
Accuracy and Safety Between Robot-Assisted and Conventional Freehand Fluoroscope-Assisted Placement of Pedicle Screws in Thoracolumbar Spine: Meta-Analysis

 , ,
, ,  and
and
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Protocol Registration
2.4. Screening and Full-Text Review
2.5. Data Extraction
2.6. Risk-of-Bias Assessment
2.7. Statistical Analysis
3. Results
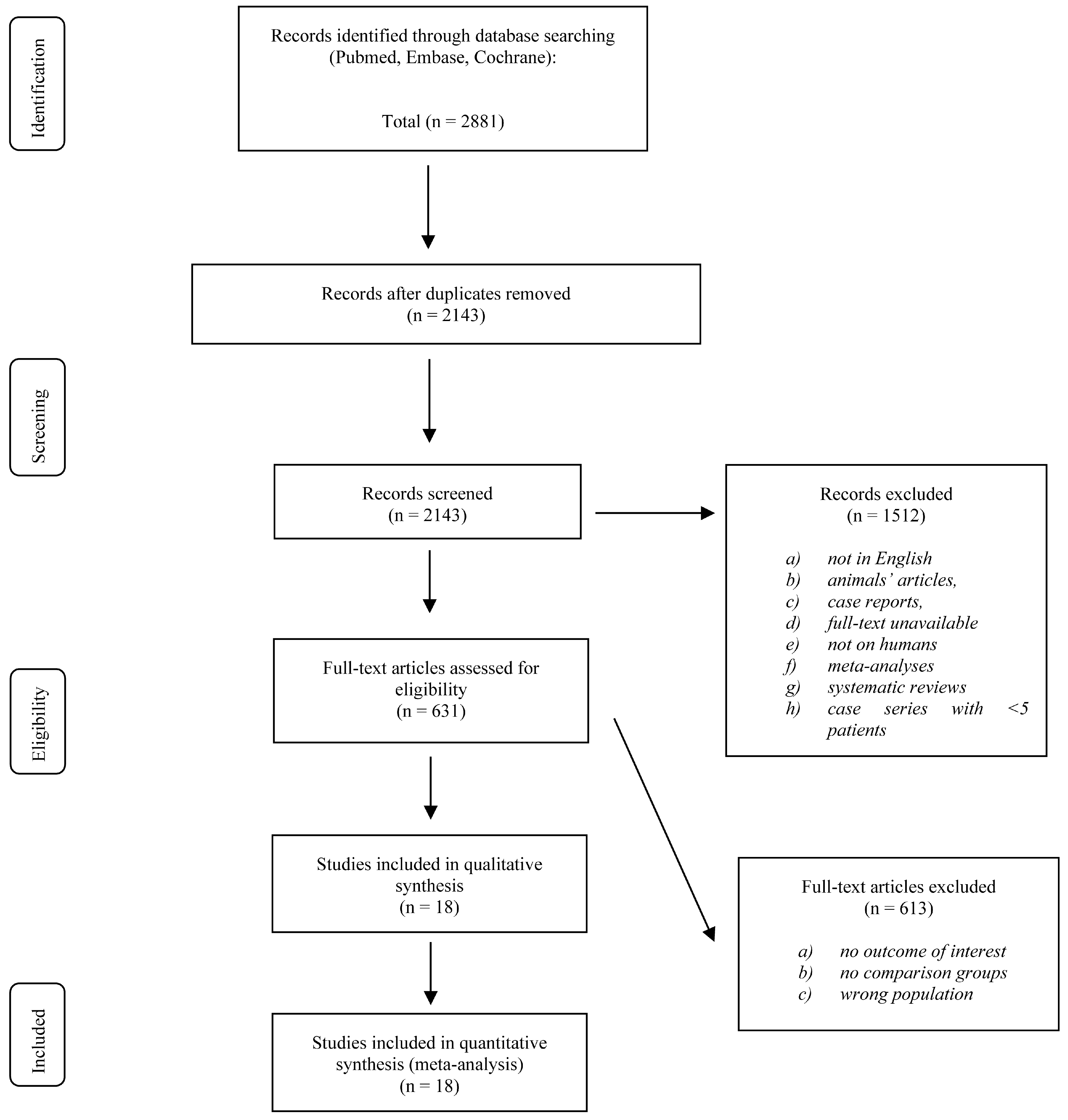
3.1. Literature Search
3.2. Study Characteristics and Quality
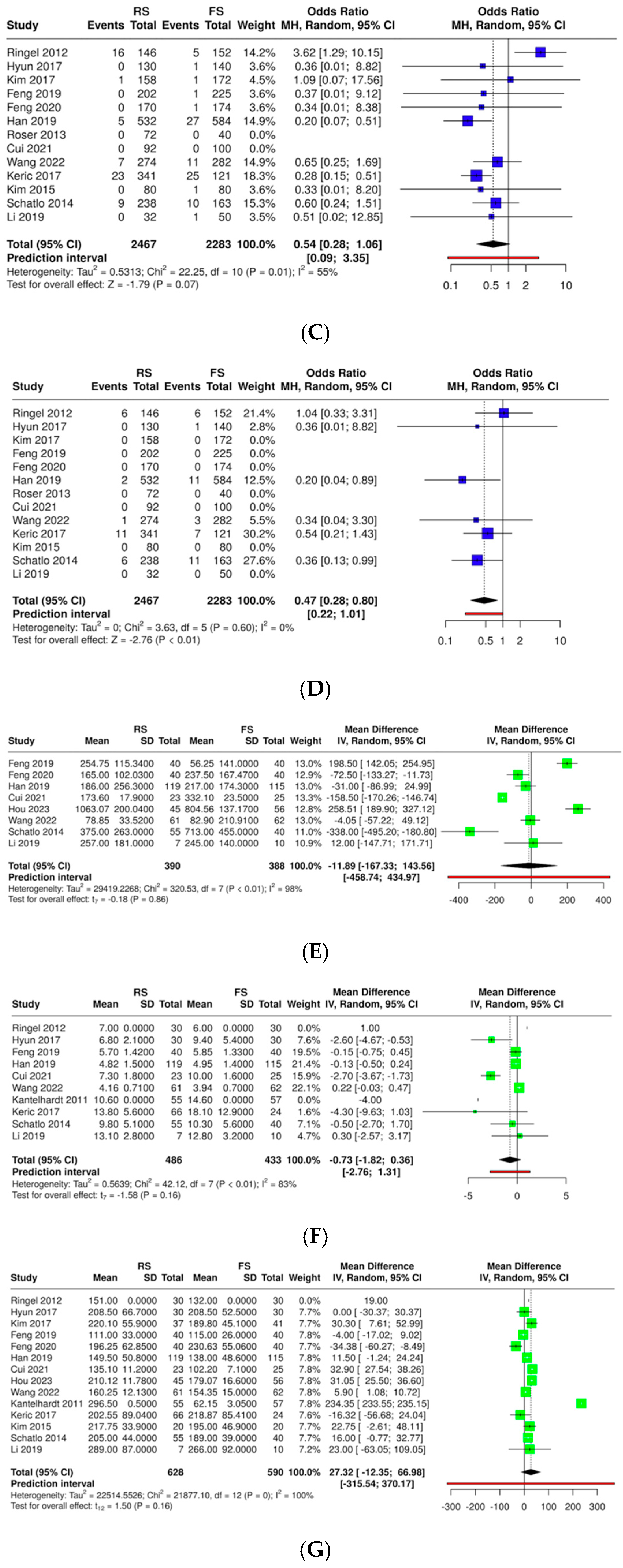
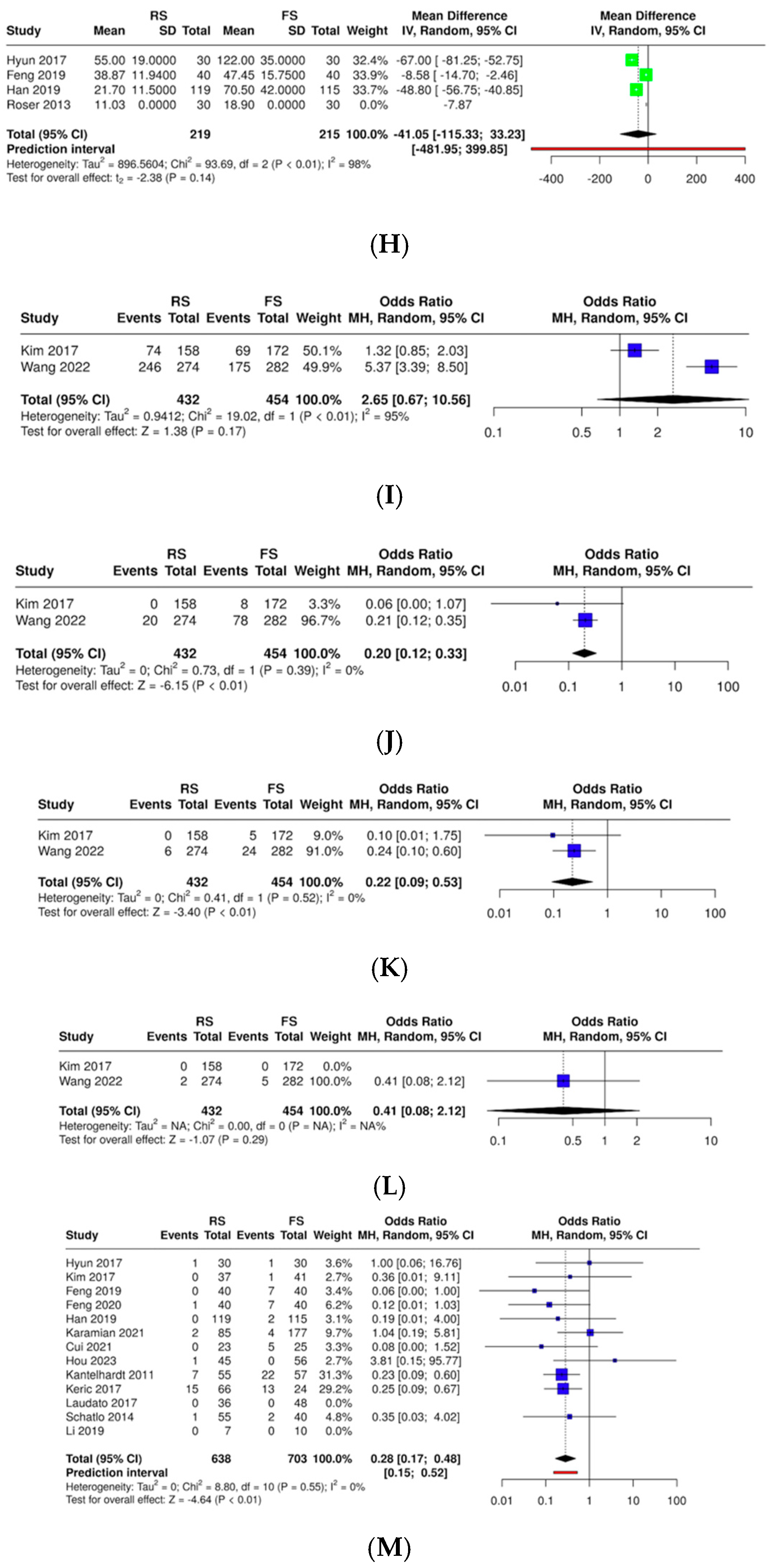
3.3. Quantitative Results (Figure 2)
- ▪
- Screw accuracy of pedicle screw position (A)
- ▪
- Screw accuracy of pedicle screw position (B)
- ▪
- Screw accuracy of pedicle screw position (C)
- ▪
- Screw accuracy of pedicle screw position (D–E)
- ▪
- Intraoperative blood loss
- ▪
- Hospital stays
- ▪
- Operation time
- ▪
- Radiation dose exposure
- ▪
- Superior facet joint violation
- ▪
- Total complications

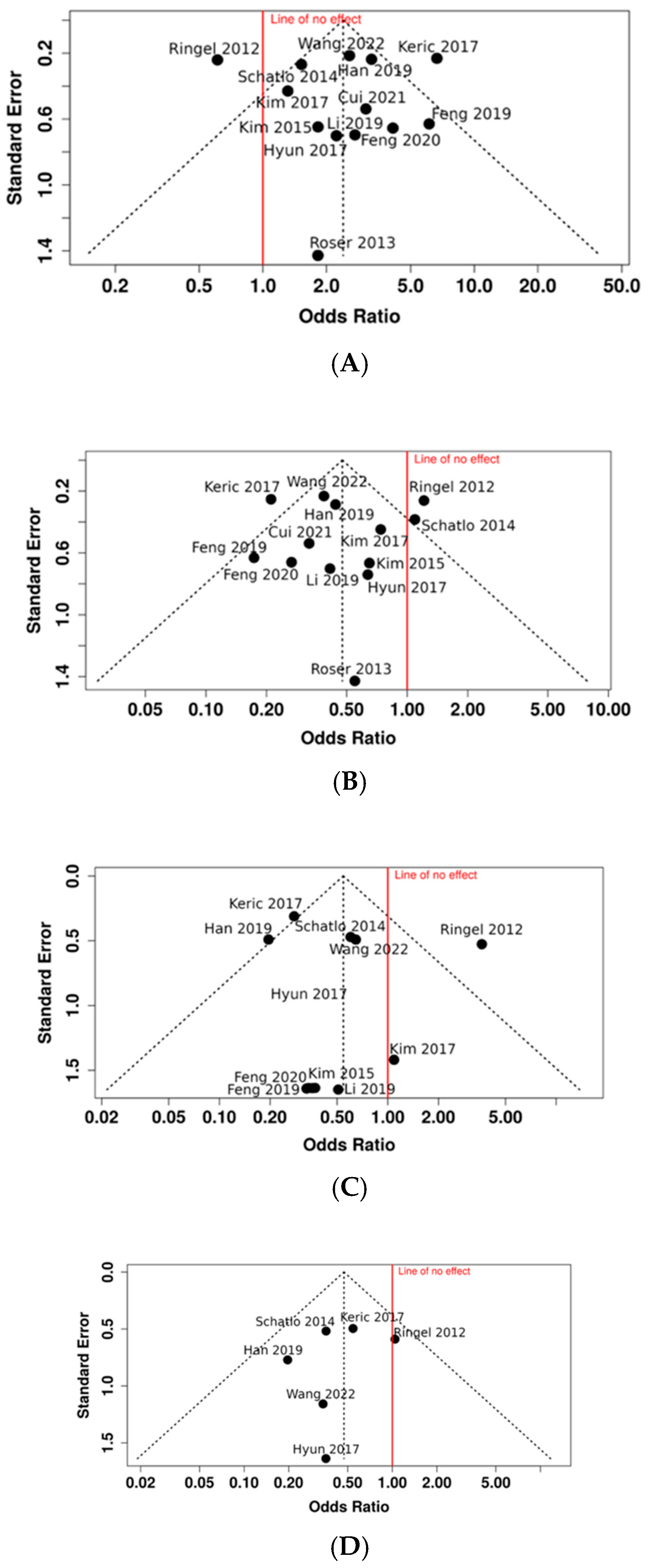
3.4. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations and Acronyms
| RS | robotic-assisted surgery |
| FS | fluoroscopy-assisted surgery |
| FJV | superior facet joint violation |
| LoH | length of hospitalization |
| VAS | Visual Analog Scale |
| ODI | Oswestry Disability Index |
References
- Maddern, G. The Australian Safety and Efficacy Register of New Interventional Procedures-Surgical (ASERNIP-S) assesses new surgeries. Aust. Health Rev. 2004, 28, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Swann, M.C.; Hoes, K.S.; Aoun, S.G.; McDonagh, D.L. Postoperative complications of spine surgery. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 103–120. [Google Scholar] [CrossRef]
