
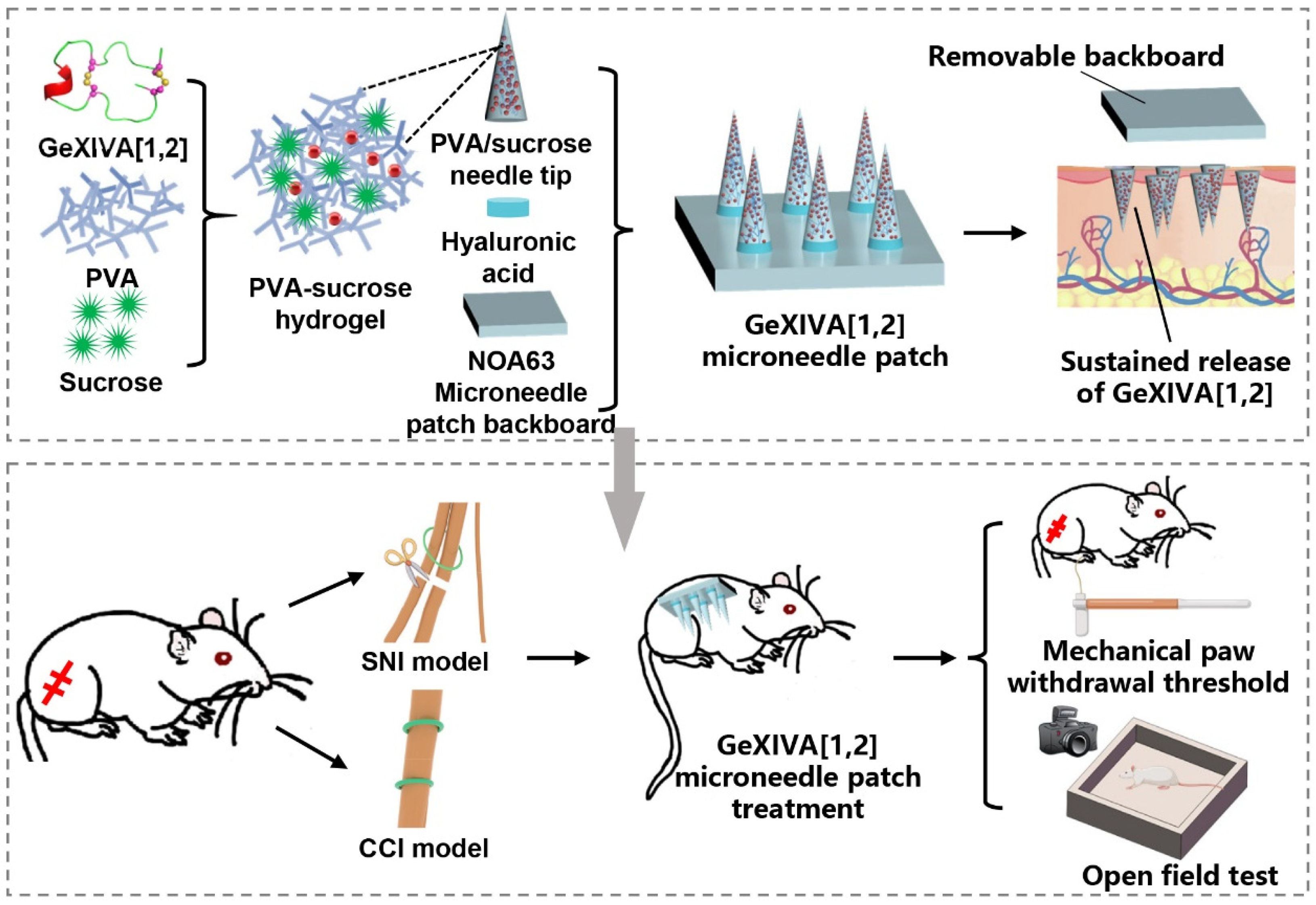
Sustained Release of αO-Conotoxin GeXIVA[1,2] via Hydrogel Microneedle Patch for Chronic Neuropathic Pain Management



Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results
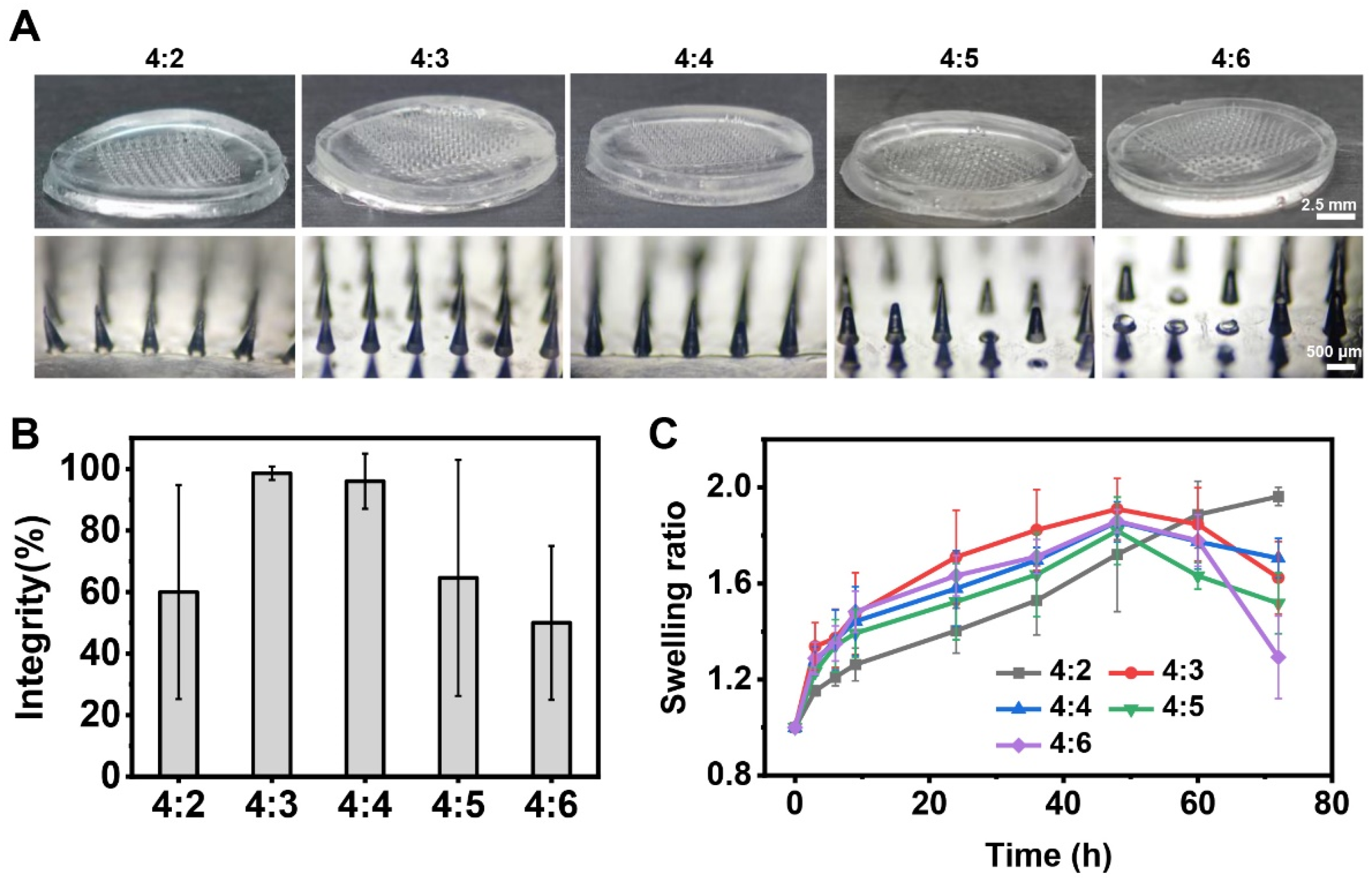
2.1. Optimization of Composition Ratios of Hydrogel Microneedle Patches
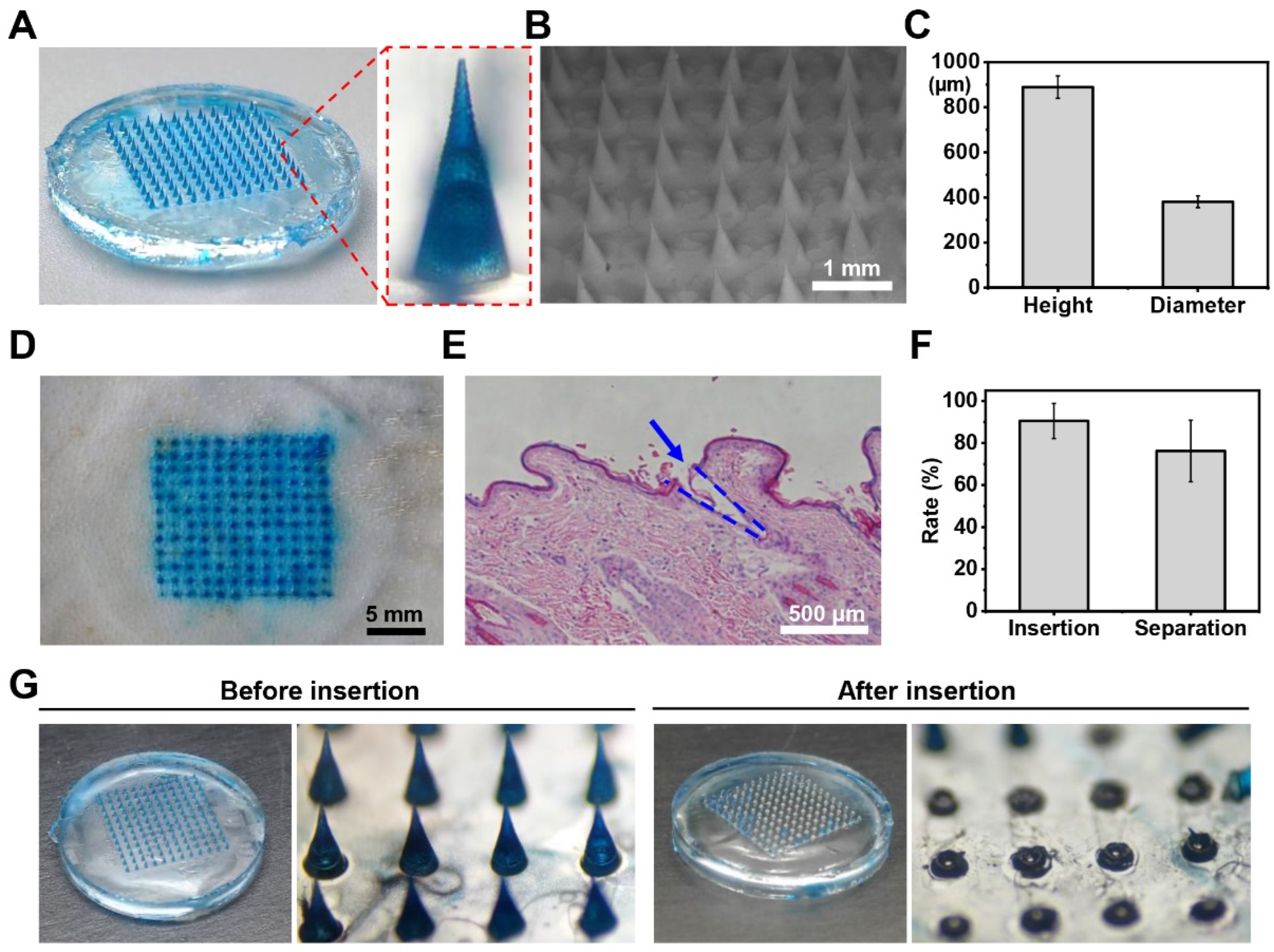
2.2. Fabrication and Characterization of Hydrogel Microneedle Patches
2.3. In Vitro Release of the GeXIVA[1,2] Microneedle Patches
2.4. Evaluation of Drug Release In Vivo
2.5. GeXIVA[1,2] Microneedle Patches for Neuropathic Pain Management
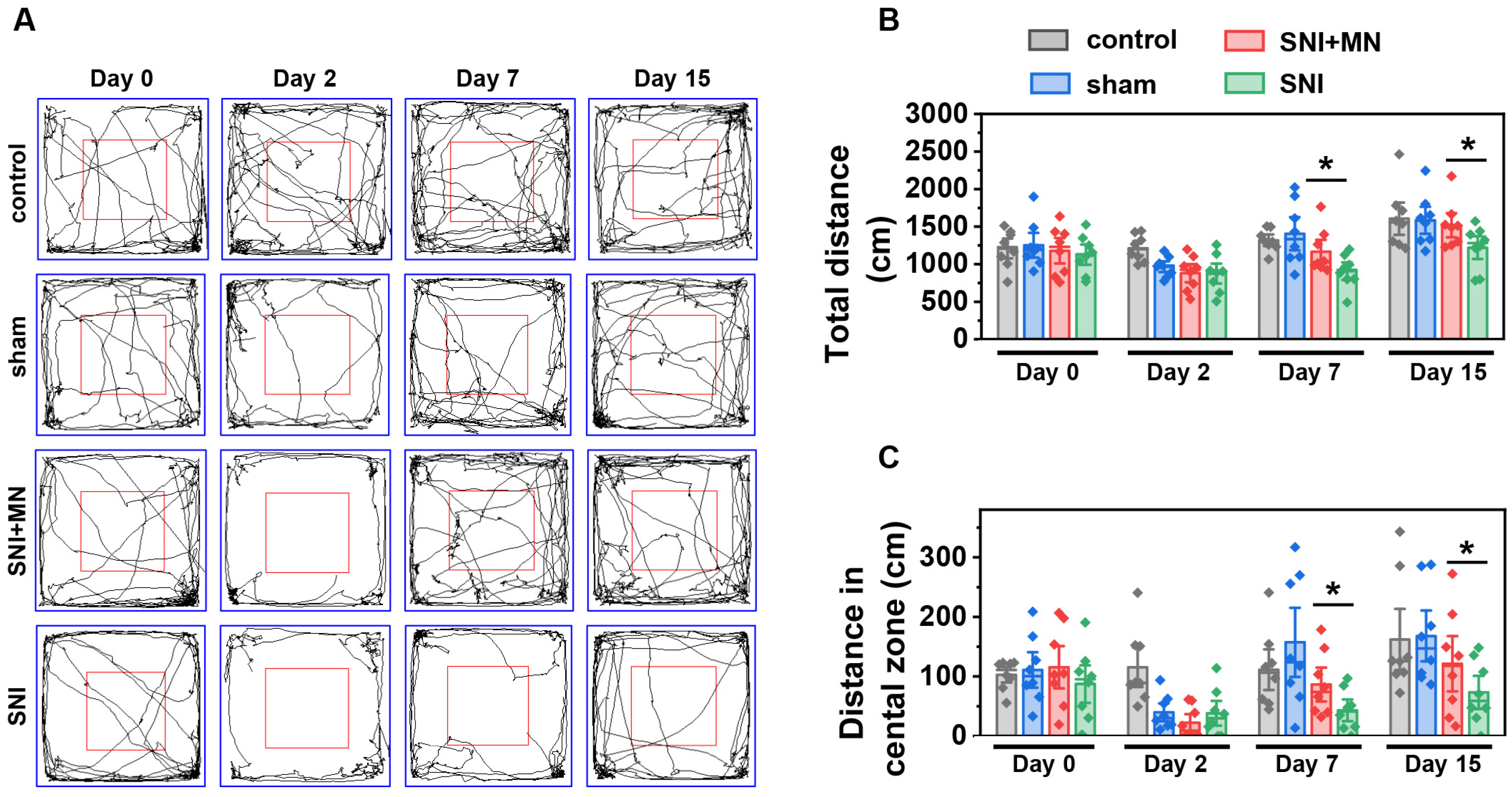
2.6. The Effect of GeXIVA[1,2] Microneedle Patch on Motor Function Recovery
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Fabrication of GeXIVA[1,2] Hydrogel Microneedle Patches
4.3. Exploration of Optimal Ratio of PVA–Sucrose Hydrogel
4.4. Characterizations of GeXIVA[1,2] Microneedle Patch
4.5. In Vitro Release Study of GeXIVA[1,2] from Hydrogel Microneedle Patches
4.6. Drug Release In Vivo
4.7. Mechanical Allodynia Testing
4.8. Animal Chronic Neuropathic Pain Models
4.9. Administration of GeXIVA[1,2] Microneedle Patches
4.10. Open Field Test
4.11. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| nAChR | nicotinic acetylcholine receptor |
| PVA | polyvinyl alcohol |
| NOA63 | Norland optical adhesive 63 |
| HA | hyaluronic acid |
| RP-HPLC | reverse-phase high-performance liquid chromatography |
| ESI-MS | electrospray-ionization mass spectroscopy |
