Low Molecular Weight Chitosan-Insulin Complexes Solubilized in a Mixture of Self-Assembled Labrosol and Plurol Oleaque and Their Glucose Reduction Activity in Rats

Abstract
1. Introduction
2. Results and Discussion
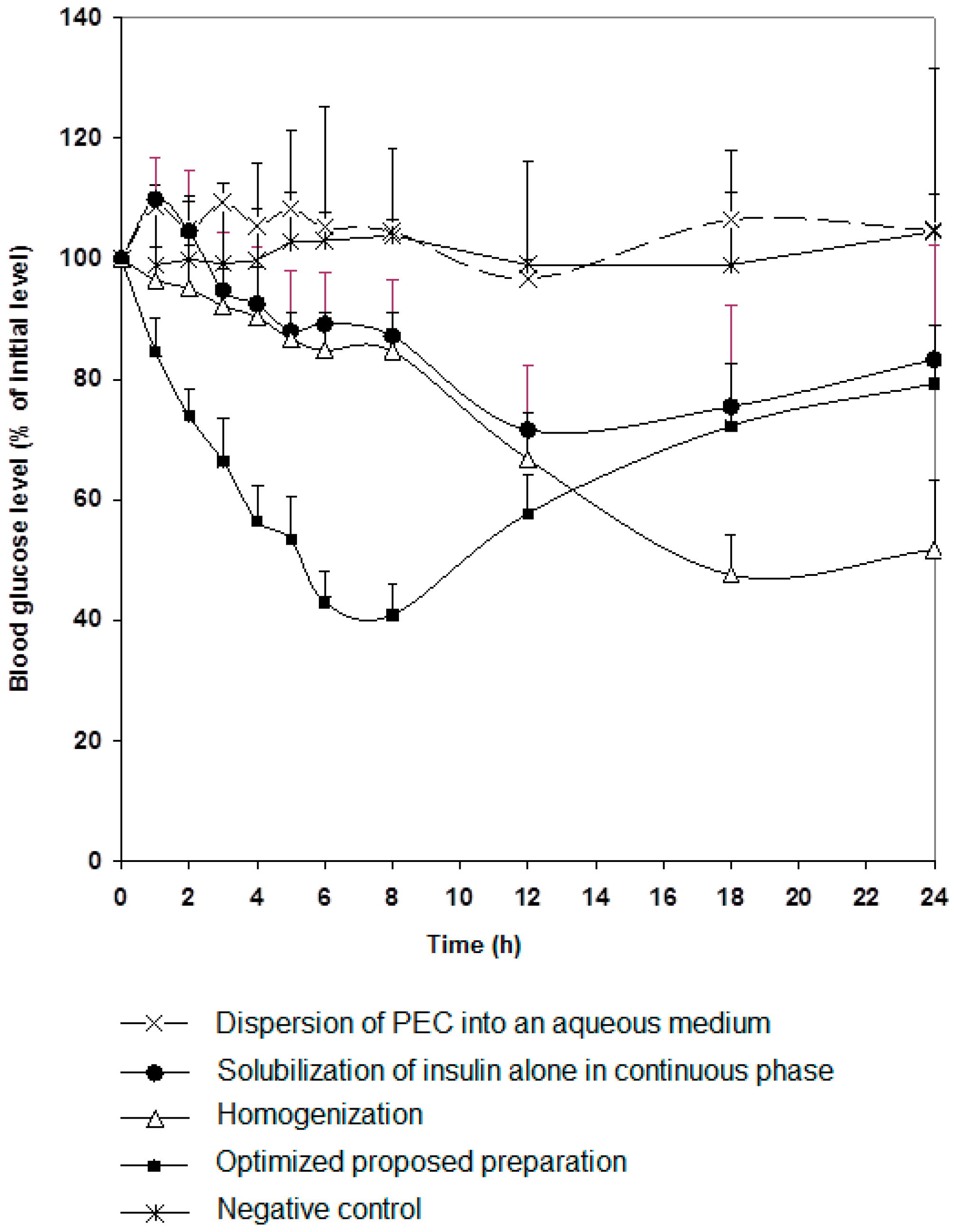
2.1. Formulation and Characterization of Nanoparticles
2.2. Measurement of the Protection Ability of Our Formula against Simulated Gastric and Intestinal Conditions In Vitro
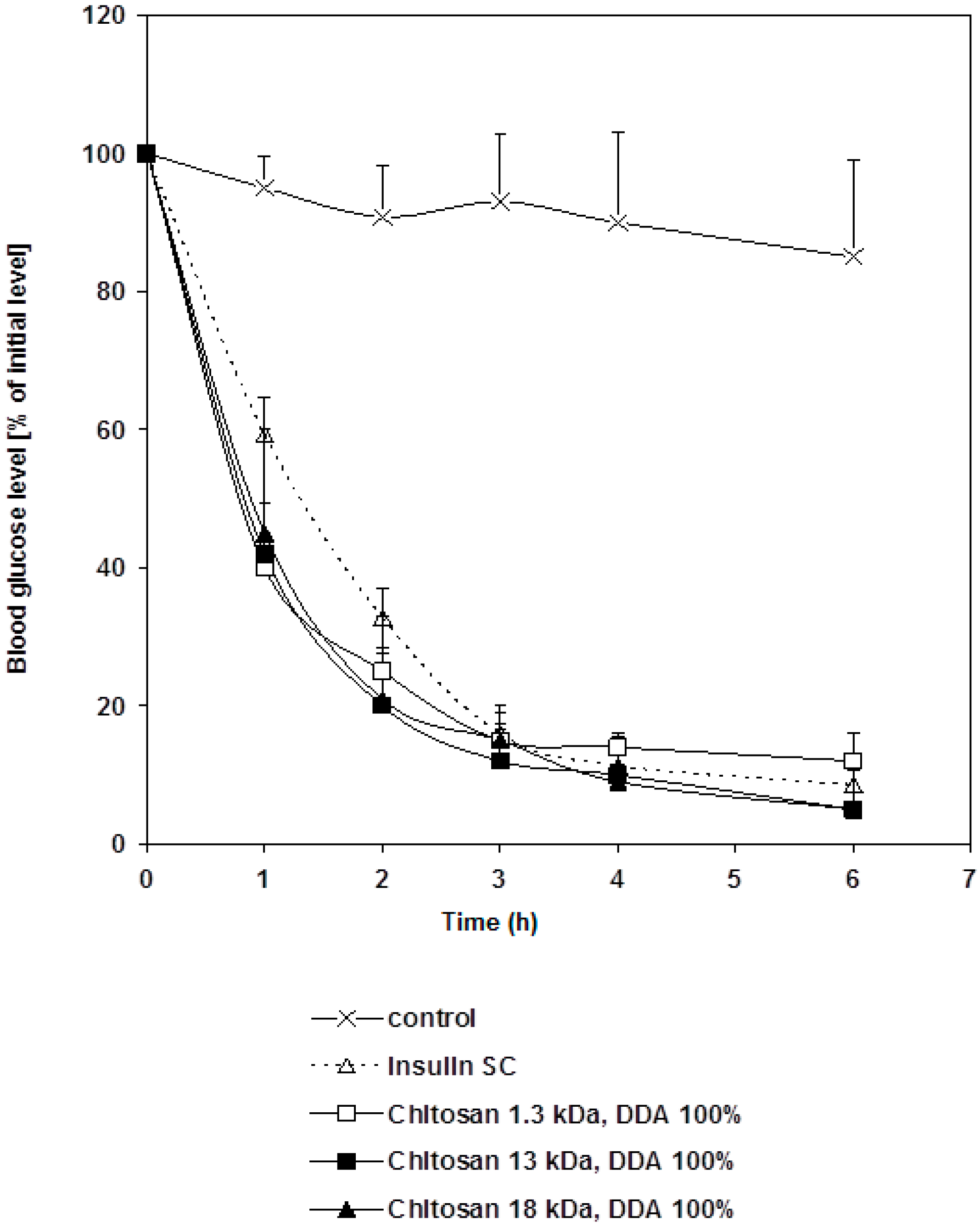
2.3. Pharmacological Activity of Chitosan-Insulin Complex Given Subcutaneously to Diabetic Rats
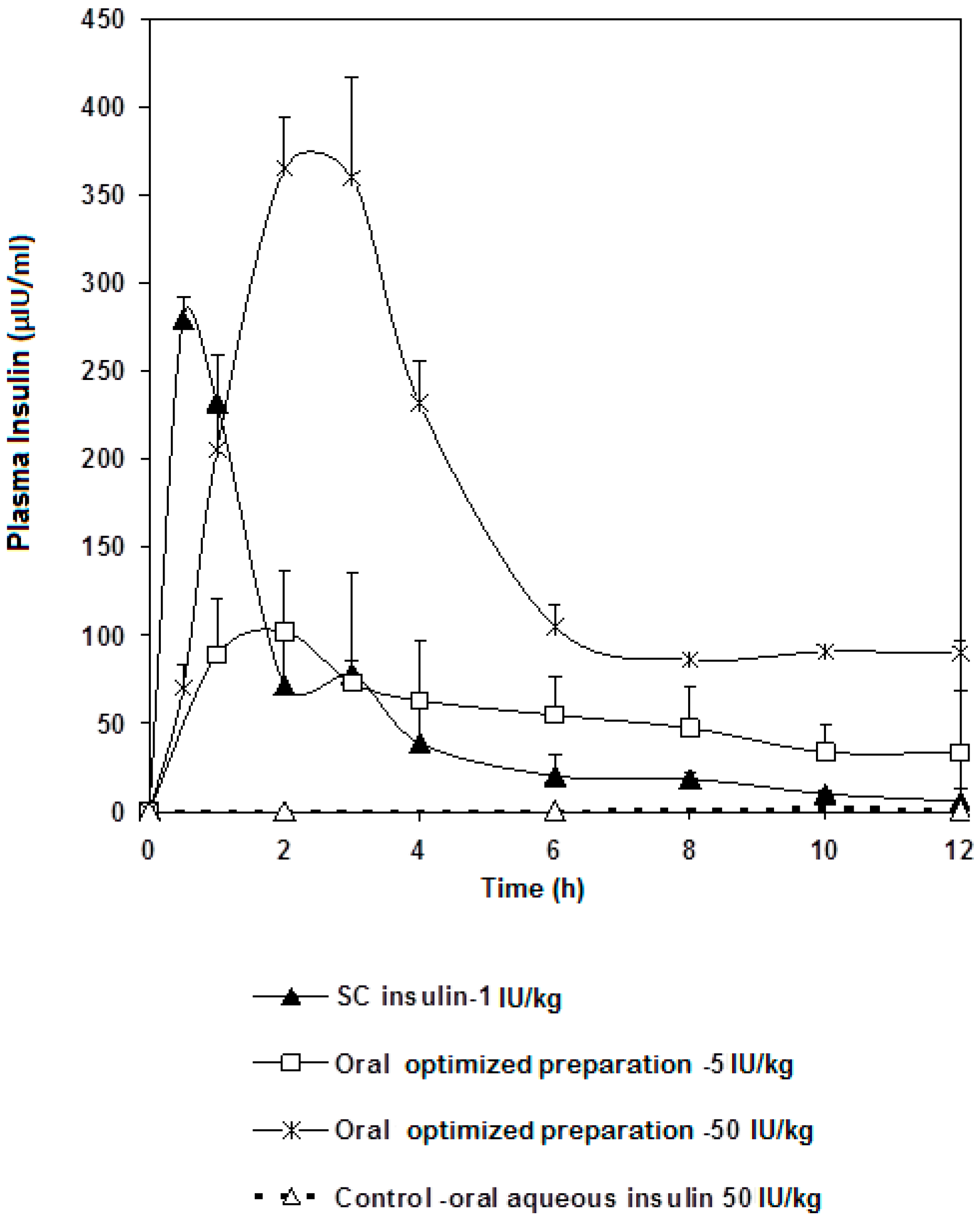
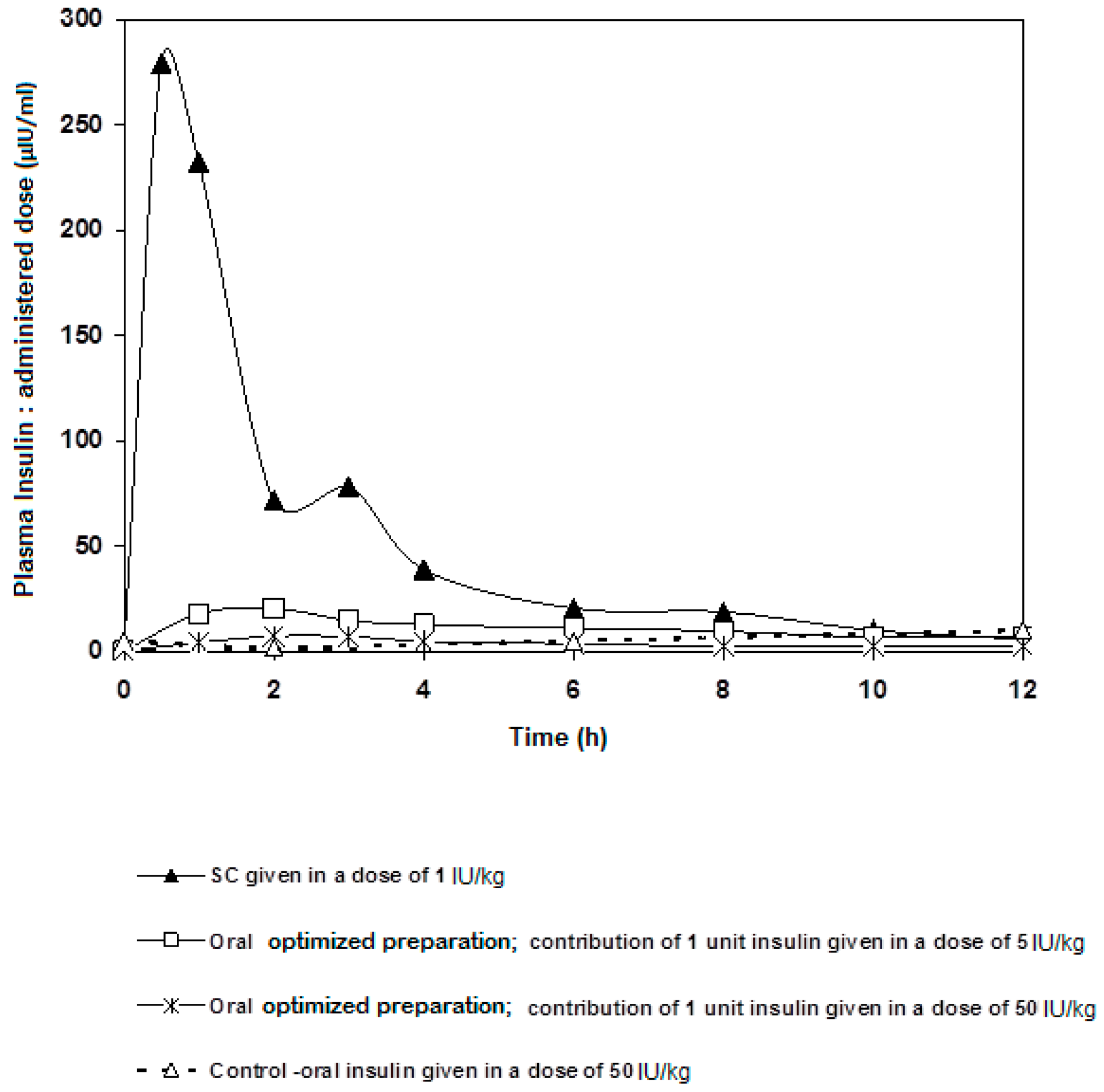
2.4. Bioavailability of Insulin-Loaded Nanoparticles
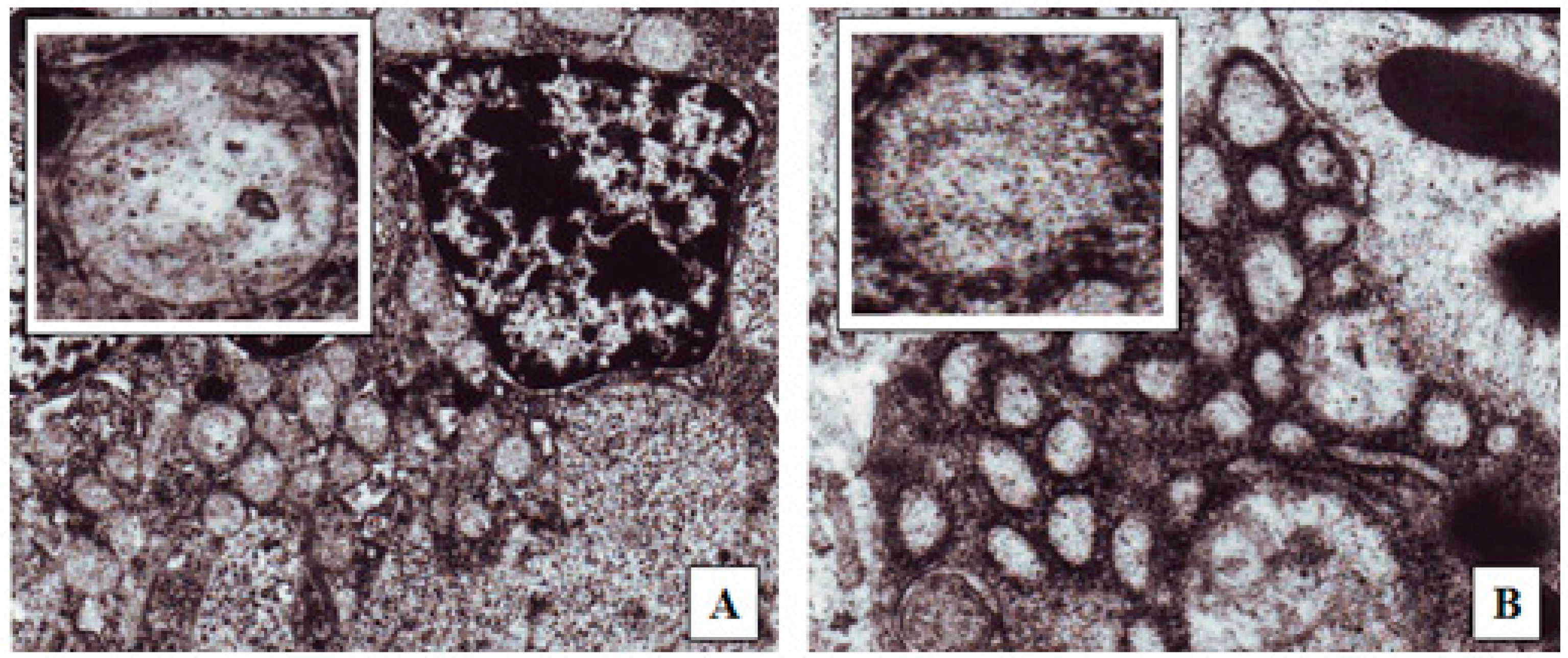
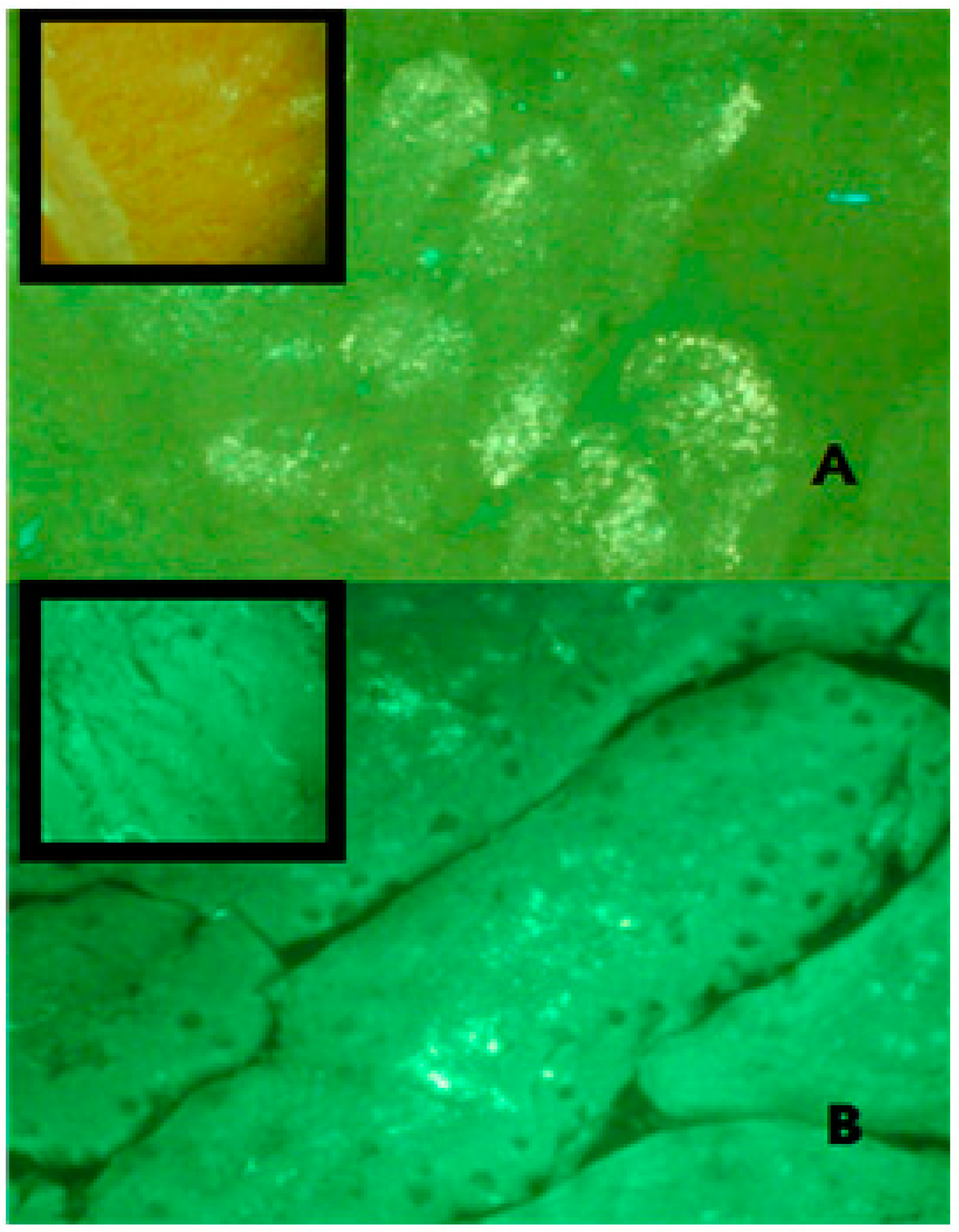
2.5. Overview of the Mechanism of Absorption
3. Materials and Methods
3.1. Materials
3.2. Methods
3.2.1. Chitosan Depolymerization and Deacetylation
Preparation of the Oral Insulin Nanoparticle System
3.2.2. Characterization of Insulin Preparations
3.2.3. Insulin Content
3.2.4. Particle Size Analysis
3.2.5. In Vitro Evaluation of Protection against Simulated Gastric Fluid (SGF) and Simulated Intestinal Fluid (SIF) of the Nano Formulation
3.2.6. Procedure for Animal Preparation
3.2.7. Comparison of Glucose Reduction by Insulin and Chitosan-Insulin Complex Injected Subcutaneously
3.2.8. Comparison of Different Oral Preparations
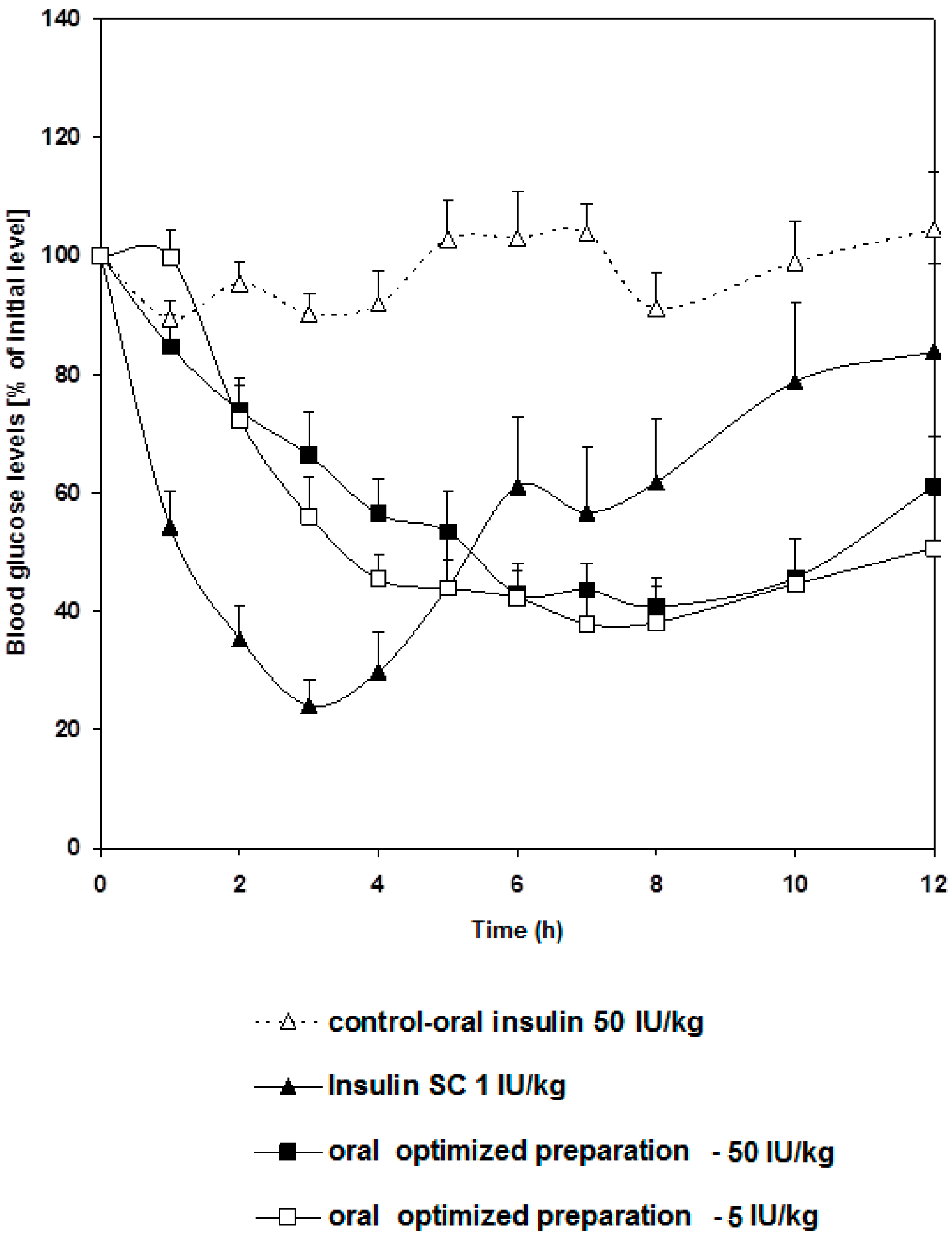
3.2.9. Comparison of the Effect of 5 and 50 IU/kg Doses Administered Orally
3.2.10. Monitoring Insulin Levels in Rats Following Oral Administration of 5 and 50 IU/kg
3.2.11. Pharmacokinetics and Relative Bioavailability Treatment
3.2.12. Statistical Analysis
