
The Clinical Utility of Serum Alpha-1-Acid Glycoprotein in Reflecting the Cross-Sectional Activity of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Centre Retrospective Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Data
2.3. Measurement of AGP
2.4. Statistical Analyses
3. Results
3.1. Characteristics
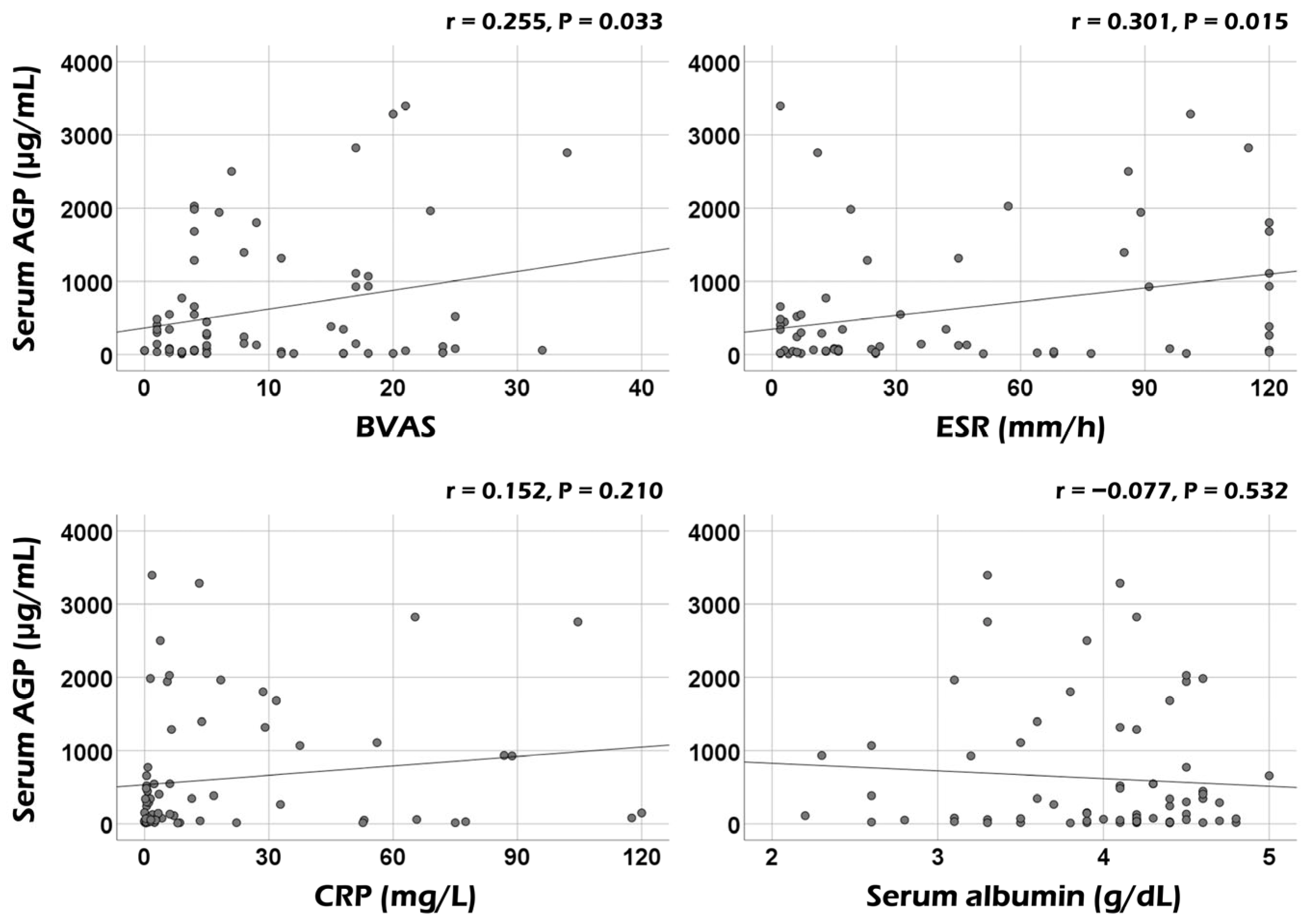
3.2. Correlation Analysis
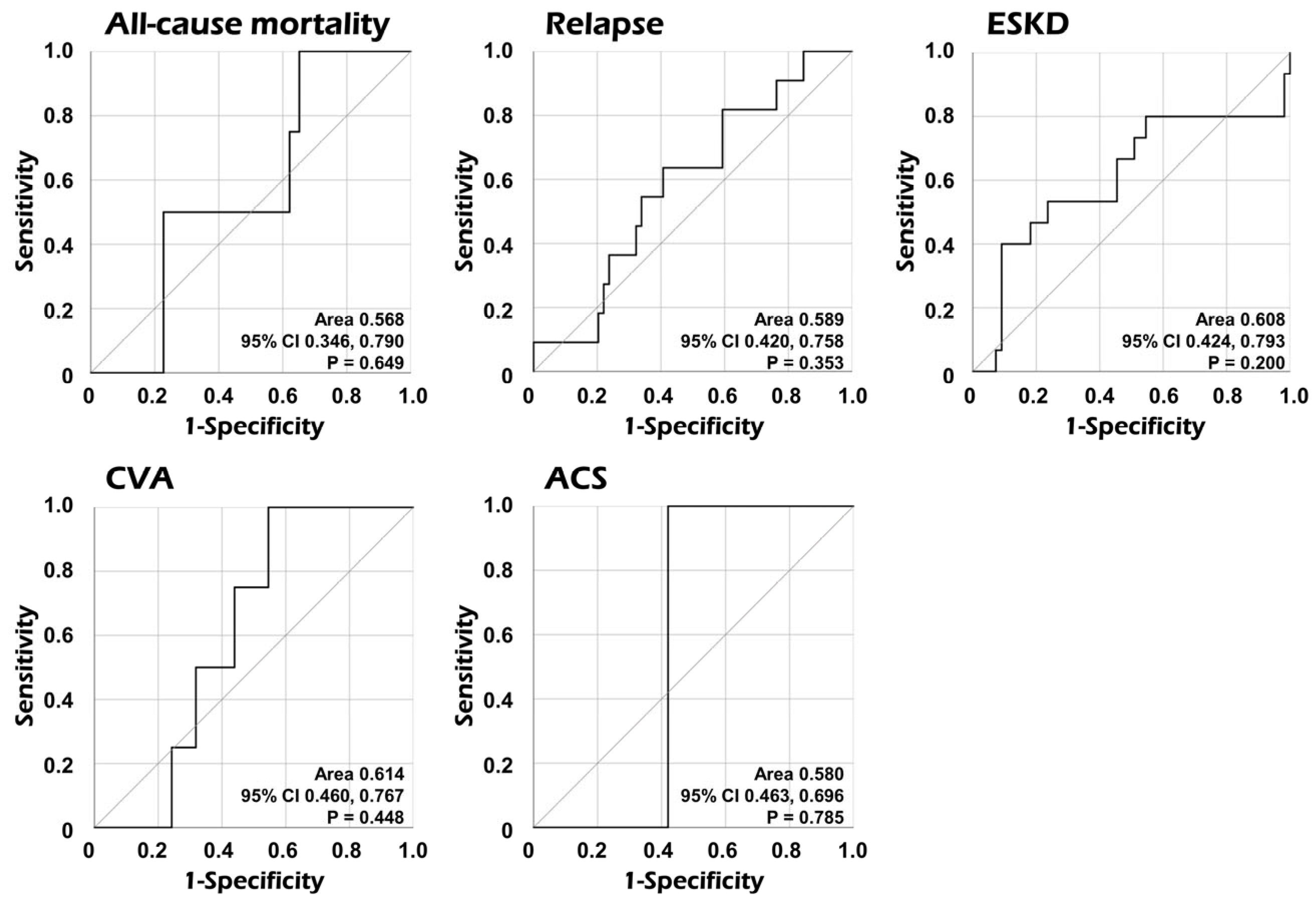
3.3. AUC of Serum AGP for Poor Outcomes
3.4. Cox Proportional Hazards Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheumatol. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, R.; Robson, J.C.; Grayson, P.C.; Ponte, C.; Craven, A.; Khalid, S.; Judge, A.; Hutchings, A.; Merkel, P.A.; Luqmani, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis. Ann. Rheum. Dis. 2022, 81, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Robson, J.C.; Grayson, P.C.; Ponte, C.; Suppiah, R.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Watts, R.A.; Merkel, P.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Ann. Rheum. Dis. 2022, 81, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, J.C.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Luqmani, R.A.; Watts, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann. Rheum. Dis. 2022, 81, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.Y.; Lee, L.E.; Park, Y.B.; Lee, S.W. Comparison of the 2022 ACR/EULAR Classification Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Previous Criteria. Yonsei Med. J. 2023, 64, 11–17. [Google Scholar] [CrossRef]
- Ahn, S.S.; Park, Y.B.; Lee, S.W. Serological Biomarkers and Indices for the Current Activity and Prognosis of ANCA-Associated Vasculitis: Experience in a Single Centre in Korea. Yonsei Med. J. 2021, 62, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Pagnoux, C.; Seror, R.; Mahr, A.; Mouthon, L.; Toumelin, P.L.; French Vasculitis Study Group (FVSG). The Five-Factor Score revisited: Assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine 2011, 90, 19–27. [Google Scholar] [CrossRef]
