
Effectiveness and Safety of Pharmacopuncture Therapy Compared to Standard Physical Therapy in Patients with Chronic Knee Pain: A Pilot Study for a Pragmatic Randomized Controlled Trial
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Interventions
2.3.1. Control Group: Standard Physical Therapy (PT)
2.3.2. Experimental Group: PPT
2.4. Outcomes
2.4.1. Primary Outcome: NRS Score
2.4.2. Secondary Outcomes
Visual Analog Scale (VAS) Score
Range of Motion (ROM) of the Knee
Korean Western Ontario and McMaster (K-WOMAC) Score
Patient Global Impression of Change Score
Short Form-12 Health Survey (SF-12) Version 2 Score
Five-Level EuroQol 5-Dimension (EQ-5D-5L) Score
Feasibility-Related Outcomes
Drug Consumption
Adverse Events
2.5. Sample Size Calculation
2.6. Recruitment
2.7. Randomization
2.8. Blinding
2.9. Data Collection and Management
2.10. Statistical Analysis
3. Results
3.1. Participant Flow
3.2. Baseline Characteristics
3.3. Treatment
3.4. Primary and Secondary Outcomes
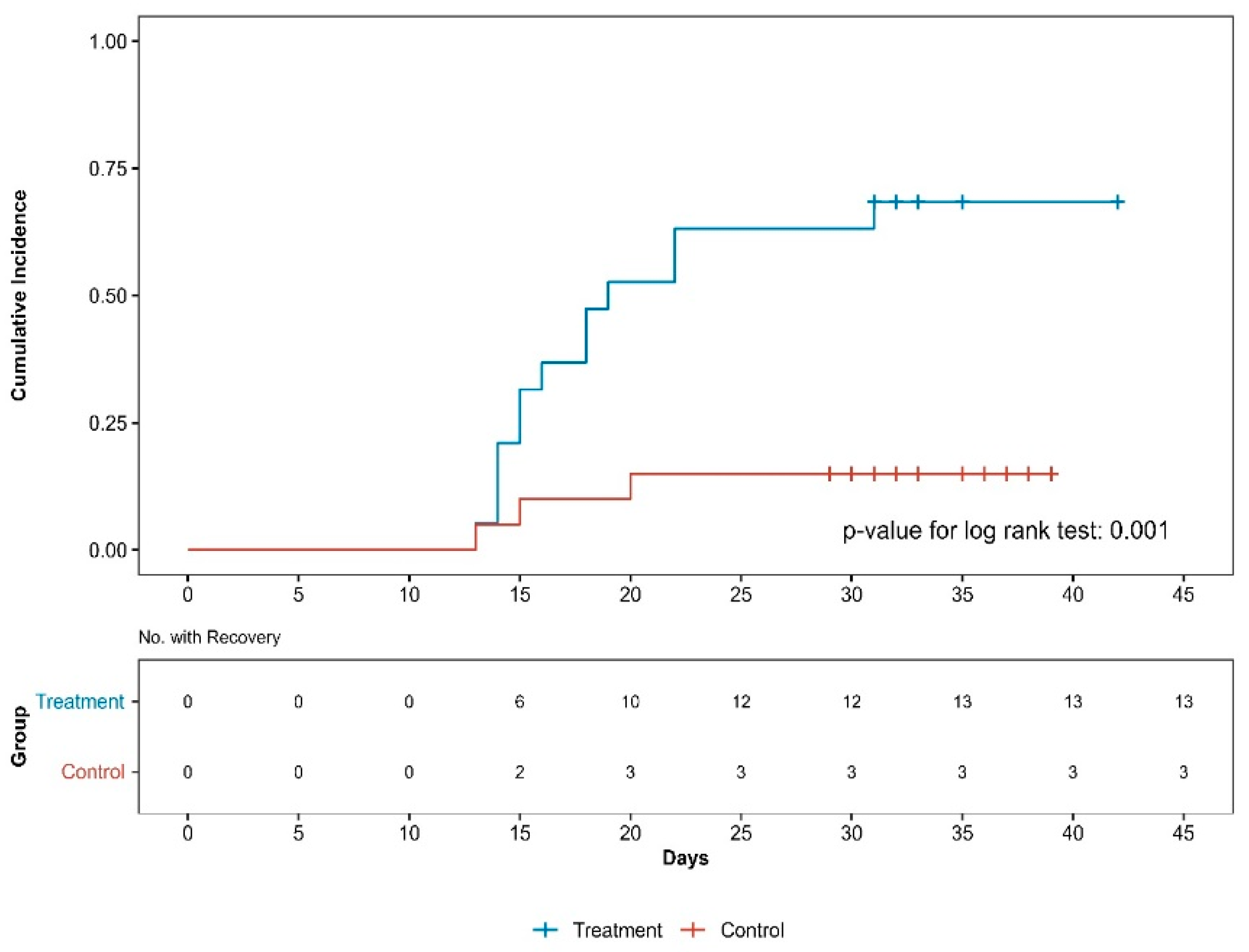
3.5. Survival Analysis
3.6. Feasibility-Related Outcomes
3.7. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OA | osteoarthritis |
| TENS | transcutaneous electrical nerve stimulation |
| ICT | interferential current therapy |
| KM | Korean medicine |
| PPT | pharmacopuncture therapy |
| RCTs | randomized controlled trials |
| NRS | numeric rating scale |
| PT | physical therapy |
| KMDs | KM doctors |
| VAS | visual analog scale |
| ROM | range of motion |
| K-WOMAC | Korean Western Ontario and McMaster |
| SF-12 | Short Form-12 Health Survey |
| HRQoL | health-related quality of life |
| EQ-5D-5L | five-level EuroQol 5 dimensions |
| AEs | adverse events |
| ADLs | activities of daily living |
| CRF | case report form |
| ITT | Intention to treat |
| PP | per protocol |
| LMM | linear mixed model |
| ANCOVA | analysis of covariance |
| AUC | area under the curve |
| LOCF | last observation carried forward |
| CI | confidence interval |
| PASS | patient-acceptable symptom state |
| MCID | minimal clinically important difference |
| MMP | matrix metalloproteinase |
References
- Jhun, H.J.; Ahn, K.; Lee, S.C. Estimation of the prevalence of osteoarthritis in Korean adults based on the data from the fourth Korea national health and nutrition examination survey. Anesth. Pain Med. 2010, 5, 201–206. [Google Scholar]
- Jones, B.Q.; Covey, C.J.; Sineath, M.H., Jr. Nonsurgical management of knee pain in adults. Am. Fam. Physician 2015, 92, 875–883. [Google Scholar] [PubMed]
- Duong, V.; Oo, W.M.; Ding, C.; Culvenor, A.G.; Hunter, D.J. Evaluation and treatment of knee pain: A review. Jama 2023, 330, 1568–1580. [Google Scholar] [CrossRef]
