
Predictive Value of Heart Rate Variability for Postoperative Atrial Fibrillation in Off-Pump Coronary Artery Bypass Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Enrollment Criteria
2.2. Arrhythmia Surveillance
2.3. ECG Measurement Protocol
2.4. HRV Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrmann, F.E.M.; Taha, A.; Nielsen, S.J.; Martinsson, A.; Hansson, E.C.; Juchem, G.; Jeppsson, A. Recurrence of Atrial Fibrillation in Patients with New-Onset Postoperative Atrial Fibrillation After Coronary Artery Bypass Grafting. JAMA Netw. Open 2024, 7, e241537. [Google Scholar] [CrossRef]
- Benedetto, U.; Gaudino, M.F.; Dimagli, A.; Gerry, S.; Gray, A.; Lees, B.; Flather, M.; Taggart, D.P. Postoperative Atrial Fibrillation and Long-Term Risk of Stroke After Isolated Coronary Artery Bypass Graft Surgery. Circulation 2020, 142, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.; Nielsen, S.J.; Bergfeldt, L.; Ahlsson, A.; Friberg, L.; Bjorck, S.; Franzén, S.; Jeppsson, A. New-Onset Atrial Fibrillation After Coronary Artery Bypass Grafting and Long-Term Outcome: A Population-Based Nationwide Study from the SWEDEHEART Registry. J. Am. Heart Assoc. 2021, 10, e017966. [Google Scholar] [CrossRef]
- Seo, E.J.; Hong, J.; Lee, H.J.; Son, Y.J. Perioperative risk factors for new-onset postoperative atrial fibrillation after coronary artery bypass grafting: A systematic review. BMC Cardiovasc. Disord. 2021, 21, 418. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [PubMed]
- van de Kar, M.R.D.; van Brakel, T.J.; Van’t Veer, M.; van Steenbergen, G.J.; Daeter, E.J.; Crijns, H.; van Veghel, D.; Dekker, L.R.; Otterspoor, L.C. Anticoagulation for post-operative atrial fibrillation after isolated coronary artery bypass grafting: A meta-analysis. Eur. Heart J. 2024, 45, 2620–2630. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, R.; Kumar, R.; Malik, S.; Raj, T.; Kumar, P. Analysis of Heart Rate Variability and Implication of Different Factors on Heart Rate Variability. Curr. Cardiol. Rev. 2021, 17, e160721189770. [Google Scholar] [CrossRef]
- Francesco, B.; Maria Grazia, B.; Emanuele, G.; Valentina, F.; Sara, C.; Chiara, F.; Riccardo, M.; Francesco, F. Linear and nonlinear heart rate variability indexes in clinical practice. Comput. Math. Methods Med. 2012, 2012, 219080. [Google Scholar] [CrossRef]
