
Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source
2.3. Statistical Analysis
3. Results
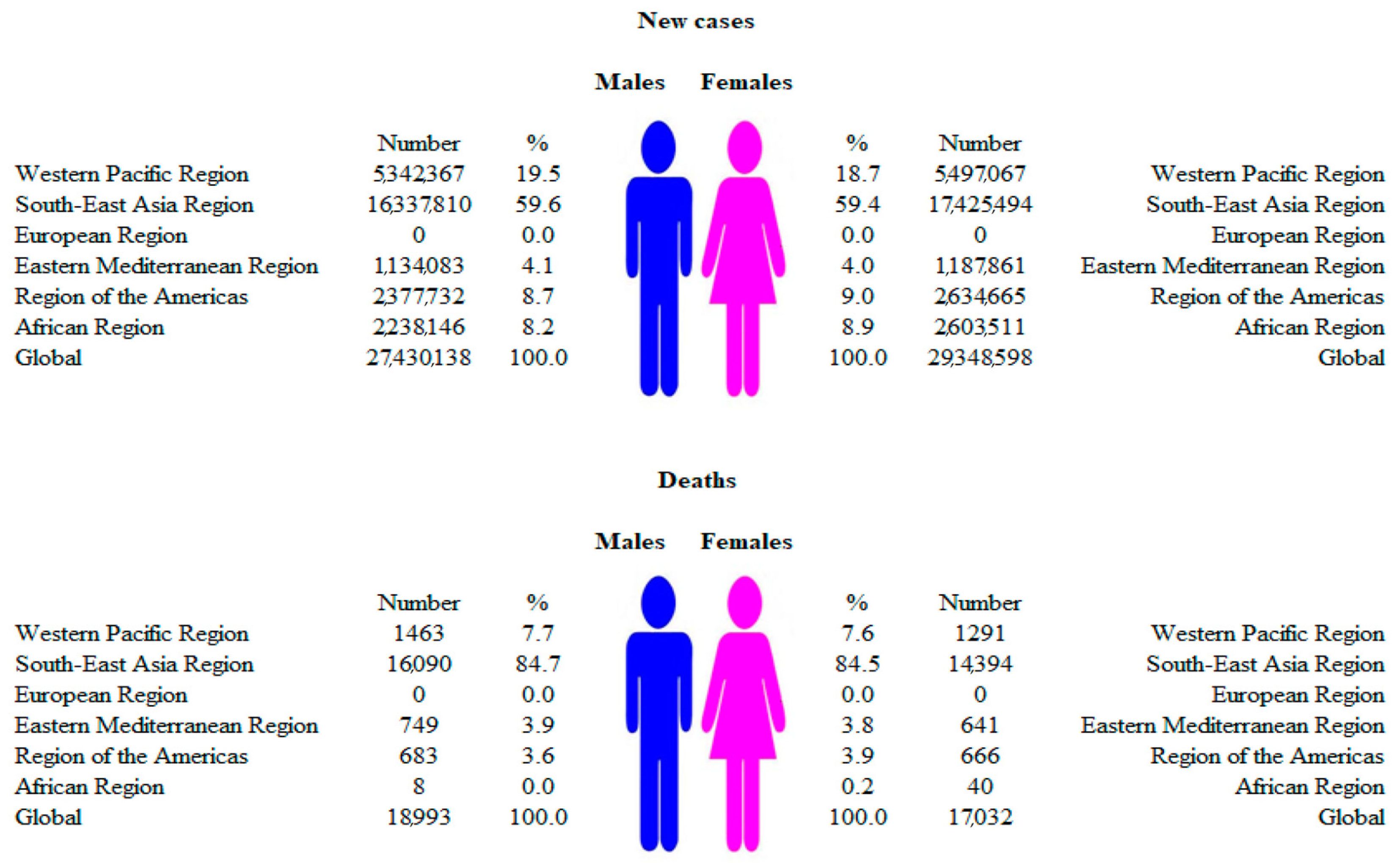
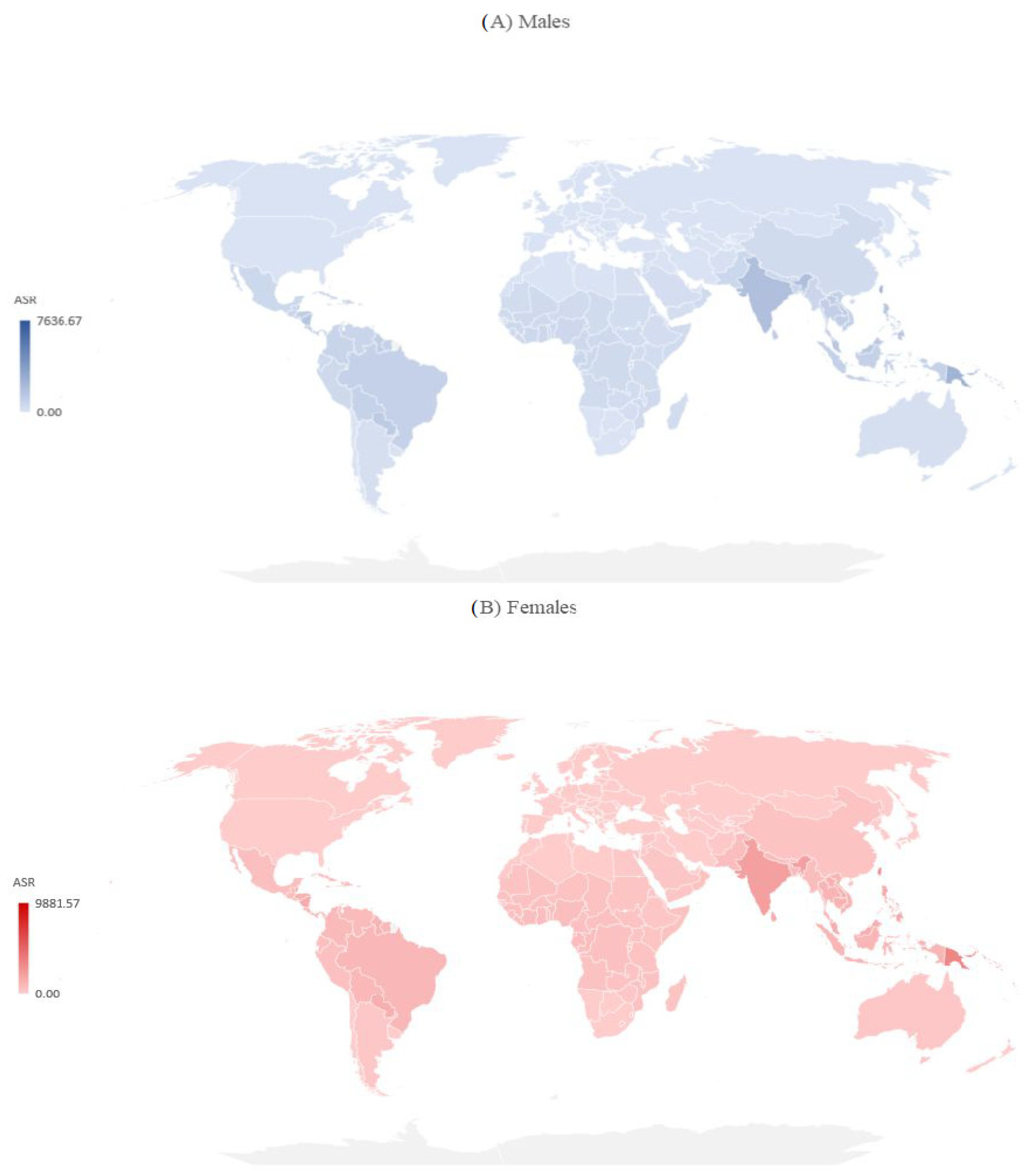
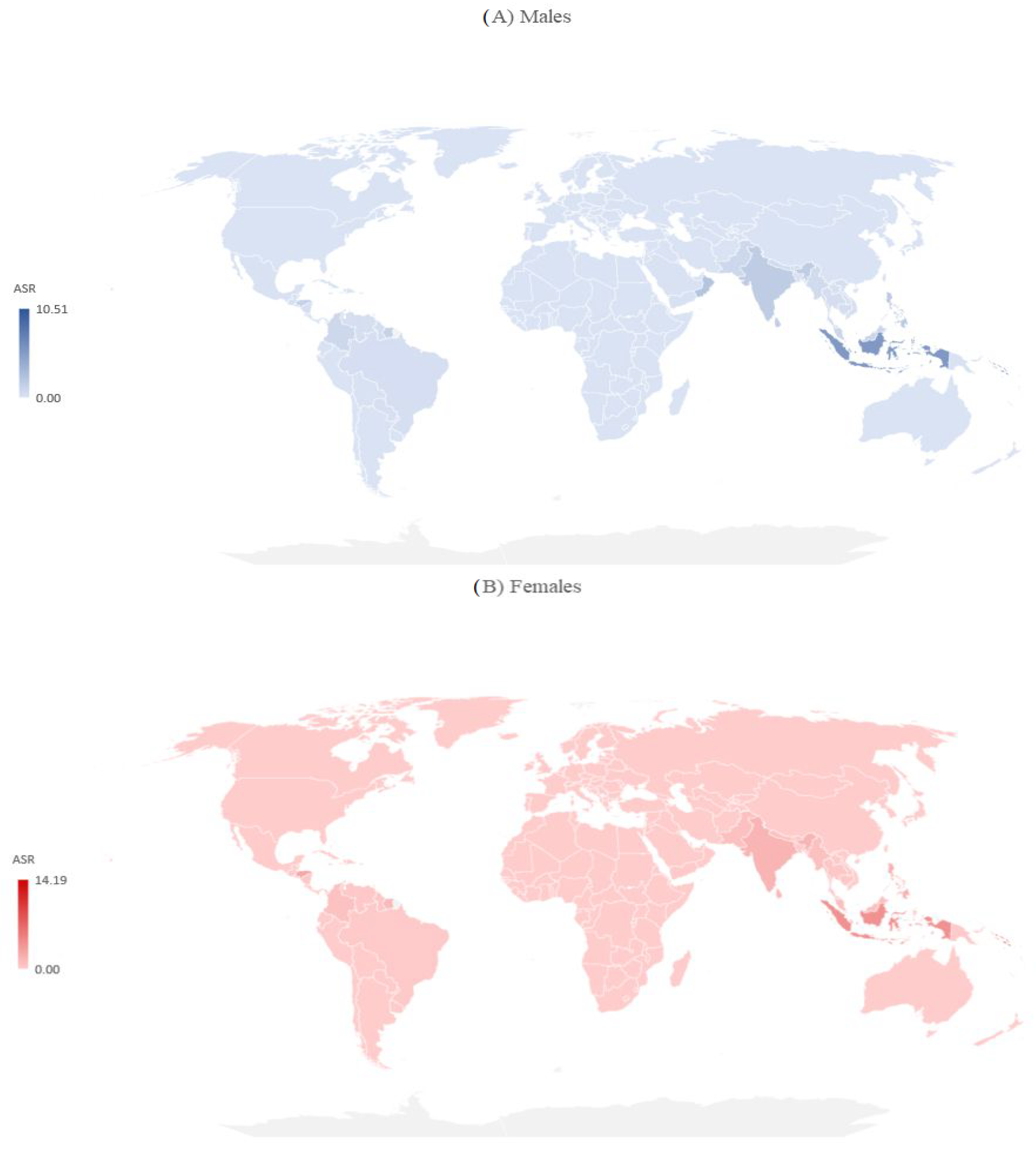
3.1. Incidence and Mortality Due to Dengue: 2019 Results
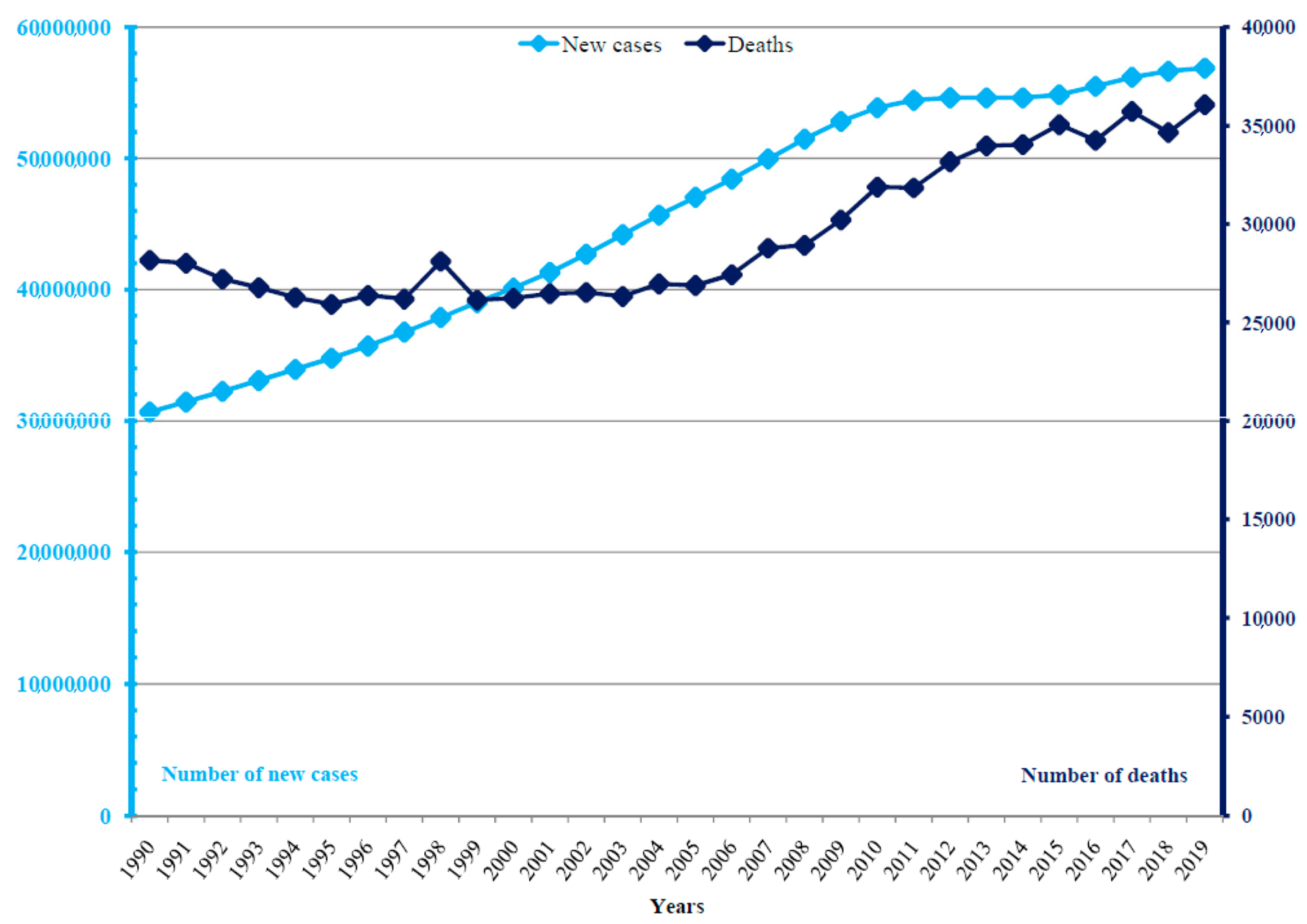