| PBS | phosphate buffer saline |
| SNI | spared nerve injury |
| CCI | chronic constriction injury |
| PWT | paw withdrawal threshold |
| UV | ultraviolet |
| PDMS | polydimethylsiloxane |
| TFA | trifluoroacetic acid |
| SEM | scanning electron microscope |
| H&E | hematoxylin–eosin |
References
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef] [PubMed]
- Glare, P.; Mahendran, M.; Weiss, A.D. Update on chronic pain management. Intern. Med. J. 2025, 55, 200–206. [Google Scholar] [CrossRef]
- Llorca-Torralba, M.; Camarena-Delgado, C.; Suárez-Pereira, I.; Bravo, L.; Mariscal, P.; Garcia-Partida, J.A.; López-Martín, C.; Wei, H.; Pertovaara, A.; Mico, J.A.; et al. Pain and depression comorbidity causes asymmetric plasticity in the locus coeruleus neurons. Brain 2022, 145, 154–167. [Google Scholar] [CrossRef]
- Sun, L.; Liu, R.; Guo, F.; Wen, M.Q.; Ma, X.L.; Li, K.Y.; Sun, H.; Xu, C.L.; Li, Y.Y.; Wu, M.Y.; et al. Parabrachial nucleus circuit governs neuropathic pain-like behavior. Nat. Commun. 2020, 11, 5974. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef] [PubMed]
- Attal, N.; Bouhassira, D.; Colvin, L. Advances and challenges in neuropathic pain: A narrative review and future directions. Br. J. Anaesth. 2023, 131, 79–92. [Google Scholar] [CrossRef]
- Cohen, S.P.; Mao, J. Neuropathic pain: Mechanisms and their clinical implications. BMJ 2014, 348, f7656. [Google Scholar] [CrossRef] [PubMed]
- Varadi, G. Mechanism of Analgesia by Gabapentinoid Drugs: Involvement of Modulation of Synaptogenesis and Trafficking of Glutamate-Gated Ion Channels. J. Pharmacol. Exp. Ther. 2024, 388, 121–133. [Google Scholar] [CrossRef]
