
Evaluation of Secondary Prevention Knowledge in Patients with Coronary Artery Disease


Abstract
1. Introduction
2. Study Objective
3. Materials and Methods
3.1. Inclusion Criteria
3.2. Exclusion Criteria
3.3. Data Collection
3.4. Data Analysis
4. Results
Sample Characteristics
5. Discussion
6. Conclusions
- Nursing with assessment tools in order to fill knowledge gaps with regard to secondary prevention among coronary artery disease patients;
- Focusing on education for coronary artery disease patients with comorbidities and behaviour that increases cardiovascular risk;
- Stressing the promotion of knowledge and secondary prevention education among patients hospitalised with coronary artery disease.
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mareš, J.; Kebza, V.; Blatný, M.; Fafejda, O.; Fraňková, S.; Hacklová, R.; Holčík, J.; Hoskovec, J.; Hošek, V.; Hrachovinová, T.; et al. Psychologie zdraví; Grada Publishing: Prague, Czech Republic, 2024; 608p. [Google Scholar]
- Beauchamp, A.; Talevski, J.; Niebauer, J.; Gutenberg, J.; Kefalianos, E.; Mayr, B.; Sareban, M.; Kulnik, S.T. Health literacy interventions for secondary prevention of coronary artery disease: A scoping review. Open Heart 2022, 9, e001895. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Geng, J.; Wang, M.; Hu, L.; De Melo Ghisi, G.L.; Yu, H. The Chinese version of the Coronary Artery Disease Education Questionnaire-II (CADEQ-II): Translation and validation. Patient Prefer. Adherence 2018, 12, 1587–1596. [Google Scholar] [CrossRef] [PubMed]
- Jennings, C.; Astin, F.; Fitzsimons, D.; Lambrinou, E.; Neubeck, L.; Thomson, R.D. ESC Textbook of Cardiovascular Nursing; Oxford University Press: Oxford, UK, 2022; 472p. [Google Scholar]
- Dunbar, S.B.; Braun, L.T. Preventive Cardiovascular Nursing, Resilience Across the Lifespan for Optimal Cardiovascular Wellness; Springer Nature AG: Cham, Switzerland, 2024; 734p. [Google Scholar]
- De Melo Ghisi, G.L.; Da Silva Chaves, G.S.; Britto, R.R.; Oh, P. Health literacy and coronary artery disease: A systematic review. Patient Educ. Couns. 2017, 101, 177–184. [Google Scholar] [CrossRef] [PubMed]