- Lange, N.; Stadtmüller, T.; Scheibel, S.; Reischer, G.; Wagner, A.; Meyer, B.; Gempt, J. Analysis of risk factors for perioperative complications in spine surgery. Sci. Rep. 2022, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Petrone, S.; Ajello, M.; Marengo, N.; Bozzaro, M.; Pesaresi, A.; Allevi, M.; Fiumefreddo, A.; Denegri, F.; Cogoni, M.; Garnero, A.; et al. Clinical outcomes, MRI evaluation and predictive factors of indirect decompression with lateral transpsoas approach for lumbar interbody fusion: A multicenter experience. Front. Surg. 2023, 10, 1158836. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Ma, X.; Ma, J.; Dong, B.; Yang, P.; Sun, Y.; Zhou, L.; Shen, J. Comparison of short-term clinical outcomes between robot-assisted and freehand pedicle screw placement in spine surgery: A meta-analysis and systematic review. J. Orthop. Surg. Res. 2023, 18, 359. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.; Paulsen, R.; Babuska, J.M.; Rajpal, S.; Burneikiene, S.; Nelson, E.L.; Villavicencio, A.T. The accuracy of pedicle screw placement using intraoperative image guidance systems. J. Neurosurg. Spine 2014, 20, 196–203. [Google Scholar] [CrossRef]
- Fu, W.; Tong, J.; Liu, G.; Zheng, Y.; Wang, S.; Abdelrahim, M.E.A.; Gong, S. Robot-assisted technique vs conventional freehand technique in spine surgery: A meta-analysis. Int. J. Clin. Pr. 2020, 75, e13964. [Google Scholar] [CrossRef]
- Luengo-Matos, S.; Sánchez-Gómez, L.M.; Hijas-Gómez, A.I.; García-Carpintero, E.E.; Ballesteros-Massó, R.; Polo-Desantos, M. Efficacy and safety of robotic spine surgery: Systematic review and meta-analysis. J. Orthop. Traumatol. 2022, 23, 1–12. [Google Scholar] [CrossRef]
- Yang, Z.; Sun, Y.; Deng, C.; Dong, X.; Hao, L. Comparative efficacy of robotic-assisted and freehand techniques for pedicle screw placement in spinal disorders: A meta-analysis and systematic review. J. Robot. Surg. 2024, 18, 1–11. [Google Scholar] [CrossRef]
