A Cross-Cultural Comparison of Health Behaviors between Saudi and British Adolescents Living in Urban Areas: Gender by Country Analyses



Abstract
:1. Introduction
2. Methods
2.1. Locations and Participants
2.2. Anthropometric Measurements
2.3. Assessment of Health Behaviors
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Variable | Male | Female | All | p-value | |||
|---|---|---|---|---|---|---|---|
| Saudi | British | Saudi | British | Saudi | British | ||
| Number of participants | 797 | 590 | 851 | 568 | 1648 | 1158 | |
| Age (year) a | 16.5 ± 1.0 | 15.2 ± 0.96 | 16.4 ± 0.95 | 15.2 ± 0.95 | 16.5 ± 0.98 | 15.2 ± 0.95 | country: 0.010 gender × country interaction: 0.599 |
| Weight (kg) b | 69.1 ± 20.3 | 64.4 ± 13.9 | 58.3 ± 15.1 | 57.8 ± 11.5 | 63.5 ± 18.6 | 61.2 ± 13.3 | country: 0.403 gender × country interaction: 0.001 |
| Height (cm) b | 168.3 ± 7.6 | 171.6 ± 8.2 | 157.2 ± 5.9 | 161.8 ± 7.6 | 162.6 ± 8.8 | 166.9 ± 9.3 | country: <0.001 gender × country interaction: 0.027 |
| BMI (kg/m2) b | 24.3 ± 6.7 | 21.8 ± 4.0 | 23.6 ± 5.8 | 22.1 ± 4.0 | 23.9 ± 6.3 | 22.9 ± 4.0 | country: <0.001 gender × country interaction: 0.025 |
| Overweight (%) c | 19.3 | 18.2 | 21.9 | 17.7 | 20.7 | 17.9 | <0.001 |
| Obesity (%) c | 22.6 | 6.1 | 12.9 | 6.3 | 17.6 | 6.2 | <0.001 |
| Overweight or obesity (%) c | 41.9 | 24.3 | 34.8 | 24.0 | 38.3 | 24.1 | <0.001 |
| Variable | Male | Female | All | |||
|---|---|---|---|---|---|---|
| Saudi | British | Saudi | British | Saudi | British | |
| Walking a, b, c, d | 351.5 ± 19.1 | 580.9 ± 22.4 | 187.9 ± 7.2 | 527.9 ± 20.6 | 271.6 ± 11.5 | 554.6 ± 15.2 |
| Stair Stepping a, b, c | 123.4 ± 3.4 | 183.4 ± 6.0 | 129.6 ± 3.3 | 202.7 ± 5.9 | 126.4 ± 2.4 | 192.9 ± 4.3 |
| Jogging b ,c, d | 444.7 ± 30.6 | 812.5 ± 44.3 | 176.1 ± 15.4 | 373.1 ± 28.4 | 313.6 ± 17.7 | 594.7 ± 27.2 |
| Cycling a, b, d | 148.6 ± 20.4 | 284.4 ± 31.9 | 72.3 ± 9.8 | 42.7 ± 6.6 | 111.3 ± 11.5 | 164.6 ± 16.8 |
