
The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities

Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. General Features
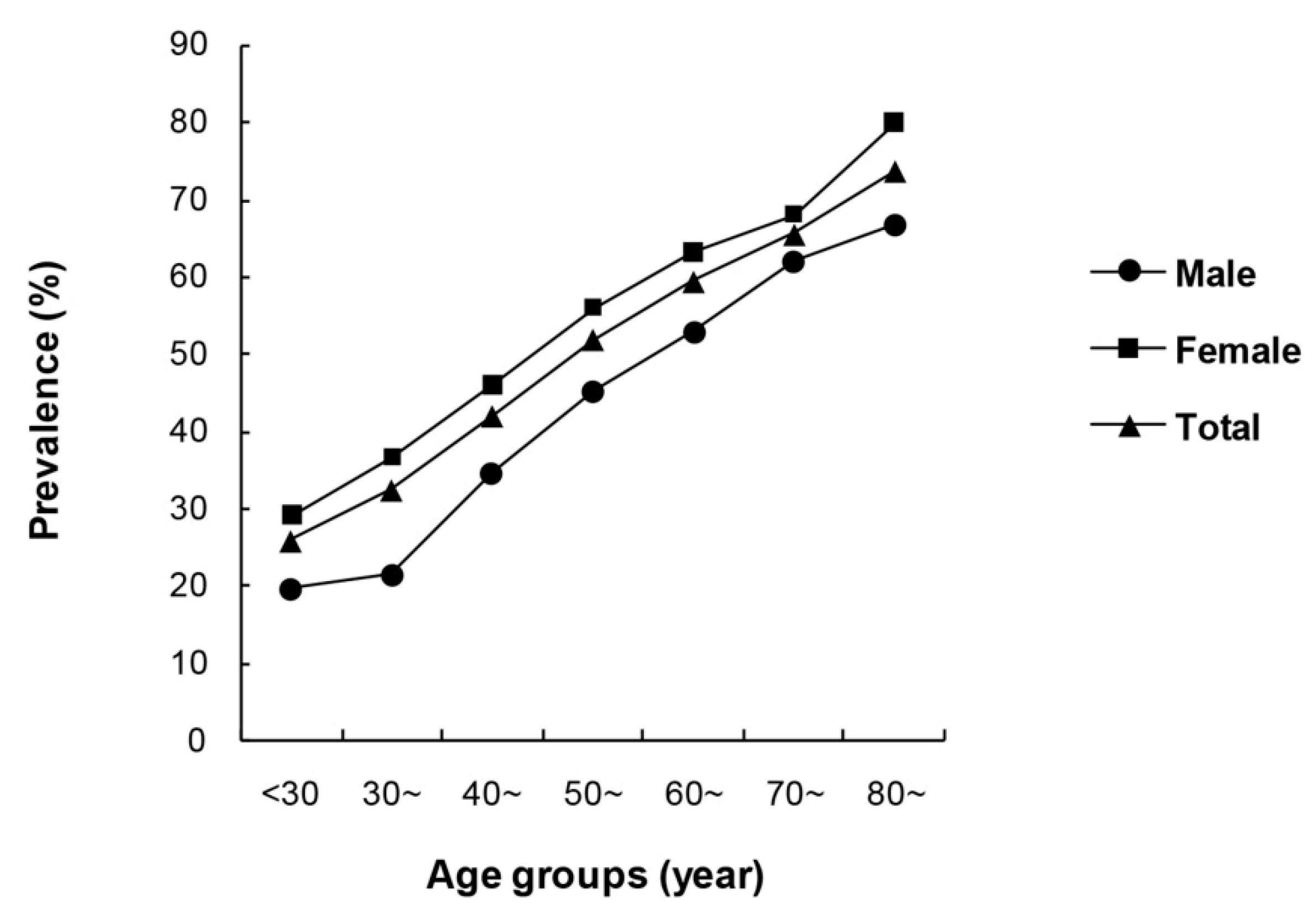
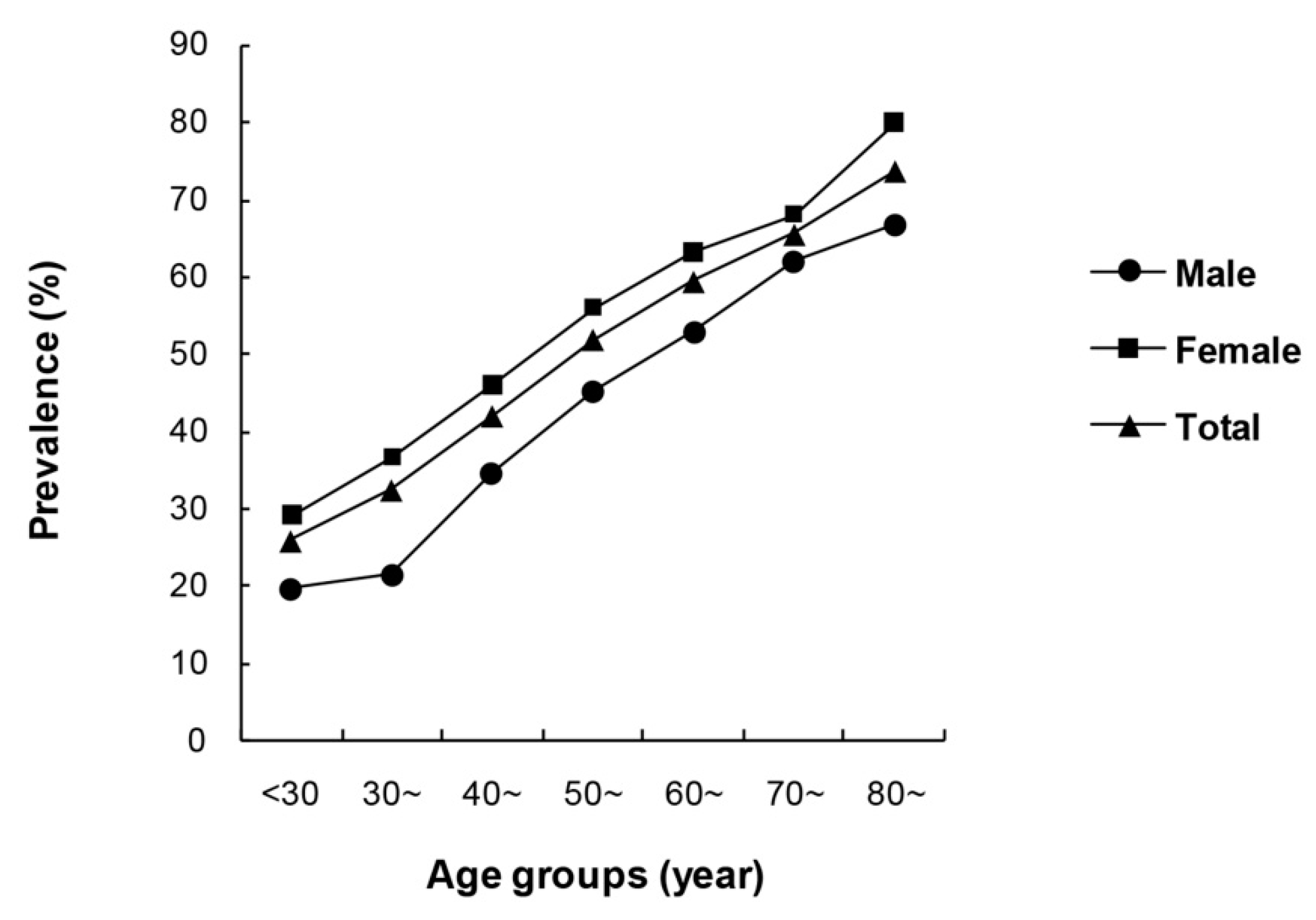
3.2. Epidemiological Characteristics of Thyroid Nodules
3.3. Correlation Analysis of Thyroid Nodules and Lifestyles
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PLA | People’s Liberation Army |
| TN | Thyroid nodules |
| WHO | World Health Organization |
| OR | Odds ratio |
| BMI | Body mass index |
| TSH | Thyrotropin |
| IR | Insulin resistance |
References
- Hegedus, L. The thyroid nodule. N. Engl. J. Med. 2004, 351, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.H.; Gharib, H. Thyroid incidentalomas: Management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann. Intern. Med. 1997, 126, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Siegel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA Cancer J. Clin. 2010, 60, 277–300. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Jung, E.J.; Park, S.T.; Jeong, S.H.; Jeong, C.Y.; Ju, Y.T.; Lee, Y.J.; Hong, S.C.; Choi, S.K.; Ha, W.S. Body size and thyroid nodules in healthy Korean population. J. Korean Surg. Soc. 2012, 82, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Sousa, P.A.; Vaisman, M.; Carneiro, J.R.; Guimaraes, L.; Freitas, H.; Pinheiro, M.F.; Liechocki, S.; Monteiro, C.M.; Teixeira, P.F. Prevalence of goiter and thyroid nodular disease in patients with class III obesity. Arq. Bras. Endocrinol. Metabol. 2013, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Ayturk, S.; Gursoy, A.; Kut, A.; Anil, C.; Nar, A.; Tutuncu, N.B. Metabolic syndrome and its components are associated with increased thyroid volume and nodule prevalence in a mild-to-moderate iodine-deficient area. Eur. J. Endocrinol. 2009, 161, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Xu, W.; Huang, Y.; Jin, X.; Deng, J.; Zhu, S.; Liu, H.; Zhang, S.; Yu, Y. Associations of noniodized salt and thyroid nodule among the Chinese population: A large cross-sectional study. Am. J. Clin. Nutr. 2013, 98, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Sun, M.; He, W.; Chen, H.; Li, W.; Tang, J.; Tang, W.; Lu, J.; Bi, Y.; Ning, G.; et al. The prevalence of thyroid nodules and its relationship with metabolic parameters in a Chinese community-based population aged over 40 years. Endocrine 2014, 45, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, S.; Sarti, D.A.; Cain, D.R.; Braunstein, G.D. Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch. Intern. Med. 1994, 154, 1838–1840. [Google Scholar] [CrossRef] [PubMed]