- Yugar, L.B.T.; Yugar-Toledo, J.C.; Dinamarco, N.; Sedenho-Prado, L.G.; Moreno, B.V.D.; Rubio, T.A.; Fattori, A.; Rodrigues, B.; Vilela-Martin, J.F.; Moreno, H. The Role of Heart Rate Variability (HRV) in Different Hypertensive Syndromes. Diagnostics 2023, 13, 785. [Google Scholar] [CrossRef]
- Bogdan, C.; Apostol, A.; Ivan, V.M.; Sandu, O.E.; Petre, I.; Suciu, O.; Marc, L.-E.; Maralescu, F.-M.; Lighezan, D.F. Heart Rate Variability and Global Longitudinal Strain for Prognostic Evaluation and Recovery Assessment in Conservatively Managed Post-Myocardial Infarction Patients. J. Clin. Med. 2024, 13, 5435. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Norby, F.L.; Whitsel, E.A.; Soliman, E.Z.; Chen, L.Y.; Loehr, L.R.; Fuster, V.; Heiss, G.; Coresh, J.; Alonso, A. Cardiac Autonomic Dysfunction and Incidence of Atrial Fibrillation: Results from 20 Years Follow-Up. J. Am. Coll. Cardiol. 2017, 69, 291–299. [Google Scholar] [CrossRef]
- Thanh, N.V.; Hien, N.S.; Son, P.N.; Pho, D.C.; Son, P.T. Heart Rate Variability and Its Role in Predicting Atrial Fibrillation in Patients Undergoing Coronary Artery Bypass Graft. Int. J. Gen. Med. 2023, 16, 4919–4930. [Google Scholar] [CrossRef] [PubMed]
- Hakala, T.; Vanninen, E.; Hedman, A.; Hippelainen, M. Analysis of heart rate variability does not identify the patients at risk of atrial fibrillation after coronary artery bypass grafting. Scand. Cardiovasc. J. 2002, 36, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Chamchad, D.; Horrow, J.C.; Samuels, L.E.; Nakhamchik, L. Heart rate variability measures poorly predict atrial fibrillation after off-pump coronary artery bypass grafting. J. Clin. Anesth. 2011, 23, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Parolari, A.; Camera, M.; Alamanni, F.; Naliato, M.; Polvani, G.L.; Agrifoglio, M.; Brambilla, M.; Biancardi, C.; Mussoni, L.; Biglioli, P.; et al. Systemic inflammation after on-pump and off-pump coronary bypass surgery: A one-month follow-up. Ann. Thorac. Surg. 2007, 84, 823–828. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef]
- Peng, C.K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef]