3.2.13. Mechanism of Intestinal Absorption
Fluorescent Microscopy
Transmission Electron Microscopy (TEM)
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Myers, M.G.; White, M.F. The molecular basis of insulin action. In Insulin Signaling from Cultured Cells to Animal Models; Grunberger, G., Zick, Y., Eds.; Taylor & Frances, Inc.: New York, NY, USA, 2002; pp. 58–87. [Google Scholar]
- Vikas, A.; Mansoor, K.A. Current status of the oral delivery of insulin. Pharm. Technol. 2011, 25, 76–90. [Google Scholar]
- Heinemann, L. New ways of insulin delivery. Int. J. Clin. Pract. 2010, 64, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, G.; Einstein, A. Delivery of insulin to the buccal mucosa utilizing the RapidMist™ system. Expert Opin. Drug Deliv. 2008, 5, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Lalej-Bennis, D.; Boillot, J.; Bardin, C.; Zirinis, P.; Coste, A.; Escudier, E.; Chast, F.; Peynegre, R.; Slama, G.; Selam, J.L. Six-month administration of gelified intranasal insulin in type 1 diabetic patients under multiple injections: Efficacy versus subcutaneous injections and local tolerance. Diabetes Metab. 2001, 27, 372–377. [Google Scholar] [PubMed]
- Caldwell, L.; Nishihata, T.; Fix, J.; Cargell, R.; Cargill, C.; Higuchi, T. Absorption promoting adjuvants: Animal Studies on their Effects on Rectal Drug Absorption. In Proceeding of the Symposium on the Advantages and Problems Encountered in Rectal Therapy; Glas, B., Blaey, C., Eds.; J.R. Prous: Barcelona, Spain, 1984; Volume 7, pp. 57–61. [Google Scholar]
- Lee, E.; Lee, J.; Jon, S. A Novel Approach to Oral Delivery of Insulin by Conjugating with Low Molecular Weight Chitosan. Bioconjug. Chem. 2010, 21, 1720–1723. [Google Scholar] [CrossRef] [PubMed]
