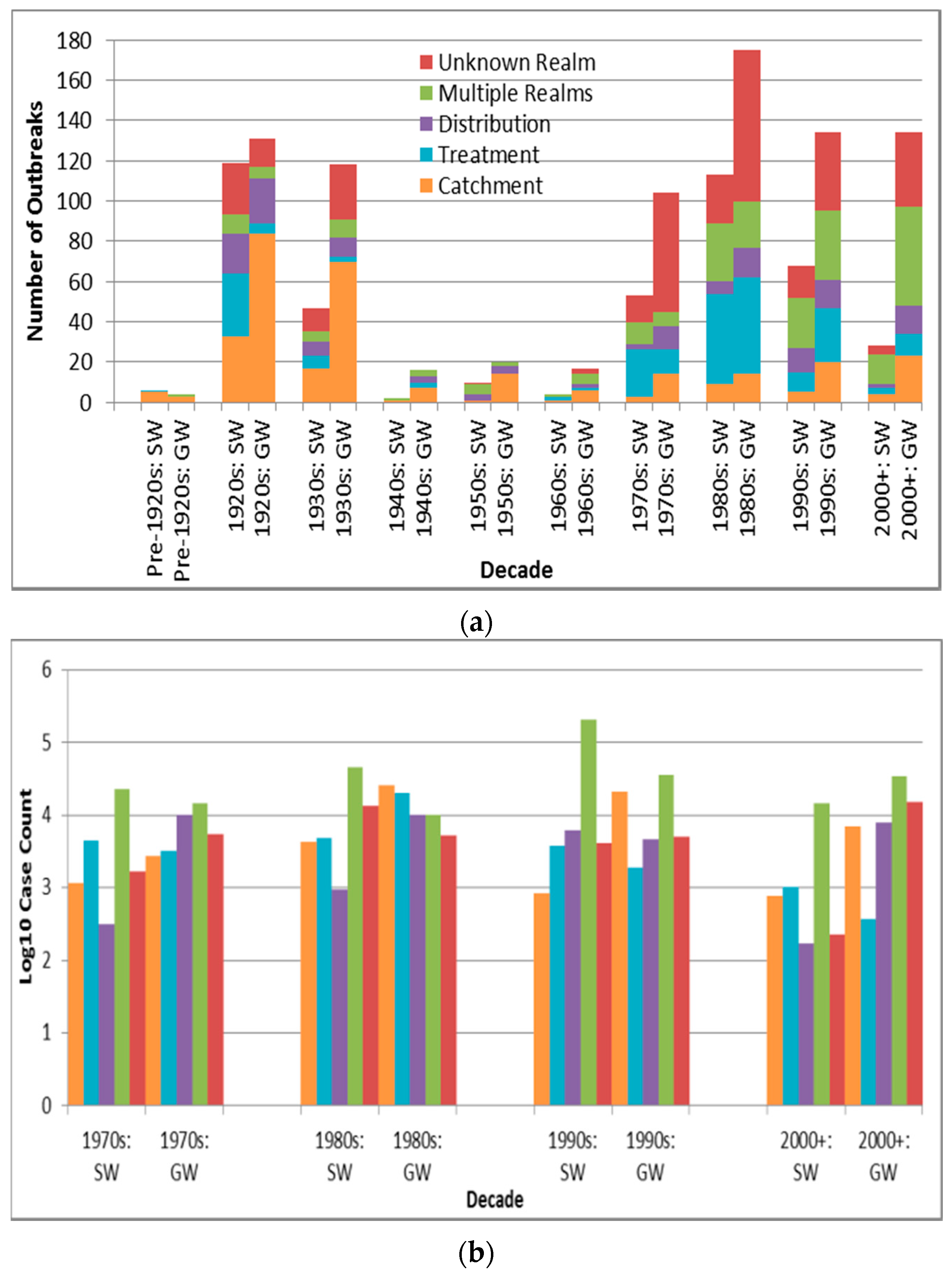
Figure 3a also suggests a decreasing frequency of surface water protozoan-associated outbreaks, which corroborates the nearly statistically-significant (
p = 0.0560) decrease in the annual proportion of U.S. surface water protozoan-associated outbreaks after 1989 as described in a 2010 review of 1971–2006 CDCS data [
31]. This may largely derive from the increased oversight of surface water especially following recognition of waterborne transmission of
Giardia and
Cryptosporidium as exemplified by the passage of the 1989 U.S. Surface Water Treatment Rule (SWTR). The emphasis in the rule on those two protozoans, which are used for developing SWTR-specified treatment and monitoring programs, may also have contributed to the decreasing log
10 decadal case count for surface water protozoan-associated outbreaks starting in the 1990s (
Figure 3b). Decreasing log
10 decadal case count for surface water outbreaks associated with each of the other four pathogen types from the 1990s might also derive from the implementation of the European Union (EU) Council Directive 75/440/EEC of 16 June 1975 Concerning the Quality Required of Surface Water Intended for the Abstraction of Drinking Water in Member States [
32].