- Siccoli, A.; Klukowska, A.M.; Schröder, M.L.; Staartjes, V.E. A Systematic Review and Meta-Analysis of Perioperative Parameters in Robot-Guided, Navigated, and Freehand Thoracolumbar Pedicle Screw Instrumentation. World Neurosurg. 2019, 127, 576–587.e5. [Google Scholar] [CrossRef]
- Han, X.; Tian, W.; Liu, Y.; Liu, B.; He, D.; Sun, Y.; Han, X.; Fan, M.; Zhao, J.; Xu, Y.; et al. Safety and accuracy of robot-assisted versus fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery: A prospective randomized controlled trial. J. Neurosurg. Spine 2019, 30, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Veronese, N.; Nottegar, A.; Shin, J.I.; Gentile, G.; Granziol, U.; Soysal, P.; Alexinschi, O.; Smith, L.; Solmi, M. Assessing the quality of studies in meta-research: Review/guidelines on the most important quality assessment tools. Pharm. Stat. 2021, 20, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of Pedicular Screw Placement In Vivo. Spine (Phila Pa 1976) 1990, 15, 11–14. [Google Scholar] [CrossRef]
- Babu, R.; Park, J.G.; Mehta, A.I.; Shan, T.; Grossi, P.M.; Brown, C.R.; Richardson, W.J.; Isaacs, R.E.; Bagley, C.A.; Kuchibhatla, M.; et al. Comparison of Superior-Level Facet Joint Violations During Open and Percutaneous Pedicle Screw Placement. Neurosurgery 2012, 71, 962–970. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Kantelhardt, S.R.; Martinez, R.; Baerwinkel, S.; Burger, R.; Giese, A.; Rohde, V. Perioperative course and accuracy of screw positioning in conventional, open robotic-guided and percutaneous robotic-guided, pedicle screw placement. Eur. Spine J. 2011, 20, 860–868. [Google Scholar] [CrossRef]
- Roser, F.; Tatagiba, M.; Maier, G. Spinal robotics: Current applications and future perspectives. Neurosurgery 2013, 72 (Suppl. S1), 12–18. [Google Scholar] [CrossRef]