- Srivastava, A.B.; Mariani, J.J.; Levin, F.R. New directions in the treatment of opioid withdrawal. Lancet 2020, 395, 1938–1948. [Google Scholar] [CrossRef]
- Fiorotti, H.B.; Figueiredo, S.G.; Campos, F.V.; Pimenta, D.C. Cone snail species off the Brazilian coast and their venoms: A review and update. J. Venom. Anim. Toxins Incl. Trop. Dis. 2023, 29, e20220052. [Google Scholar] [CrossRef]
- Luo, S.; Zhangsun, D.; Harvey, P.J.; Kaas, Q.; Wu, Y.; Zhu, X.; Hu, Y.; Li, X.; Tsetlin, V.I.; Christensen, S.; et al. Cloning, synthesis, and characterization of αO-conotoxin GeXIVA, a potent α9α10 nicotinic acetylcholine receptor antagonist. Proc. Natl. Acad. Sci. USA 2015, 112, E4026–E4035. [Google Scholar] [PubMed]
- Li, Z.; Han, X.; Hong, X.; Li, X.; Gao, J.; Zhang, H.; Zheng, A. Lyophilization Serves as an Effective Strategy for Drug Development of the α9α10 Nicotinic Acetylcholine Receptor Antagonist α-Conotoxin GeXIVA[1,2]. Mar. Drugs 2021, 19, 121. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, X.; Zhangsun, D.; Yu, G.; Su, R.; Luo, S. The α9α10 Nicotinic Acetylcholine Receptor Antagonist αO-Conotoxin GeXIVA[1,2] Alleviates and Reverses Chemotherapy-Induced Neuropathic Pain. Mar. Drugs 2019, 17, 265. [Google Scholar] [CrossRef]
- Wang, H.; Li, X.; Qiao, Y.; Wang, M.; Wang, W.; McIntosh, J.M.; Zhangsun, D.; Luo, S. αO-Conotoxin GeXIVA[1,2] Reduced Neuropathic Pain and Changed Gene Expression in Chronic Oxaliplatin-Induced Neuropathy Mice Model. Mar. Drugs 2024, 22, 49. [Google Scholar] [CrossRef]