In contrast with the decrease in surface water viral outbreak frequency and log
10 decadal case count starting in the 1990s, groundwater viral outbreak frequency and log
10 decadal case count increased from the 1970s-onward. This could be due to slow progress in improving groundwater management policies (e.g., the delay in passage of the U.S. Groundwater Rule until 2007 [
33]).
4.2.4. Associated Water Sources
The finding that groundwater outbreaks are 1.9 times as frequent as surface water ones is comparable with proportions reported in two similar reviews of 3.2 [
11] and 4.5 [
12]. The latter may be elevated by the Pons
et al. study’s focus on small systems (more likely to be rural than large systems given their association with populations of less than 5000 people in that study) if, as seems credible, a higher proportion of small systems are groundwater-fed. This is supported by comparing the rural-only outbreaks and urban-only outbreaks in the present review; the rural-associated proportion of groundwater to surface water outbreaks of 2.5 (390/159) is greater than the urban-associated proportion of 1.1 (184/162).
The higher prevalence of groundwater outbreaks relative to surface water ones, and of well outbreaks relative to those of the second-highest recording source subtype (rivers), might arise from groundwater sources being more vulnerable to contamination (because they often have fewer treatment steps) than surface water sources in the countries represented by identified outbreaks. However, this reasoning is called into question when considering how surface water sources can be more directly contaminated by human and animal fecal and other waste, and is confounded by the unknown number of groundwater sources studied in this review’s outbreaks that were under the direct influence of surface water. Surface water outbreaks having significantly higher case counts than groundwater outbreaks (p = 0.0021) could derive from how the former source type typically serves larger populations.
4.2.5. Associated Water Treatment
The attribution of 46.3% of outbreaks to untreated systems lies in between the proportions reported in two similar reviews (23.9% [
12] and 69.7% [
11]). This may be because both of those reviews had narrower scope and included grey literature and thus are likely to have captured different outbreaks; the former studied Canada Communicable Disease Reports, ProMED-mail and Google grey literature, while the latter reviewed only the limited-access, likely non-English NWDOS system data for four countries.