- Keric, N.; Eum, D.J.; Afghanyar, F.; Rachwal-Czyzewicz, I.; Renovanz, M.; Conrad, J.; Wesp, D.M.; Kantelhardt, S.R.; Giese, A. Evaluation of surgical strategy of conventional vs. percutaneous robot-assisted spinal trans-pedicular instrumentation in spondylodiscitis. J. Robot. Surg. 2017, 11, 17–25. [Google Scholar] [CrossRef]
- Li, Z.; Chen, J.; Zhu, Q.A.; Zheng, S.; Zhong, Z.; Yang, J.; Yang, D.; Jiang, H.; Jiang, W.; Zhu, Y.; et al. A preliminary study of a novel robotic system for pedicle screw fixation: A randomised controlled trial. J. Orthop. Translat. 2019, 20, 73–79. [Google Scholar] [CrossRef]
- Laudato, P.A.; Pierzchala, K.; Schizas, C. Pedicle Screw Insertion Accuracy Using O-Arm, Robotic Guidance, or Freehand Technique: A Comparative Study. Spine 2018, 43, E373–E378. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Tian, W.; Sun, Y.; Liu, Y.; Wei, Y. Effect of Robot-Assisted Surgery on Lumbar Pedicle Screw Internal Fixation in Patients with Osteoporosis. World Neurosurg. 2019, 125, e1057–e1062. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Tian, W.; Wei, Y. Clinical Effects of Oblique Lateral Interbody Fusion by Conventional Open versus Percutaneous Robot-Assisted Minimally Invasive Pedicle Screw Placement in Elderly Patients. Orthop. Surg. 2020, 12, 86–93. [Google Scholar] [CrossRef]
- Wang, L.; Li, C.; Wang, Z.; Li, D.; Tian, Y.; Yuan, S.; Liu, X. Comparison of robot-assisted versus fluoroscopy-assisted minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar spinal diseases: 2-year follow-up. J. Robot. Surg. 2022, 17, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.J.; Kim, K.J.; Jahng, T.A.; Kim, H.J. Minimally Invasive Robotic Versus Open Fluoroscopic-guided Spinal Instrumented Fusions. Spine 2017, 42, 353–358. [Google Scholar] [CrossRef]
- Ringel, F.; Stüer, C.; Reinke, A.; Preuss, A.; Behr, M.; Auer, F.; Stoffel, M.; Meyer, B. Accuracy of Robot-Assisted Placement of Lumbar and Sacral Pedicle Screws. Spine 2012, 37, E496–E501. [Google Scholar] [CrossRef]