- Kapitza, C.; Zijlstra, E.; Heinemann, L.; Castelli, M.; Riley, G.; Heise, T. Oral insulin: A comparison with subcutaneous regular human insulin in patients with Type 2 diabetes. Diabetes Care 2009, 33, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Marais, E.; Hamman, J.; Plessis, L.D.; Lemmer, R.; Steenekamp, J. Eudragit® L100/N-trimethylchitosan chloride microspheres for oral insulin delivery. Molecules 2013, 7, 6734–6747. [Google Scholar] [CrossRef] [PubMed]
- Al-Remawi, M.; Elsayed, A.M.; Maghrabi, I.; Hamaidi, M.; Jaber, N. Chitosan/lecithin liposomal nanovesicles as an oral insulin delivery system. Pharm. Dev. Technol. 2017, 22, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Wilson, K.; van der Walle, C.F.; Sattar, N.; Petrie, J.R.; Ravi, M.N. Microemulsions for oral delivery of insulin: Design, development and evaluation in streptozotocin induced diabetic rats. Eur. J. Pharm. Biopharm. 2010, 76, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, A.; Al-Remawi, M.; Qinna, N.; Farouk, A.; Al-Sou’od, K.; Badwan, A. Chitosan–Sodium Lauryl Sulfate Nanoparticles as a carrier system for the in vivo delivery of oral insulin. AAPS PharmSciTech 2010, 12, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.; Dorkoosh, F.; Avadi, M.; Saadat, P.; Rafiee-Tehrani, M.; Junginger, H.E. Preparation, characterization and antibacterial activities of chitosan, Ntrimethyl chitosan (TMC) and N-diethylmethyl chitosan (DEMC) nanoparticles loaded with insulin using both the ionotropic gelation and polyelectrolyte complexation methods. Int. J. Pharm. 2008, 355, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, A.; Al-Remawi, M.; Qinna, N.; Farouk, A.; Badwan, A. Formulation and characterization of an oily-based system for oral delivery of insulin. Eur. J. Pharm. Biopharm. 