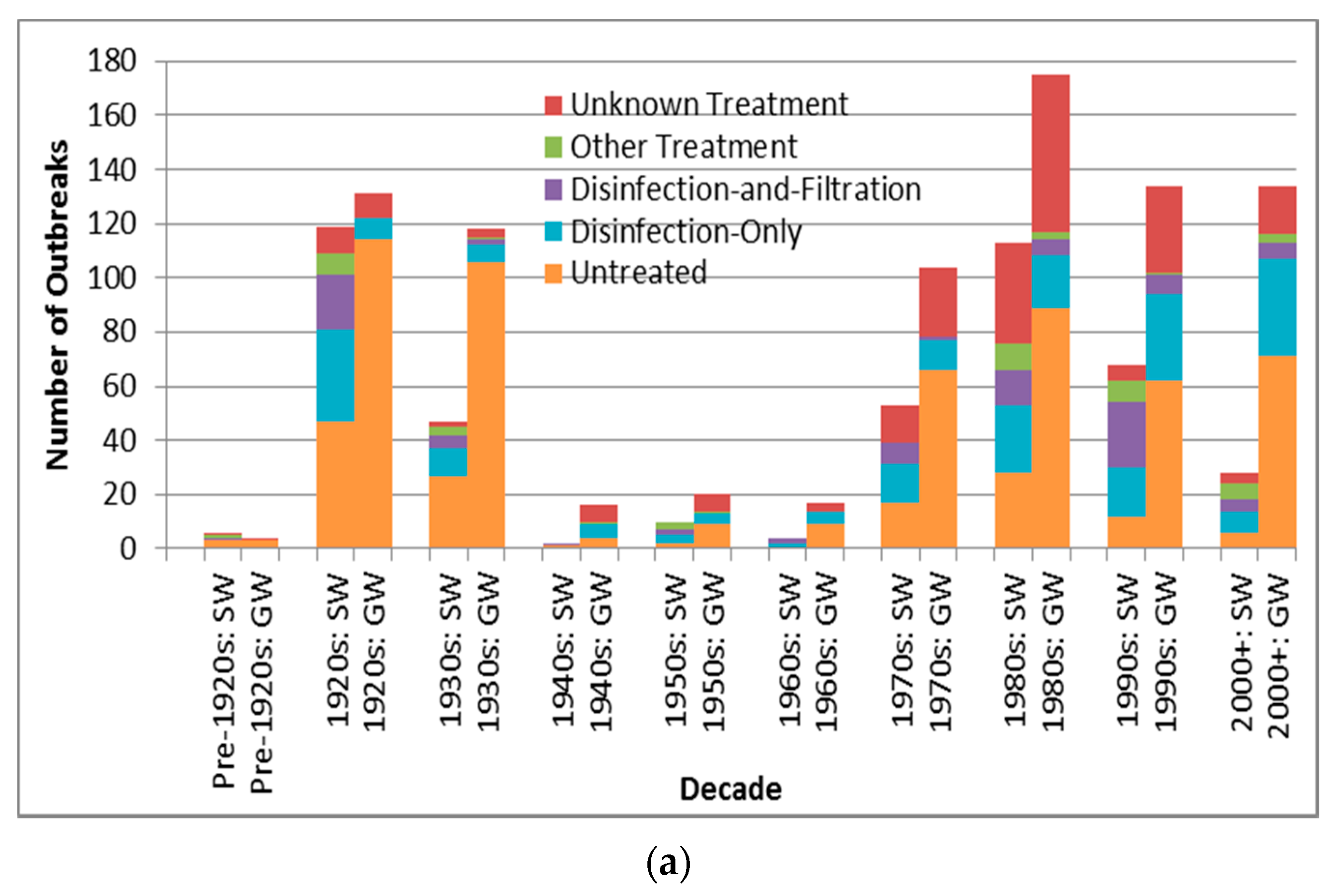
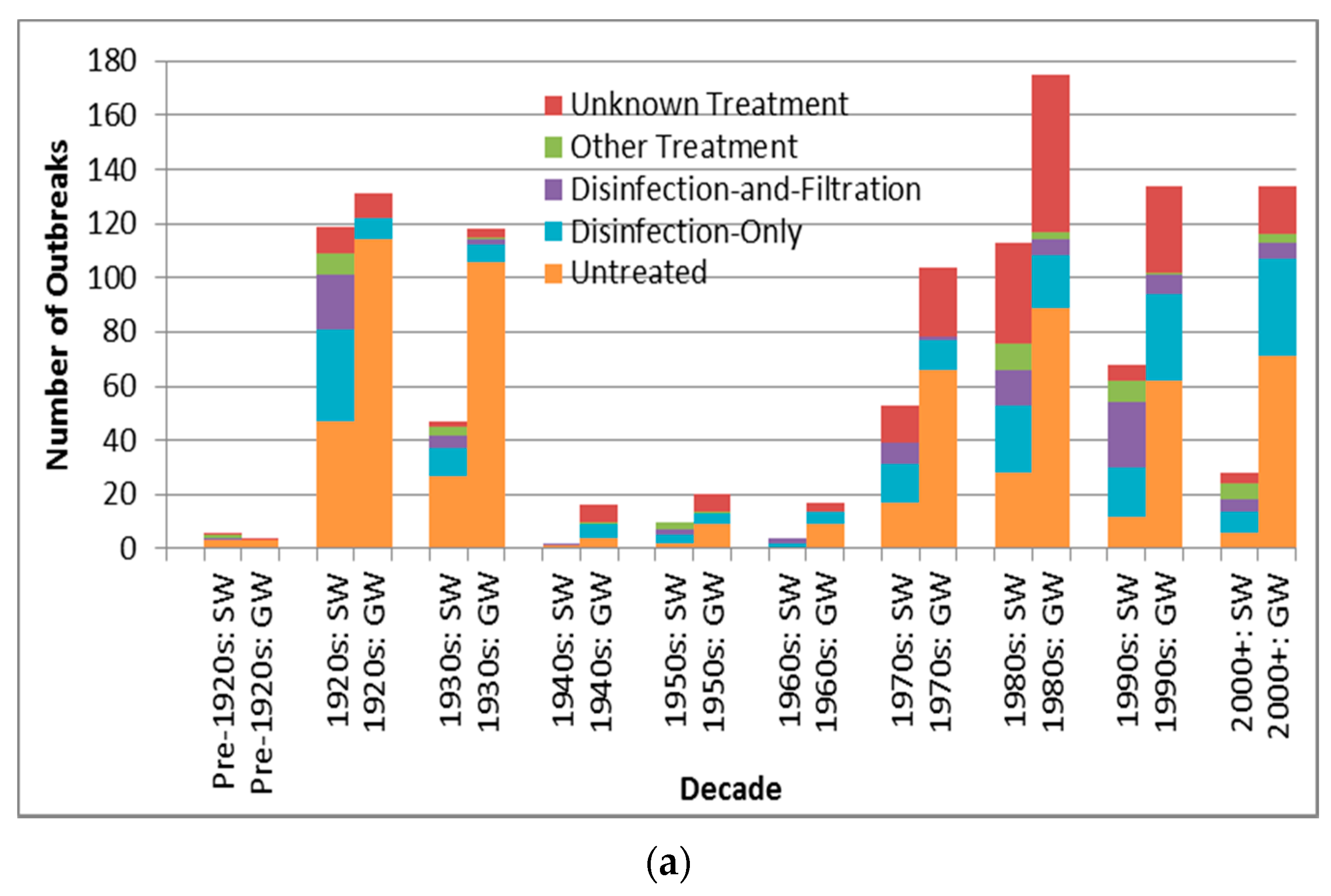
The descending order in outbreak frequency for untreated, disinfection-only, and disinfection -and-filtration system outbreaks could arise from the relative extent of treatment applied and/or from the relative size of population served by each category, which likely changed substantively during the period analyzed in this review for example with the conversion of untreated systems to treated systems in much of the developed world. For example, many U.S. cities implemented filtration and chlorination treatment in the early 20th century [
34]. This trend towards decreasing untreated system outbreaks (both surface water and groundwater) starting in the 1920s, excluding the low-reporting 1940s–1960s period, is supported by
Figure 4a. The decline in unknown type treatment attribution beyond the 1980s could suggest improved DWDO reporting in developed countries (host to almost all identified outbreaks) associated with the adoptions of NWDOS by several European countries.