- Fournier, T.; Medjoubi-N, N.; Porquet, D. Alpha-1-acid glycoprotein. Biochim. Biophys. Acta 2000, 1482, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Ceciliani, F.; Lecchi, C. The Immune Functions of α1 Acid Glycoprotein. Curr. Protein Pept. Sci. 2019, 20, 505–524. [Google Scholar] [CrossRef] [PubMed]
- Hochepied, T.; Berger, F.G.; Baumann, H.; Libert, C. Alpha(1)-acid glycoprotein: An acute phase protein with inflammatory and immunomodulating properties. Cytokine Growth Factor. Rev. 2003, 14, 25–34. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Shipley, M.J.; Bell, J.A.; Canonico, M.; Elbaz, A.; Kivimäki, M. Association between inflammatory biomarkers and all-cause, cardiovascular and cancer-related mortality. CMAJ 2017, 189, E384–E390. [Google Scholar] [CrossRef] [PubMed]
- Ayyub, A.; Saleem, M.; Fatima, I.; Tariq, A.; Hashmi, N.; Musharraf, S.G. Glycosylated Alpha-1-acid glycoprotein 1 as a potential lung cancer serum biomarker. Int. J. Biochem. Cell Biol. 2016, 70, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Yokobori, T.; Yazawa, S.; Asao, T.; Nakazawa, N.; Mogi, A.; Sano, R.; Kuwano, H.; Kaira, K.; Shirabe, K. Fucosylated α1-acid glycoprotein as a biomarker to predict prognosis following tumor immunotherapy of patients with lung cancer. Sci. Rep. 2019, 9, 14503. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, S.Y.; Lai, Y.R.; Kung, C.T.; Tsai, N.W.; Su, C.M.; Huang, C.C.; Wang, H.C.; Cheng, B.C.; Su, Y.J.; Lin, W.C.; et al. α-1-Acid Glycoprotein Concentration as an Outcome Predictor in Adult Patients with Sepsis. Biomed. Res. Int. 2019, 2019, 3174896. [Google Scholar] [CrossRef] [PubMed]
- Chapelle, J.P.; Albert, A.; Smeets, J.P.; Heusghem, C.; Kulbertus, H.E. The prognostic significance of serum alpha 1-acid glycoprotein changes in acute myocardial infarction. Clin. Chim. Acta 1981, 115, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Park, P.G.; Song, J.J.; Park, Y.B.; Lee, S.W. Clinical application of low erythrocyte sedimentation rate/high C-reactive protein to antineutrophil cytoplasmic antibody-associated vasculitis. J. Clin. Lab. Anal. 2022, 36, e24237. [Google Scholar] [CrossRef] [PubMed]
