Abstract
Background and Objectives: Patients presenting with ST Elevation Myocardial Infarction (STEMI) due to occlusive coronary arteries remain at a higher risk of excess morbidity and mortality despite being treated with primary percutaneous coronary intervention (PPCI). Identifying high-risk patients is prudent so that close monitoring and timely interventions can improve outcomes. Materials and Methods: A cohort of 605 STEMI patients [64.2 ± 13.2 years, 432 (71.41%) males] treated with PPCI were recruited. Their arterial pressure (AP) wave recorded throughout the PPCI procedure was analyzed to extract features to predict 1-year mortality. After denoising and extracting features, we developed two distinct feature selection strategies. The first strategy uses linear discriminant analysis (LDA), and the second employs principal component analysis (PCA), with each method selecting the top five features. Then, three machine learning algorithms were employed: LDA, K-nearest neighbor (KNN), and support vector machine (SVM). Results: The performance of these algorithms, measured by the area under the curve (AUC), ranged from 0.73 to 0.77, with accuracy, specificity, and sensitivity ranging between 68% and 73%. Moreover, we extended the analysis by incorporating demographics, risk factors, and catheterization information. This significantly improved the overall accuracy and specificity to more than 76% while maintaining the same level of sensitivity. This resulted in an AUC greater than 0.80 for most models. Conclusions: Machine learning algorithms analyzing hemodynamic traces in STEMI patients identify high-risk patients at risk of mortality.
1. Introduction
Myocardial infarction (MI), or a heart attack, is one of the leading causes of death worldwide [1,2]. It is estimated to result in over 4 million deaths in Europe and northern Asia and 2.4 million deaths in the United States each year [3]. In 2022, heart disease ranked as the second leading cause of death in Canada [4]. Moreover, in the USA alone, approximately USD 29.8 billion was spent on the direct management of MI in 2016 [5].
In current medical practice, MI is identified based on clinical presentation, dynamic electrocardiogram (ECG) changes, and a rise in troponin, a cardiac-specific biomarker. Patients exhibiting ST-segment elevation with reciprocal changes in ECG are diagnosed with ST elevation myocardial infarction (STEMI) [6]; that is typically because of complete occlusion of coronary arteries [7]. In comparison, patients with chest pain, a rise in troponin levels, and ECG changes other than STEMI are defined as having non-STEMI (NSTEMI). Primary percutaneous coronary intervention (PPCI) is the gold-standard care for patients with STEMI. However, this procedure is time sensitive. Hence, patients who cannot be brought to a cardiac catheter laboratory within 120 min of their first contact with medical personnel are treated with thrombolytic therapy aiming at dissolving intracoronary clots, restoring flow, and transferring them to the nearby cardiac center for further care.
Mortality and morbidity among MI patients have markedly improved over the last four decades, primarily due to proactive detection and management of cardiovascular risk factors [8], along with timely myocardial salvage by coronary revascularization [9]. Despite such success, 30-day mortality among patients admitted with MI remains between 6.5–9.3% across the European countries [10]. Data from Denmark, where all STEMI patients are treated with PPCI, demonstrated a 1-year mortality reduction from 10.8% (2003–2006) to 7.7% (2015–2018); the majority of this mortality reduction was observed within the first 30 days [11]. In addition to higher mortality, these patients may also experience complications, including life-threatening arrhythmias, heart failure, a prolonged in-hospital stay, and various mechanical complications despite successful PPCI [12,13,14]. Hence, it is prudent to identify high-risk patients who may benefit from close monitoring and timely intervention that may plausibly improve their outcomes.
Various risk assessments in the context of myocardial infarction (MI) have been developed. The Global Registry of Acute Coronary Events (GRACE) [15], the most widely used source that is recommended by the European Society of Cardiology STEMI guidelines [16], estimates the mortality risk in hospital, at 6 months, 1 year, and 3 years. The thrombolysis in myocardial infarction (TIMI) [17] risk score was initially developed for 30-day mortality in patients after thrombolysis and then validated for patients with STEMI [18]. Based on clinical and electrocardiographic characteristics, the primary angioplasty in myocardial infarction (PAMI) score is used to predict late mortality in patients with STEMI treated by PPCI [19]. The controlled used of abciximab and the investigation of device usage to lower late angioplasty complications (CADILLAC) considers the initial measurement of left ventricular function and predicts 1-year mortality [20]. Finally, the Zwolle [21] score was developed for 30-day mortality prediction.
These traditional methods for determining cardiovascular disease (CVD) risk typically presuppose a linear relationship between risk factors and clinical outcomes. However, such a linear approach might be oversimplifying their relationship. Cardiovascular diseases are inherently complex and diverse, influenced by genetic predispositions, environmental conditions, and lifestyle choices [16,22]. These approaches primarily focus on conventional prognostic factors [23], limiting their effectiveness due to the emerging need to incorporate and examine various information sources, including those describing MI-related pathophysiology. Moreover, these scoring systems are routinely not utilized in the current era of prompt coronary revascularization. Aortic pulse wave is a physiological marker describing cardiovascular health [24,25] that may provide valuable information about changing physiological status among patients undergoing PPCI.
Machine learning (ML) has the potential to bypass the restrictions of the approaches mentioned above [26]. Static assumptions about data behavior do not constrain ML data analysis and can train models to uncover patterns within the data. The application of ML, especially in predicting in-hospital mortality [27], 30-day mortality [28], short- and long-term mortality [29], arrhythmia [30], and readmission [31] has seen rapid growth. ML has been widely compared with traditional methods such as TIMI and GRACE. ML has demonstrated superior performance to traditional risk-scoring methods in mortality prediction [32,33,34,35,36]. ML outperformed the TIMI score in predicting both short- and long-term mortality [33]. Additionally, it demonstrated better outcomes for 30-day [35] and 1-year [32,34,36] mortality predictions compared to the GRACE score for patients with STEMI. Most ML algorithms have primarily employed continuous and categorical data from patients’ records during angioplasty. To the best of our knowledge, none of the previous ML research has focused on extracting features from hemodynamic traces, such as the arterial pressure (AP) signal obtained throughout the PPCI procedure.
2. Materials and Methods
2.1. Study Population and Data Acquisition
This retrospective study included 800 consecutive patients suspected to have STEMI who were referred to the St Boniface General Hospital, Winnipeg, MB, Canada, for consideration of PPCI between January 2020 and October 2021.
Patients’ demographics, cardiovascular risk factors, catheterization data and outcomes were collected by reviewing individual electronic patient records (EPRs). The arterial pressure (AP) wave tracings throughout the PPCI procedure were obtained through the MacLab system database (GE Healthcare; Milwaukee, WI, USA). Given these retrospective data analyses, individual patient consent was not obtained. This study was approved by the local Research and Ethics Board, University of Manitoba [REB: HS25542 (H2022: 196)].
During catheterization, specifically the pullback of a catheter from the left ventricle (LV) back to the ascending aorta (AO) across the aortic valve, the MacLab software calculates the ejection systolic period (ESP), which is the duration of ejection in seconds/minute that can be converted to left ventricular ejection systolic time (EST) measured in seconds/heartbeat.
2.2. Statistical Analysis
Statistical analysis was performed using MATLAB software 9.13. The mean values were compared using the Mann–Whitney U test for continuous variables. In contrast, categorical variables were analyzed using the χ2 (chi-square) test. A two-tailed p-value of less than 0.05 was considered statistically significant. Effect size was calculated using the phi coefficient (φ) for categorical variables and Cohen’s d for continuous variables. Effect size measures the strength and practical significance of a relationship or difference between variables, showing the extent of this variation or association in real-world contexts. Effect sizes of 0.10, 0.30, and 0.50 indicate small, medium, and large effects, respectively [37].
2.3. Pre-Processing and Denoising of Data
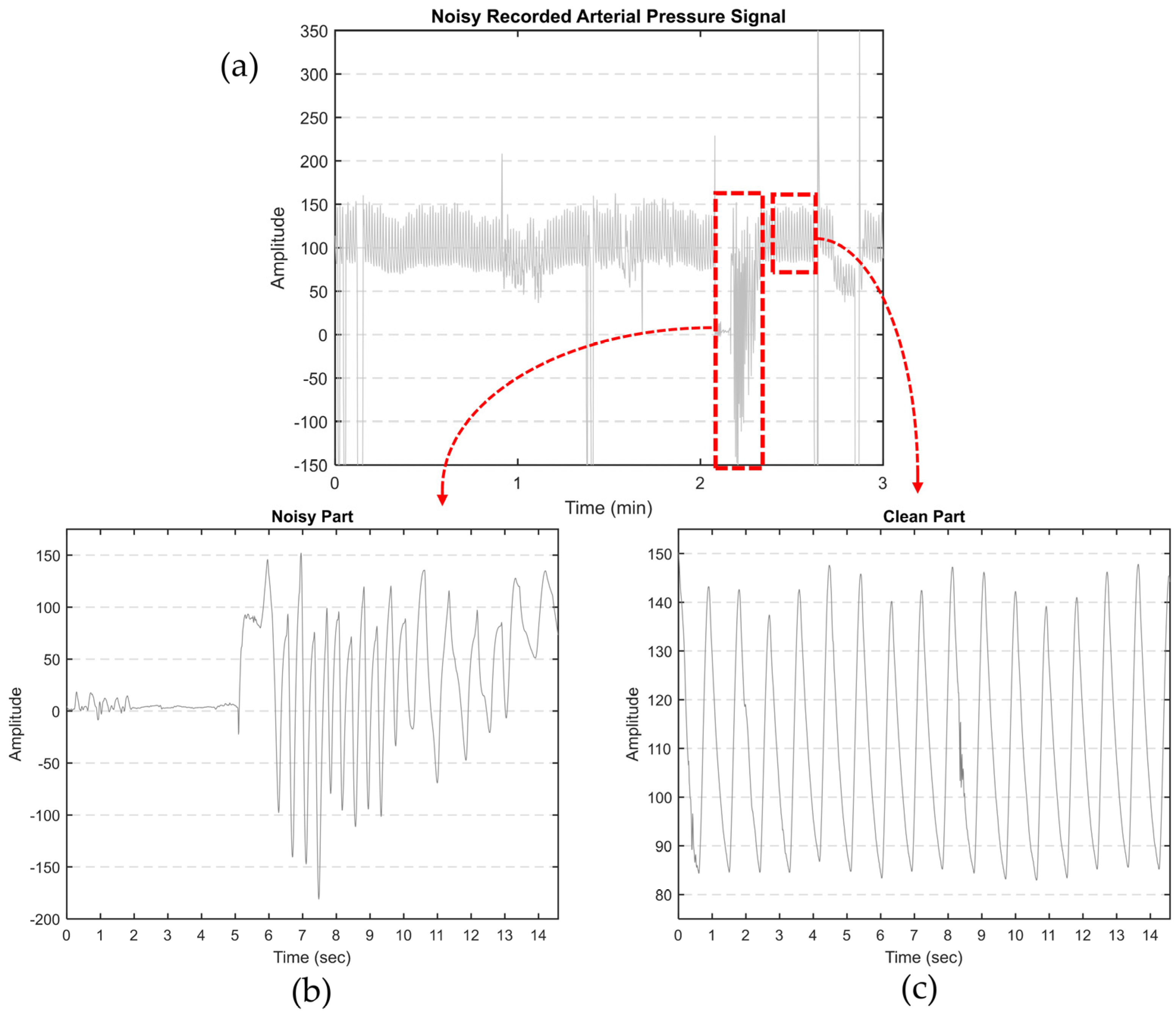
Our primary objective is to derive features from aortic pulse wave tracing obtained throughout the PPCI procedure. However, such AP signals can be affected by different types of noise. This includes motion artifacts (resulting from the movement of the catheter, transducer, or patient), electrode polarization, and electrical interference. Figure 1a illustrates an AP signal captured using MacLab that requires noise reduction. Figure 2 displays different parts of a typical recorded AP signal. As can be seen in Figure 1b, the selected part is noisy and should be excluded from the analysis. On the other hand, Figure 1c illustrates a part of the signal suitable for further analysis and feature extraction. This shows the importance of having a denoising strategy to extract the high-quality part of the AP signal.