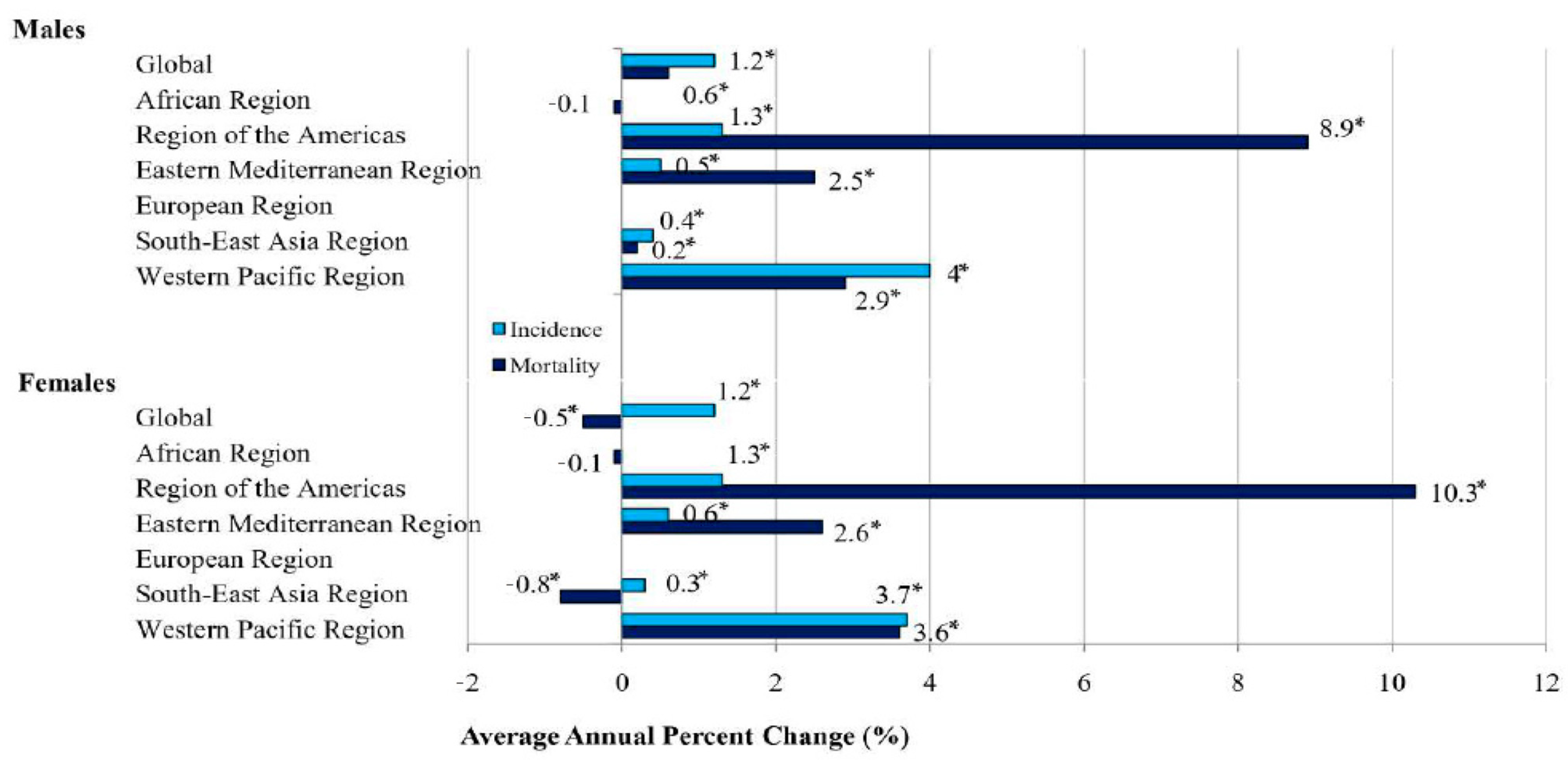
3.2. Trends of Dengue Incidence and Mortality, 1990–2019
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 27 September 2023).
- World Health Organization (WHO). Dengue and Severe Dengue; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 27 September 2023).
- Tian, N.; Zheng, J.X.; Guo, Z.Y.; Li, L.H.; Xia, S.; Lv, S.; Zhou, X.N. Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019. Trop. Med. Infect. Dis. 2022, 7, 180. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castañeda-Orjuela, C.A.; et al. The global burden of dengue: An analysis from the Global Burden of Disease Study 2013. Lancet Infect Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Gubler, D.J. Geographic expansion of dengue: The impact of international travel. Med. Clin. N. Am. 2008, 92, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Chanasit, J.; Haditsch, M.; Schoneberg, I.; Gunther, S.; Stark, K.; Frank, C. Dengue virus infection in a traveller returning from Croatia to Germany. Euro Surveill. 2010, 15, 19677. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Surveillance, Threats and Outbreaks of Dengue Fever. Available online: https://www.ecdc.europa.eu/en/dengue-fever/surveillance (accessed on 27 September 2023).