- Acharya, U.R.; Bhat, P.S.; Kannathal, N.; Rao, A.; Lim, C.M. Analysis of cardiac health using fractal dimension and wavelet transformation. ITBM-RBM 2005, 26, 133–139. [Google Scholar] [CrossRef]
- Higuchi, T. Relationship between the fractal dimension and the power law index for a time series: A numerical investigation. Phys. D Nonlinear Phenom. 1990, 46, 254–264. [Google Scholar] [CrossRef]
- Higuchi, T. Approach to an irregular time series on the basis of the fractal theory. Phys. D Nonlinear Phenom. 1988, 31, 277–283. [Google Scholar] [CrossRef]
- Ivanov, P.C.; Amaral, L.A.; Goldberger, A.L.; Havlin, S.; Rosenblum, M.G.; Struzik, Z.R.; Stanley, H.E. Multifractality in human heartbeat dynamics. Nature 1999, 399, 461–465. [Google Scholar] [CrossRef]
- Kinoshita, T.; Asai, T.; Ishigaki, T.; Suzuki, T.; Kambara, A.; Matsubayashi, K. Preoperative heart rate variability predicts atrial fibrillation after coronary bypass grafting. Ann. Thorac. Surg. 2011, 91, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Stein, P.K.; Bigger, J.T., Jr. Heart rate variability: Measurement and clinical utility. Ann. Noninvasive Electrocardiol. 2005, 10, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Matusik, P.S.; Alomar, O.; Hussain, M.R.; Akrmah, M.; Matusik, P.T.; Chen, D.M.; Alomar, M.; Stein, P.K. Heart Rate Variability and Coronary Artery Bypass Grafting: A Systematic Review. Rev. Cardiovasc. Med. 2024, 25, 36. [Google Scholar] [CrossRef]
- Tarkiainen, T.H.; Hakala, T.; Hedman, A.; Vanninen, E. Preoperative alterations in correlation properties and complexity of R-R interval dynamics predict the risk of atrial fibrillation after coronary artery bypass grafting in patients with preserved left ventricular function. J. Cardiovasc. Electrophysiol. 2008, 19, 907–912. [Google Scholar] [CrossRef]
- Wu, Z.K.; Vikman, S.; Laurikka, J.; Pehkonen, E.; Iivainen, T.; Huikuri, H.V.; Tarkka, M.R. Nonlinear heart rate variability in CABG patients and the preconditioning effect. Eur. J. Cardiothorac. Surg. 2005, 28, 109–113. [Google Scholar] [CrossRef]