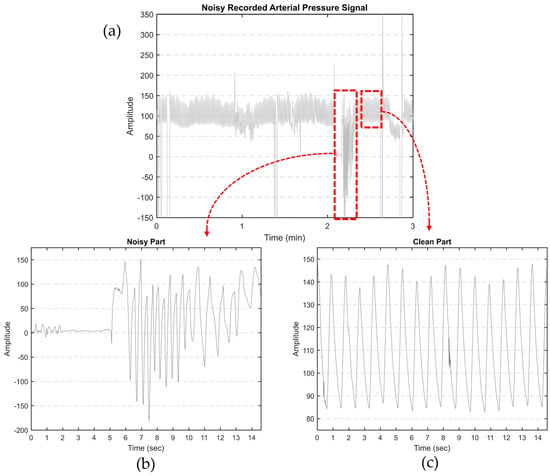
Figure 1.
(a) Noisy AP signal recorded by MacLab. The artifacts were manually clipped to the maximum shown in the figure; (b) an example of noisy and (c) clean parts of a typical recorded AP signal.
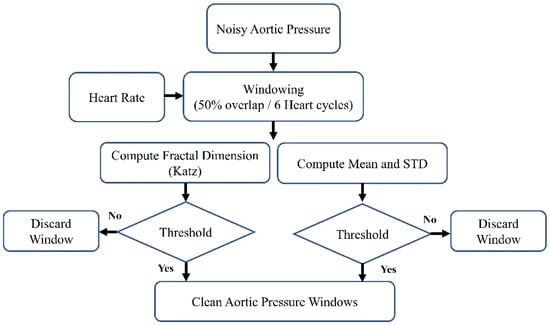
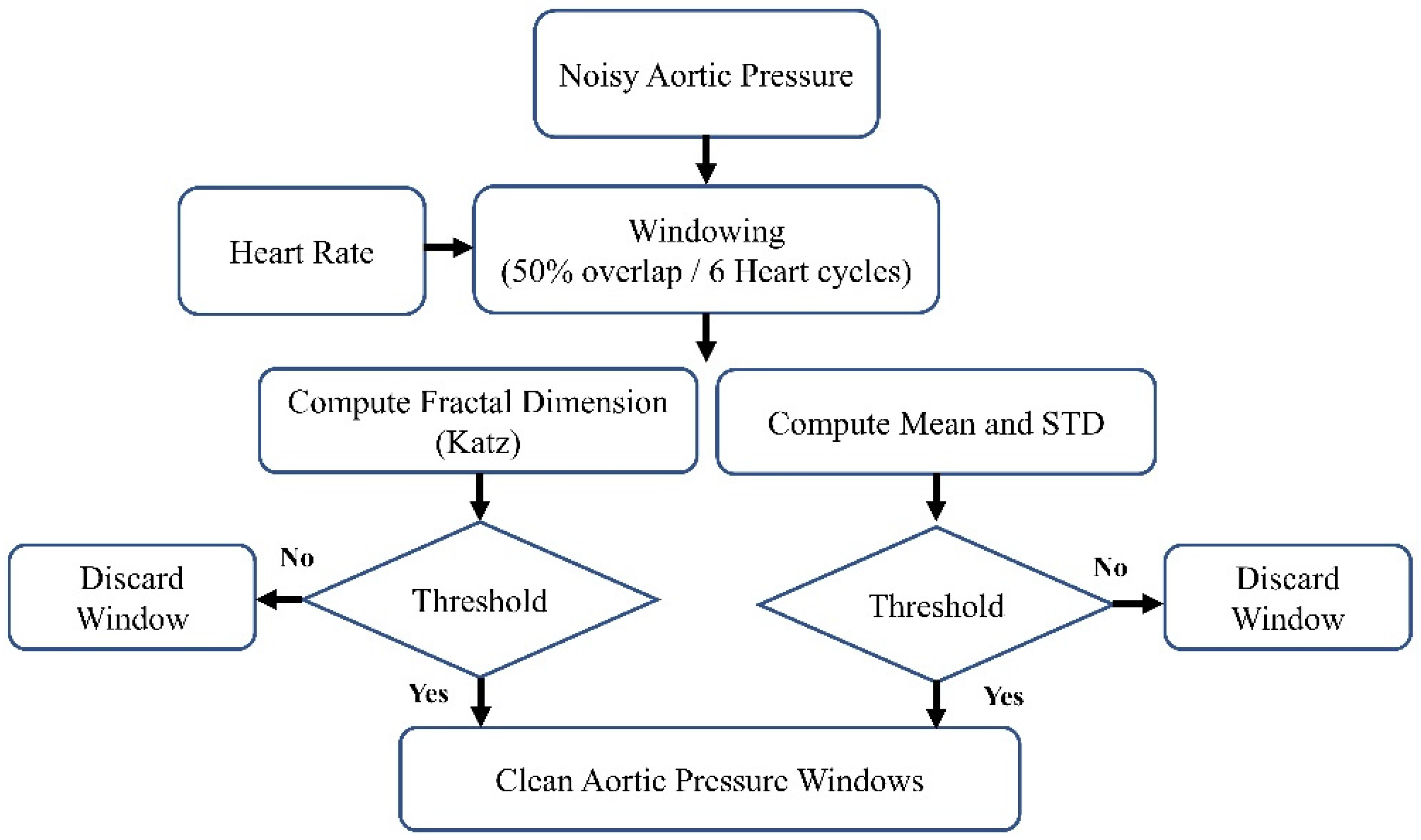
Figure 2.
The block diagram of the denoising method.
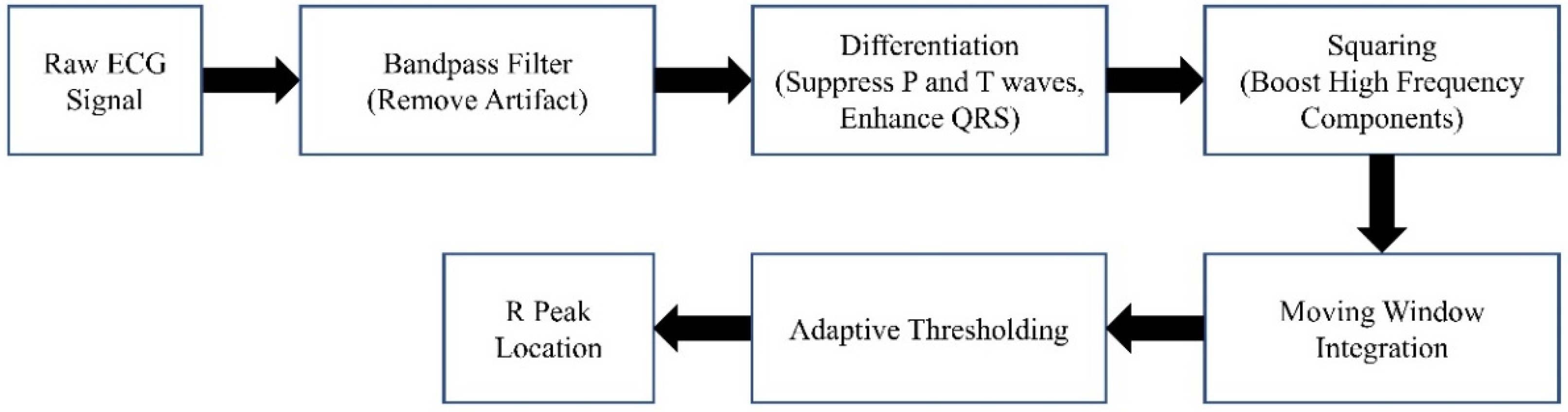
The block diagram of the denoising procedure is shown in Figure 2. It can generally be summarized as windowing the AP signal and discarding the noisy windows. We extracted the heartbeat (HB) from lead II ECG (also recorded by MacLab) to achieve an adaptive window size. We considered the window size to be six times the heart cycle length of each individual’s data. We extracted the heart rate using the Pan–Tompkins algorithm [38]. This algorithm employs band-pass filtering to enhance the signal-to-noise ratio (SNR) and eliminate low-frequency artifacts. A derivative operation is used to diminish the P and T waves, thus highlighting the QRS complex. This is followed by a squaring operation that amplifies the high-frequency elements. Subsequently, moving window integration is applied to create a smooth pulse corresponding to each QRS complex. Finally, the R peaks in QRS complexes are identified through adaptive thresholding, as depicted in Figure 3.
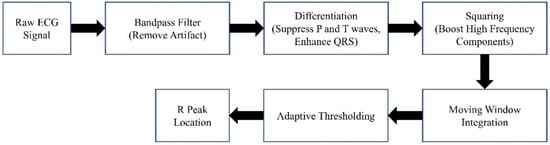
Figure 3.
The Pan–Tompkins algorithm.
After extracting the HB, we windowed the high-pass-filtered AP signal (with a cutoff frequency of 0.4 Hz) using a 50% overlap and a duration of six heart cycles. Following the windowing of the AP signal, we computed the fractal dimension (FD), mean, and standard deviation (SD). In this research, we used one of the most commonly used algorithms to estimate the fractal dimension: the Katz fractal dimension (KFD) [39]. The comprehensive set of features derived from each window of the AP signal includes:
- Mean values: Each window was segmented into three equal parts. For each segment, the mean value of the AP signal was calculated, resulting in three values.
- SD analysis: This involves calculating four SD values. The SD was computed for the entire window, and then the window was divided into three equal parts to determine the SD for each segment.
- FD Calculation: Each window was divided into three segments, and the FD was computed for each segment.
These characteristics were calculated for every AO window. To eliminate noisy windows, we applied thresholds to each characteristic, which were determined based on the physiological properties of the AO signal.
2.4. Feature Extraction
We separated each AP waveform after denoising the AP signal and discarding the noisy AP windows. From each waveform, we extracted a total of 18 features, as detailed in Table 1. The first 14 features relate to the time aspect, whereas spectral entropy (SE) and average power (Pave) are associated with frequency. We have tried to capture every aspect of the AP that might be useful for prediction. In the table below, skewness quantifies the asymmetry in a data set, while kurtosis evaluates whether the data have heavier or lighter tails compared to a normal distribution. SE measures the irregularity or complexity of digital signals within the frequency domain, and Pave indicates the mean energy transmission of a signal over a certain period.

Table 1.
The extracted 18 features.
Except for the overall time (OT) feature, which refers to the entire duration of the surgery, all other extracted features have multiple values per subject. This is because they are extracted from each AP waveform, and we have multiple waveforms for each subject’s AP signal. We applied a 20% trimmed mean for multi-value features to derive a single representative value for each characteristic per subject. The trimmed mean method excludes a specified percentage of the extreme values, both largest and smallest, before the mean calculation. This technique is beneficial in reducing the impact of outliers that could potentially bias the traditional mean.
2.5. Feature Selection
We also implemented feature selection methods to reduce the number of variables further, thereby shortening training time and enhancing model performance. We employed two feature-reduction methods: principal component analysis (PCA) [40] and linear discriminant analysis (LDA) [41]. In both approaches, we selected the top five features.