- De Melo Ghisi, G.L.; Sandison, N.; Oh, P. Development, pilot testing and psychometric validation of a short version of the coronary artery disease education questionnaire: The CADE-Q SV. Patient Educ. Couns. 2015, 99, 443–447. [Google Scholar] [CrossRef] [PubMed]
- De Melo Ghisi, G.L.; Grace, S.L.; Thomas, S.; Evans, M.F.; Oh, P. Development and psychometric validation of the second version of the Coronary Artery Disease Education Questionnaire (CADE-Q II). Patient Educ. Couns. 2014, 98, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S. Precision Medicine in Cardiovascular Disease Prevention; Springer Nature AG: Cham, Switzerland, 2021; 187p. [Google Scholar]
- De Melo Ghisi, G.L.; Oh, P. Validation of the French-Canadian version of a short questionnaire to assess knowledge in cardiac Patients (CADE-Q SV). Can. J. Nurs. Res. 2021, 54, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Jennings, C.; Graham, I.; Gielen, S. The ESC Handbook of Preventive Cardiology: Putting Prevention into Practice; Oxford University Press: Oxford, UK, 2016; 222p. [Google Scholar]
- Dosbaba, F.; Baťalík, L.; Filáková, K.; Felšöci, M.; Gombošová, A.; Hartman, M.; Hnatiak, J.; Charvát, R.; Chvojková, L.; Janoušek, J.; et al. Kardiovaskulární Rehabilitace a Prevence; Grada Publishing: Prague, Czech Republic, 2023; 376p. [Google Scholar]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. ESC Guidelines for the management of chronic coronary syndromes: Developed by the task force for the management of chronic coronary syndromes of the European Society of Cardiology Endorsed by the European Association for Cardio-Thoracic Surgery. Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef] [PubMed]
- Laskova, A.; Lopatin, Y. Translation, cross-cultural adaptation, and psychometric validation of the Russian Coronary Artery Disease Education Questionnaire II (CADE–Q II) in chronic coronary syndrome patients. Рoссийский Кардиoлoгический Журнал 2022, 4, 93–99. [Google Scholar] [CrossRef]