- Hou, C.; Yang, H.; Chen, Y.; Yang, Y.; Zhang, B.; Chen, K.; Li, M.; Yang, M.; Chen, K. Comparison of robot versus fluoroscopy-assisted pedicle screw instrumentation in adolescent idiopathic scoliosis surgery: A retrospective study. Front. Surg. 2023, 9, 1085580. [Google Scholar] [CrossRef]
- Cui, G.; Han, X.; Wei, Y.; Liu, Y.; He, D.; Sun, Y.; Liu, B.; Tian, W. Robot-Assisted Minimally Invasive Transforaminal Lumbar Interbody Fusion in the Treatment of Lumbar Spondylolisthesis. Orthop. Surg. 2021, 13, 1960–1968. [Google Scholar] [CrossRef]
- Schatlo, B.; Molliqaj, G.; Cuvinciuc, V.; Kotowski, M.; Schaller, K.; Tessitore, E. Safety and accuracy of robot-assisted versus fluoroscopy-guided pedicle screw insertion for degenerative diseases of the lumbar spine: A matched cohort comparison. J. Neurosurg. Spine 2014, 20, 636–643. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, S.H.; Chang, B.S.; Lee, C.K.; Lim, T.O.; Hoo, L.P.; Yi, J.M.; Yeom, J.S. Monitoring the Quality of Robot-Assisted Pedicle screw fixation in the lumbar spine by using a cumulative summation test. Spine 2015, 40, 87–94. [Google Scholar] [CrossRef]
- Kim, H.-J.; Jung, W.-I.; Chang, B.-S.; Lee, C.-K.; Kang, K.-T.; Yeom, J.S. A prospective, randomized, controlled trial of robot—Assisted vs freehand pedicle screw fixation in spine surgery. Int. J. Med. Robot. 2017, 13. [Google Scholar] [CrossRef] [PubMed]
- Karamian, B.A.; DiMaria, S.L.; Sawires, A.N.; Canseco, J.A.; Basques, B.A.; Toci, G.R.; Radcliff, K.E.; Rihn, J.A.; Kaye, I.D.; Hilibrand, A.S.; et al. Clinical Outcomes of Robotic Versus Freehand Pedicle Screw Placement After One-to Three-Level Lumbar Fusion. Glob. Spine J. 2021, 13, 1871–1877. [Google Scholar] [CrossRef]
- Chizas, C.S.; Hein, E.T.; Barbara, K.; Ulik, G.K. Pedicle screw insertion: Robotic assistance versus conventional C-arm fluoroscopy. Acta Orthop. Belg. 2012, 78, 240–245. [Google Scholar]