2.5.1. LDA-Based Feature Selection (LBFS)
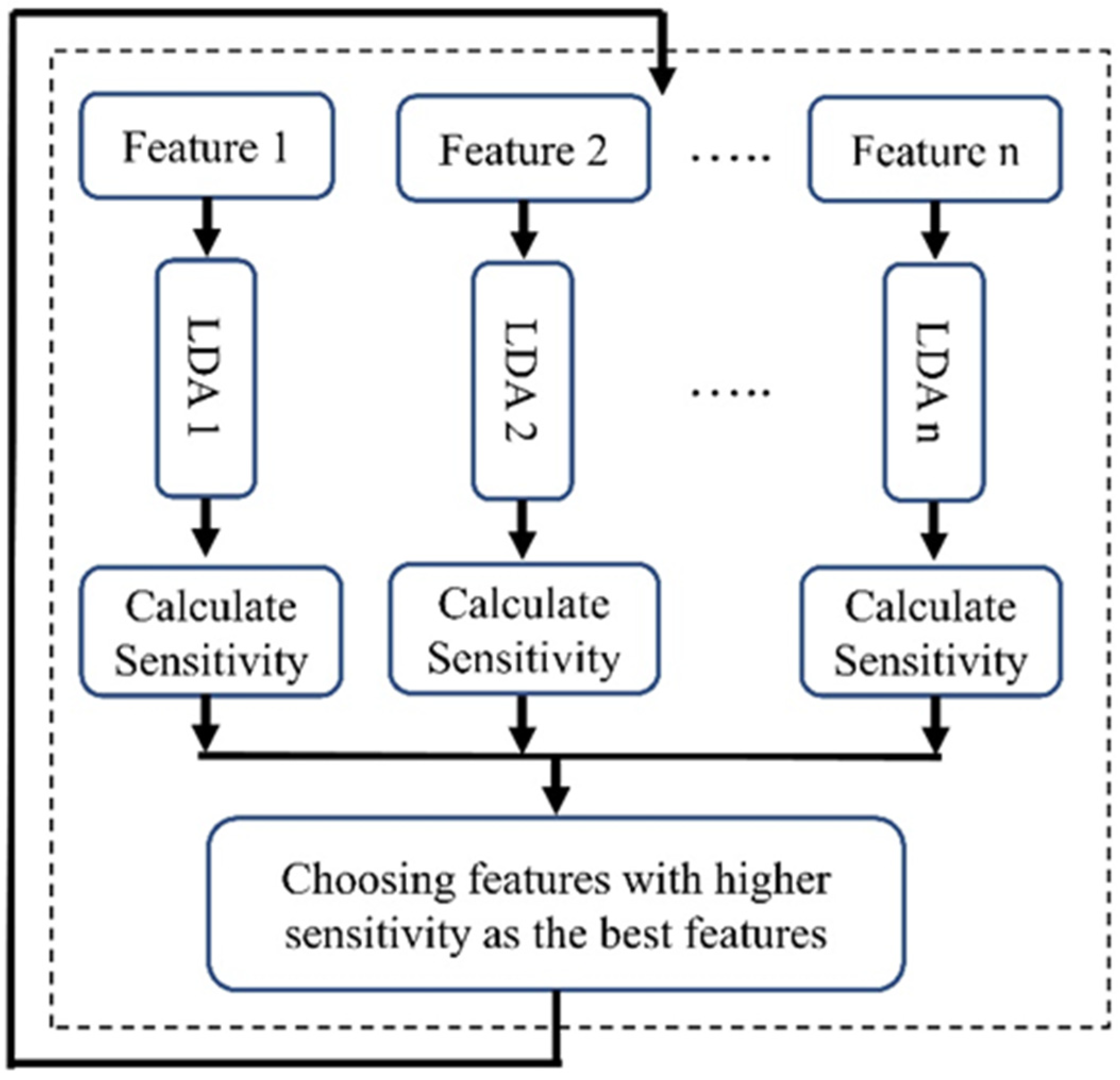
LDA, a supervised learning algorithm, was used for the feature selection in machine learning. As described in Figure 4, for each feature we utilized an individual LDA classifier to determine the power of each feature in distinguishing two classes. We divided our dataset into two sections (70% for training and 30% for validation) and classified patients into two groups: survivors and non-survivors at one year after admission. After training, we evaluated the sensitivity of each classifier, focusing on the top five features with the highest sensitivity. This emphasis on sensitivity is crucial for accurately predicting the non-surviving group, a key concern in our research.
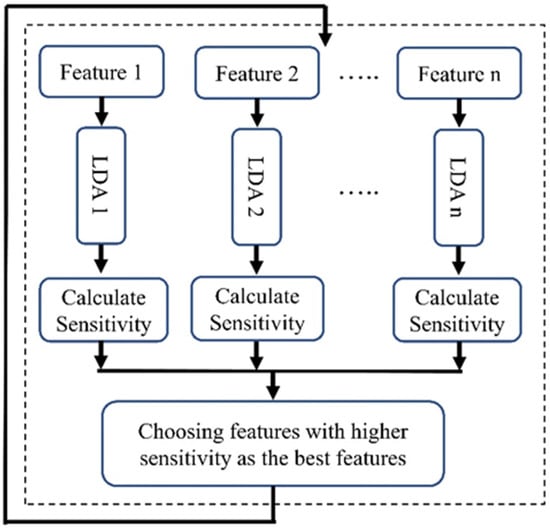
Figure 4.
Block diagram of the LBFS method.
This procedure was iterated 1000 times, with the training and validation sets being reshuffled each time. To tackle issues related to class imbalance, we employed the technique of down sampling (we randomly selected from class 1 (survived) to attain a more balanced number of patients across both classes).
2.5.2. PCA-Based Feature Selection (PBFS)
PCA is a widely recognized technique used for extracting features and reducing dimensionality. PCA aims to project data that initially existed in a d-dimensional space into a space of lower dimensions. In PCA, the process begins with calculating the dataset’s mean vector and covariance matrix. Then, eigenvectors and eigenvalues are computed and sorted by the eigenvalues’ magnitude. The largest k eigenvectors are selected, often based on an eigenvector spectrum analysis. The PCA output is a k-vector that prioritizes significance, with the first few principal components usually representing most of the dataset’s variability.
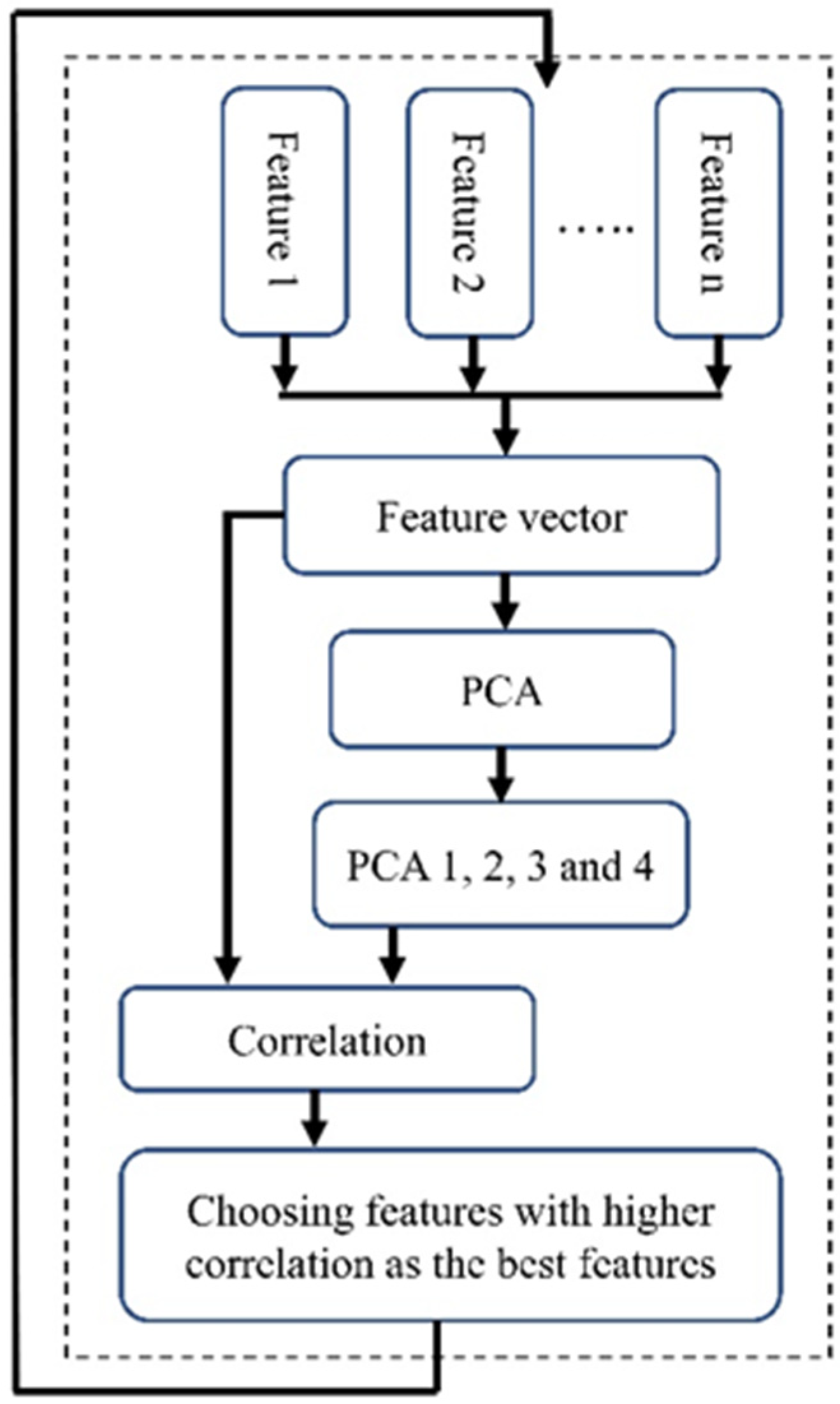
To employ PCA for feature selection, we initially calculated PCA using all features. Subsequently, we focused on the first four eigenvectors (PCA 1–PCA 4), which together represent nearly 80 percent of the variability in the dataset. A limitation of these PCAs is their lack of clarity regarding which specific features contribute most significantly to their formation, thereby not clearly indicating the most important features. To address this, we calculated the correlation between each feature and these four PCA vectors (Figure 5). We then computed the average of the values in each column, resulting in a single vector. The next step was to identify the feature corresponding to the highest value in this vector. We selected the five top features with higher correlation as the features selected by this method.
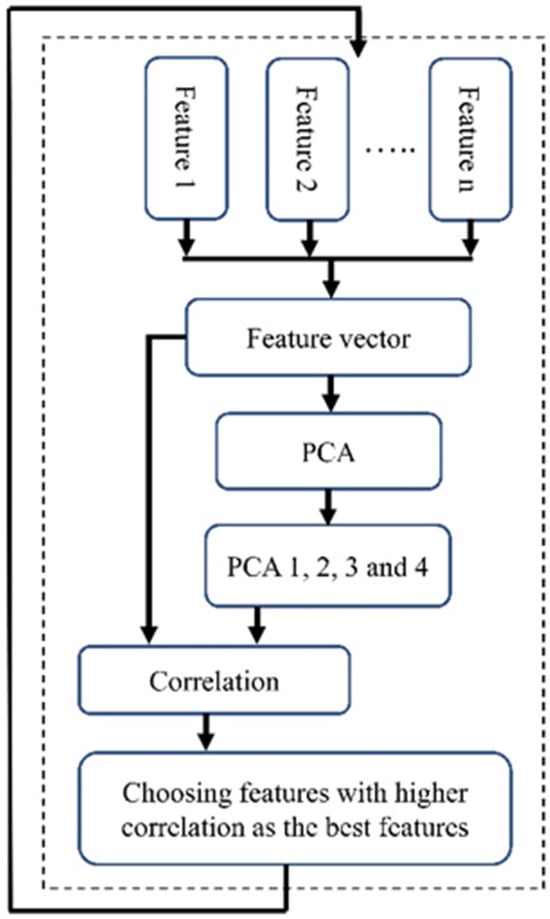
Figure 5.
The block diagram of the PBFS method.
Like the previous feature selection method, we addressed the imbalance issue by using the down-sampling method and repeating the process 1000 times to avoid bias towards a particular class. Additionally, we performed scaling before conducting the PCA. The block diagram of the implemented PBFS is shown in Figure 5.
2.6. Data Imbalance and Separation of Data into Training and Testing
The effectiveness of many standard binary classification algorithms in machine learning is higher with balanced datasets, as highlighted in [42]. However, the true challenge arises with imbalanced datasets, where these algorithms often struggle, especially since the consequences of misclassifying the minority class tend to be significantly more severe than those of misclassifying the majority class. Numerous strategies have been developed to manage imbalanced datasets. However, these methods have been criticized for changing the dataset’s original class distribution by generating new data (over-sampling), which may lead to overfitting, or by removing valuable data (under-sampling).