- Santos, R.Z.D.; Ghisi, G.L.M.; Bonin, C.D.B.; Chaves, G.; Haase, C.M.; Britto, R.R.; Benetti, M. Validation of the Brazilian version of CADE-Q II to assess knowledge of coronary artery disease patients. Arq. Bras. Cardiol. 2019, 112, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Tuka, V.; Daňková, M.; Ibarburu Lorenzo, Y.L.V.; Kosák, M.; Kovárnik, T.; Krupička, J.; Lambert, L.; Matoulek, M.; Oreská, S.; Pánková, A.; et al. Preventivní Kardiologie pro Praxis; NOL: Prague, Czech Republic, 2018; 204p. [Google Scholar]
- Frank, L.J.; Mach, F.; Yvo, M.; Carballo, D.; Konstantinos, C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.; Capodanno, D. ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Fattirolli, F.; Bettinardi, O.; Angelino, E.; da Vico, L.; Ferrari, M.; Pierobon, A.; Temporelli, D.; Agostini, S.; Ambrosetti, M.; Biffi, B.; et al. What constitutes the ‘Minimal Care’ interventions of the nurse, physiotherapist, dietician and psychologist in Cardiovascular Rehabilitation and secondary prevention: A position paper from the Italian Association for Cardiovascular Prevention, Rehabilitation and Epidemiology. Eur. J. Prev. Cardiol. 2018, 25, 1799–1810. [Google Scholar] [CrossRef] [PubMed]
- Valérie, T.; Ivana, C.; Radka, P. Význam Ošetřovateľství v Preventivní Kardiológii; Grada Publishing: Prague, Czech Republic, 2019; 160p. [Google Scholar]
- Vysoký, R.; Konečný, P. Rehabilitace a Preskripce Pohybové Aktivity u Kardiovaskulárních a Vybraných Interních Onemocnĕní; Univerzita Palackého: Olomouc, Czech Republic, 2022; 190p. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2020, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients with Chronic Coronary Disease. J. Am. Coll. Cardiol. 2023, 82, 833–955. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.; Schmid, J.P.; Piepoli, M. Cardiac Rehabilitation: A Practical Clinical Guide; Oxford University Press: Oxford, UK, 2020; 190p. [Google Scholar]
- Honzák, R. Psycho-Somatická Prvouka; Vyšehrad: Prague, Czech Republic, 2017; 352p. [Google Scholar]
- Kopecky, S. Live Younger Longer, 6 Steps to Prevent Heart Disease, Cancer, Alzheimer’s, Diabetes and More; Mayo Clinic Press: Rochester, NY, USA, 2021; 224p. [Google Scholar]

{kind=link}
{kind=link}
| Sex | n | % | CADE-Q II (mean ± SD) |
| Male | 191 | 75.5 | 61.45 ± 10.94 |
| Female | 62 | 24.5 | 60.27 ± 12.84 |
| Education level | |||