- Li, X.; Hu, Y.; Wu, Y.; Huang, Y.; Yu, S.; Ding, Q.; Zhangsun, D.; Luo, S. Anti-hypersensitive effect of intramuscular administration of αO-conotoxin GeXIVA[1,2] and GeXIVA [1,4] in rats of neuropathic pain. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 66, 112–119. [Google Scholar]
- Wang, M.Z.; Li, X.D.; Wang, H.B.; Luo, S.L.; Zhangsun, D.T. Preliminaryevaluating toxicity of αO-conotoxin GeXIVA[1,2] in mice. Toxicon 2019, 158, S80. [Google Scholar]
- Imperial, J.S.; Bansal, P.S.; Alewood, P.F.; Daly, N.L.; Craik, D.J.; Sporning, A.; Terlau, H.; López-Vera, E.; Bandyopadhyay, P.K.; Olivera, B.M. A novel conotoxin inhibitor of Kv1.6 channel and nAChR subtypes defines a new superfamily of conotoxins. Biochemistry 2006, 45, 8331–8340. [Google Scholar] [CrossRef]
- Lin, J.; Chen, S.; Butt, U.D.; Yan, M.; Wu, B. A comprehensive review on ziconotide. Heliyon 2024, 10, e31105. [Google Scholar] [CrossRef]
- McLenon, J.; Rogers, M.A.M. The fear of needles: A systematic review and meta-analysis. J. Adv. Nurs. 2019, 75, 30–42. [Google Scholar]
- Vora, L.K.; Sabri, A.H.; Naser, Y.; Himawan, A.; Hutton, A.R.J.; Anjani, Q.K.; Volpe-Zanutto, F.; Mishra, D.; Li, M.; Rodgers, A.M.; et al. Long-acting microneedle formulations. Adv. Drug Deliv. Rev. 2023, 201, 115055. [Google Scholar]