- Kwon, S.-H.; Lee, J.-H.; Kim, K.-K. The Accuracy of Lower Extremity Alignment in Total Knee Arthroplasty Using Navigation System-Data Analysis of 661 Cases. J. Korean Orthop. Assoc. 2009, 44, 599–603. [Google Scholar] [CrossRef]
- Zhang, W.; Nuki, G.; Moskowitz, R.; Abramson, S.; Altman, R.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.; Croft, P.; Doherty, M. OARSI recommendations for the management of hip and knee osteoarthritis: Part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthr. Cartil. 2010, 18, 476–499. [Google Scholar] [CrossRef]
- de Almeida, C.C.; da Silva, V.Z.M.; Júnior, G.C.; Liebano, R.E.; Durigan, J.L.Q. Transcutaneous electrical nerve stimulation and interferential current demonstrate similar effects in relieving acute and chronic pain: A systematic review with meta-analysis. Braz. J. Phys. Ther. 2018, 22, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.Y.; Lee, Y.J.; Shin, J.-S.; Lee, J.; Kim, M.-r.; Koh, W.; Cha, Y.-Y.; Shin, B.-C.; Hwang, E.-H.; Suhr, K.; et al. Analysis of medical service use of knee osteoarthritis and knee meniscal and ligament injuries in Korea: A cross-sectional study of national patient sample data. BMC Musculoskelet. Disord. 2017, 18, 438. [Google Scholar] [CrossRef]
- Lee, G.-e.; Huh, S.-w.; Lee, H.-h.; Jeong, S.-h.; Jo, K.-s.; Han, S.-h.; Choi, J.-h.; Roh, J.-a. The study on correlation between the KL-grade and improvement of knee pain treated by Korean medicine therapy. J. Korean Med. Rehabil. 2017, 27, 137–146. [Google Scholar] [CrossRef]
- Mr, K.; Lee, S.; Lee, Y.; Ha, I. Clinical research on pharmacopuncture in Korea: A scoping review. Perspect. Integr. Med. 2023, 2, 8–23. [Google Scholar]
- Choi, S.; Chae, H.K.; Heo, H.; Hahm, D.-H.; Kim, W.; Kim, S.K. Analgesic effect of melittin on oxaliplatin-induced peripheral neuropathy in rats. Toxins 2019, 11, 396. [Google Scholar] [CrossRef]
- Lee, M.S.; Pittler, M.H.; Shin, B.-C.; Kong, J.C.; Ernst, E. Bee venom acupuncture for musculoskeletal pain: A review. J. Pain 2008, 9, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.-W.; Kim, S.-J. A review of clinical study on Jungsongouhyul pharmacopuncture treatment published in Korea. J. Korean Med. Rehabil. 2017, 27, 75–84. [Google Scholar] [CrossRef]
- Lee, S.-H.; Kwon, G.-S.; Kang, M.-S.; Yoon, H.-M.; Kim, C.-H. Comparative study on the effects of bee venom pharmacopuncture according to the treatment method for knee osteoarthritis. J. Pharmacopunct. 2012, 15, 7. [Google Scholar] [CrossRef]
- Shin, S.Y.; Seo, D.K.; Kim, S.Y.; Seo, J.C.; Seo, Y.J.; Lee, Y.J.; Bin, C.H.; Jung, T.G.; Song, C.H.; Yoon, H.M.; et al. The effect of chinemys reevesii gray pharmacopuncture for women with knee osteoarthritis. Acupuncture 2015, 32, 163–173. [Google Scholar] [CrossRef]