| Swimming b, c, d | 291.8 ± 23.4 | 123.7 ± 14.0 | 193.8 ± 21.9 | 107.6 ± 15.7 | 243.9 ± 16.1 | 115.7 ± 10.5 |
| Martial art b, c, d | 114.6 ± 18.8 | 296.4 ± 29.7 | 28.3 ± 7.8 | 73.1 ± 13.4 | 72.5 ± 10.4 | 185.7 ± 16.7 |
| Weight training a, b, c, d | 204.5 ± 23.2 | 415.3 ± 30.4 | 15.3 ± 3.2 | 65.6 ± 9.8 | 112.1 ± 12.2 | 241.9 ± 16.9 |
| Household b, c | 107.6 ± 10.4 | 194.5 ± 14.3 | 250.8 ± 18.2 | 397.9 ± 22.4 | 177.5 ± 10.5 | 295.3 ± 13.6 |
| Moderate-intensity sport games a, b, c, d | 250.7 ± 17.1 | 500.5 ± 25.0 | 85.7 ± 10.8 | 436.5 ± 23.1 | 170.2 ± 10.5 | 468.8 ± 17.0 |
| Vigorous-intensity sport games b, c | 1,072.8 ± 55.1 | 1,423.3 ± 60.4 | 146.9 ± 15.9 | 549.7 ± 37.9 | 620.7 ± 31.8 | 990.3 ± 38.0 |
| Sum of all moderate-intensity physical activity b, c, d | 1,001.6 ± 42.0 | 1,399.6 ± 40.6 | 718.2 ± 33.6 | 1,469.9 ± 43.8 | 863.2 ± 27.3 | 1,434.5 ± 29.9 |
| Sum of all vigorous-intensity physical activity b, c, d | 2,108.6 ± 85.3 | 3,415.2 ± 109.5 | 568.6 ± 30.4 | 1,306.9 ± 61.4 | 1,356.6 ± 50.5 | 2,370.4 ± 70.4 |
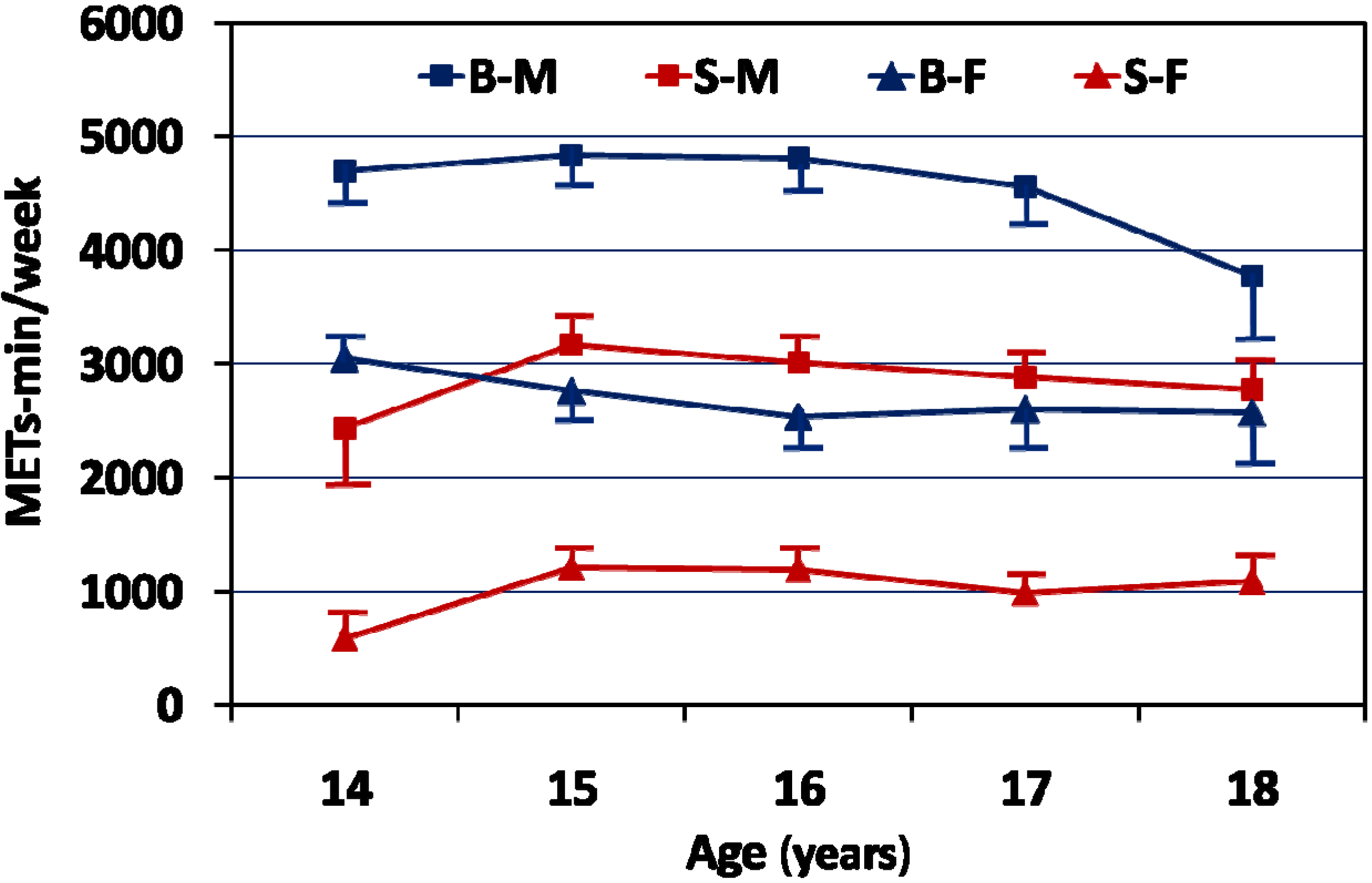
| Total physical activity a, b, c | 3,110.3 ± 107.9 | 4,814.8 ± 124.7 | 1,286.8 ± 52.5 | 2,776.9 ± 85.1 | 2,219.9 ± 65.5 | 3,804.8 ± 81.5 |

| Activity Category * | Age category | Male | Female | All | |||
|---|---|---|---|---|---|---|---|
| Saudi | British | Saudi | British | Saudi | British | ||
| Low active (<1,680 METs-min/week) | 14–16 | 45.2 | 17.8 | 76.9 | 33.7 | 61.9 | 25.8 |
| >16–18 | 47.9 | 14.3 | 83.8 | 35.2 | 66.0 | 23.9 | |
| 14–18 | 46.6 | 17.3 | 80.3 | 34.0 | 64.0 | 25.4 | |
| Sufficiently Active (1,680–2,519 METs-min/week) | 14–16 | 12.2 | 8.4 | 11.0 | 24.2 | 11.6 | 16.2 |
| >16–18 | 11.9 | 15.9 | 7.0 | 24.1 | 9.4 | 19.7 | |
| 14–18 | 12.0 | 9.3 | 9.0 | 24.1 | 10.5 | 16.6 | |
| High Active (≥2,520 METs-min/week) | 14–16 | 42.6 | 73.8 | 12.1 | 42.0 | 26.5 | 58.0 |
| >16–18 | 40.2 | 69.8 | 9.2 | 40.7 | 24.6 | 56.4 | |
| 14–18 | 41.4 | 73.4 | 10.7 | 41.9 | 25.5 | 57.9 | |