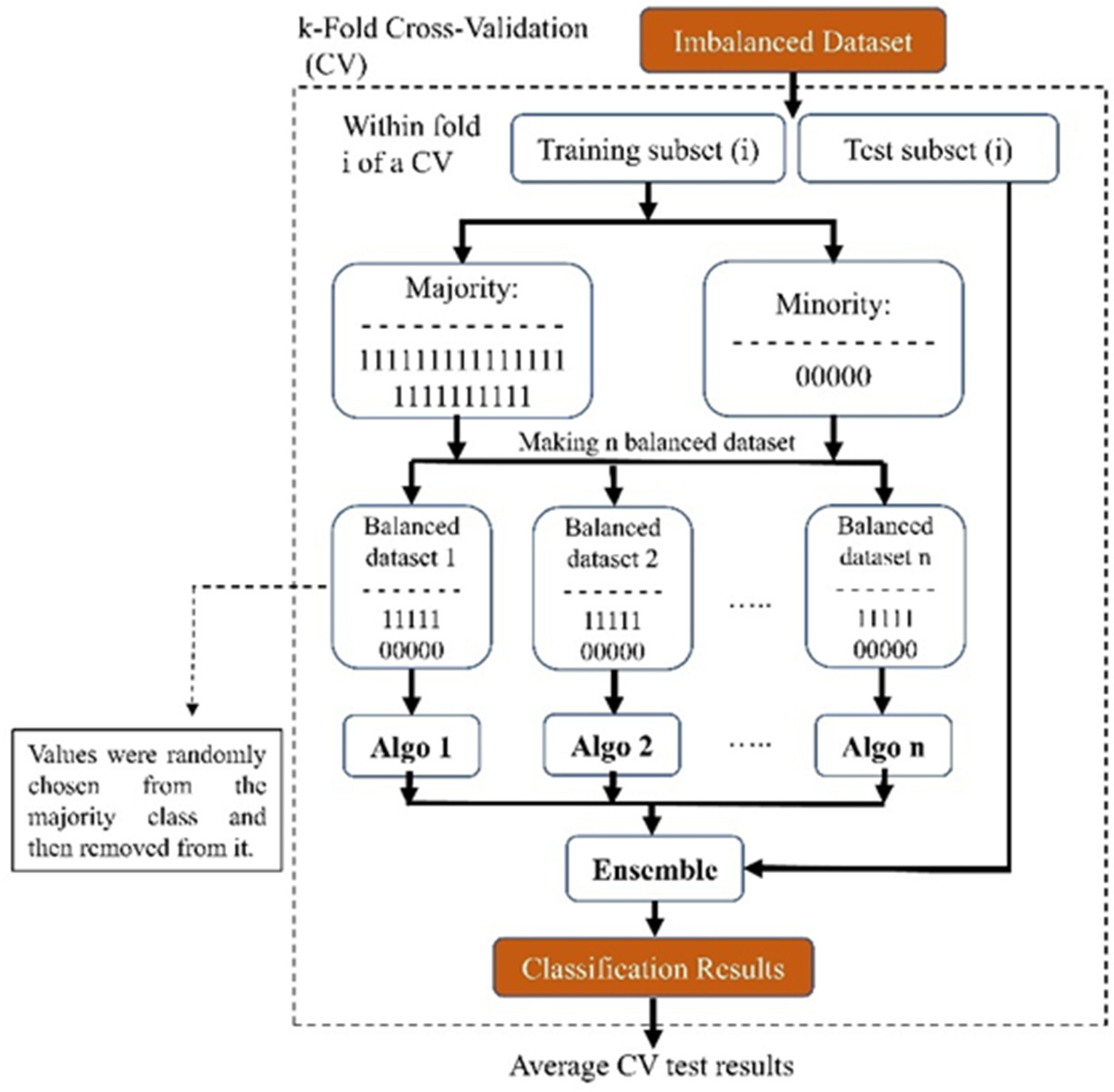
Our proposed ensemble-based methods will try to tackle the possible problems of the conventional methods mentioned above for handling class imbalance problems by converting an imbalanced dataset into several balanced datasets that do not suffer anymore from the challenge of an imbalanced dataset without creating new extra data or discarding potentially useful original data. As depicted in Figure 6, our method utilized a 10-fold cross-validation technique for the entire dataset. This ensured that the distribution of the whole data set was maintained for our test set.
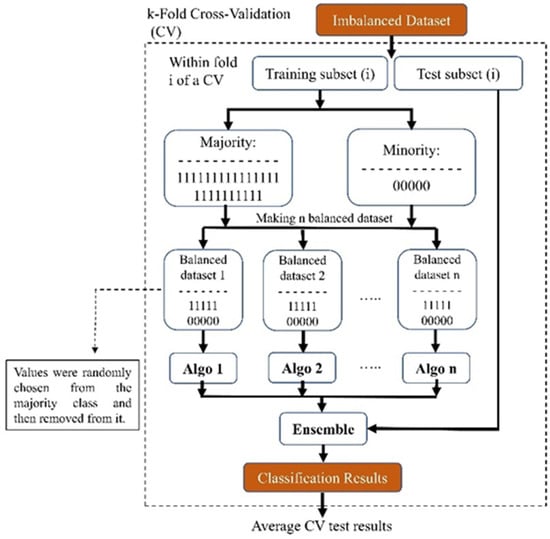
Figure 6.
Block diagram of our proposed ensemble-based method for addressing imbalanced datasets.
We used an ensemble method for the training part of the study: We created ‘n’ balanced sub-datasets from the imbalanced training dataset. To form these sub-datasets, we included all subjects from the minority class and randomly selected an equal number from the majority class. After selection, these subjects were removed from the majority dataset. Each sub-dataset, starting with the first, was used to train a model (referred to as ‘algo 1’ in Figure 6). We repeated this process across the entire majority dataset, resulting in ‘n’ distinct models. This approach ensured that no subjects were discarded, thus preserving essential information. Due to the disparity in the number of subjects between the minority and majority classes, our finally created sub-dataset might be slightly imbalanced. After training the models, we used the test set and evaluated each model’s performance and averaged the results of all the trained models. Eventually, because we implemented the 10-fold technique, we achieved the performance of that fold each time. In the end, we also averaged the test results from all of the folds and reported this value.
2.7. ML Predictive Models
The predictive models for 1-year mortality were developed using three different machine learning techniques: K-nearest neighbor (KNN) [43], LDA [41], and support vector machine (SVM) [44]. The KNN classifier, used for multiclass classification, identifies the nearest neighbors by calculating distances between a test sample and training data. KNN determines the nearest neighbors and uses a majority vote among them to classify the new sample. SVM, notable in biomedical fields for its precision and handling of multiple predictors [45], works by finding an optimal hyperplane for linear separation between classes. It categorizes data using this hyperplane, and it is effective in linear and nonlinear contexts. LDA combines features into a new variable to distinguish classes in a dataset. It reduces multi-dimensional data to one dimension, aiming for distinct class separation based on the discriminant score. This simplifies analysis and highlights differences between classes.
These models were trained and tested using two different strategies. Initially, we trained and tested the three models mentioned above using the top five features selected by each of our proposed feature selection methods. This evaluated the impact of considering only the top five features derived from the AP signal. In the second part, we explored the potential of enhancing model performance by incorporating demographic, risk factor, and catheterization data. These additional features were added to the top five AP curve features that were selected based on their p-value and effect size.
2.8. Models’ Evaluation
Evaluating the effectiveness of machine learning algorithms is crucial for determining their performance. We assessed our proposed machine learning approaches using accuracy, specificity, sensitivity (recall), and precision measures. Additionally, we plotted the ROC (receiver operating characteristic) curve to demonstrate the performance of our binary classification model at various thresholds. Subsequently, we computed the AUC (area under the ROC curve), a singular metric summarizing the overall effectiveness of the binary classification model.
3. Results
3.1. Patients’ Characteristics
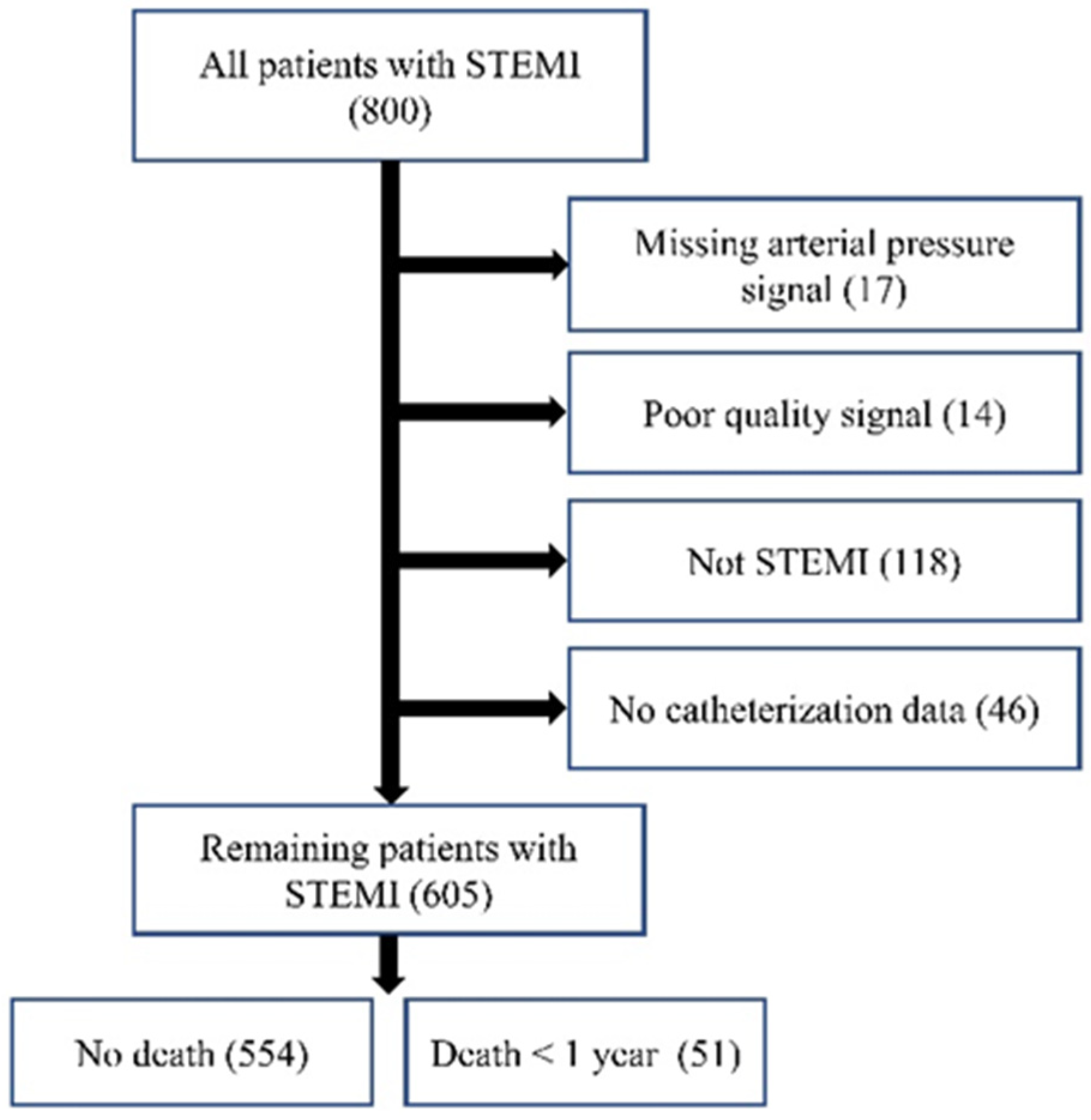
Out of 800 patients, data from 605 patients [age: 64.2 + 13.2 years; 432 (71.41%) males] with STEMI were selected for analysis. In total, 195 patients were excluded due to lacking adequate AP signals (n = 17), having poor-quality signals (n = 14), having an alternative diagnosis other than STEMI (n = 118), or not having catheterization data (n = 46). Figure 7 shows this exclusion schematically. The included patients were identified as having STEMI through ERP. This study reports 1-year mortality, defined as the period starting from admission, with patient follow-ups confirming the outcomes.
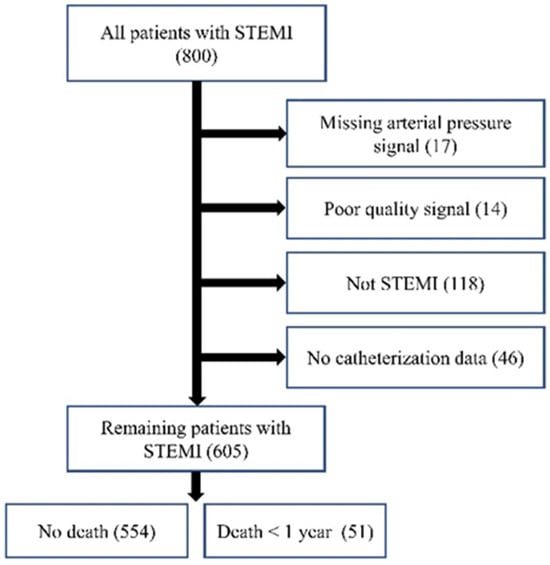
Figure 7.
Data collection flowchart.
Among these patients, STEMI localization was inferior [313 (51.74%)], anterior [230 (38.02%)], lateral [43 (7.11%)] and posterior [19 (3.14%)]. We investigated how the site of STEMI impacted patient survival, differentiating between survivors and non-survivors. Our research found no significant connection between survival rates and the STEMI’s location (inferior, anterior, lateral, or posterior), supported by non-significant p-values and effect sizes under 0.1. At 1-year follow-up, 554 (91.6%) patients survived and 51 (8.4%) died. Their demographic, risk factors, and catheterization data are described in Table 2.
Table 2.
Demographic, risk factors, and catheterization data for STEMI patients of this study.