- Yang, K.-R.; Song, H.-S. A comparative study of warm needling and bee venom pharmacopuncture on osteoarthritis of the knee-a randomized controlled trial. J. Pharmacopunct. 2008, 11, 21–31. [Google Scholar] [CrossRef]
- Sun, X. Acupoint Injection Therapy for Knee Osteoarthritis Clinical Observation. Master’s Thesis, Nanjing University of Chinese Medicine, Nanjing, China, 2009. [Google Scholar]
- Welsh, J.T. Assessing pain in the ED including the use of pain scales (such as OSBD, FLACC, VRS, NRS, CRS, and Oucher). Curr. Emerg. Hosp. Med. Rep. 2016, 4, 19–25. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Ko, T.-S.; Kim, S.-Y.; Lee, J.-S. Reliability and validity of the Korean Western Ontario and McMaster Universities (WOMAC) osteoarthritis index in patients with osteoarthritis of the knee. J. Korean Med. Rehabil. 2009, 19, 251–260. [Google Scholar]
- Scott, W.; McCracken, L.M. Patients’ impression of change following treatment for chronic pain: Global, specific, a single dimension, or many? J. Pain 2015, 16, 518–526. [Google Scholar] [CrossRef]
- Kim, S.-H.; Jo, M.-W.; Ahn, J.; Ock, M.; Shin, S.; Park, J. Assessment of psychometric properties of the Korean SF-12 v2 in the general population. BMC Public Health 2014, 14, 1086. [Google Scholar] [CrossRef]
- Kim, S.-H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.-W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Kieser, M.; Wassmer, G. On the use of the upper confidence limit for the variance from a pilot sample for sample size determination. Biom. J. 1996, 38, 941–949. [Google Scholar] [CrossRef]
- Browne, R.H. On the use of a pilot sample for sample size determination. Stat. Med. 1995, 14, 1933–1940. [Google Scholar] [CrossRef]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant states in patient reported outcomes in knee and hip osteoarthritis: The patient acceptable symptom state. Ann. Rheum. Dis. 2005, 64, 34–37. [Google Scholar] [CrossRef]
- Kim, M.S.; Koh, I.J.; Choi, K.Y.; Sung, Y.G.; Park, D.C.; Lee, H.J.; In, Y. The minimal clinically important difference (MCID) for the WOMAC and factors related to achievement of the MCID after medial opening wedge high tibial osteotomy for knee osteoarthritis. Am. J. Sports Med. 2021, 49, 2406–2415. [Google Scholar] [CrossRef]
- Luna, S.P.; Angeli, A.L.; Ferreira, C.L.; Lettry, V.; Scognamillo-Szabo, M. Comparison of pharmacopuncture, aquapuncture and acepromazine for sedation of horses. Evid.-Based Complement. Altern. Med. 2008, 5, 194584. [Google Scholar] [CrossRef] [PubMed]
- Strudwick, M.W.; Hinks, R.C.; Choy, S.B. Point injection as an alternative acupuncture technique–an exploratory study of responses in healthy subjects. Acupunct. Med. 2007, 25, 166–174. [Google Scholar] [CrossRef]