- Wang, X.; Liu, H.-C.; Ma, Y.-H.; Zhu, Q.-S.; Zhu, Y.-H. Effectiveness and safety of robot-assisted minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar spinal diseases: A systematic review and meta-analysis. J. Robot. Surg. 2024, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, H.X.; Zhu, Q.S.; Zhu, Y.H. Effectiveness and safety of robot-assisted versus fluoroscopy-assisted pedicle screw implantation in scoliosis surgery: A systematic review and meta-analysis. Neurosurg. Rev. 2024, 47, 108. [Google Scholar] [CrossRef]
- Han, X.; Tang, G.; Xing, Y.; Zhang, Q.; He, D.; Tian, W. Comparison of Outcomes between Robot-Assisted Minimally Invasive Transforaminal Lumbar Interbody Fusion and Oblique Lumbar Interbody Fusion in Single-Level Lumbar Spondylolisthesis. Orthop. Surg. 2021, 13, 2093–2101. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2013834383&from=export (accessed on 4 January 2025). [CrossRef]
- Li, C.; Li, W.; Gao, S.; Cao, C.; Li, C.; He, L.; Ma, X.; Li, M. Comparison of accuracy and safety between robot-assisted and conventional fluoroscope assisted placement of pedicle screws in thoracolumbar spine. Medicine 2021, 100, e27282. [Google Scholar] [CrossRef]
- MacLean, L.; Hersh, A.M.; Bhimreddy, M.; Jiang, K.; Davidar, A.D.; Weber-Levine, C.; Alomari, S.; Judy, B.F.; Lubelski, D.; Theodore, N. Comparison of accuracy, revision, and perioperative outcomes in robot-assisted spine surgeries: Systematic review and meta-analysis. J. Neurosurg. Spine 2024, 41, 519–531. [Google Scholar] [CrossRef]
- Marengo, N.; Pecoraro, F.; Bue, E.L.; Colonna, S.; Panico, F.; Morello, A.; Ajello, M.; Zenga, F.; Garbossa, D.; Cofano, F. Enabling technology with minimally invasive strategies: Robot-assisted Cortical Bone Trajectory screws fixation in lateral transpsoas interbody fusion. World Neurosurg. 2025, 123890. [Google Scholar] [CrossRef]