3.2. Denoised AP Signal
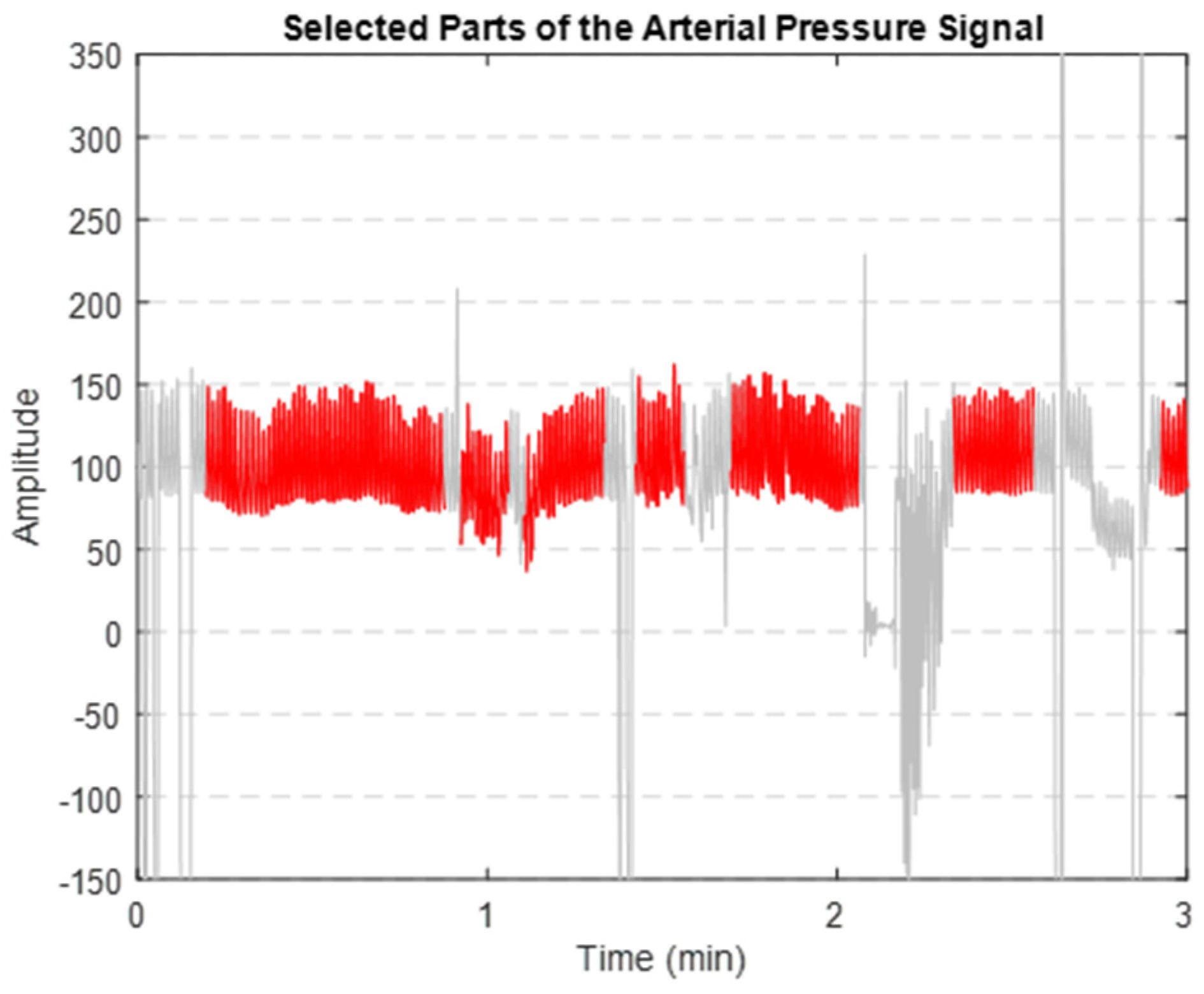
After implementing the proposed denoising method, we successfully extracted the clean segments of the AP signal. Figure 8 illustrates that the segments highlighted in red are the clearer, less noisy parts of the AP signal. These segments were then used to extract key features.
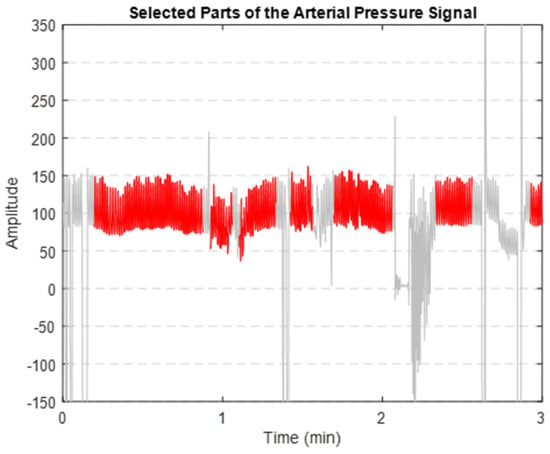
Figure 8.
Extracted clean segments (shown in red) of the AP signal (depicted in grey).
3.3. Extracted Features
A major challenge with the 18 features extracted initially (Table 1) was their high correlation. To address this, we calculated the correlation coefficient for each feature pair. We eliminated those with a correlation of more than 0.7, ensuring a more independent and effective set of features for our analysis. Without this correlation step, our feature selection methods might pick similar features and miss out on important different ones. The final set of features is nine in total, as shown in Table 3.
Table 3.
The extracted features after removal of highly correlated features.
3.4. Feature Selection Results
3.4.1. LBFS
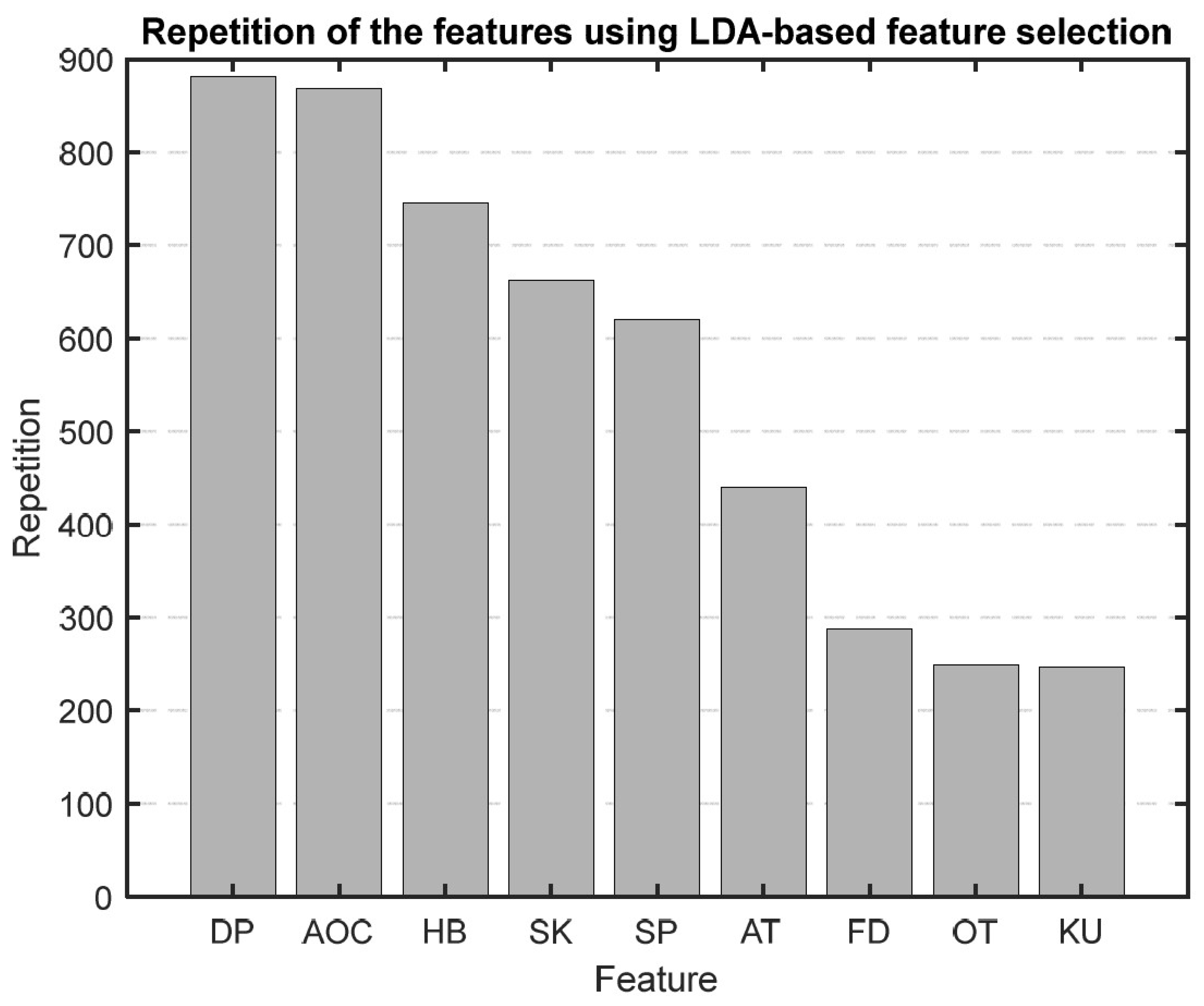
After running our first feature selection method, which uses LDA 1000 times, based on how often each feature was chosen as the most sensitive one, we made a bar graph (Figure 9) to show how important each feature is. As illustrated in Figure 9, features like diastolic blood pressure (DBP), area under the curve (AOC), HB, skewness, and systolic blood pressure (SBP) consistently emerged as the top five selections in this method.
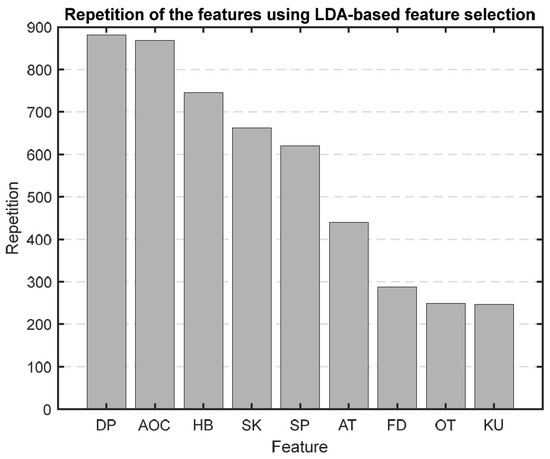
Figure 9.
Bar graph showing the repetition of each feature in the LBFS method.
In a two-class problem with a single feature, LDA simplifies to a process of threshold determination. It starts by calculating the mean of each class’s single feature and then computes between-class and within-class variances. The main objective is to find an optimal threshold that maximizes the between-class variance relative to the within-class variance, effectively creating a decision boundary. This threshold helps classify new instances.