- Frates, M.C.; Benson, C.B.; Doubilet, P.M.; Cibas, E.S.; Marqusee, E. Can color Doppler sonography aid in the prediction of malignancy of thyroid nodules. J. Ultrasound Med. 2003, 22, 127–131. [Google Scholar] [PubMed]
- Akarsu, E.; Akcay, G.; Capoglu, I.; Unuvar, N. Iodine deficiency and goiter prevalence of the adult population in Erzurum. Acta Medica Hradec Kralove 2005, 48, 39–42. [Google Scholar] [PubMed]
- McCaffrey, T.V. Evaluation of the thyroid nodule. Cancer Control 2000, 7, 223–228. [Google Scholar] [PubMed]
- Knudsen, N.; Laurberg, P.; Perrild, H.; Bulow, I.; Ovesen, L.; Jorgensen, T. Risk factors for goiter and thyroid nodules. Thyroid 2002, 12, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Bartolotta, T.V.; Midiri, M.; Runza, G.; Galia, M.; Taibbi, A.; Damiani, L.; Palermo, P.G.; Lagalla, R. Incidentally discovered thyroid nodules: Incidence, and greyscale and colour Doppler pattern in an adult population screened by real-time compound spatial sonography. Radiol. Med. 2006, 111, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Aghini-Lombardi, F.; Antonangeli, L.; Martino, E.; Vitti, P.; Maccherini, D.; Leoli, F.; Rago, T.; Grasso, L.; Valeriano, R.; Balestrieri, A.; et al. The spectrum of thyroid disorders in an iodine-deficient community: The Pescopagano survey. J. Clin. Endocrinol. Metab. 1999, 84, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Hampel, R.; Kulberg, T.; Klein, K.; Jerichow, J.U.; Pichmann, E.G.; Clausen, V.; Schmidt, I. Goiter incidence in Germany is greater than previously suspected. Med. Klin. 1995, 90, 324–329. [Google Scholar]
- Furlanetto, T.W.; Peccin, S.; de O. Schneider, M.A.; dos, S. Z.; Zimme, A.; dos Reis, P.S.; Genro, S.K.; Ferreira, E.V.; Bittelbrum, F.; Muller, A.S.; Silva, R.W.; et al. Prevalence of thyroid nodules in 40 years-old or old women. Rev. Assoc. Medica Brasil. 2000, 46, 331–334. [Google Scholar] [CrossRef]
- Knudsen, N.; Bulow, I.; Jorgensen, T.; Laurberg, P.; Ovesen, L.; Perrild, H. Goitre prevalence and thyroid abnormalities at ultrasonography: A comparative epidemiological study in two regions with slightly different iodine status. Clin. Endocrinol. 2000, 53, 479–485. [Google Scholar] [CrossRef]