2009, 73, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Assaf, S.; Al-Jbour, N.; Eftaiha, A.; Elsayed, A.; Al-Remawi, M.; Qinna, N.; Chowdhry, B.; Leharne, S.; Badwan, A. Factors involved in formulation of oily delivery system for proteins based on PEG-8 caprylic/capric glycerides and polyglyceryl-6 dioleate in a mixture of oleic acid with chitosan. J. Disper. Sci. Technol. 2011, 32, 623–633. [Google Scholar] [CrossRef]
- Qinna, N.A.; Karwi, Q.G.; Al-Jbour, N.; Al-Remawi, M.A.; Alhussainy, T.M.; Al-So’ud, K.A. Influence of molecular weight and degree of deacetylation of low molecular weight chitosan on the bioactivity of oral insulin preparations. Mar. Drugs 2015, 13, 1710–1725. [Google Scholar] [CrossRef] [PubMed]
- Badwan, A.; Remawi, M.; Qinna, N.; Elsayed, A.; Arafat, T.; Melhim, M.; Hijleh, O.; Idkaidek, N. Enhancement of oral bioavailability of insulin in humans. Neuro Endocrinol. Lett. 2009, 30, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Demarger-Andre, S.; Domard, A. Chitosan behaviours in a dispersion of undecylenic acid. Carbohydr. Polym. 1993, 22, 117–126. [Google Scholar] [CrossRef]
- Hargreaves, W.; Deamer, D. Liposomes from ionic, single-chain amphiphiles. Biochemistry 1978, 17, 3759–3767. [Google Scholar] [CrossRef] [PubMed]
- Cistola, D.; Hamilton, J.; Jackson, D.; Small, D. Ionization and phase behavior of fatty acids in water: Application of the Gibbs phase rule. Biochemistry 1988, 27, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Walde, P.; Wick, R.; Fresta, M.; Mangone, A.; Luisi, P. Autopoietic self-reproduction of fatty acid vesicles. J. Am. Chem. Soc. 1994, 116, 11649–11654. [Google Scholar] [CrossRef]