3.4.2. PBFS
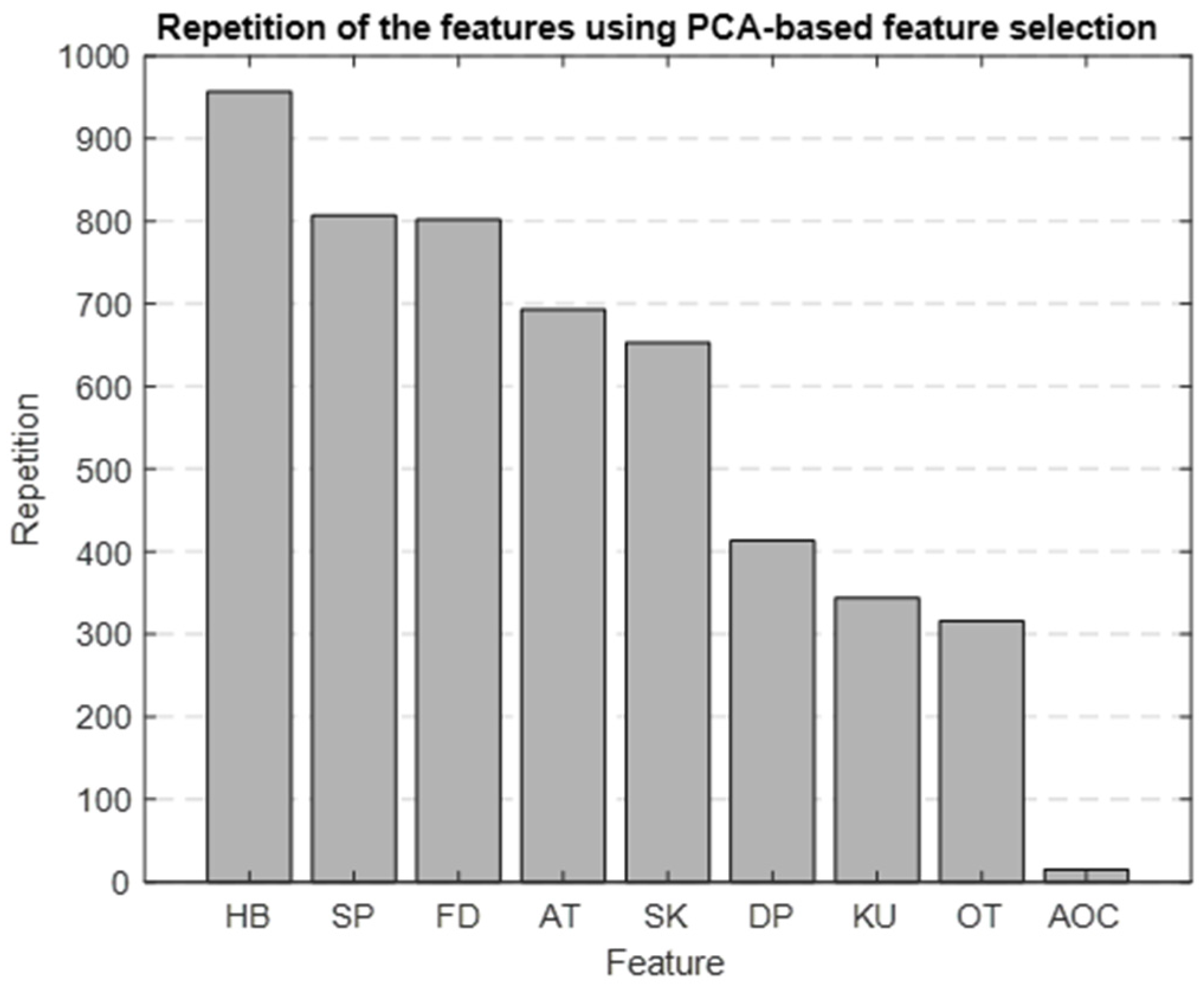
Using PCA as the foundation for our feature selection method, we generated a bar graph that highlights the most significant features identified through this approach. Figure 10 is the result of repeating the selection process 1000 times, showing which features are most important. The top five selected features were HB, SBP, FD, ascending time (AT), and skewness.
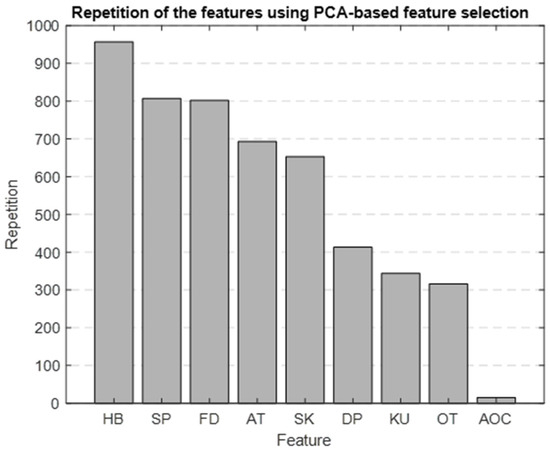
Figure 10.
Bar graph showing the repetition of each feature in the PBFS method.
3.5. Results on ML Models (Hemodynamic Trace Features)
Table 4 shows mortality prediction using the five selected features from the AP signal. The performance of the predictions differs based on the classifier and the method used for selecting features. The accuracy of these predictions falls between 69% and 72%, while the AUC values range from 0.73 to 0.77.
Table 4.
Prediction results using three different classifiers with features selected by PBFS and LBFS methods.
The SVM classifier, employing PBFS, achieved the same levels of accuracy and specificity as the KNN classifier but showed a higher sensitivity. In comparison, the LDA classifier, utilizing PBFS features, achieved the best overall prediction, slightly outperforming both the KNN and SVM classifiers in AUC. When we used LBFS, the KNN classifier’s accuracy was lower, while LDA and SVM classifiers showed improved accuracy. The sensitivity and specificity across these classifiers also varied slightly. The most effective model among those tested was the LDA classifier.
Our method’s approach to handling data imbalance, which maintained the dataset’s distribution in our test set, resulted in an imbalanced test set. This led to a higher incidence of false positives compared to the use of a balanced test set, consequently yielding a lower precision value. Additionally, it is noteworthy that three out of the five features selected by each feature selection method remained the same, demonstrating consistency across different techniques.
3.6. Results from ML Models (Adding Demographics, Risk Factors, and Catheterization Data)
In addition to classification using features extracted only from the AP signal, we investigated whether adding extra information such as demographics, risk factors, and catheterization information to the top five features from the AP signal would improve the prediction accuracy. We chose these additional variables based on two criteria: their p-values and the sizes of their effects (details shown in Table 2). We selected variables with a p-value < 0.01 and an effect size > 0.2. The variables selected were age, renal dysfunction (RD), dialysis, and EST, with effect sizes of 0.57, 0.26, 0.24, and 0.46, respectively; all had a p-value < 0.01.
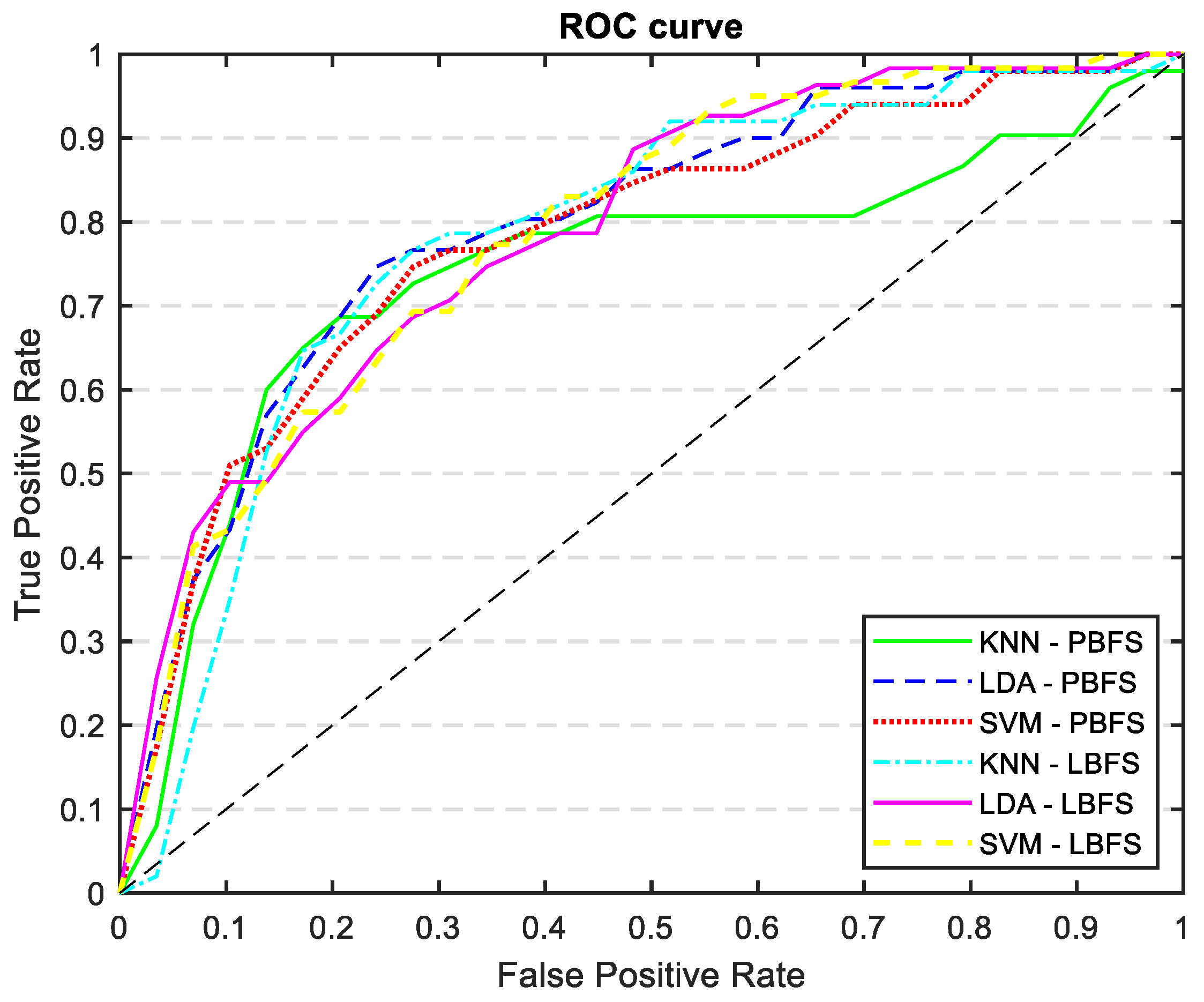
Table 5 shows the results of mortality prediction accuracy with the new variables added to the AP-driven features. By including these new features, we were able to keep the same level of sensitivity but we improved the accuracy, specificity, and AUC, particularly for the LDA classifier. Figure 11 displays the ROC curves for every trained model outlined in Table 5. The ROC curve and AUC values represent the average calculated across all folds.
Table 5.
Prediction results after adding demographic, risk factors, and catheterization information.
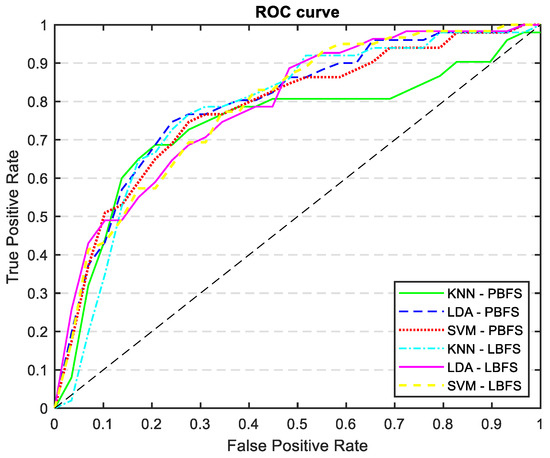
Figure 11.
ROC curves of all the trained models: KNN, LDA, and SVM classifiers trained with PCA and LDA selected features, incorporating demographics, risk factors, and catheterization information.
4. Discussion
Using three supervised machine learning approaches (KNN, LDA, and SVM) for the first time, this study demonstrates that the AP-derived features can be effective in developing a risk-predictive model for 1-year outcome in patients with STEMI. When age, RD, dialysis, and EST information were also included, the accuracy and sensitivity of our best model (LDA with PBFS) improved by 7% and 9%, respectively, while maintaining almost the same specificity. For the same model, the AUC also improved from 0.77 to 0.82.
For denoising of the AP signal, we extracted characteristics primarily based on mean, SD, and FD. The mean and SD are utilized to establish a threshold for identifying and removing data segments with abnormally high or low AP waveform values. To the best of our knowledge, we are the first group to investigate the application of FD in the denoising of the AP signal. FD is a nonlinear metric that measures complexity and irregularity in time-domain signals. We used this feature to discard abnormally complex AP waveforms. In an existing study [46], researchers examined the influences of various signal properties such as amplitude, frequency, harmonics, noise power, and bandwidth on FD. They concluded that FD is effective for identifying structural changes in signals, providing a rapid and efficient way to assess variations in signal complexity.
We chose to use PBFS and LBFS methods to further reduce the number of features, allowing us to interpret the model better and enhance its predictive accuracy. Each method selected the top five features, providing more precise insights into the AP waveform characteristics associated with mortality. Figure 9 and Figure 10 display the ranked importance of each AP feature as determined by the LBFS and PBFS methods, respectively. We categorize important AP features into two groups. The first group of features are the overlapping features identified by both methods: skewness, HB, and SBP. The second group is the remaining two unique features selected by each method: DBP and AOC, chosen by LBFS, and AT and FD, selected by PBFS.
The features selected by our feature selection methods are supported by other studies which show their importance. In [47], entropy, skewness, and kurtosis values derived from ECG signals were fed into a least squares SVM classifier for MI detection. This research marks the first instance of calculating kurtosis and skewness from ECG signals specifically for mortality prediction, demonstrating their pivotal role in such predictive analysis. Similarly, previous research highlighted a positive correlation between elevated HB and mortality [48,49]. Lower SBP and DBP were also shown to be predictors for in-hospital, 30-day, and 1-year mortality in patients with STEMI [29]. Moreover, FD has been previously employed in the analysis of AP signals for various purposes, and it has an intricate association with arterial stiffness [50]; arterial stiffness is correlated with the risk of cardiovascular mortality and morbidity [51]. Abrupt myocardial damage due to STEMI compromises the myocardial ability to maintain adequate stroke volume or the amount of blood ejected per heartbeat. Many of these patients with low stroke volume are noted to have narrow pulse pressure (SBP–DBP, mmHg), slow uprise of the AP tracing (smaller AT), or smaller AOC [52,53].