- Gjenero-Margan, I.; Aleraj, B.; Krajcar, D.; Lesnikar, V.; Klobučar, A.; Pem-Novosel, I.; Kurečić-Filipović, S.; Komparak, S.; Martić, R.; Đuričić, S.; et al. Autochthonous dengue fever in Croatia, August-September 2010. Euro Surveill. 2011, 16, 19805. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.T.; Varani, G. Structure of the dengue virus RNA promoter. RNA 2022, 28, 1210–1223. [Google Scholar] [CrossRef]
- Murugesan, A.; Manoharan, M. Dengue virus. In Emerging and Reemerging Viral Pathogens; Academic Press: Cambridge, MA, USA, 2020; pp. 281–359. [Google Scholar] [CrossRef]
- Murray, N.E.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Ni, H.; Xu, R.; Barrett, A.D.; Watowich, S.J.; Gubler, D.J.; Weaver, S.C. Evolutionary relationships of endemic/epidemic and sylvatic dengue viruses. J. Virol. 2000, 74, 3227–3234. [Google Scholar] [CrossRef]
- Paixão, E.S.; Costa, M.d.C.N.; Rodrigues, L.C.; Rasella, D.; Cardim, L.L.; Brasileiro, A.C.; Teixeira, M.G.L.C. Trends and factors associated with dengue mortality and fatality in Brazil. Rev. Soc. Bras. Med. Trop. 2015, 48, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Sotcheff, S.; Routh, A. Understanding Flavivirus Capsid Protein Functions: The Tip of the Iceberg. Pathogens 2020, 9, 42. [Google Scholar] [CrossRef]
- Sunil, S.; Sirisena, P.N.; Mahilkar, S.; Sharma, C.; Jain, J. Concurrent dengue infections: Epidemiology & clinical implications. Indian J. Med. Res. 2021, 154, 669–679. [Google Scholar] [CrossRef]
- Nujum, Z.T.; Saritha, N.; Raj, M.P.; Gayathri, A.; Nirmala, C.; Vijayakumar, K.; Varghese, S. Seroprevalence of dengue infection in pregnant women and placental antibody transfer. Med. J. Armed. Forces India 2019, 75, 90–95. [Google Scholar] [CrossRef]
- Velandia-Romero, M.L.; Coronel-Ruiz, C.; Castro-Bonilla, L.; Camacho-Ortega, S.; Calderón-Peláez, M.A.; Castellanos, A.; Olano, V.A.; Porras, A.; Arevalo-Herrera, M.; Villamil-Gómez, W.; et al. Prevalence of dengue antibodies in healthy children and adults in different Colombian endemic areas. Int. J. Infect. Dis. 2020, 91, 9–16. [Google Scholar] [CrossRef]
- Indu, P.S.; Anish, T.S.; Chintha, S.; Libu, G.K.; Lawrence, T.; Siju, N.S.; Sreekumar, E.; Santhoshkumar, A.; Aravind, R.; Saradadevi, K.L.; et al. The Burden of Dengue and Force of Infection Among Children in Kerala, India; Seroprevalence Estimates from Government of Kerala—WHO Dengue Study. Available online: https://ssrn.com/abstract=4325236 (accessed on 25 February 2024). [CrossRef]
- Guzman, M.G.; Alvarez, M.; Halstead, S.B. Secondary infection as a risk factor for dengue hemorrhagic fever/dengue shock syndrome: An historical perspective and role of antibody-dependent enhancement of infection. Arch. Virol. 2013, 158, 1445–1459. [Google Scholar] [CrossRef] [PubMed]
- Guy, B.; Lang, J.; Saville, M.; Jackson, N. Vaccination Against Dengue: Challenges and Current Developments. Annu. Rev. Med. 2016, 67, 387–404. [Google Scholar] [CrossRef]
- WHO. Dengue Vaccine: WHO position paper, September 2018—Recommendations. Vaccine 2019, 37, 4848–4849. [Google Scholar] [CrossRef]