- Knudsen, N.; Perrild, H.; Christiansen, E.; Rasmussen, S.; Dige-Petersen, H.; Jorgensen, T. Thyroid structure and size and two-year follow-up of solitary cold thyroid nodules in an unselected population with borderline iodine deficiency. Eur. J. Endocrinol. 2000, 142, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.W.; No, J.H.; Chung, J.H.; Min, Y.K.; Lee, M.S.; Lee, M.K.; Yang, J.H.; Kim, K.W. Prevalence, clinical and ultrasonographic characteristics of thyroid incidentalomas. Thyroid 2004, 14, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Vander, J.B.; Gaston, E.A.; Dawber, T.R. The significance of nontoxic thyroid nodules. Final report of a 15-year study of the incidence of thyroid malignancy. Ann. Intern. Med. 1968, 69, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Kung, A.W.; Chau, M.T.; Lao, T.T.; Tam, S.C.; Low, L.C. The effect of pregnancy on thyroid nodule formation. J. Clin. Endocrinol. Metab. 2002, 87, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Struve, C.W.; Haupt, S.; Ohlen, S. Influence of frequency of previous pregnancies on the prevalence of thyroid nodules in women without clinical evidence of thyroid disease. Thyroid 1993, 3, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Lean, A.D.; Ferland, L.; Drouin, J.; Kelly, P.A.; Labrie, F. Modulation of pituitary thyrotropin releasing hormone receptor levels by estrogens and thyroid hormones. Endocrinology 1977, 100, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Franklyn, J.A.; Wood, D.F.; Balfour, N.J.; Ramsden, D.B.; Docherty, K.; Sheppard, M.C. Modulation by oestrogen of thyroid hormone effects on thyrotrophin gene expression. J. Endocrinol. 1987, 115, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Yane, K.; Kitahori, Y.; Konishi, N.; Okaichi, K.; Ohnishi, T.; Miyahara, H.; Matsunaga, T.; Lin, J.C.; Hiasa, Y. Expression of the estrogen receptor in human thyroid neoplasms. Cancer Lett. 1994, 84, 59–66. [Google Scholar] [CrossRef]
- Del, S.L.; Degli, U.E.; Hanau, S.; Piva, R.; Rossi, R.; Trasforini, G. In vitro effects of estrogen on tgb and c-myc gene expression in normal and neoplastic human thyroids. Mol. Cell. Endocrinol. 1989, 63, 67–74. [Google Scholar]
- Furlanetto, T.W.; Nguyen, L.Q.; Jameson, J.L. Estradiol increases proliferation and down-regulates the sodium/iodide symporter gene in FRTL-5 cells. Endocrinology 1999, 140, 5705–5711. [Google Scholar] [CrossRef] [PubMed]