- Melzack, R.; Stillwell, D.M.; Fox, E.J. Trigger points and acupuncture points for pain: Correlations and implications. Pain 1977, 3, 3–23. [Google Scholar] [CrossRef]
- Kim, W.K.; Chung, H.J.; Pyee, Y.; Choi, T.J.; Park, H.J.; Hong, J.Y.; Shin, J.S.; Lee, J.H.; Ha, I.H.; Lee, S.K. Effects of intra-articular SHINBARO treatment on monosodium iodoacetate-induced osteoarthritis in rats. Chin. Med. 2016, 11, 17. [Google Scholar] [CrossRef]
- Kim, H.; Hong, J.Y.; Jeon, W.J.; Kim, H.; Yeo, C.; Lee, J.; Lee, Y.J.; Ha, I.H. Synergistic attenuation of complete freund’s adjuvant-induced inflammation in mice using shinbaro-pelubiprofen: A novel therapeutic complex. Mol. Med. 2025, 31, 17. [Google Scholar] [CrossRef]
- Dye, S.F. The pathophysiology of patellofemoral pain: A tissue homeostasis perspective. Clin. Orthop. Relat. Res. 2005, 436, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Oliva, E.; Martínez-Pozas, O.; Sinatti, P.; Martín Carreras-Presas, C.; Cuenca-Zaldívar, J.N.; Turroni, S.; Sánchez Romero, E.A. Relationship Between the Gut Microbiome, Tryptophan-Derived Metabolites, and Osteoarthritis-Related Pain: A Systematic Review with Meta-Analysis. Nutrients 2025, 17, 264. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Zaldívar, J.N.; del Corral-Villar, C.; García-Torres, S.; Araujo-Zamora, R.; Gragera-Peña, P.; Martínez-Lozano, P.; Sánchez-Romero, E.A. Fourteen-Year Retrospective Cohort Study on the Impact of Climatic Factors on Chronic Musculoskeletal Pain: A Spanish Primary Care Analysis. Int. J. Rheum. Dis. 2025, 28, e70125. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Lee, K.; Ju, J.H. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int. J. Mol. Sci. 2021, 22, 2619. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudian, A.; Lohmander, L.S.; Mobasheri, A.; Englund, M.; Luyten, F.P. Early-stage symptomatic osteoarthritis of the knee—Time for action. Nat. Rev. Rheumatol. 2021, 17, 621–632. [Google Scholar] [CrossRef]
- Liew, J.; King, L.; Mahmoudian, A.; Wang, Q.; Flynn, D.; Appleton, T.; Englund, M.; Haugen, I.; Lohmander, S.; Runhaar, J.; et al. Defining Early-Stage Knee Osteoarthritis: A Scoping Review. Osteoarthr. Cartil. 2023, 31, S201–S202. [Google Scholar] [CrossRef]
- Li, X.; Li, C.; Zhang, P. Predictive models of radiographic progression and pain progression in patients with knee osteoarthritis: Data from the FNIH OA biomarkers consortium project. Arthritis Res. Ther. 2024, 26, 112. [Google Scholar] [CrossRef]