| University | 76 | 30.0 | 65.67 ± 10.05 |
| Secondary School | 173 | 68.4 | 59.48 ± 11.28 |
| Primary School | 4 | 1.6 | 48.50 ± 15.05 |
| Living area | |||
| City | 170 | 67.2 | 62.11 ± 11.20 |
| Countryside | 83 | 32.8 | 59.21 ± 11.69 |
| Age groups | |||
| Patients ≤ 60 years | 140 | 55.3 | 62.67 ± 11.93 |
| Patients ≥ 61 years | 113 | 44.7 | 59.29 ± 10.52 |
| Clinical Characteristics | n | % | CADE-Q II (mean ± SD) |
| STEMI | 139 | 54.5 | 61.17 ± 11.30 |
| NSTEMI | 114 | 45.5 | 61.15 ± 11.62 |
| CCS | 30 | 11.9 | 62.16 ± 12.04 |
| Indicated PCI | 183 | 72.3 | 60.87 ± 11.87 |
| Indicated CABG | 45 | 17.8 | 60.71 ± 11.73 |
| Arterial hypertension | 174 | 66.8 | 61.01 ± 11.04 |
| Diabetes mellitus | 56 | 22.1 | 59.66 ± 12.10 |
| Tobacco use | |||
| Smoking profile | n | % | CADE-Q II (mean ± SD) |
| Current smokers | 93 | 36.8 | 59.52 ± 11.81 |
| Former smokers | 68 | 26.9 | 61.47 ± 11.46 |
| Never smokers | 72 | 28.5 | 63.70 ± 11.56 |
| Quitting smokers | 12 | 4.7 | 60.33 ± 7.42 |
| Occasional smokers | 8 | 3.2 | 56.0 ± 5.6 |
| Anthropometric characteristics (mean + SD) | |||
| Male | Female | N = 253 | |
| Body mass index | 28.77 ± 4.12 | 28.05 ± 5.99 | 28.59± 4.64 |
| Waist circumference (cm) | 104.97 ± 10.64 | 94.73 ± 12.11 | 102.63 ± 11.79 |
| Body Mass Index | n | % | |
| BMI 18.5–24.9 | 59 | 23.3 | |
| BMI 25–29.9 | 103 | 40.7 | |
| BMI 30–34.9 | 72 | 28.5 | |
| BMI 35–39.9 | 15 | 5.9 | |
| BMI ≥ 40 | 4 | 1.6 | |
| Biological parameter | |||
| Lipid profile | |||
| N = 253 | Mean + SD | Median (Me) | 95% CI |
| TC−7 | 5.25 ± 1.37 | 5.3 | 5.08; 5.42 |
| LDL-C−4 | 3.55 ± 1.23 | 3.57 | 3.39; 3.7 |
| HDL-C−4 | 1.17 ± 0.32 | 1.13 | 1.12; 1.21 |
| TG−6 | 1.37 | 1.58; 2.01 | |
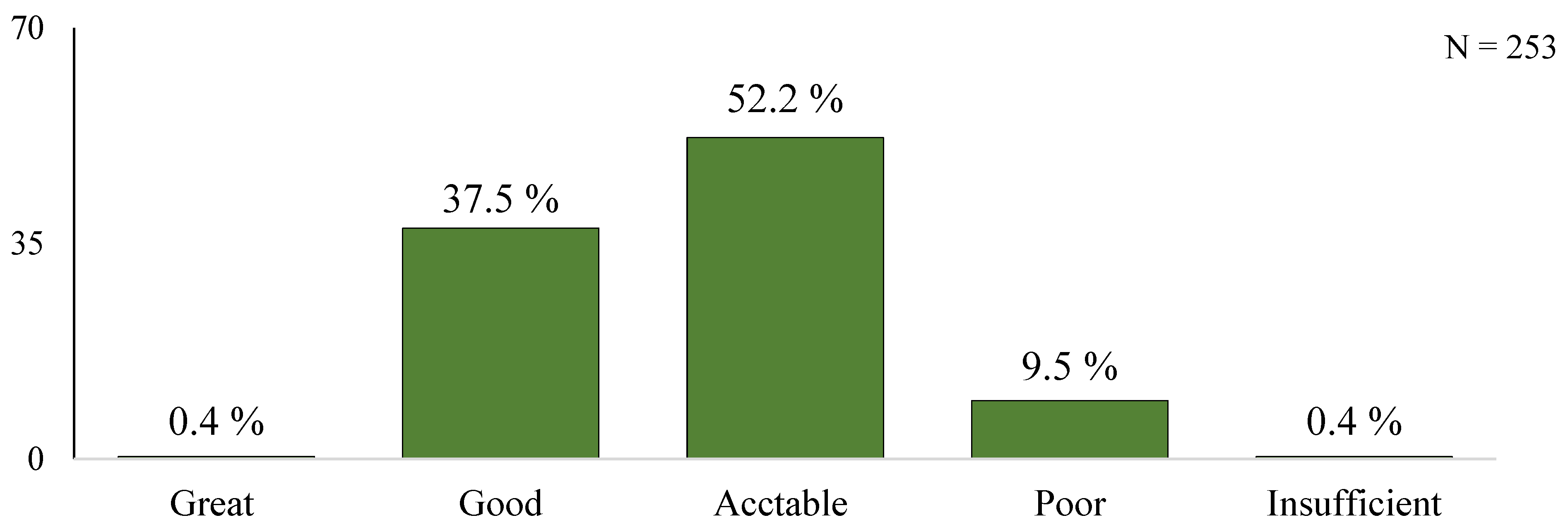
| KNOWLEDGE LEVEL | SCORE | n | % |
|---|---|---|---|
| Great | 93–84 | 1 | 0.4 |
| Good | 83–66 | 95 | 37.5 |
| Acceptable | 65–47 | 132 | 52.2 |
| Poor | 46–28 | 24 | 9.5 |
| Insufficient | <27 | 1 | 0.4 |
| DOMAIN | 3 Points Scored | 1 Point Scored | 0 Points Scored | n |
|---|---|---|---|---|
| Health status | 940 | 617 | 214 | 1771 |
| Risk factors | 592 | 555 | 118 | 1265 |
| Exercise | 1151 | 468 | 152 | 1771 |