- Manole, D.; Schildknecht, B.; Gosnell, B.; Adams, E.; Derwahl, M. Estrogen promotes growth of human thyroid tumor cells by different molecular mechanisms. J. Clin. Endocrinol. Metab. 2001, 86, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Ceresini, G.; Milli, B.; Morganti, S.; Maggio, M.; Bacchi-Modena, A.; Sgarabotto, M.P.; Chirico, C.; Di, D.P.; Campanati, P.; Valcavi, R.; et al. Effect of estrogen therapy for 1 year on thyroid volume and thyroid nodules in postmenopausal women. Menopause 2008, 15, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Park, Y.R.; Lim, D.J.; Yoon, K.H.; Kang, M.I.; Cha, B.Y.; Lee, K.W.; Son, H.Y. The relationship between thyroid nodules and uterine fibroids. Endocr. J. 2010, 57, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Sumitani, H.; Shozu, M.; Segawa, T.; Murakami, K.; Yang, H.J.; Shimada, K.; Inoue, M. In situ estrogen synthesized by aromatase P450 in uterine leiomyoma cells promotes cell growth probably via an autocrine/intracrine mechanism. Endocrinology 2000, 141, 3852–3861. [Google Scholar] [CrossRef] [PubMed]
- Dalla, V.L.; Ramina, A.; Vianello, S.; Fassina, A.; Belvedere, P.; Colombo, L. Potential for estrogen synthesis and action in human normal and neoplastic thyroid tissues. J. Clin. Endocrinol. Metab. 1998, 83, 3702–3709. [Google Scholar] [CrossRef]
- Kawabata, W.; Suzuki, T.; Moriya, T.; Fujimori, K.; Naganuma, H.; Inoue, S.; Kinouchi, Y.; Kameyama, K.; Takami, H.; Shimosegawa, T.; et al. Estrogen receptors (alpha and beta) and 17beta-hydroxysteroid dehydrogenase type 1 and 2 in thyroid disorders: Possible in situ estrogen synthesis and actions. Mod. Pathol. 2003, 16, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Barrere, X.; Valeix, P.; Preziosi, P.; Bensimon, M.; Pelletier, B.; Galan, P.; Hercberg, S. Determinants of thyroid volume in healthy French adults participating in the SU.VI.MAX cohort. Clin. Endocrinol. 2000, 52, 273–278. [Google Scholar] [CrossRef]
- Brix, T.H.; Hansen, P.S.; Kyvik, K.O.; Hegedus, L. Cigarette smoking and risk of clinically overt thyroid disease: A population-based twin case-control study. Arch. Intern. Med. 2000, 160, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.M.; Maravall, F.J.; Gomez, N.; Guma, A.; Soler, J. Determinants of thyroid volume as measured by ultrasonography in healthy adults randomly selected. Clin. Endocrinol. 2000, 53, 629–634. [Google Scholar] [CrossRef]