| Variable | Male | Female | All | |||
|---|---|---|---|---|---|---|
| Saudi | British | Saudi | British | Saudi | British | |
| TV viewing b | 2.70 ± 2.0 | 2.70 ± 1.7 | 3.00 ± 2.1 | 2.87 ± 1.7 | 2.85 ± 2.0 | 2.78 ± 1.7 |
| Computer use b, c, d | 2.62 ± 2.2 | 2.68 ± 1.8 | 3.49 ± 2.5 | 2.88 ± 1.8 | 3.04 ± 2.4 | 2.78 ± 1.8 |
| Total screen time b, c, d | 5.31 ± 3.1 | 5.38 ± 2.8 | 6.48 ± 3.3 | 5.75 ± 2.7 | 5.89 ± 3.3 | 5.57 ± 2.7 |
| Variable | Male | Female | All | |||
|---|---|---|---|---|---|---|
| Saudi | British | Saudi | British | Saudi | British | |
| Breakfast consumption (frequency /week) a, b | 4.17 ± 2.7 | 4.34 ± 2.7 | 3.53 ± 2.6 | 3.35 ± 2.8 | 3.84 ± 2.7 | 3.84 ± 2.8 |
| Vegetables consumption (frequency/week) | 3.70 ± 2.4 | 3.87 ± 2.2 | 3.69 ± 2.4 | 4.12 ± 2.2 | 3.69 ± 2.4 | 4.00 ± 2.2 |
| Fruits consumption (frequency /week) a, b, c, d | 3.28 ± 2.3 | 3.54 ± 2.2 | 2.45 ± 2.1 | 3.56 ± 2.2 | 2.85 ± 2.2 | 3.55 ± 2.2 |
| Milk/dairy products intake (frequency/week) b, c, d | 4.49 ± 2.4 | 4.56 ± 2.1 | 3.86 ± 2.5 | 4.32 ± 2.1 | 4.16 ± 2.5 | 4.44 ± 2.1 |
| Sugar-sweetened drinks intake (frequency /week) b, c | 4.96 ± 2.2 | 3.85 ± 2.3 | 4.44 ± 2.3 | 3.34 ± 2.3 | 4.69 ± 2.3 | 3.60 ± 2.3 |
| Fast foods intake (frequency/week) b | 2.90 ± 1.9 | 2.63 ± 1.8 | 2.60 ± 1.8 | 2.57 ± 1.8 | 2.74 ± 1.9 | 2.60 ± 1.8 |
| French fries/potato chips intake (frequency /week) b, c, d | 2.36 ± 2.0 | 3.00 ± 1.9 | 2.90 ± 2.0 | 2.93 ± 1.9 | 2.64 ± 2.0 | 2.96 ± 1.9 |
| Cake/donuts intake (frequency/week) b, c | 2.52 ± 2.1 | 3.10 ± 2.0 | 2.76 ± 2.1 | 3.28 ± 2.0 | 2.65 ± 2.1 | 3.19 ± 2.0 |
| Sweets intake (frequency/week) b, d | 3.04 ± 2.3 | 3.56 ± 2.1 | 4.08 ± 2.3 | 3.86 ± 2.0 | 3.58 ± 2.3 | 3.71 ± 2.0 |
| Energy drinks intake (frequency/week) b, c | 1.48 ± 2.1 | 2.23 ± 2.2 | 0.89 ± 1.7 | 1.42 ± 2.0 | 1.17 ± 2.0 | 1.82 ± 2.2 |
| Variable | Gender | Saudi | British | p-value * |
|---|---|---|---|---|
| Sedentary (>2 hours/day of screen time) | M | 84.2 | 89.5 | 0.003 |