| Nutrition | 868 | 542 | 361 | 1771 |
| Psychosocial risk | 815 | 206 | 244 | 1265 |
| N total | 4366 | 2388 | 1089 | 7843 |
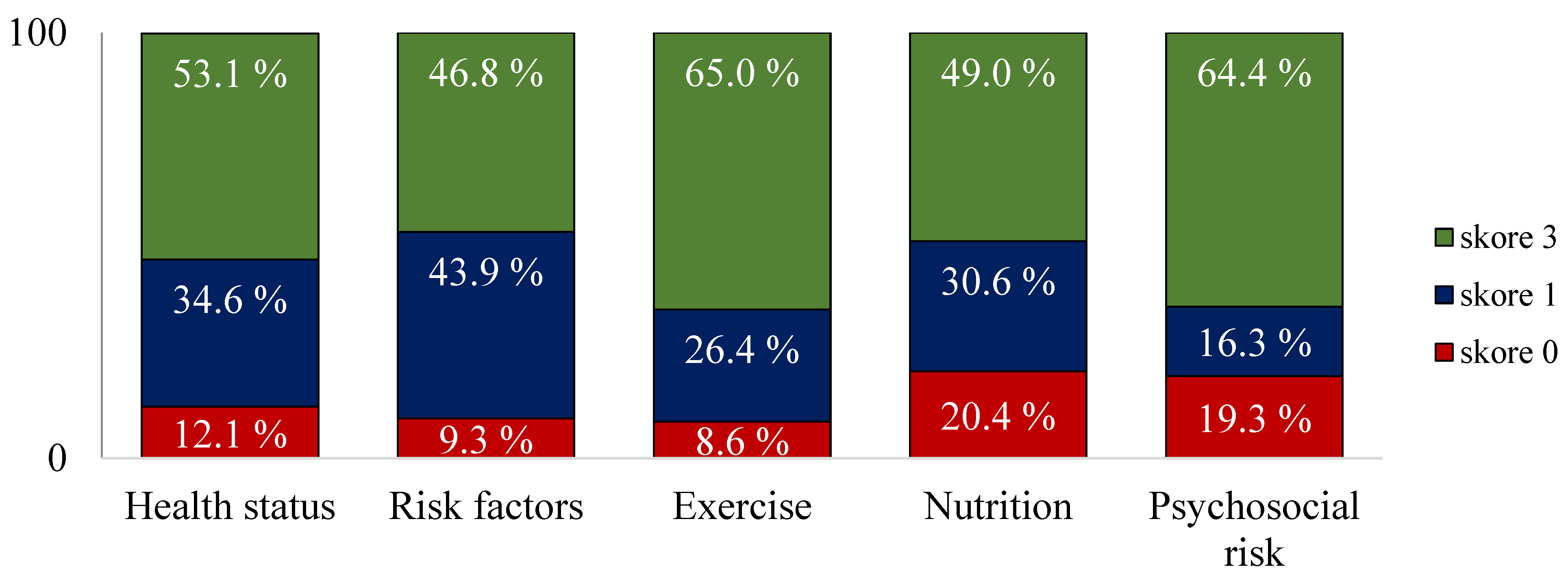
| DOMAIN | 3 Points Scored | 1 Points Scored | 0 Points Scored |
|---|---|---|---|
| Health status | 53.1% | 34.6% | 12.1% |
| Risk factors | 46.8% | 43.9% | 9.3% |
| Exercise | 65.0% | 26.4% | 8.6% |
| Nutrition | 49.0% | 30.6% | 20.4% |
| Psychosocial risk | 64.4% | 16.3% | 19.3% |
| DOMAIN | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 |
|---|---|---|---|---|---|---|---|
| Health status | 45.5% | 85.4% | 79.8% | 62.1% | 38.7% | 28.1% | 32.0% |
| Risk factors | 58.9% | 68.0% | 54.2% | 34.4% | 18.6% | ||
| Exercise | 80.2% | 55.7% | 81.0% | 44.7% | 68.0% | 65.6% | 59.7% |
| Nutrition | 71.1% | 18.6% | 78.7% | 71.1% | 85.0% | 1.6% | 17.0% |
| Psychosocial risk | 66.0% | 69.2% | 80.6% | 54.5% | 51.8% |
| DOMAIN | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | SCORE |
|---|---|---|---|---|---|---|---|---|
| Health status | 1.72 | 2.64 | 2.53 | 2.22 | 1.76 | 1.43 | 1.25 | 13.55/21 |
| Risk factors | 2.17 | 2.29 | 2.03 | 1.4 | 1.3 | 9.19/15 | ||
| Exercise | 2.53 | 2.0 | 2.58 | 1.76 | 2.24 | 2.3 | 2.05 | 15.46/21 |
| Nutrition | 2.37 | 0.68 | 2.51 | 2.36 | 2.65 | 0.97 | 0.85 | 12.39/21 |
| Psychosocial risk | 2.28 | 2.19 | 2.45 | 1.8 | 1.74 | 10.46/15 | ||
| N = 253 | 61.05/93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bálint, G.; Slezáková, Z. Evaluation of Secondary Prevention Knowledge in Patients with Coronary Artery Disease. Medicina 2025, 61, 693. https://doi.org/10.3390/medicina61040693
Bálint G, Slezáková Z. Evaluation of Secondary Prevention Knowledge in Patients with Coronary Artery Disease. Medicina. 2025; 61(4):693. https://doi.org/10.3390/medicina61040693
Chicago/Turabian StyleBálint, Gabriel, and Zuzana Slezáková. 2025. "Evaluation of Secondary Prevention Knowledge in Patients with Coronary Artery Disease" Medicina 61, no. 4: 693. https://doi.org/10.3390/medicina61040693
APA StyleBálint, G., & Slezáková, Z. (2025). Evaluation of Secondary Prevention Knowledge in Patients with Coronary Artery Disease. Medicina, 61(4), 693. https://doi.org/10.3390/medicina61040693