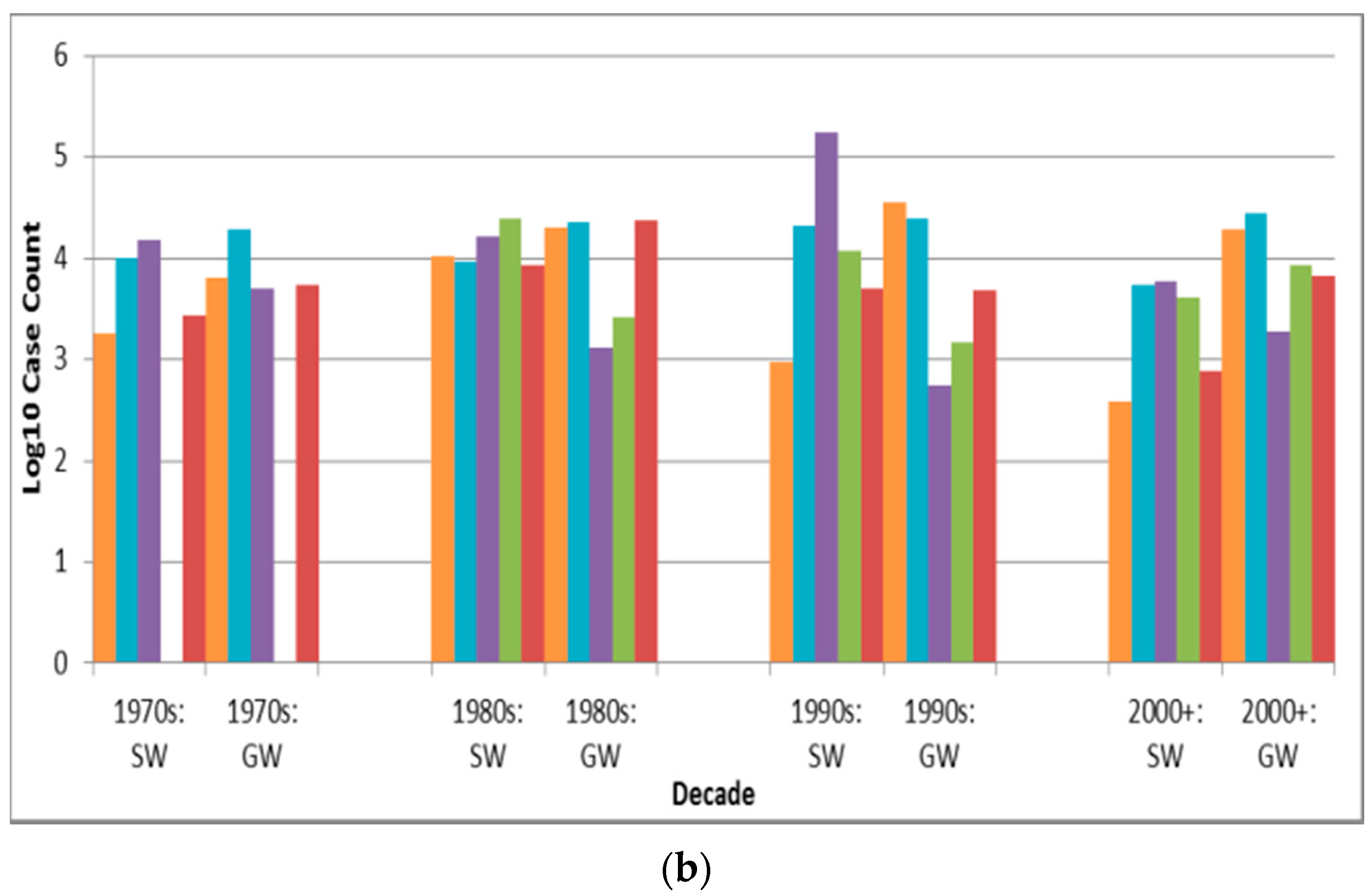
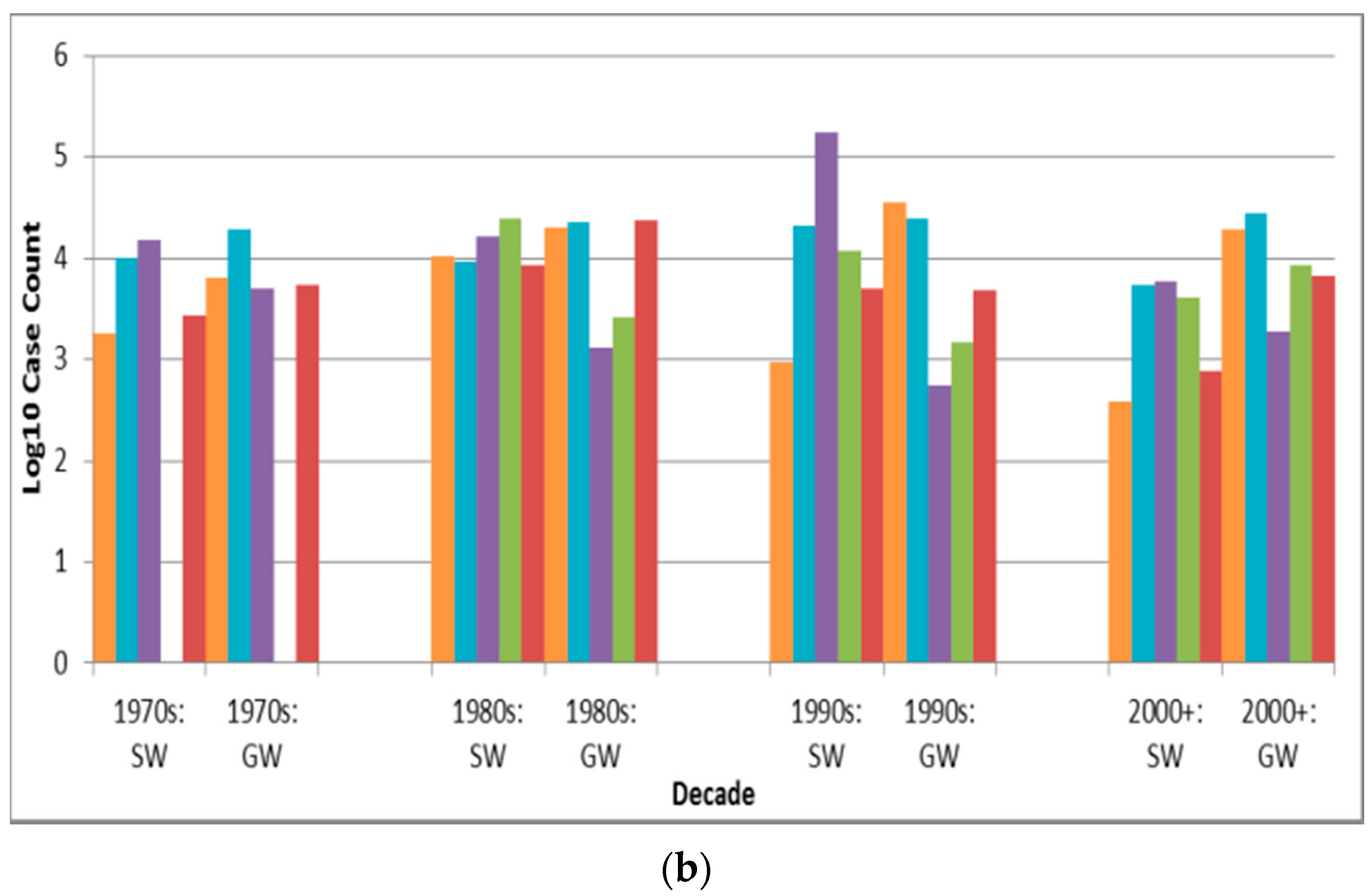
The increase in groundwater disinfection-only system outbreak frequency (
Figure 4a) and the slight increase in log
10 decadal case count for such outbreaks (
Figure 4b) from the 1970s suggest the need for enhanced treatment and oversight of such systems. This contrasts the decrease in log
10 decadal case count for surface water outbreaks of all five treatment types from the 1990s–on (which may further reflect the success of the aforementioned surface water-focused policies in reducing surface water DWDO disease burden). The increase in groundwater disinfection-only outbreak log
10 decadal case count implies that the widespread approach of permitting disinfection-only groundwater systems may be insufficient. However, it is also possible that the increase derives from improved outbreak reporting, which could also explain other increasing frequency and case count trends.