| F | 91.6 | 92.2 | 0.374 | |
| All | 88.0 | 90.8 | 0.010 | |
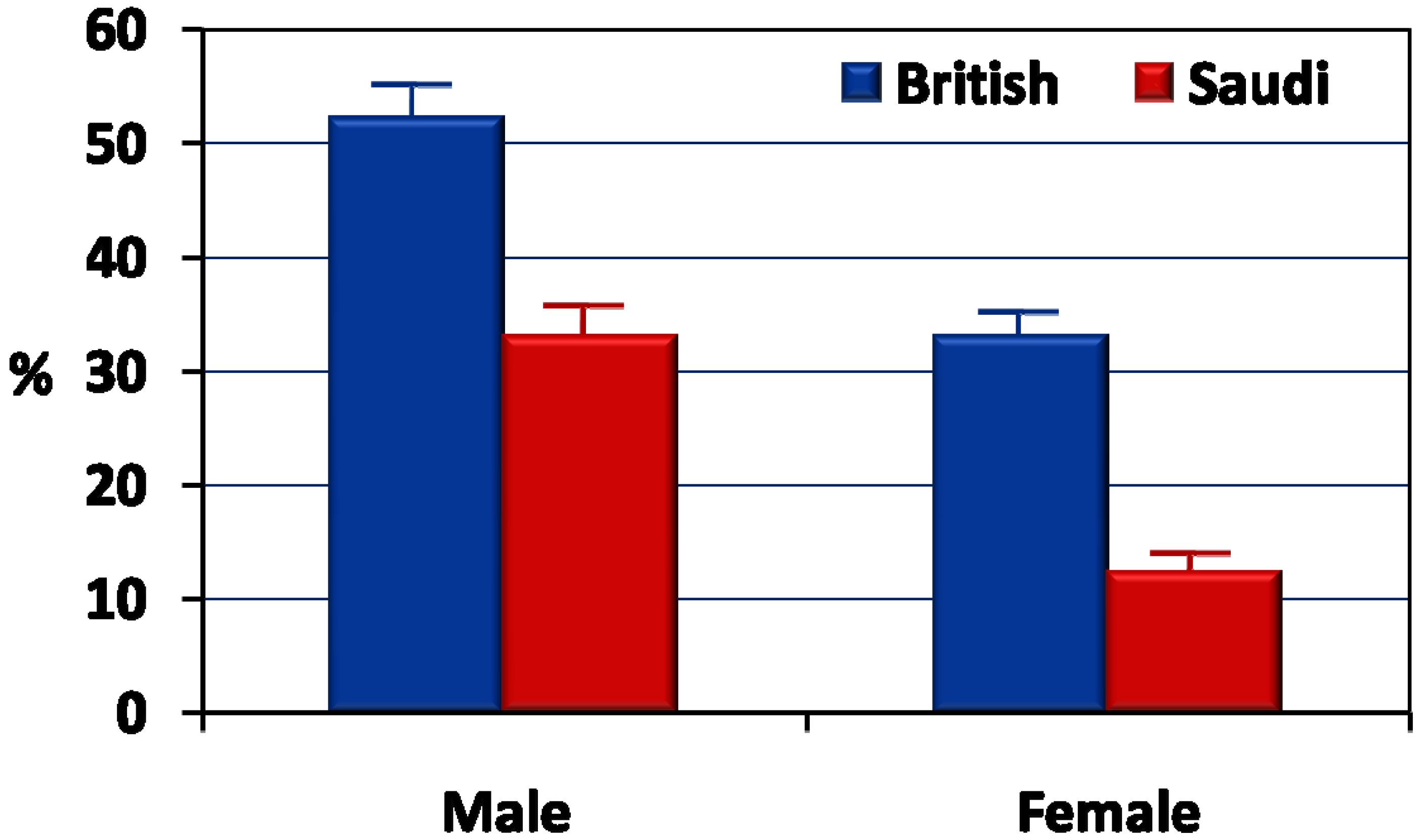
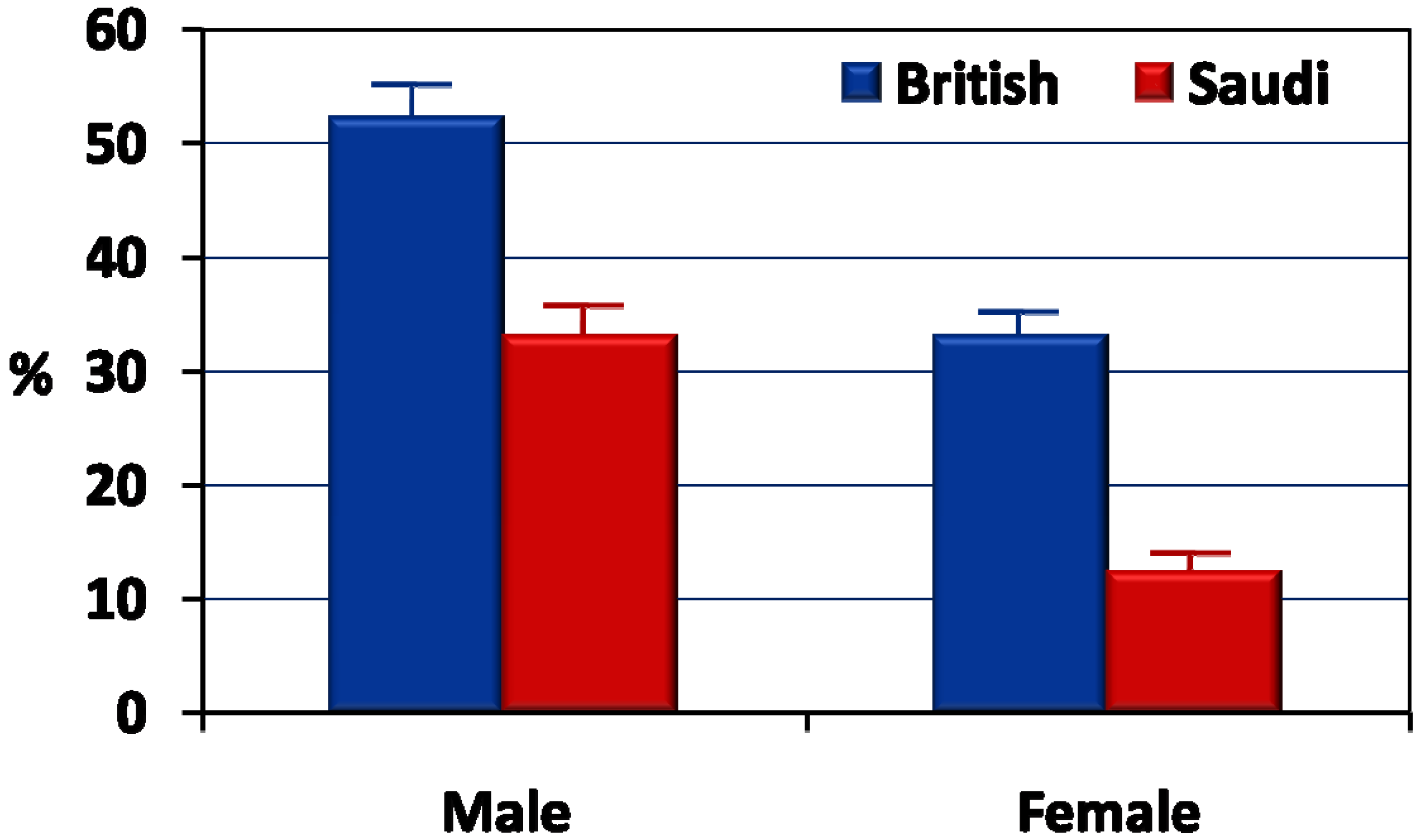
| Inactive (<1,680 METs-min/week) 1 | M | 46.5 | 17.3 | <0.001 |
| F | 80.3 | 33.9 | <0.001 | |
| All | 64.0 | 25.5 | <0.001 | |
| Daily breakfast intake | M | 34.4 | 39.4 | 0.035 |
| F | 22.8 | 27.4 | 0.031 | |
| All | 28.4 | 33.5 | 0.002 | |
| Daily vegetables intake | M | 23.2 | 18.7 | 0.026 |
| F | 22.7 | 24.4 | 0.256 | |
| All | 23.0 | 21.5 | 0.194 | |
| Daily fruit intake | M | 16.6 | 15.8 | 0.366 |
| F | 9.8 | 17.3 | <0.001 | |
| All | 13.1 | 16.5 | 0.008 | |
| Daily milk intake | M | 35.4 | 30.5 | 0.032 |
| F | 27.9 | 26.9 | 0.360 | |
| All | 31.6 | 28.7 | 0.058 | |
| Sugar-sweetened drinks intake (4+ day/week) | M | 70.2 | 53.1 | <0.001 |
| F | 60.0 | 44.6 | <0.001 | |
| All | 64.9 | 48.9 | <0.001 | |
| Fast food intake (4+ day/week) | M | 30.0 | 24.1 | 0.010 |
| F | 24.3 | 24.2 | 0.514 | |
| All | 27.1 | 24.2 | 0.047 | |
| French fries/potato chips intake (4+ day/week) | M | 23.4 | 34.5 | <0.001 |
| F | 31.7 | 35.6 | 0.071 | |
| All | 27.7 | 35.0 | <0.001 | |
| Cake/donut/biscuit intake (4+ day/week) | M | 26.3 | 39.4 | <0.001 |
| F | 29.3 | 41.5 | <0.001 | |
| All | 27.9 | 40.4 | <0.001 | |
| Sweets/chocolates intake (4+ day/week) | M | 36.5 | 45.9 | 0.015 |
| F | 54.6 | 54.4 | 0.503 | |
| All | 45.8 | 50.1 | 0.015 | |
| Energy drinks intake (4+ day/week) | M | 15.6 | 27.5 | <0.001 |
| F | 9.0 | 15.5 | <0.001 | |
| All | 12.2 | 21.5 | <0.001 |
4. Discussion
5. Conclusions
Acknowledgments
Authors’ Contributions
Conflicts of Interest
References
- World Health Organization. WHA57.17: Global Strategy on Diet, Physical Activity and Health; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.; Ezzati, M. The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Popkin, B.M. Global nutrition dynamics. The world is shifting rapidly toward a diet linked with noncommunicable diseases. Amer. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar]