- Knudsen, N.; Bulow, I.; Laurberg, P.; Ovesen, L.; Perrild, H.; Jorgensen, T. Association of tobacco smoking with goiter in a low-iodine-intake area. Arch. Intern. Med. 2002, 162, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.F.; Yang, Y.; Li, J.Y.; Li, X.M.; Ma, A.G. Prevalence of thyroid nodules and influencing factors among employees of a company in Qingdao. Chin. J. Prev. Med. 2012, 46, 228–232. [Google Scholar]
- Aydin, L.Y.; Aydin, Y.; Besir, F.H.; Demirin, H.; Yildirim, H.; Onder, E.; Dumlu, T.; Celbek, G. Effect of smoking intensity on thyroid volume, thyroid nodularity and thyroid function: The Melen study. Minerva Endocrinol. 2011, 36, 273–280. [Google Scholar] [PubMed]
- Knudsen, N.; Bulow, I.; Laurberg, P.; Perrild, H.; Ovesen, L.; Jorgensen, T. High occurrence of thyroid multinodularity and low occurrence of subclinical hypothyroidism among tobacco smokers in a large population study. J. Endocrinol. 2002, 175, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Carle, A.; Laurberg, P.; Pedersen, I.B.; Rasmussen, L.B.; Ovesen, L.; Jorgensen, T. The impact of smoking on thyroid volume and function in relation to a shift towards iodine sufficiency. Eur. J. Epidemiol. 2008, 23, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Karatoprak, C.; Kartal, I.; Kayatas, K.; Ozdemir, A.; Yolbas, S.; Meric, K.; Demirtunc, R. Does smoking affect thyroid gland enlargement and nodule formation in iodine-sufficient regions. Ann. Endocrinol. 2012, 73, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, N.; Bulow, I.; Laurberg, P.; Perrild, H.; Ovesen, L.; Jorgensen, T. Alcohol consumption is associated with reduced prevalence of goitre and solitary thyroid nodules. Clin. Endocrinol. 2001, 55, 41–46. [Google Scholar] [CrossRef]
- Rezzonico, J.; Rezzonico, M.; Pusiol, E.; Pitoia, F.; Niepomniszcze, H. Introducing the thyroid gland as another victim of the insulin resistance syndrome. Thyroid 2008, 18, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Dramaix, M.; Moreno-Reyes, R. Does a small difference in iodine status among children in two regions of Belgium translate into a different prevalence of thyroid nodular diseases in adults. Eur. J. Nutr. 2012, 51, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Szabolcs, I.; Podoba, J.; Feldkamp, J.; Dohan, O.; Farkas, I.; Sajgo, M.; Takats, K.I.; Goth, M.; Kovacs, L.; Kressinszky, K.; et al. Comparative screening for thyroid disorders in old age in areas of iodine deficiency, long-term iodine prophylaxis and abundant iodine intake. Clin. Endocrinol. 1997, 47, 87–92. [Google Scholar] [CrossRef]