- Fukuda, H.; Goto, A.; Yoshioka, H.; Goto, R.; Morigaki, K.; Walde, P. Electron spin resonance study of the pH-Induced transformation of micelles to vesicles in an aqueous oleic acid/oleate system. Langmuir 2001, 17, 4223–4231. [Google Scholar] [CrossRef]
- Morishita, M.; Goto, T.; Nakamura, K.; Lowman, A.; Takayama, K.; Peppas, N. Novel oral insulin delivery systems based on complexation polymer hydrogels: Single and multiple administration studies in type 1 and 2 diabetic rats. J. Control. Release 2006, 110, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, Y.; Yamamoto, H.; Takeuchi, H.; Kuno, Y. Mucoadhesive DL-Lactide/Glycolide copolymer nanospheres coated with chitosan to improve oral delivery of elcatonin. Pharm. Dev. Technol. 2000, 5, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Yamamoto, H.; Niwa, T.; Hino, T.; Kawashima, Y. Enteral absorption of insulin in rats from mucoadhesive chitosan-coated liposomes. Pharm. Res. 1996, 13, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Morishita, M.; Kajita, M.; Suzuki, A.; Takayama, K.; Chiba, Y.; Tokiwa, S.; Nagai, T. The dose-related hypoglycemic effects of insulin emulsions incorporating highly purified EPA and DHA. Int. J. Pharm. 2000, 201, 175–185. [Google Scholar] [CrossRef]
- Xiong, X.Y.; Li, Y.P.; Li, Z.L.; Zhou, C.L.; Tam, K.C.; Liu, Z.Y.; Xie, G.X. Vesicles from Pluronic/poly (lactic acid) block copolymers as new carriers for oral insulin delivery. J. Control. Release 2007, 120, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Mondon, C.E.; Olfsky, J.M.; Dolkas, C.B.; Reaven, G.M. Removal of insulin by perfused rat liver: Effect of concentration. Metabolism 1975, 24, 153–160. [Google Scholar] [CrossRef]