In general, all classifiers, along with the selected features, yielded similar results. These results highlight the effectiveness of our method, utilizing only five features extracted from the AP signal. Notably, the LDA model with LBFS outperformed the others, achieving the highest accuracy, specificity, sensitivity, and AUC. Typically, machine learning models exhibit a slight decrease in performance on validation data (unseen data) compared to training data (seen data), as they are optimized based on the training dataset. In our study, this was true as well; the performance of the ML models on the validation dataset was slightly lower than on the training dataset, but it did not result in overfitting.
Incorporating demographics, risk factors, and catheterization information such as age, RD, dialysis, and EST into the selected features led to improvements across various metrics. The most effective model, which demonstrated a slightly better AUC, was the LDA trained with PBFS. Both selected risk factors are related to abnormal kidney function, emphasizing its crucial role. The relationship between renal dysfunction and cardiovascular outcomes in the general population [54], and STEMI patients [55] is well established. Age has been widely used as a predictor for mortality, especially in-hospital [29,56], 30-day [29], and 1-year mortality [29,57,58]. Similarly, EST is also independently linked to a higher risk of cardiovascular disease and related death [53].
Different studies have previously focused on mortality prediction in patients with STEMI using different methodologies. Oliveira et al. [27] conducted a study employing ML algorithms to predict in-hospital mortality in acute MI patients, including STEMI cases. Their research involved three distinct experiments, each utilizing varying feature sets. The first two experiments used 1179 discharge episodes, initially focusing on admission variables and adding laboratory data, comorbidities, and interventions. The third experiment, using 445 episodes, included more specific pathology-related variables than the previously added variables. The best performance was observed in the third experiment, without data balancing and with all 44 variables, where the KNN algorithm achieved 87% accuracy, 36% precision, 90% recall, and an AUC of 0.89. In another study [28] involving 3191 STEMI patients, five different machine learning models were trained and tested using 31 candidate features, with the Extra-tree classifier proving to be the most effective for predicting all-cause 30-day mortality following STEMI. This model achieved a sensitivity of 85%, specificity of 74%, accuracy of 79%, and an AUC of 79.7%. In another study [29] using the data from a registry of 27592 STEMI patients, researchers applied ML to predict and identify factors associated with short- and long-term mortality in Asian patients with STEMI. These models were developed for in-hospital (6299 patients), 30-day (3130 patients), and 1-year (2939 patients) mortality. The analysis considered 50 variables (9 continuous, 41 categorical) and three ML algorithms (RF, SVM, and Linear Regression). This study evaluated model performance using both a complete and reduced set of variables, achieving an AUC ranging from 0.73 to 0.90. SVM classifier (with feature selection) displayed the highest predictive performance for in-hospital, 30-day, and 1-year models, achieving AUCs of 0.88, 0.90, and 0.84, respectively. Notably, for 1-year mortality prediction the same model achieved the best results with an accuracy of 77%, specificity of 77%, and sensitivity of 75%.
Our study has several limitations. First, the patient data is collected from a single institution, which may not be universally representative and could introduce bias in outcome measurements. However, our hospital is the only cardiac center providing tertiary cardiac care in the province of Manitoba. Second, not all potential risk factors leading to STEMI were available or included in this study. Thirdly, the limited number of patients is a major limitation and expanding the dataset could lead to an increased number of patients in the non-survivor group, potentially enhancing prediction. Fourthly, we could not compare our results with conventional scoring methods due to a lack of access to Killip class data that is essential for conventional scoring methods [59]. Finally, another challenge was our dataset’s highly imbalanced nature. We developed a method to address this imbalance while retaining key features and preserving the dataset’s distribution. Although this strategy improved our model training, the imbalance inevitably may affect the observed predictions. One notable consequence is reduced precision, resulting from maintaining class distribution in our final test set. This may have led to a higher representation of patients in class 1 (survived) compared to class 2 (the non-survived group), resulting in an increased number of false positives and a consequent significant decrease in precision.
In our future research, we plan to extract additional features from the AP signal to develop more comprehensive models. The dicrotic notch is a key point in AP. It identifies a specific point on the AP curve, allowing us to divide the waveform into systolic and diastolic sections. This distinction is vital as it enables us to extract different features from these two phases of heart function, compare them, and potentially utilize them in training our advanced models. However, accurately identifying the dicrotic notch can be challenging, as it may not be present in all waveforms and may require varied strategies for different waveforms or patients. A more complex model we aim to develop involves tree-based methods, which have shown effectiveness in mortality prediction in other studies [32,60,61]. These methods offer promising avenues for enhancing our predictive capabilities. While our primary focus in this study was on predicting mortality at 1-year post-PPCI, future research could expand to include other complications, including but not limited to prolonged in-hospital stays, identifying new diagnoses of heart failure, and more. This broader scope could provide deeper insights into identifying high-risk patients, which is important as careful monitoring and timely intervention can plausibly improve outcomes and quality of life and reduce health-related expenditure.
5. Conclusions
Machine learning analyzing AP signal, incorporating other clinical parameters, can predict 1-year mortality in STEMI patients treated with PPCI. Our work showed that such a hemodynamic tracing has the potential to be a marker of clinical significance in identifying patients at risk for adverse outcomes. We identified skewness, HB, and SBP as the most significant AP features for our prediction. Our findings should be validated in a larger, prospective, multi-center study.
Author Contributions
Conceptualization, S.R.R., A.H.S. and Z.M.; methodology, S.R.R., A.H.S. and Z.M.; software, S.R.R.; validation, S.R.R., A.H.S. and Z.M.; formal analysis, S.R.R., A.H.S. and Z.M.; investigation, S.R.R., A.H.S. and Z.M.; resources, A.H.S. and Z.M.; data curation, S.R.R., T.S. and A.C.Z.; T.S. and A.C.Z. contributed equally; writing—original draft preparation, S.R.R.; writing—review and editing, S.R.R., A.H.S. and Z.M.; visualization, S.R.R., A.H.S. and Z.M.; supervision, A.H.S. and Z.M.; project administration, A.H.S. and Z.M.; funding acquisition, A.H.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Max Rady College of Medicine Establishment Grant, University of Manitoba.
Institutional Review Board Statement
This study was approved by the local Research and Ethics Board, University of Manitoba (REB: HS25542 (H2022:196)—approval date: 15 September 2023).
Informed Consent Statement
This retrospective study included consecutive 800 patients suspected to have STEMI who were referred to the St Boniface General Hospital, Winnipeg, MB, Canada for consideration of PPCI between January 2020 to October 2021. De-identified patients’ demographic data, cardiovascular risk factors, catheterization data, and outcomes were collected by reviewing each electronic patient record (EPR). The arterial pressure (AP) wave tracings throughout the PPCI procedure were obtained through the MacLab system database (GE Healthcare; Milwaukee, WI, USA). Given these retrospective data analysis, individual patient consent was not obtained.
Data Availability Statement
The datasets presented in this article are not readily available as the data are part of an ongoing study. Requests for accessing the dataset should be directed to Dr. Ashish H. Shah.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kasim, S.; Malek, S.; Aziz, M.F.; Ibrahim, K.S. Machine Learning to Predict In-Hospital Mortality Risk among Heterogenous STEMI Patients with Diabetes. Eur. Heart J. 2022, 43, ehab849-176. [Google Scholar] [CrossRef]
- Shah, B.R.; Hux, J.E.; Zinman, B. Increasing Rates of Ischemic Heart Disease in the Native Population of Ontario, Canada. Arch. Intern. Med. 2000, 160, 1862–1866. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular Disease in Europe 2014: Epidemiological Update. Eur. Heart J. 2014, 35, 2950–2959, Erratum in Eur. Heart J. 2015, 36, 794. [Google Scholar] [CrossRef] [PubMed]
- CANSIM-102-0561—Leading Causes of Death, Total Population, by Age Group and Sex, Canada. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401 (accessed on 31 March 2023).
- Bishu, K.G.; Lekoubou, A.; Kirkland, E.; Schumann, S.O.; Schreiner, A.; Heincelman, M.; Moran, W.P.; Mauldin, P.D. Estimating the Economic Burden of Acute Myocardial Infarction in the US: 12 Year National Data. Am. J. Med. Sci. 2020, 359, 257–265. [Google Scholar] [CrossRef]
- Vogel, B.; Claessen, B.E.; Arnold, S.V.; Chan, D.; Cohen, D.J.; Giannitsis, E.; Gibson, C.M.; Goto, S.; Katus, H.A.; Kerneis, M.; et al. ST-Segment Elevation Myocardial Infarction. Nat. Rev. Dis. Prim. 2019, 5, 39. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, Y.; Zhi, W.; Fu, Y.; Wang, Q.; Zhou, J.; Zheng, S.; Hao, G. Safety and Feasibility of Low-Dose Ticagrelor in Patients with ST-Segment Elevation Myocardial Infarction. Clin. Cardiol. 2021, 44, 123–128. [Google Scholar] [CrossRef]
- Mensah, G.A.; Wei, G.S.; Sorlie, P.D.; Fine, L.J.; Rosenberg, Y.; Kaufmann, P.G.; Mussolino, M.E.; Hsu, L.L.; Addou, E.; Engelgau, M.M.; et al. Decline in Cardiovascular Mortality. Circ. Res. 2017, 120, 366–380. [Google Scholar] [CrossRef] [PubMed]
- de Boer, S.P.M.; Westerhout, C.M.; Simes, R.J.; Granger, C.B.; Zijlstra, F.; Boersma, E. Mortality and Morbidity Reduction by Primary Percutaneous Coronary Intervention Is Independent of the Patient’s Age. JACC Cardiovasc. Interv. 2010, 3, 324–331. [Google Scholar] [CrossRef]
- OECD/European Union (2020). Health at a Glance: Europe 2020; Health at a Glance: Europe; OECD: Paris, France, 2020; ISBN 9789264365643. [Google Scholar]
- Thrane, P.G.; Olesen, K.K.W.; Thim, T.; Gyldenkerne, C.; Mortensen, M.B.; Kristensen, S.D.; Maeng, M. Mortality Trends After Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2023, 82, 999–1010. [Google Scholar] [CrossRef]
- Kandala, J.; Oommen, C.; Kern, K.B. Sudden Cardiac Death. Br. Med. Bull. 2017, 122, 5–15. [Google Scholar] [CrossRef]
- Elbadawi, A.; Elgendy, I.Y.; Mahmoud, K.; Barakat, A.F.; Mentias, A.; Mohamed, A.H.; Ogunbayo, G.O.; Megaly, M.; Saad, M.; Omer, M.A.; et al. Temporal Trends and Outcomes of Mechanical Complications in Patients With Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2019, 12, 1825–1836. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, B. ST-Segment Elevation Myocardial Infarction. In Practical Cardiology: Principles and Approaches; Elsevier: Amsterdam, The Netherlands, 2022; ISBN 9780323809153. [Google Scholar]