- Kalisnik, J.M.; Avbelj, V.; Vratanar, J.; Santarpino, G.; Gersak, B.; Fischlein, T.; Trobec, R.; Žibert, J. Cardiac autonomic regulation and PR interval determination for enhanced atrial fibrillation risk prediction after cardiac surgery. Int. J. Cardiol. 2019, 289, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, V.; Tauveron, I.; Bagheri, R.; Ugbolue, U.C.; Magnon, V.; Navel, V.; Bouillon-Minois, J.-B.; Dutheil, F. Heart rate variability in hypothyroid patients: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0269277. [Google Scholar] [CrossRef]
- Korpelainen, J.T.; Sotaniemi, K.A.; Huikuri, H.V.; Myllya, V.V. Abnormal heart rate variability as a manifestation of autonomic dysfunction in hemispheric brain infarction. Stroke 1996, 27, 2059–2063. [Google Scholar] [CrossRef]
- Vinik, A.I.; Ziegler, D. Diabetic cardiovascular autonomic neuropathy. Circulation 2007, 115, 387–397. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall (N = 67) | No AF (N = 40) | AF (N = 27) | p-Value |
|---|---|---|---|---|
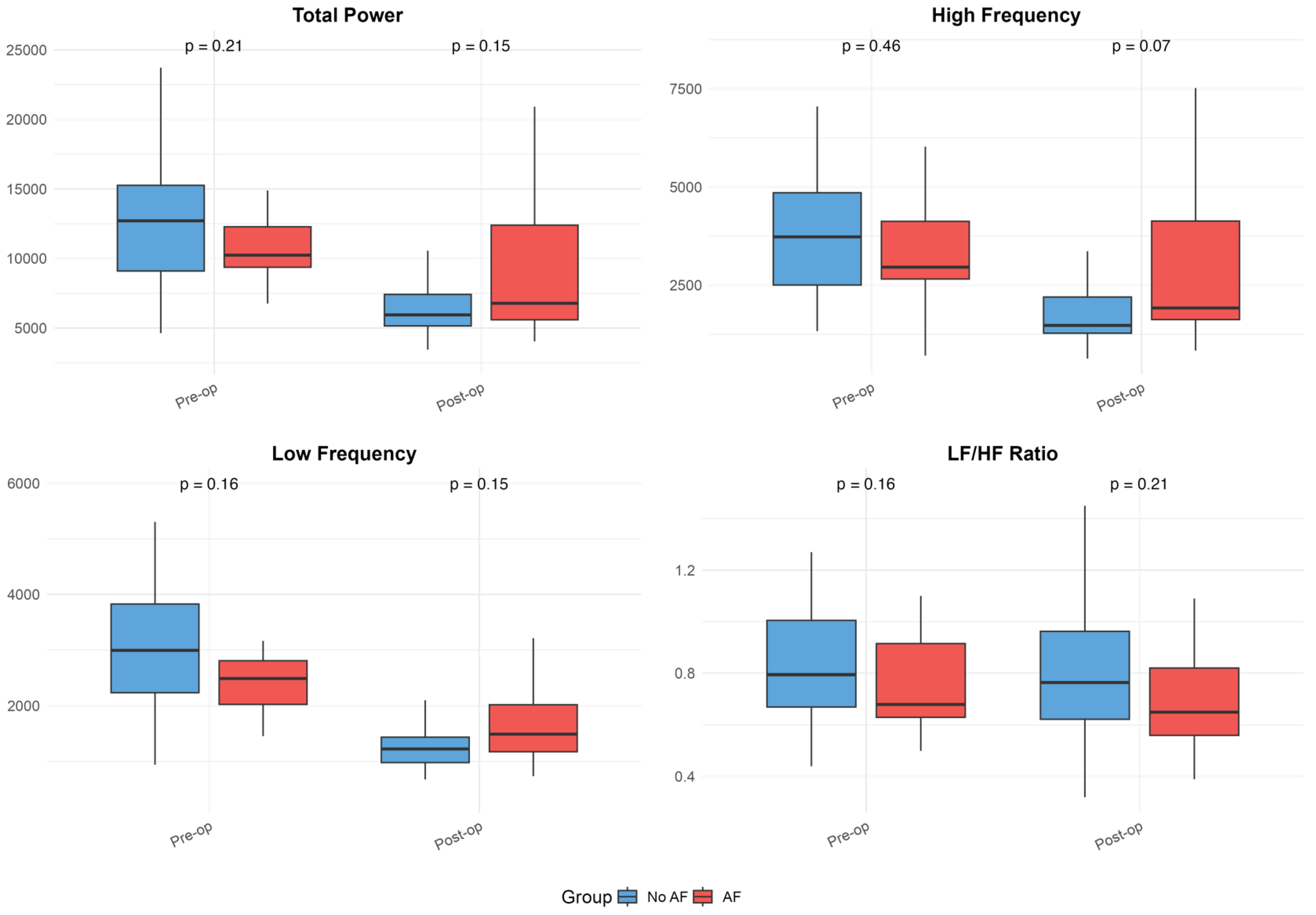
| Total Power pre-op (ms2) | 13,333.0 ± 9760.3 | 14,601.2 ± 11,892.2 | 11,381.9 ± 4531.2 | 0.210 |
| Total Power post-op (ms2) a | 7864.3 ± 4469.3 | 7114.6 ± 3997.2 | 9220.9 ± 5036.6 | 0.147 |
| High Frequency pre-op (ms2) | 3967.7 ± 2570.8 | 4219.7 ± 2907.6 | 3580.2 ± 1933.3 | 0.459 |
| High Frequency post-op (ms2) a | 2250.3 ± 1539.1 | 1944.1 ± 1317.5 | 2804.3 ± 1777.0 | 0.065 |
| Low Frequency pre-op (ms2) | 3269.5 ± 3664.9 | 3689.1 ± 4592.8 | 2624.0 ± 1140.4 | 0.156 |
| Low Frequency post-op (ms2) a | 1564.2 ± 1024.8 | 1466.7 ± 1101.4 | 1740.6 ± 866.3 | 0.147 |
| LF/HF Ratio pre-op | 0.82 ± 0.24 | 0.85 ± 0.25 | 0.78 ± 0.23 | 0.156 |
| LF/HF Ratio post-op a | 0.77 ± 0.26 | 0.80 ± 0.26 | 0.72 ± 0.26 | 0.210 |
| Alpha 1 pre-op | 1.17 ± 0.25 | 1.25 ± 0.18 | 1.05 ± 0.29 | 0.010 |
| Alpha 1 post-op day 3 b | 1.01 ± 0.42 | 1.13 ± 0.44 | 0.8 ± 0.29 | 0.009 |
| Alpha 1 post-op day 7 c | 1.05 ± 0.38 | 1.18 ± 0.37 | 0.86 ± 0.32 | 0.005 |
| Alpha 2 pre-op | 0.92 ± 0.11 | 0.91 ± 0.13 | 0.93 ± 0.08 | 0.394 |
| Alpha 2 post-op day 3 b | 0.98 ± 0.16 | 0.97 ± 0.18 | 0.98 ± 0.12 | 0.793 |
| Alpha 2 post-op day 7 c | 0.99 ± 0.14 | 1.0 ± 0.14 | 0.98 ± 0.16 | 0.719 |
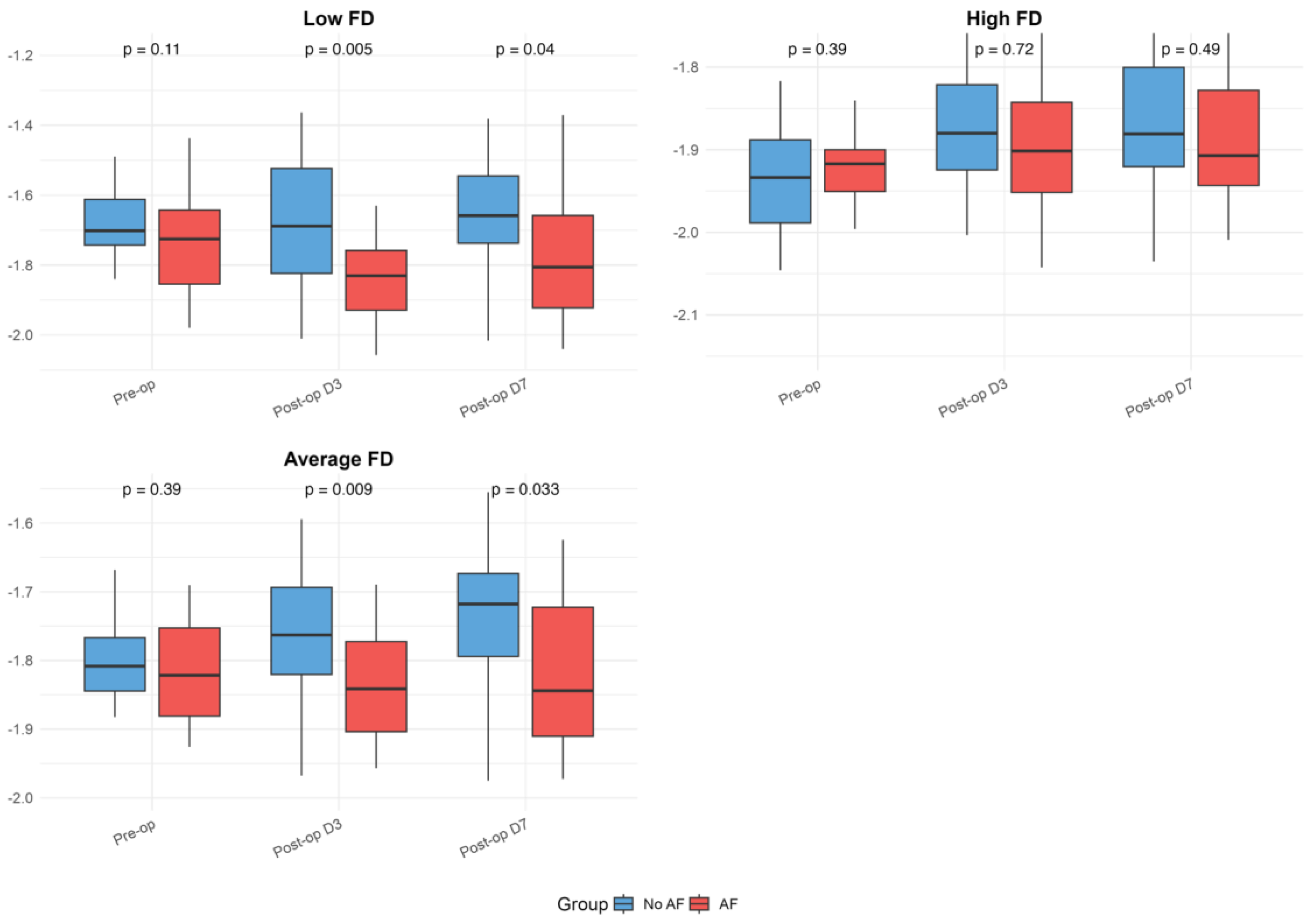
| Low FD pre-op | −1.71 ± 0.11 | −1.68 ± 0.09 | −1.74 ± 0.13 | 0.108 |
| Low FD post-op day 3 b | −1.74 ± 0.19 | −1.68 ± 0.19 | −1.84 ± 0.14 | 0.005 |