- Qinna, N.A.; Badwan, A.A. Impact of streptozotocin on altering normal glucose homeostasis during insulin testing in diabetic rats compared to normoglycemic rats. Drug Des. Dev. Ther. 2015, 9, 2515–2525. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, J.; Yang, K. Enhanced modelling of the glucose–insulin system and its applications in insulin therapies. J. Biol. Dyn. 2009, 3, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Des, R.A.; Fievez, V.; Garinot, M.; Schneider, Y.J.; Preat, V. Nanoparticles as potential oral delivery systems of proteins and vaccines: A mechanistic approach. J. Control. Release 2006, 116, 1–27. [Google Scholar]
- Jani, P.; Halbert, G.W.; Langridge, J.; Florence, A.T. Nanoparticle uptake by the rat gastrointestinal mucosa: Quantitation and particle size dependency. J. Pharm. Pharmacol. 1990, 42, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Jani, P.; Halbert, G.W.; Langridge, J.A.; Florence, T. The uptake and translocation of latex nanospheres and microspheres after oral administration to rats. J. Pharm. Pharmacol. 1989, 41, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Conner, S.D.; Schmid, S.L. Regulated portals of entry into the cell. Nature 2003, 422, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Neutra, M.R.; Phillips, T.L.; Mayer, E.L.; Fishkind, D.J. Transport of membrane-bound macromolecules by M cells in follicle-associated epithelium of rabbit Peyer’s patch. Cell Tissue Res. 1987, 247, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Lim, L.Y. Uptake of chitosan and associated insulin in Caco-2 cell monolayers: A Comparison between chitosan molecules and chitosan nanoparticles. Pharm. Res. 2003, 20, 1812–1818. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Zhang, Z.; Sun, X.; Zuo, J.; Zhao, D.; Gong, T. Mechanisms of phospholipid complex loaded nanoparticles enhancing the oral bioavailability. Mol. Pharm. 2010, 7, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Gianninna, T.; Steinetz, B.G.; Melia, A. Pathway of absorption of orally administered ethynyl esradiol-3-cyclopenyl ether in the rat as influenced by vehicle of administration. Proc. Soc. Exp. Biol. Med. 1966, 121, 1175–1179. [Google Scholar] [CrossRef]
- Al-Souod, K.; Abu-Falaha, R.; Al-Remawi, M. Surface Activity of Some Low Molecular Weight Chitosan Derivatives. Jordan J. Chem. 2013, 8, 1–17. [Google Scholar] [CrossRef]
- Cilek, A.; Celebi, N.; Tirnaksiz, F.; Tay, A. A lecithin-based microemulsion of insulin with aprotinin for oral administration: Investigation of hypoglycemic effects in non-diabetic and STZ-induced diabetic rats. Int. J. Pharm. 2005, 298, 176–185. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Modifications | Mean Diameter (nm) ± SD | Assay of Insulin * ± SD |
|---|---|---|
| Dispersion of PEC into an aqueous medium | 8 ± 0.4 | 100 ± 5% |
| Solubilization of insulin alone in continuous phase | 685 ± 16 | 100 ± 5% |
| Homogenization | 2040 ± 63 | 101 ± 5% |
| Optimized proposed preparation | 200 ± 12 | 100 ± 4% |
| Negative control | 108 ± 9 | 99 ± 2% |
| Preparation | Percent Insulin Recovery ± SD |
|---|---|
| 1.3 kDa MWt, 99% DDA | 66.3 ± 0.44 |
| 1.3 kDa MWt, 80% DDA | 77.99 ± 9.41 |
| 1.3 kDa MWt, 55% DDA | 27.2 ± 1.6 |
| 13 kDa MWt, 99% DDA | 86.83 ± 3.98 |
| 18 kDa MWt, 99% DDA | 78.08 ± 2.2 |
| Incubation Media | Percent Insulin Recovery ± SD |
|---|---|