- Fox, K.A.; Dabbous, O.H.; Goldberg, R.J.; Pieper, K.S.; Eagle, K.A.; Van de Werf, F.; Avezum, Á.; Goodman, S.G.; Flather, M.D.; Anderson, F.A.; et al. Prediction of Risk of Death and Myocardial Infarction in the Six Months after Presentation with Acute Coronary Syndrome: Prospective Multinational Observational Study (GRACE). Br. Med. J. 2006, 333, 1091. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. Kardiol. Pol. 2018, 76, 229–313. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; Antman, E.M.; Charlesworth, A.; Cairns, R.; Murphy, S.A.; de Lemos, J.A.; Giugliano, R.P.; McCabe, C.H.; Braunwald, E. TIMI Risk Score for ST-Elevation Myocardial Infarction: A Convenient, Bedside, Clinical Score for Risk Assessment at Presentation. Circulation 2000, 102, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; Antman, E.M.; Parsons, L.; De Lemos, J.A.; Cannon, C.P.; Giugliano, R.P.; McCabe, C.H.; Barron, H.V.; Braunwald, E. Application of the TIMI Risk Score for ST-Elevation MI in the National Registry of Myocardial Infarction 3. JAMA 2001, 286, 1356–1359. [Google Scholar] [CrossRef] [PubMed]
- Scruth, E.A.; Cheng, E.; Worrall-Carter, L. Risk Score Comparison of Outcomes in Patients Presenting with ST-Elevation Myocardial Infarction Treated with Percutaneous Coronary Intervention. Eur. J. Cardiovasc. Nurs. 2013, 12, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Halkin, A.; Singh, M.; Nikolsky, E.; Grines, C.L.; Tcheng, J.E.; Garcia, E.; Cox, D.A.; Turco, M.; Stuckey, T.D.; Na, Y.; et al. Prediction of Mortality after Primary Percutaneous Coronary Intervention for Acute Myocardial Infarction: The CADILLAC Risk Score. J. Am. Coll. Cardiol. 2005, 45, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Suryapranata, H.; Van’t Hof, A.W.J.; De Boer, M.J.; Hoorntje, J.C.A.; Dambrink, J.H.E.; Gosselink, A.T.M.; Ottervanger, J.P.; Zijlstra, F. Prognostic Assessment of Patients with Acute Myocardial Infarction Treated with Primary Angioplasty: Implications for Early Discharge. Circulation 2004, 109, 2737–2743. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Bauersachs, J.; Dendale, P.; Edvardsen, T.; Gale, C.P.; Jobs, A.; Lambrinou, E.; Mehilli, J.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.M.; Jeon, K.H.; Kim, H.M.; Kim, M.J.; Lim, S.; Kim, K.H.; Song, P.S.; Park, J.; Choi, R.K.; Oh, B.-H.; et al. Deep-Learning-Based out-of-Hospital Cardiac Arrest Prognostic System to Predict Clinical Outcomes. Resuscitation 2019, 139, 84–91. [Google Scholar] [CrossRef]
- Hametner, B.; Wassertheurer, S.; Mayer, C.C.; Danninger, K.; Binder, R.K.; Weber, T. Aortic Pulse Wave Velocity Predicts Cardiovascular Events and Mortality in Patients Undergoing Coronary Angiography. Hypertension 2021, 77, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Blacher, J.; Asmar, R.; Djane, S.; London, G.M.; Safar, M.E. Aortic Pulse Wave Velocity as a Marker of Cardiovascular Risk in Hypertensive Patients. Hypertension 1999, 33, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; De Filippo, O.; Gallone, G.; Mittone, G.; Deriu, M.A.; Iannaccone, M.; Ariza-Solé, A.; Liebetrau, C.; Manzano-Fernández, S.; Quadri, G.; et al. Machine Learning-Based Prediction of Adverse Events Following an Acute Coronary Syndrome (PRAISE): A Modelling Study of Pooled Datasets. Lancet 2021, 397, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Seringa, J.; Pinto, F.J.; Henriques, R.; Magalhães, T. Machine Learning Prediction of Mortality in Acute Myocardial Infarction. BMC Med. Inform. Decis. Mak. 2023, 23, 70. [Google Scholar] [CrossRef] [PubMed]
- Shetty, M.K.; Kunal, S.; Girish, M.P.; Qamar, A.; Arora, S.; Hendrickson, M.; Mohanan, P.P.; Gupta, P.; Ramakrishnan, S.; Yadav, R.; et al. Machine Learning Based Model for Risk Prediction after ST-Elevation Myocardial Infarction: Insights from the North India ST Elevation Myocardial Infarction (NORIN-STEMI) Registry. Int. J. Cardiol. 2022, 362, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Aziz, F.; Malek, S.; Ibrahim, K.S.; Shariff, R.E.R.; Wan Ahmad, W.A.; Ali, R.M.; Liu, K.T.; Selvaraj, G.; Kasim, S. Short- and Long-Term Mortality Prediction after an Acute ST-Elevation Myocardial Infarction (STEMI) in Asians: A Machine Learning Approach. PLoS ONE 2021, 16, e0254894. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, J.; Sun, L.; Cai, J.; Wang, S.; Zeng, L.; Sun, S. Application of Machine Learning to Predict the Occurrence of Arrhythmia after Acute Myocardial Infarction. BMC Med. Inform. Decis. Mak. 2021, 21, 301. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Qiu, H.; Li, W.; Chen, Y. A Stacking-Based Model for Predicting 30-Day All-Cause Hospital Readmissions of Patients with Acute Myocardial Infarction. BMC Med. Inform. Decis. Mak. 2020, 20, 335. [Google Scholar] [CrossRef]
- Sherazi, S.W.A.; Jeong, Y.J.; Jae, M.H.; Bae, J.W.; Lee, J.Y. A Machine Learning–Based 1-Year Mortality Prediction Model after Hospital Discharge for Clinical Patients with Acute Coronary Syndrome. Health Inform. J. 2020, 26, 1289–1304. [Google Scholar] [CrossRef]
- Kasim, S.; Malek, S.; Ibrahim, K.K.; Aziz, M. Risk Stratification of Asian Patients after ST-Elevation Myocardial Infarction Using Machine Learning Methods. Eur. Heart J. 2020, 41, ehaa946-3494. [Google Scholar] [CrossRef]
- Li, Y.M.; Jiang, L.C.; He, J.J.; Jia, K.Y.; Peng, Y.; Chen, M. Machine Learning to Predict the 1-Year Mortality Rate after Acute Anterior Myocardial Infarction in Chinese Patients. Ther. Clin. Risk Manag. 2020, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hadanny, A.; Shouval, R.; Wu, J.; Shlomo, N.; Unger, R.; Zahger, D.; Matetzky, S.; Goldenberg, I.; Beigel, R.; Gale, C.; et al. Predicting 30-Day Mortality after ST Elevation Myocardial Infarction: Machine Learning- Based Random Forest and Its External Validation Using Two Independent Nationwide Datasets. J. Cardiol. 2021, 78, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Bai, Z.; Lu, J.; Li, T.; Ma, Y.; Liu, Z.; Zhao, R.; Wang, Z.; Shi, B. Clinical Feature-Based Machine Learning Model for 1-Year Mortality Risk Prediction of ST-Segment Elevation Myocardial Infarction in Patients with Hyperuricemia: A Retrospective Study. Comput. Math. Methods Med. 2021, 2021, 7252280. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.J. Fractals and the Analysis of Waveforms. Comput. Biol. Med. 1988, 18, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Abdi, H.; Williams, L.J. Principal Component Analysis. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Xanthopoulos, P.; Pardalos, P.M.; Trafalis, T.B. Linear Discriminant Analysis. In Robust Data Mining; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Wei, Q.; Dunbrack, R.L. The Role of Balanced Training and Testing Data Sets for Binary Classifiers in Bioinformatics. PLoS ONE 2013, 8, e67863. [Google Scholar] [CrossRef] [PubMed]
- Cover, T.M.; Hart, P.E. Nearest Neighbor Pattern Classification. IEEE Trans. Inf. Theory 1967, 13, 21–27. [Google Scholar] [CrossRef]
- Burges, C.J.C. A Tutorial on Support Vector Machines for Pattern Recognition. Data Min. Knowl. Discov. 1998, 2, 121–167. [Google Scholar] [CrossRef]
- Subasi, A.; Gursoy, M.I. EEG Signal Classification Using PCA, ICA, LDA and Support Vector Machines. Expert Syst. Appl. 2010, 37, 8659–8666. [Google Scholar] [CrossRef]
- Raghavendra, B.S.; Dutt, D.N. Signal Characterization Using Fractal Dimension. Fractals 2010, 18, 287–292. [Google Scholar] [CrossRef]
- Tripathy, R.K.; Bhattacharyya, A.; Pachori, R.B. A Novel Approach for Detection of Myocardial Infarction from ECG Signals of Multiple Electrodes. IEEE Sens. J. 2019, 19, 4509–4517. [Google Scholar] [CrossRef]
- Zheng, Y.Y.; Wu, T.T.; Chen, Y.; Hou, X.G.; Yang, Y.; Ma, X.; Ma, Y.T.; Zhang, J.Y.; Xie, X. Resting Heart Rate and Long-Term Outcomes in Patients with Percutaneous Coronary Intervention: Results from a 10-Year Follow-Up of the CORFCHD-PCI Study. Cardiol. Res. Pract. 2019, 2019, 5432076. [Google Scholar] [CrossRef]
- Lahti, R.; Rankinen, J.; Lyytikäinen, L.P.; Eskola, M.; Nikus, K.; Hernesniemi, J. High-Risk ECG Patterns in ST Elevation Myocardial Infarction for Mortality Prediction. J. Electrocardiol. 2022, 74, 13–19. [Google Scholar] [CrossRef]
- Cymberknop, L.; Legnani, W.; Pessana, F.; Bia, D.; Zócalo, Y.; Armentano, R.L. Stiffness Indices and Fractal Dimension Relationship in Arterial Pressure and Diameter Time Series In-Vitro. J. Phys. Conf. Ser. 2011, 332, 012024. [Google Scholar] [CrossRef]
- Lehmann, E.D.; Hopkins, K.D.; Rawesh, A.; Joseph, R.C.; Kongola, K.; Coppack, S.W.; Gosling, R.G. Relation between Number of Cardiovascular Risk Factors/Events and Noninvasive Doppler Ultrasound Assessments of Aortic Compliance. Hypertension 1998, 32, 565–569. [Google Scholar] [CrossRef]
- Reant, P.; Dijos, M.; Donal, E.; Mignot, A.; Ritter, P.; Bordachar, P.; Dos Santos, P.; Leclercq, C.; Roudaut, R.; Habib, G.; et al. Systolic Time Intervals as Simple Echocardiographic Parameters of Left Ventricular Systolic Performance: Correlation with Ejection Fraction and Longitudinal Two-Dimensional Strain. Eur. J. Echocardiogr. 2010, 11, 834–844. [Google Scholar] [CrossRef]
- Patel, P.A.; Ambrosy, A.P.; Phelan, M.; Alenezi, F.; Chiswell, K.; Van Dyke, M.K.; Tomfohr, J.; Honarpour, N.; Velazquez, E.J. Association between Systolic Ejection Time and Outcomes in Heart Failure by Ejection Fraction. Eur. J. Heart Fail. 2020, 22, 1174–1182. [Google Scholar] [CrossRef]
- Said, S.; Hernandez, G.T. The Link between Chronic Kidney Disease and Cardiovascular Disease. J. Nephropathol. 2014, 3, 99–104. [Google Scholar] [CrossRef]
- Alkhalil, M.; McCune, C.; McClenaghan, L.; Mailey, J.; Collins, P.; Kearney, A.; Todd, M.; McKavanagh, P. Comparative Analysis of the Effect of Renal Function on the Spectrum of Coronary Artery Disease. Am. J. Med. 2020, 133, e631–e640. [Google Scholar] [CrossRef]
- Al’Aref, S.J.; Singh, G.; van Rosendael, A.R.; Kolli, K.K.; Ma, X.; Maliakal, G.; Pandey, M.; Lee, B.C.; Wang, J.; Xu, Z.; et al. Determinants of In-Hospital Mortality After Percutaneous Coronary Intervention: A Machine Learning Approach. J. Am. Heart Assoc. 2019, 8, e011160. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Park, J.S.; Choe, J.C.; Ahn, J.H.; Lee, H.W.; Oh, J.H.; Choi, J.H.; Cha, K.S.; Hong, T.J.; Jeong, M.H. Prediction of 1-Year Mortality from Acute Myocardial Infarction Using Machine Learning. Am. J. Cardiol. 2020, 133, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Weichwald, S.; Candreva, A.; Burkholz, R.; Klingenberg, R.; Räber, L.; Heg, D.; Manka, R.; Gencer, B.; Mach, F.; Nanchen, D.; et al. Improving 1-Year Mortality Prediction in ACS Patients Using Machine Learning. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Hizoh, I.; Domokos, D.; Banhegyi, G.; Becker, D.; Merkely, B.; Ruzsa, Z. Mortality Prediction Algorithms for Patients Undergoing Primary Percutaneous Coronary Intervention. J. Thorac. Dis. 2020, 12, 1706–1720. [Google Scholar] [CrossRef] [PubMed]
- Ke, J.; Chen, Y.; Wang, X.; Wu, Z.; Zhang, Q.; Lian, Y.; Chen, F. Machine Learning-Based in-Hospital Mortality Prediction Models for Patients with Acute Coronary Syndrome. Am. J. Emerg. Med. 2022, 53, 127–134. [Google Scholar] [CrossRef]
- Lee, W.; Lee, J.; Woo, S.I.; Choi, S.H.; Bae, J.W.; Jung, S.; Jeong, M.H.; Lee, W.K. Machine Learning Enhances the Performance of Short and Long-Term Mortality Prediction Model in Non-ST-Segment Elevation Myocardial Infarction. Sci. Rep. 2021, 11, 12886. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).