- Kompel, A.J.; Roemer, F.W.; Murakami, A.M.; Diaz, L.E.; Crema, M.D.; Guermazi, A. Intra-articular corticosteroid injections in the hip and knee: Perhaps not as safe as we thought? Radiology 2019, 293, 656–663. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Total | PT Group | PPT Group | p-Value | |
|---|---|---|---|---|
| N = 39 | n = 19 | n = 20 | ||
| Sex | ||||
| Male | 17 (43.6) | 9 (47.4) | 8 (40.0) | 0.888 |
| Female | 22 (56.4) | 10 (52.6) | 12 (60.0) | |
| Age, years | ||||
| Mean ± SD | 43.92 ± 15.26 | 45.05 ± 16.34 | 42.85 ± 14.50 | 0.658 |
| <30 | 10 (25.6) | 6 (31.6) | 4 (20.0) | 0.288 |
| 30–39 | 9 (23.1) | 3 (15.8) | 6 (30.0) | |
| 40–49 | 3 (7.7) | - | 3 (15.0) | |
| 50–59 | 8 (20.5) | 4 (21.1) | 4 (20.0) | |
| ≥60 | 9 (23.1) | 6 (31.6) | 3 (15.0) | |
| BMI, kg/m2 | ||||
| Mean ± SD | 22.24 ± 3.69 | 22.47 ± 3.68 | 22.02 ± 3.78 | 0.705 |
| <25 | 30 (76.9) | 13 (68.4) | 17 (85.0) | 0.273 |
| ≥25 | 9 (23.1) | 6 (31.6) | 3 (15.0) | |
| Knee radiograph findings | ||||
| normal | 34 (87.2) | 16 (84.2) | 18 (90.0) | 0.661 |
| NCS | 5 (12.8) | 3 (15.8) | 2 (10.0) | |
| Pain location | ||||
| Lt. knee | 18 (46.2) | 9 (47.4) | 9 (45.0) | 1.000 |
| Rt. knee | 21 (53.8) | 10 (52.6) | 11 (55.0) | |
| Symptom severity | ||||
| Mild (not uncomfortable) | - | - | - | 0.431 |
| Moderate (uncomfortable but manageable) | 22 (56.4) | 9 (47.4) | 13 (65.0) | |
| Severe (serious but untreated) | 17 (43.6) | 10 (52.6) | 7 (35.0) | |
| Severe (serious and requires treatment) | - | - | - | |
| Medication history | ||||
| Yes | 22 (56.4) | 11 (57.9) | 11 (55.0) | 1.000 |
| No | 17 (43.6) | 8 (42.1) | 9 (45.0) |
| Week 1-1 | Week 2-1 | Week 3-1 | Week 4 | Week 6 | ||
|---|---|---|---|---|---|---|
| NRS score | PPT group | 5.87 (5.62–6.12) | 5.16 (4.64–5.67) | 3.89 (3.38–4.39) | 3.15 (2.64–3.66) | 3.15 (2.64–3.66) |
| PT group | 5.45 (4.96–5.95) | 5.05 (4.56–5.55) | 5.20 (4.71–5.70) | 5.20 (4.71–5.70) | ||
| Difference | — | −0.29 (−1.01 to 0.42) | −1.17 (−1.88 to −0.46) | −2.05 (−2.76 to −1.34) | −2.05 (−2.76 to −1.34) | |
| p-value | — | 0.417 | 0.002 ** | <0.001 *** | <0.001 *** | |
| VAS score | PPT group | 59.18 (56.77–61.59) | 51.40 (45.72–57.09) | 38.74 (33.16–44.32) | 30.63 (25.05–36.21) | 32.17 (25.98 to 38.35) |
| PT group | 54.97 (49.51–60.42) | 50.67 (45.21–56.12) | 52.22 (46.76–57.67) | 50.92 (44.93 to 56.91) | ||
| Difference | — | −3.56 (−11.48 to 4.35) | −11.93 (−19.77 to −4.09) | −21.58 (−29.42 to −13.74) | −18.75 (−27.39 to −10.11) | |
| p-value | — | 0.373 | 0.003 ** | <0.001 *** | <0.001 *** | |
| K-WOMAC score | PPT group | 59.31 (53.69–64.92) | — | — | 43.02 (36.96–49.07) | 41.49 (35.43–47.55) |
| PT group | — | — | 56.18 (50.28–62.09) | 54.93 (49.03–60.84) | ||
| Difference | — | — | — | −13.17 (−21.67 to −4.67) | −13.45 (−21.95 to −4.94) | |