- Hu, F.N.; Teng, X.C.; Teng, W.P.; Guan, H.X.; Yang, F.; Gao, T.S.; Wang, W.B.; Shi, X.G.; Tong, Y.J. A comparative epidemic study of goiter and thyroid nodules in areas with different iodine intake. Chin. J. Endemiol. 2002, 21, 464–467. [Google Scholar]
- Leng, S.; Liu, Y.; Liu, H.X.; Zhao, H.; Sun, G.H.; Liang, H.W. Thyroid nodule disease among adult health examination participants in Dalian. Med. Philos. 2011, 32, 22–24. [Google Scholar]
- Knudsen, N.; Bulow, I.; Laurberg, P.; Ovesen, L.; Perrild, H.; Jorgensen, T. Low socio-economic status and familial occurrence of goitre are associated with a high prevalence of goitre. Eur. J. Epidemiol. 2003, 18, 175–181. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Total | Male | Female | p |
|---|---|---|---|---|
| n (%) | 6324 (100) | 2264 (35.8) | 4060 (64.2) | |
| Age (years) | 52.15 ± 11.58 | 52.88 ± 11.38 | 51.75 ± 11.68 | <0.001 |
| History of coronary heart disease (%) | 7.8 | 6.0 | 8.8 | <0.001 |
| History of diabetes (%) | 11.5 | 11.9 | 11.3 | 0.511 |
| History of hypertension (%) | 30.2 | 30.8 | 29.8 | 0.411 |
| History of dyslipidemia (%) | 10.5 | 10.5 | 10.5 | 0.962 |
| Smoker (%) | 30.0 | 72.6 | 6.2 | <0.001 |
| Drinker (%) | 27.2 | 67.9 | 4.4 | <0.001 |
| BMI (kg/m2) | 27.02 ± 3.98 | 27.18 ± 3.78 | 26.93 ± 4.08 | 0.014 |
| Prevalence | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Solitary nodules | 395 | 40.8 | 704 | 33.0 | 1099 | 35.5 |
| Multiple nodules | 572 | 59.2 | 1429 | 67.0 | 2001 | 64.5 |
| Total | 967 | 42.7 | 2133 | 52.5 | 3100 | 49.0 |
| Parameters | Male | p | Female | p | |||
|---|---|---|---|---|---|---|---|
| TN (+) (%) | TN (−) (%) | TN (+) (%) | TN (−) (%) | ||||
| Smoking History | Current smokers | 43.7 | 56.3 | 0.376 | 61.4 | 38.6 | 0.007 |
| Former smokers | 42.1 | 57.9 | 64.4 | 35.6 | |||
| Non-smokers | 40.3 | 59.7 | 51.9 | 48.1 | |||
| Missing | 3.9 | ||||||
| Drinking History | Current drinkers | 43.1 | 56.9 | 0.376 | 49.0 | 51.0 | 0.061 |
| Former drinkers | 45.4 | 54.6 | 75.0 | 25.0 | |||
| Non-drinkers | 40.5 | 59.5 | 52.5 | 47.5 | |||
| Missing | 4.1 | ||||||
| Parameters | Categories | TN (+) (%) | TN (−) (%) | p |