- Vasson, M.P.; Baguet, J.C.; Arveiller, M.R.; Bargnoux, P.J.; Giroud, J.P.; Raichvarg, D. Serum and urinary alpha-1 acid glycoprotein in chronic renal failure. Nephron 1993, 65, 299–303. [Google Scholar] [CrossRef]
- Watanabe, H.; Fujimura, R.; Hiramoto, Y.; Murata, R.; Nishida, K.; Bi, J.; Imafuku, T.; Komori, H.; Maeda, H.; Mukunoki, A.; et al. An acute phase protein α1-acid glycoprotein mitigates AKI and its progression to CKD through its anti-inflammatory action. Sci. Rep. 2021, 11, 7953. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| At diagnosis | |
| Demographic data | |
| Age (years) | 63.0 (52.0–72.3) |
| Male sex (N, (%)) | 29 (41.4) |
| Female sex (N, (%)) | 41 (58.6) |
| Ex-smoker (N, (%)) | 2 (2.9) |
| Body mass index (kg/m2) | 224 (20.8–24.7) |
| AAV subtypes (N, (%)) | |
| MPA | 35 (50.0) |
| GPA | 20 (28.6) |
| EGPA | 15 (21.4) |
| ANCA titres and positivity (N, (%)) | |
| MPO-ANCA (or P-ANCA) titre | 0 (0–32.5) |
| PR3-ANCA (or C-ANCA) titre | 0 (0–0) |
| MPO-ANCA (or P-ANCA)-positive | 40 (57.1) |
| PR3-ANCA (or C-ANCA)-positive | 11 (15.7) |
| Both ANCA-positive | 2 (2.9) |
| ANCA-negative | 21 (30.0) |
| AAV-specific indices | |
| BVAS | 5.0 (3.0–17.0) |
| FFS | 0 (0–1.0) |
| Comorbidities (N, (%)) | |
| Type 2 diabetes mellitus | 14 (20.0) |
| Hypertension | 23 (32.9) |
| Dyslipidaemia | 11 (15.7) |
| Acute-phase reactants | |
| ESR (mm/h) | 23.0 (6.5–81.0) |
| CRP (mg/L) | 3.4 (0.7–23.8) |
| Laboratory results | |
| White blood cell count (/mm3) | 7495.0 (5930.0–10,485.0) |
| Haemoglobin (g/dL) | 12.0 (10.2–13.6) |
| Platelet count (×1000/mm3) | 248.0 (191.5–352.5) |
| Blood urea nitrogen (mg/dL) | 18.7 (12.9–28.6) |
| Serum creatinine (mg/dL) | 0.8 (0.6–1.6) |
| Total serum protein (g/dL) | 6.8 (6.4–7.3) |
| Serum albumin (g/dL) | 4.2 (3.6–4.4) |
| Serum AGP (μg/mL) | 150.9 (41.6–929.6) |
| During follow-up | |
| Poor outcomes (N, (%)) | |
| All-cause mortality | 4 (5.7) |
| Relapse | 11 (15.7) |
| ESKD | 15 (21.4) |
| CVA | 4 (5.7) |
| ACS | 1 (1.4) |