| Low FD post-op day 7 c | −1.72 ± 0.19 | −1.67 ± 0.18 | −1.79 ± 0.18 | 0.040 |
| High FD pre-op | −1.93 ± 0.06 | −1.93 ± 0.07 | −1.92 ± 0.05 | 0.394 |
| High FD post-op day 3 b | −1.88 ± 0.09 | −1.87 ± 0.09 | −1.88 ± 0.09 | 0.719 |
| High FD post-op day 7 c | −1.87 ± 0.09 | −1.86 ± 0.09 | −1.88 ± 0.08 | 0.489 |
| Average FD pre-op | −1.81 ± 0.06 | −1.8 ± 0.06 | −1.82 ± 0.07 | 0.394 |
| Average FD post-op day 3 b | −1.79 ± 0.1 | −1.76 ± 0.1 | −1.83 ± 0.08 | 0.009 |
| Average FD post-op day 7 c | −1.77 ± 0.11 | −1.74 ± 0.1 | −1.82 ± 0.11 | 0.033 |
| Variable | Value |
|---|---|
| Coronary artery disease | |
| Two-vessel disease | 21 (31%) |
| Three-vessel disease | 46 (69%) |
| Prior myocardial infarction | 33 (49%) |
| Arterial hypertension | 60 (90%) |
| Diabetes mellitus | 19 (28%) |
| Dyslipidemia | 67 (100%) |
| Left ventricular ejection fraction (%) | 55.3 ± 9.8 |
| Left atrial diameter (cm) | 4.0 ± 0.5 |
| EuroSCORE | 2.9 ± 2.6 |
| Number of grafts performed | 2.5 ± 0.9 |
| Medication use (admission/discharge) | |
| β-blockers | 100%/100% |
| ACE inhibitors | 53%/51% |
| Calcium channel blockers | 13%/2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kšela, J.; Kafol, J.; Avbelj, V.; Kališnik, J.M. Predictive Value of Heart Rate Variability for Postoperative Atrial Fibrillation in Off-Pump Coronary Artery Bypass Patients. Medicina 2025, 61, 984. https://doi.org/10.3390/medicina61060984
Kšela J, Kafol J, Avbelj V, Kališnik JM. Predictive Value of Heart Rate Variability for Postoperative Atrial Fibrillation in Off-Pump Coronary Artery Bypass Patients. Medicina. 2025; 61(6):984. https://doi.org/10.3390/medicina61060984
Chicago/Turabian StyleKšela, Juš, Jan Kafol, Viktor Avbelj, and Jurij Matija Kališnik. 2025. "Predictive Value of Heart Rate Variability for Postoperative Atrial Fibrillation in Off-Pump Coronary Artery Bypass Patients" Medicina 61, no. 6: 984. https://doi.org/10.3390/medicina61060984
APA StyleKšela, J., Kafol, J., Avbelj, V., & Kališnik, J. M. (2025). Predictive Value of Heart Rate Variability for Postoperative Atrial Fibrillation in Off-Pump Coronary Artery Bypass Patients. Medicina, 61(6), 984. https://doi.org/10.3390/medicina61060984