|---|---|---|---|---|
| Taste preference | Salty | 48.6 | 51.4 | 0.854 |
| Average | 49.4 | 50.6 | ||
| Less Salty | 48.8 | 51.2 | ||
| Missing | 4.1 | |||
| Seafood intake | Frequently | 46.1 | 53.9 | 0.048 |
| Occasionally | 48.5 | 51.5 | ||
| Never | 52.4 | 47.6 | ||
| Missing | 4.1 | |||
| Physical labor intensity | Very light | 50.5 | 49.5 | 0.001 |
| Light | 45.4 | 54.6 | ||
| Moderate | 43.1 | 56.9 | ||
| Heavy | 25.0 | 75.0 | ||
| Missing | 4.4 | |||
| Physical exercise intensity | Mild | 49.6 | 50.4 | 0.01 |
| Moderate | 47.5 | 52.5 | ||
| High | 34.4 | 65.6 | ||
| Missing | 8.3 | |||
| Education level | Illiteracy | 63.9 | 36.1 | <0.001 |
| Primary school | 56.8 | 43.2 | ||
| Secondary school | 47.9 | 52.1 | ||
| High school | 46.6 | 53.4 | ||
| Polytechnic school | 37.4 | 62.6 | ||
| Undergraduate and above | 32.2 | 67.8 | ||
| Missing | 1.2 |
| Variables | β | SE | p | OR | 95% CI |
|---|---|---|---|---|---|
| Age | 0.038 | 0.003 | <0.001 | 1.039 | 1.034–1.044 |
| Female | 0.582 | 0.081 | <0.001 | 1.789 | 1.527–2.097 |
| BMI | 0.019 | 0.007 | 0.006 | 1.019 | 1.005–1.034 |
| Smoking | 0.017 | ||||
| Former Smokers | −0.045 | 0.129 | 0.729 | 0.956 | 0.743–1.231 |
| Current Smokers | 0.220 | 0.089 | 0.014 | 1.246 | 1.046–1.483 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, H.; Tian, Y.; Yan, W.; Kong, Y.; Wang, H.; Wang, A.; Dou, J.; Liang, P.; Mu, Y. The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities. Int. J. Environ. Res. Public Health 2016, 13, 442. https://doi.org/10.3390/ijerph13040442
Jiang H, Tian Y, Yan W, Kong Y, Wang H, Wang A, Dou J, Liang P, Mu Y. The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities. International Journal of Environmental Research and Public Health. 2016; 13(4):442. https://doi.org/10.3390/ijerph13040442
Chicago/Turabian StyleJiang, Hua, Yongfeng Tian, Wenhua Yan, Yue Kong, Haibin Wang, Anping Wang, Jingtao Dou, Ping Liang, and Yiming Mu. 2016. "The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities" International Journal of Environmental Research and Public Health 13, no. 4: 442. https://doi.org/10.3390/ijerph13040442
APA StyleJiang, H., Tian, Y., Yan, W., Kong, Y., Wang, H., Wang, A., Dou, J., Liang, P., & Mu, Y. (2016). The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities. International Journal of Environmental Research and Public Health, 13(4), 442. https://doi.org/10.3390/ijerph13040442