- Call, K.T.; Riedel, A.A.; Hein, K.; McLoyd, V.; Petersen, A.; Kipke, M. Adolescent health and well-being in the twenty-first century: A global perspective. J. Res. Adolesce. 2002, 12, 69–98. [Google Scholar]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sport. Exercise 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Mitchell, J.A.; Pate, R.R.; Dowda, M.; Mattocks, C.; Riddoch, C.; Ness, A.R.; Blair, S.N. A prospective study of sedentary behavior in a large cohort of youth. Med. Sci. Sport. Exercise 2012, 44, 1081–1087. [Google Scholar] [CrossRef]
- Ekelund, U.; Brage, S.; Froberg, K.; Harro, M.; Anderssen, S.A.; Sardinha, L.B.; Riddoch, C.; Andersen, L.B. TV viewing and physical activity are independently associated with metabolic risk in children: The european youth heart study. PLoS Med. 2006, 3. [Google Scholar] [CrossRef]
- Sardinha, L.B.; Andersen, L.B.; Anderssen, S.A.; Quitério, A.L.; Ornelas, R.; Froberg, K.; Riddoch, C.J.; Ekelund, U. Objectively measured time spent sedentary is associated with insulin resistance independent of overall and central body fat in 9- to 10-year-old Portuguese children. Diabetes Care 2008, 31, 569–575. [Google Scholar]
- Lake, A.A.; Adamson, A.J.; Craigie, A.M.; Rugg-Gunn, A.J.; Mathers, J.C. Tracking of dietary intake and factors associated with dietary change from early adolescence to adulthood: The ASH30 study. Obes. Facts 2009, 2, 157–165. [Google Scholar] [CrossRef]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts. 2009, 2, 187–195. [Google Scholar] [CrossRef]
- Harris, M.I. Epidemiological correlates of NIDDM in Hispanics, whites, and blacks in the U.S. population. Diabetes Care 1991, 14, 639–648. [Google Scholar]
- Perez-Stable, E.J.; Marin, G.; Marin, B.V. Behavioral risk factors: A comparison of Latinos and non-Latino whites in San Francisco. Amer. J. Public. Health. 1994, 84, 971–976. [Google Scholar] [CrossRef]