- Song, K.; Hao, Y.; Tan, X.; Huang, H.; Wang, L.; Zheng, W. Microneedle-mediated delivery of Ziconotide-loaded liposomes fused with exosomes for analgesia. J. Control. Release 2023, 356, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, F.; Teymourian, H.; Wuerstle, B.; Kavner, J.; Patel, R.; Furmidge, A.; Aghavali, R.; Hosseini-Toudeshki, H.; Brown, C.; Zhang, F.; et al. An integrated wearable microneedle array for the continuous monitoring of multiple biomarkers in interstitial fluid. Nat. Biomed. Eng. 2022, 6, 1214–1224. [Google Scholar] [CrossRef]
- Wang, C.; Yang, Y.; Zhang, J.; Zhang, H.; Wang, Q.; Ma, S.; Zhao, P.; Li, Z.; Liu, Y. Microneedles at the Forefront of Next Generation Theranostics. Adv. Sci. 2025, e2412140. [Google Scholar] [CrossRef] [PubMed]
- He, R.; Liu, H.; Fang, T.; Niu, Y.; Zhang, H.; Han, F.; Gao, B.; Li, F.; Xu, F. A Colorimetric Dermal Tattoo Biosensor Fabricated by Microneedle Patch for Multiplexed Detection of Health-Related Biomarkers. Adv. Sci. 2021, 8, e2103030. [Google Scholar] [CrossRef]
- He, R.; Niu, Y.; Li, Z.; Li, A.; Yang, H.; Xu, F.; Li, F. A Hydrogel Microneedle Patch for Point-of-Care Testing Based on Skin Interstitial Fluid. Adv. Healthc. Mater. 2020, 9, e1901201. [Google Scholar] [CrossRef]
- Ghosh, S.; Kumar, N.; Chattopadhyay, S. Electrically conductive “SMART” hydrogels for on-demand drug delivery. Asian J. Pharm. Sci. 2025, 20, 101007. [Google Scholar] [CrossRef]
- Zhong, Y.; Lin, Q.; Yu, H.; Shao, L.; Cui, X.; Pang, Q.; Zhu, Y.; Hou, R. Construction methods and biomedical applications of PVA-based hydrogels. Front. Chem. 2024, 12, 1376799. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Sasaki, S. Swelling and mechanical properties of physically crosslinked poly(vinyl alcohol) hydrogels. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2015, 229, 828–844. [Google Scholar] [CrossRef]