The case counts of disinfection-only and disinfection-and-filtration source outbreaks are significantly (p < 0.0001 for both) higher than those for untreated source outbreaks. This may arise from untreated water sources being smaller and/or better-protected (e.g., with better siting) than the other two source types. In the latter case, if disinfection or one or both of disinfection and filtration failed consumers could be exposed to a higher risk source (more conducive to higher case count) as compared to typical untreated sources.
4.2.6. Associated Deficiencies
Outbreaks associated with deficiencies in the realms of catchment or treatment are recorded more frequently (1.7 and 1.4 times, respectively) than outbreaks associated with distribution realm-associated deficiencies, a finding confirmed in an E.U. public drinking water supply-focused, 1990–2005 online DWDO literature review and analysis [
35]. In that study, catchment and treatment realm-associated deficiencies were each (not necessarily singularly) recorded for 41 of the total 61 outbreaks, making them far more frequent than distribution realm-associated deficiencies, recorded for 19 outbreaks. However, although distribution realm-associated deficiencies are less frequent than those of the other realms, their outbreak case counts are significantly higher than those for outbreaks associated with the realms of catchment and treatment (
p < 0.0001 and 0.0007, respectively). This could be due to increased ease of associating all ill patients with the same (more-localized) exposure in a more limited number of jurisdictions in distribution realm-associated deficiency outbreaks, increasing the probability of successful case reporting and attribution to a single outbreak.
There was a relatively high number of groundwater catchment realm-associated deficiency outbreaks in the 1920s and 1930s (
Figure 5a) compared to the groundwater outbreaks associated with the other four deficiency realms. This may be explained by lower wastewater treatment capabilities during those decades. For example, with fewer U.S. cities implementing primary sewage treatment and sewage chlorination than water treatment by that time [
34], sewage infiltration into (often untreated) water supplies might have presented a greater public health threat than treatment or distribution realm-associated deficiencies.
The decreasing frequency (and log
10 decadal case count,
Figure 5b) of treatment realm-associated deficiency outbreaks from the 1980s noted for surface water (and less so for groundwater) systems, consistent with the statistically-significant decrease (apparent for surface water outbreaks after introduction of the SWTR in 1989) in annual proportion of deficiencies related to treatment for the U.S. from 1971 to 2006 described in a 2010 review [
31], could reflect improved treatment, especially in the U.S, the E.U., Australia and Canada. In the latter three, filtration of surface water is not required but rather recommended, with requirements for filtration existing at more local jurisdictional scales, e.g., in the Canadian provinces of Nova Scotia, Quebec, Ontario, Saskatchewan and Alberta [
36]. In contrast, broadly steady outbreak frequency and log
10 decadal case count for outbreaks with catchment or distribution realm-associated deficiencies in both surface water and groundwater systems since the 1980s (also consistent with the 2010 U.S. review’s determination of lack of statistically-significant change in annual proportion of distribution system deficiencies [
31]) reflect the need to similarly strengthen oversight of those two realms. This could potentially be achieved through application of an integrated approach such as the Water Safety Plan, crafted and shown to successfully evaluate and manage risk from the catchment to the consumer (leading to statistically significant reductions in water supply contamination and waterborne disease in implementing areas in Iceland [
37]).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}