- Crespo, C.J.; Smit, E.; Carter-Pokras, O.; Andersen, R. Acculturation and leisure-time physical inactivity in Mexican American adults: Results from NHANES III, 1988–1994. Amer. J. Public. Health. 2001, 91, 1254–1257. [Google Scholar] [CrossRef]
- Duncan, M.J.; Birch, S.; Al-Nakeeb, Y.; Nevill, A.M. Ambulatory physical activity levels of white and South Asian children in Central England. Acta Paediatr. 2012, 101. [Google Scholar] [CrossRef]
- Owen, C.G.; Nightingale, C.M.; Rudnicka, A.R.; Cook, D.G.; Ekelund, U.; Whincup, P.H. Ethnic and gender differences in physical activity levels among 9-10-year-old children of white European, South Asian and African-Caribbean origin: The child heart health study in England (CHASE study). Int. J. Epidemiol. 2009, 38, 1082–1093. [Google Scholar] [CrossRef]
- Sluyter, J.D.; Schaaf, D.; Metcalf, P.A.; Scragg, R.K. Dietary intakes of Pacific, Maori, Asian and European adolescents: The Auckland high school heart survey. Aust. N. Z. J. Publ. Health. 2010, 34, 32–37. [Google Scholar] [CrossRef]
- Rogers, A.; Adamson, J.E.; McCarthy, M. Variations in health behaviours among inner city 12-year-olds from four ethnic groups. Ethn. Health 1997, 2, 309–316. [Google Scholar] [CrossRef]
- Green, J.; Waters, E.; Haikerwal, A.; O’Neill, C.; Raman, S.; Booth, M.L.; Gibbons, K. Social, cultural and environmental influences on child activity and eating in Australian migrant communities. Child Care Health Develop. 2003, 29, 441–448. [Google Scholar] [CrossRef]
- Chen, M.Y.; James, K.; Wang, E.K. Comparison of health-promoting behavior between Taiwanese and American adolescents: A cross-sectional questionnaire survey. Int. J. Nurs. Stud. 2007, 44, 59–69. [Google Scholar] [CrossRef]
- International Monetary Fund. World Economic Outlook Database—October 2012. Available online: http://www.imf.org/external/pubs/ft/weo/2012/02/weodata/index.aspx (accessed on 20 November 2012).