- Zhao, J.; Li, Y.; Wang, M. Fabrication of robust transparent hydrogel with stretchable, self-healing, easily recyclable and adhesive properties and its application. Mater. Res. Bull. 2019, 112, 292–296. [Google Scholar] [CrossRef]
- Oltulu, P.; Ince, B.; Kokbudak, N.; Findik, S.; Kilinc, F. Measurement of epidermis, dermis, and total skin thicknesses from six different body regions with a new ethical histometric technique. Turk. J. Plast. Surg. 2018, 26, 56–61. [Google Scholar]
- Beebe, J.A.; Kronman, C.; Mahmud, F.; Basch, M.; Hogan, M.; Li, E.; Ploski, C.; Simons, L.E. Gait Variability and Relationships With Fear, Avoidance, and Pain in Adolescents With Chronic Pain. Phys. Ther. 2021, 101, pzab012. [Google Scholar] [PubMed]
- Ganguly, A.; McEwen, C.; Troy, E.L.; Colburn, R.W.; Caggiano, A.O.; Schallert, T.J.; Parry, T.J. Recovery of sensorimotor function following sciatic nerve injury across multiple rat strains. J. Neurosci. Methods 2017, 275, 25–32. [Google Scholar] [PubMed]
- Yu, S.; Wu, Y.; Xu, P.; Wang, S.; Zhangsun, D.; Luo, S. Effects of serum, enzyme, thiol, and forced degradation on the stabilities of αO-Conotoxin GeXIVA[1,2] and GeXIVA [1,4]. Chem. Biol. Drug Des. 2018, 91, 1030–1041. [Google Scholar]
- Pei, S.; Wang, N.; Mei, Z.; Zhangsun, D.; Craik, D.J.; McIntosh, J.M.; Zhu, X.; Luo, S. Conotoxins Targeting Voltage-Gated Sodium Ion Channels. Pharmacol. Rev. 2024, 76, 828–845. [Google Scholar] [CrossRef] [PubMed]