| p-value | — | — | — | 0.003 ** | 0.003 ** | |
| PCS score | PPT group | 39.62 (37.67–41.57) | — | — | 43.52 (40.84–46.20) | 44.35 (41.67–47.03) |
| PT group | — | — | 42.03 (39.41–44.64) | 42.00 (39.39–44.62) | ||
| Difference | — | — | — | 1.49 (−2.26 to 5.25) | 2.35 (−1.41 to 6.10) | |
| p-value | — | — | — | 0.429 | 0.216 | |
| MCS score | PPT group | 51.48 (48.60–54.36) | — | — | 53.27 (50.28–56.26) | 54.85 (51.86–57.84) |
| PT group | — | — | 51.89 (48.97–54.80) | 51.01 (48.09–53.92) | ||
| Difference | — | — | — | 1.39 (−2.84 to 5.61) | 3.85 (−0.38 to 8.07) | |
| p-value | — | — | — | 0.515 | 0.074 | |
| EQ-5D-5L score | PPT group | 0.73 (0.69–0.76) | — | — | 0.81 (0.77–0.85) | 0.81 (0.77–0.85) |
| PT group | — | — | 0.78 (0.74–0.82) | 0.75 (0.72–0.79) | ||
| Difference | — | — | — | 0.03 (−0.02 to 0.08) | 0.06 (0.01–0.11) | |
| p-value | — | — | — | 0.286 | 0.030 * |
| Group | Adverse Event (LLT) | Severity | Causality |
|---|---|---|---|
| PT | Bruise | Moderate | Certain |
| PT | Bruise | Moderate | Certain |
| PT | Paresthesia | Mild | Possible |
| PT | Bruise | Mild | Certain |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, M.I.; Lim, J.K.; Kim, Y.J.; Jeon, Y.S.; Kim, S.; Kim, C.Y.; Park, Y.-C.; Kim, E.-J.; Hong, Y.; Nam, D.; et al. Effectiveness and Safety of Pharmacopuncture Therapy Compared to Standard Physical Therapy in Patients with Chronic Knee Pain: A Pilot Study for a Pragmatic Randomized Controlled Trial. Medicina 2025, 61, 1106. https://doi.org/10.3390/medicina61061106
Jeong MI, Lim JK, Kim YJ, Jeon YS, Kim S, Kim CY, Park Y-C, Kim E-J, Hong Y, Nam D, et al. Effectiveness and Safety of Pharmacopuncture Therapy Compared to Standard Physical Therapy in Patients with Chronic Knee Pain: A Pilot Study for a Pragmatic Randomized Controlled Trial. Medicina. 2025; 61(6):1106. https://doi.org/10.3390/medicina61061106
Chicago/Turabian StyleJeong, Myung In, Jun Kyu Lim, Yong Jun Kim, Yu Sun Jeon, Suna Kim, Chang Youn Kim, Yeon-Cheol Park, Eun-Jung Kim, Yejin Hong, Dongwoo Nam, and et al. 2025. "Effectiveness and Safety of Pharmacopuncture Therapy Compared to Standard Physical Therapy in Patients with Chronic Knee Pain: A Pilot Study for a Pragmatic Randomized Controlled Trial" Medicina 61, no. 6: 1106. https://doi.org/10.3390/medicina61061106
APA StyleJeong, M. I., Lim, J. K., Kim, Y. J., Jeon, Y. S., Kim, S., Kim, C. Y., Park, Y.-C., Kim, E.-J., Hong, Y., Nam, D., Lee, Y. J., Kim, D., & Ha, I.-H. (2025). Effectiveness and Safety of Pharmacopuncture Therapy Compared to Standard Physical Therapy in Patients with Chronic Knee Pain: A Pilot Study for a Pragmatic Randomized Controlled Trial. Medicina, 61(6), 1106. https://doi.org/10.3390/medicina61061106