- Al-Hazzaa, H.M.; Musaiger, A.; ATLS Group. Arab teens lifestyle study (ATLS): Objectives, design, methodology and implications. Diabetes Metab. Syndr. Obes. 2011, 4, 417–426. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8. [Google Scholar] [CrossRef]
- Al-Nakeeb, Y.; Lyons, M.; Collins, P.; Al-Nuaim, A.; Al-Hazzaa, H.; Duncan, M.J.; Nevill, A. Obesity, physical activity and sedentary behavior amongst British and Saudi youth: A cross-cultural study. Int. J. Environ. Res. Public Health 2012, 9, 1490–1506. [Google Scholar] [CrossRef]
- Cole, T.; Bellizzi, M.; Flegal, K.; Dietz, W. Establishing a standard definition of child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab teens lifestyle study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Public Health 2011, 8, 3810–3820. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sport. Exercise 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Ridley, K.; Ainsworth, B.; Olds, T. Development of a compendium of energy expenditure for youth. Int. J. Behav. Nutr. Phys. Act. 2008, 5. [Google Scholar] [CrossRef]
- American Academy of Pediatrics: Committee on Public Education. Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Rising trends in BMI of Saudi adolescents: Evidence from three national cross sectional studies. Asia Pac. J. Clin. Nutr. 2007, 16, 462–466. [Google Scholar]
- Shaw, N.J.; Crabtree, N.J.; Kibirige, M.S.; Fordham, J.N. Ethnic and gender differences in body fat in British schoolchildren as measured by DXA. Arch. Dis. Child. 2007, 92, 872–875. [Google Scholar] [CrossRef]
- Lobstein, T.; Baur, L.; Uauy, R.; IASO International Obesity Task Force. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, S4–S104. [Google Scholar]
- Rokholm, B.; Baker, J.L.; Sørensen, T.I. The leveling off of the obesity epidemic since the year 1999—A review of evidence and perspectives. Obes. Rev. 2010, 11, 835–846. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Prevalence and trends in obesity among school boys in central Saudi Arabia between 1988 and 2005. Saudi Med. J. 2007, 28, 1569–1574. [Google Scholar]
- Al-Hazzaa, H. Prevalence of physical inactivity in Saudi Arabia: A brief review. East. Mediterr. Health J. 2004, 10, 663–670. [Google Scholar]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Amin, T.T.; Suleman, W.; Ali, A.; Gamal, A.; al Wehedy, A. Pattern, prevalence, and perceived personal barriers toward physical activity among adult Saudis in Al-Hassa, KSA. J. Phys. Act. Health 2011, 6, 775–784. [Google Scholar]
- Caperchione, C.M.; Kolt, G.S.; Tennent, R.; Mummery, W.K. Physical activity behaviours of Culturally and Linguistically Diverse (CALD) women living in Australia: A qualitative study of socio-cultural influences. BMC Public Health 2011, 11. [Google Scholar] [CrossRef]
- Belcher, B.R.; Berrigan, D.; Dodd, K.W.; Emken, B.A.; Chou, C.P.; Spruijt-Metz, D. Physical activity in US youth: Effect of race/ethnicity, age, gender, and weight status. Med. Sci. Sport. Exercise 2010, 42, 2211–2221. [Google Scholar] [CrossRef]
- Ng, C.; Young, T.K.; Corey, P.N. Associations of television viewing, physical activity and dietary behaviours with obesity in aboriginal and non-aboriginal Canadian youth. Public Health Nutr. 2010, 13, 1430–1437. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sport. Exercise 2000, 32, 963–975. [Google Scholar]
- Sallis, J.F.; Zakarian, J.M.; Hovell, M.F.; Hofstetter, C.R. Ethnic, socioeconomic, and sex differences in physical activity among adolescents. J. Clin. Epidemiol. 1996, 49, 125–134. [Google Scholar] [CrossRef]
- Verloigne, M.; van lippevelde, W.; Maes, L.; Yıldırım, M.; Chinapaw, M.; Manios, Y.; Androutsos, O.; Kovács, E.; Bringolf-Isler, B.; Brug, J.; de Bourdeaudhuij, I. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: An observational study within the ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef]
- Al-Hazzaa, H. School backpack: How much load do Saudi boys carry on their shoulders? Saudi Med. J. 2006, 27, 1567–1571. [Google Scholar]
- Cooper, A.R.; Andersen, L.B.; Wedderkopp, N.; Page, A.S.; Froberg, K. Physical activity levels of children who walk, cycle, or are driven to school. Amer. J. Prev. Med. 2005, 29, 179–184. [Google Scholar] [CrossRef]
- Nilsson, A.; Anderssen, S.A.; Andersen, L.B.; Froberg, K.; Riddoch, C.; Sardinha, L.B.; Ekelund, U. Between- and within-day variability in physical activity and inactivity in 9- and 15-year-old European children. Scand. J. Med. Sci Sport. 2009, 19, 10–18. [Google Scholar]