- Tietze, A.A.; Tietze, D.; Ohlenschläger, O.; Leipold, E.; Ullrich, F.; Kühl, T.; Mischo, A.; Buntkowsky, G.; Görlach, M.; Heinemann, S.H.; et al. Structurally diverse μ-conotoxin PIIIA isomers block sodium channel NaV 1.4. Angew. Chem.-Int. Ed. 2012, 51, 4058–4061. [Google Scholar]
- Tran, H.N.T.; McMahon, K.L.; Deuis, J.R.; Vetter, I.; Schroeder, C.I. Structural and functional insights into the inhibition of human voltage-gated sodium channels by μ-conotoxin KIIIA disulfide isomers. J. Biol. Chem. 2022, 298, 101728. [Google Scholar]
- Vetter, I.; Dekan, Z.; Knapp, O.; Adams, D.J.; Alewood, P.F.; Lewis, R.J. Isolation, characterization and total regioselective synthesis of the novel μO-conotoxin MfVIA from Conus magnificus that targets voltage-gated sodium channels. Biochem. Pharmacol. 2012, 84, 540–548. [Google Scholar]
- Wang, S.; Zhu, X.; Zhangsun, M.; Wu, Y.; Yu, J.; Harvey, P.J.; Kaas, Q.; Zhangsun, D.; Craik, D.J.; Luo, S. Engineered Conotoxin Differentially Blocks and Discriminates Rat and Human α7 Nicotinic Acetylcholine Receptors. J. Med. Chem. 2021, 64, 5620–5631. [Google Scholar]
- Li, L.; Li, Z.; Guo, Y.; Zhang, K.; Mi, W.; Liu, J. Preparation of uniform-sized GeXIVA[1,2]-loaded PLGA microspheres as long-effective release system with high encapsulation efficiency. Drug Deliv. 2022, 29, 2283–2295. [Google Scholar] [CrossRef]
- Dixon, W.J. Efficient analysis of experimental observations. Annu. Rev. Pharmacol. Toxicol. 1980, 20, 441–462. [Google Scholar]