- Colonna, S.; Ajello, M.; Lo Bue, E.; Panico, F.; Saaid, A.; Mai, G.; Fiumefreddo, A.; Marengo, N.; Bavaresco, E.; Zullo, N.; et al. Minimally invasive techniques in the surgical treatment of lumbar degenerative disease: A comparative study between percutaneous mis-tlif and open-tlif with cortical bone trajectory (cbt) screws. Brain Spine 2024, 4, 103643. Available online: https://www.sciencedirect.com/science/article/pii/S2772529424008993 (accessed on 4 January 2025). [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morello, A.; Colonna, S.; Lo Bue, E.; Chiari, G.; Mai, G.; Pesaresi, A.; Garbossa, D.; Cofano, F. Accuracy and Safety Between Robot-Assisted and Conventional Freehand Fluoroscope-Assisted Placement of Pedicle Screws in Thoracolumbar Spine: Meta-Analysis. Medicina 2025, 61, 690. https://doi.org/10.3390/medicina61040690
Morello A, Colonna S, Lo Bue E, Chiari G, Mai G, Pesaresi A, Garbossa D, Cofano F. Accuracy and Safety Between Robot-Assisted and Conventional Freehand Fluoroscope-Assisted Placement of Pedicle Screws in Thoracolumbar Spine: Meta-Analysis. Medicina. 2025; 61(4):690. https://doi.org/10.3390/medicina61040690
Chicago/Turabian StyleMorello, Alberto, Stefano Colonna, Enrico Lo Bue, Giulia Chiari, Giada Mai, Alessandro Pesaresi, Diego Garbossa, and Fabio Cofano. 2025. "Accuracy and Safety Between Robot-Assisted and Conventional Freehand Fluoroscope-Assisted Placement of Pedicle Screws in Thoracolumbar Spine: Meta-Analysis" Medicina 61, no. 4: 690. https://doi.org/10.3390/medicina61040690
APA StyleMorello, A., Colonna, S., Lo Bue, E., Chiari, G., Mai, G., Pesaresi, A., Garbossa, D., & Cofano, F. (2025). Accuracy and Safety Between Robot-Assisted and Conventional Freehand Fluoroscope-Assisted Placement of Pedicle Screws in Thoracolumbar Spine: Meta-Analysis. Medicina, 61(4), 690. https://doi.org/10.3390/medicina61040690