- de Cocker, K.; Ottevaere, C.; Sjöström, M.; Moreno, L.A.; Wärnberg, J.; Valtueña, J.; Manios, Y.; Dietrich, S.; Mauro, B.; Artero, E.G.; et al. Self-reported physical activity in European adolescents: Results from the HELENA (healthy lifestyle in Europe by nutrition in adolescence) study. Public Health Nutr. 2011, 14, 246–254. [Google Scholar] [CrossRef]
- Rzewnicki, R.; Auweele, Y.; DeBourdeaudhuij, I. Addressing overreporting on the international physical activity quesstionnaire (IPAQ) telephone survey with a population sample. Public Health Nutr. 2003, 6, 299–305. [Google Scholar]
- Loucaides, C.A.; Jago, R.; Theophanous, M. Physical activity and sedentary behaviours in Greek-Cypriot children and adolescents: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2011, 8. [Google Scholar] [CrossRef]
- Tammelin, T.; Ekelund, U.; Remes, J.; Näyhä, S. Physical activity and sedentary behaviors among Finnish youth. Med. Sci. Sport. Exercise 2007, 39, 1067–1074. [Google Scholar] [CrossRef]
- Fulton, J.E.; Wang, X.; Yore, M.M.; Carlson, S.A.; Galuska, D.A.; Caspersen, C.J. Television viewing, computer use, and BMI among U.S. children and adolescents. J. Phys. Act. Health 2009, 6, S28–S35. [Google Scholar]
- Mark, A.E.; Boyce, W.F.; Janssen, I. Television viewing, computer use and total screen time in Canadian youth. Paediat. Child Health 2006, 11, 595–599. [Google Scholar]
- Chinapaw, M.J.; Proper, K.I.; Brug, J.; van Mechelen, W.; Singh, A.S. Relationship between young peoples’ sedentary behaviour and biomedical health indicators: A systematic review of prospective studies. Obes. Rev. 2011, 12, 621–632. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.J. Sedentary behavior and dietary intake in children, adolescents, and adults a systematic review. Amer. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef]
- Mark, A.E.; Janssen, I. Relationship between screen time and metabolic syndrome in adolescents. J. Public Health. 2008, 30, 153–160. [Google Scholar] [CrossRef]
- Taveras, E.M.; Field, A.E.; Berkey, C.S.; Rifas-Shiman, S.L.; Frazier, A.L.; Colditz, G.A.; Gillman, M.W. Longitudinal relationship between television viewing and leisure-time physical activity during adolescence. Pediatrics 2007, 119, 314–319. [Google Scholar] [CrossRef]
- Popkin, B.M. The shift in stages of the nutrition transition in the developing world differs from past experiences. Public Health Nutr. 2002, 5, 205–214. [Google Scholar]
- Vereecken, C.A.; de henauw, S.; Maes, L. Adolescents’ food habits: Results of the Health Behaviour in School-aged Children survey. Br. J. Nutr. 2005, 94, 423–431. [Google Scholar] [CrossRef]
- Samuelson, G. Dietary habits and nutritional status in adolescents over Europe. An overview of current studies in the Nordic countries. Eur. J. Clin. Nutr. 2000, 54, S21–S28. [Google Scholar] [CrossRef]
- Cruz, J.A. Dietary habits and nutritional status in adolescents over Europe—Southern Europe. Eur. J. Clin. Nutr. 2000, 54, S29–S35. [Google Scholar] [CrossRef]
- Rasmussen, M.; Krølner, R.; Klepp, K.I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Al-Hazzaa, H.M.; Al-Nakeeb, Y.; Duncan, M.J.; Al-Sobayel, H.I.; Abahussain, N.A.; Musaiger, A.O.; Lyons, M.; Collins, P.; Nevill, A. A Cross-Cultural Comparison of Health Behaviors between Saudi and British Adolescents Living in Urban Areas: Gender by Country Analyses. Int. J. Environ. Res. Public Health 2013, 10, 6701-6720. https://doi.org/10.3390/ijerph10126701
Al-Hazzaa HM, Al-Nakeeb Y, Duncan MJ, Al-Sobayel HI, Abahussain NA, Musaiger AO, Lyons M, Collins P, Nevill A. A Cross-Cultural Comparison of Health Behaviors between Saudi and British Adolescents Living in Urban Areas: Gender by Country Analyses. International Journal of Environmental Research and Public Health. 2013; 10(12):6701-6720. https://doi.org/10.3390/ijerph10126701
Chicago/Turabian StyleAl-Hazzaa, Hazzaa M., Yahya Al-Nakeeb, Michael J. Duncan, Hana I. Al-Sobayel, Nada A. Abahussain, Abdulrahman O. Musaiger, Mark Lyons, Peter Collins, and Alan Nevill. 2013. "A Cross-Cultural Comparison of Health Behaviors between Saudi and British Adolescents Living in Urban Areas: Gender by Country Analyses" International Journal of Environmental Research and Public Health 10, no. 12: 6701-6720. https://doi.org/10.3390/ijerph10126701
APA StyleAl-Hazzaa, H. M., Al-Nakeeb, Y., Duncan, M. J., Al-Sobayel, H. I., Abahussain, N. A., Musaiger, A. O., Lyons, M., Collins, P., & Nevill, A. (2013). A Cross-Cultural Comparison of Health Behaviors between Saudi and British Adolescents Living in Urban Areas: Gender by Country Analyses. International Journal of Environmental Research and Public Health, 10(12), 6701-6720. https://doi.org/10.3390/ijerph10126701