| SGF | 86.83 ± 3.98 |
| SIF | 73.9 ± 0.2 |
| SGF followed by SIF | 58 ± 0.75 |
| Preparation | Cmax (µg/mL) | Tmax (h) | AUC0–12 (µIU.h/mL) | F % |
|---|---|---|---|---|
| S.C injection (1 IU/kg) | 279.20 | 0.5 | 665.60 | |
| Oral preparation (5 IU/kg) | 102.22 | 2 | 968.15 | 29.09 |
| Oral preparation (50 IU/kg) | 356.20 | 2 | 2130.95 | 6.40 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsayed, A.M.; Khaled, A.H.; Al Remawi, M.M.; Qinna, N.A.; Abu Farsakh, H.; Badwan, A.A. Low Molecular Weight Chitosan-Insulin Complexes Solubilized in a Mixture of Self-Assembled Labrosol and Plurol Oleaque and Their Glucose Reduction Activity in Rats. Mar. Drugs 2018, 16, 32. https://doi.org/10.3390/md16010032
Elsayed AM, Khaled AH, Al Remawi MM, Qinna NA, Abu Farsakh H, Badwan AA. Low Molecular Weight Chitosan-Insulin Complexes Solubilized in a Mixture of Self-Assembled Labrosol and Plurol Oleaque and Their Glucose Reduction Activity in Rats. Marine Drugs. 2018; 16(1):32. https://doi.org/10.3390/md16010032
Chicago/Turabian StyleElsayed, Amani M., Aseel H. Khaled, Mayyas M. Al Remawi, Nidal A. Qinna, Hussam Abu Farsakh, and Adnan A. Badwan. 2018. "Low Molecular Weight Chitosan-Insulin Complexes Solubilized in a Mixture of Self-Assembled Labrosol and Plurol Oleaque and Their Glucose Reduction Activity in Rats" Marine Drugs 16, no. 1: 32. https://doi.org/10.3390/md16010032
APA StyleElsayed, A. M., Khaled, A. H., Al Remawi, M. M., Qinna, N. A., Abu Farsakh, H., & Badwan, A. A. (2018). Low Molecular Weight Chitosan-Insulin Complexes Solubilized in a Mixture of Self-Assembled Labrosol and Plurol Oleaque and Their Glucose Reduction Activity in Rats. Marine Drugs, 16(1), 32. https://doi.org/10.3390/md16010032