- Richner, M.; Bjerrum, O.J.; Nykjaer, A.; Vaegter, C.B. The spared nerve injury (SNI) model of induced mechanical allodynia in mice. J. Vis. Exp. 2011, 54, 3092. [Google Scholar]
- Bennett, G.J.; Xie, Y.K. A peripheral mononeuropathy in rat that produces disorders of pain sensation like those seen in man. Pain 1988, 33, 87–107. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, R.; Li, M.; Li, W.; Li, W.; Xiao, S.; Cao, Q.; Wang, H.; Zhangsun, D.; Luo, S. Sustained Release of αO-Conotoxin GeXIVA[1,2] via Hydrogel Microneedle Patch for Chronic Neuropathic Pain Management. Mar. Drugs 2025, 23, 161. https://doi.org/10.3390/md23040161
He R, Li M, Li W, Li W, Xiao S, Cao Q, Wang H, Zhangsun D, Luo S. Sustained Release of αO-Conotoxin GeXIVA[1,2] via Hydrogel Microneedle Patch for Chronic Neuropathic Pain Management. Marine Drugs. 2025; 23(4):161. https://doi.org/10.3390/md23040161
Chicago/Turabian StyleHe, Rongyan, Mingjuan Li, Weitao Li, Wenqi Li, Shuting Xiao, Qiuyu Cao, Huanbai Wang, Dongting Zhangsun, and Sulan Luo. 2025. "Sustained Release of αO-Conotoxin GeXIVA[1,2] via Hydrogel Microneedle Patch for Chronic Neuropathic Pain Management" Marine Drugs 23, no. 4: 161. https://doi.org/10.3390/md23040161
APA StyleHe, R., Li, M., Li, W., Li, W., Xiao, S., Cao, Q., Wang, H., Zhangsun, D., & Luo, S. (2025). Sustained Release of αO-Conotoxin GeXIVA[1,2] via Hydrogel Microneedle Patch for Chronic Neuropathic Pain Management. Marine Drugs, 23(4), 161. https://doi.org/10.3390/md23040161