| Follow-up duration based on each poor outcome (months) | |
| All-cause mortality | 26.7 (12.3–45.9) |
| Relapse | 22.4 (7.9–32.5) |
| ESKD | 26.4 (9.2–45.9) |
| CVA | 26.6 (11.9–43.1) |
| ACS | 26.6 (12.1–43.1) |
| Medications (N, (%)) | |
| Glucocorticoids | 69 (98.6) |
| Cyclophosphamide | 45 (64.3) |
| Rituximab | 15 (21.4) |
| Mycophenolate mofetil | 19 (27.1) |
| Azathioprine | 42 (60.0) |
| Tacrolimus | 6 (8.6) |
| Methotrexate | 3 (4.3) |
| Acute-Phase Reactants | Poor Outcomes | Univariable | ||
|---|---|---|---|---|
| HR | 95% CI | p Value | ||
| Serum AGP | All-cause mortality | 1.000 | 0.999, 1.001 | 0.840 |
| Relapse | 1.000 | 1.000, 1.001 | 0.639 | |
| ESKD | 1.000 | 1.000, 1.001 | 0.175 | |
| CVA | 1.000 | 0.998, 1.001 | 0.741 | |
| ACS | 0.999 | 0.996, 1.003 | 0.759 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.; Yoon, T.; Park, Y.-B.; Ahn, S.S.; Lee, S.-W. The Clinical Utility of Serum Alpha-1-Acid Glycoprotein in Reflecting the Cross-Sectional Activity of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Centre Retrospective Study. Medicina 2024, 60, 1212. https://doi.org/10.3390/medicina60081212
Yoo J, Yoon T, Park Y-B, Ahn SS, Lee S-W. The Clinical Utility of Serum Alpha-1-Acid Glycoprotein in Reflecting the Cross-Sectional Activity of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Centre Retrospective Study. Medicina. 2024; 60(8):1212. https://doi.org/10.3390/medicina60081212
Chicago/Turabian StyleYoo, Juyoung, Taejun Yoon, Yong-Beom Park, Sung Soo Ahn, and Sang-Won Lee. 2024. "The Clinical Utility of Serum Alpha-1-Acid Glycoprotein in Reflecting the Cross-Sectional Activity of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Centre Retrospective Study" Medicina 60, no. 8: 1212. https://doi.org/10.3390/medicina60081212
APA StyleYoo, J., Yoon, T., Park, Y.-B., Ahn, S. S., & Lee, S.-W. (2024). The Clinical Utility of Serum Alpha-1-Acid Glycoprotein in Reflecting the Cross-Sectional Activity of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Centre Retrospective Study. Medicina, 60(8), 1212. https://doi.org/10.3390/medicina60081212