- Yeh, C.-Y.; Lu, B.-Z.; Liang, W.-J.; Shu, Y.-C.; Chuang, K.-T.; Chen, P.-L.; Ko, W.-C.; Ko, N.-Y. Trajectories of hepatic and coagulation dysfunctions related to a rapidly fatal outcome among hospitalized patients with dengue fever in Tainan, 2015. PLoS Negl. Trop. Dis. 2019, 13, e0007817. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Tanni, K.N.; Roy, T.; Islam, R.; Rumi, A.A.R.; Sakib, M.S.; Quader, M.A.; Bhuiyan, N.-U.; Alam Shobuj, I.; Rahman, A.S.; et al. Knowledge, Attitude and Practices Towards Dengue Fever Among Slum Dwellers: A Case Study in Dhaka City, Bangladesh. Int. J. Public Health 2023, 68, 1605364. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A. Economic and disease burden of dengue in Southeast Asia. PLoS Negl. Trop. Dis. 2013, 7, e2055. [Google Scholar] [CrossRef]
- Bouzid, M.; Colón-González, F.J.; Lung, T.; Lake, I.R.; Hunter, P.R. Climate change and the emergence of vector-borne diseases in Europe: Case study of dengue fever. BMC Public Health 2014, 14, 781. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Zhan, J.; Chen, L.; Chen, H.; Cheng, S. Global, regional, and national dengue burden from 1990 to 2017: A systematic analysis based on the global burden of disease study 2017. EClinicalMedicine 2021, 32, 100712. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 27 September 2023).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Fay, M.P.; Yu, B.; Barrett, M.J.; Feuer, E.J. Comparability of segmented line regression models. Biometrics 2004, 60, 1005–1014. [Google Scholar] [CrossRef]
- Warkentien, T.; Pavlicek, R. Dengue Fever: Historical Perspective and the Global Response. J. Infect. Dis. Epidemiol. 2016, 2, 15. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Du, M.; Jing, W.; Liu, M.; Liu, J. The Global Trends and Regional Differences in Incidence of Dengue Infection from 1990 to 2019: An Analysis from the Global Burden of Disease Study 2019. Infect. Dis. Ther. 2021, 10, 1625–1643. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Quam, M.B.M.; Zhang, T.; Sang, S. Global burden for dengue and the evolving pattern in the past 30 years. J. Travel Med. 2021, 28, taab146. [Google Scholar] [CrossRef]
- Pilot, E.; Nittas, V.; Murthy, G.V.S. The Organization, Implementation, and Functioning of Dengue Surveillance in India-A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 661. [Google Scholar] [CrossRef]
- Waggoner, J.J.; Gresh, L.; Vargas, M.J.; Ballesteros, G.; Tellez, Y.; Soda, K.J.; Sahoo, M.K.; Nuñez, A.; Balmaseda, A.; Harris, E.; et al. Viremia and Clinical Presentation in Nicaraguan Patients Infected with Zika Virus, Chikungunya Virus, and Dengue Virus. Clin. Infect. Dis. 2016, 63, 1584–1590. [Google Scholar] [CrossRef]
- Liu-Helmersson, J.; Stenlund, H.; Wilder-Smith, A.; Rocklöv, J. Vectorial capacity of Aedes aegypti: Effects of temperature and implications for global dengue epidemic potential. PLoS ONE 2014, 9, e89783. [Google Scholar] [CrossRef]
- Xu, L.; Stige, L.C.; Chan, K.-S.; Zhou, J.; Yang, J.; Sang, S.; Wang, M.; Yang, Z.; Yan, Z.; Jiang, T.; et al. Climate variation drives dengue dynamics. Proc. Natl. Acad. Sci. USA 2017, 114, 113–118. [Google Scholar] [CrossRef]
- Marinho, R.d.S.S.; Duro, R.L.S.; Mota, M.T.d.O.; Hunter, J.; Diaz, R.S.; Kawakubo, F.S.; Komninakis, S.V. Environmental Changes and the Impact on the Human Infections by Dengue, Chikungunya and Zika Viruses in Northern Brazil, 2010–2019. Int. J. Environ. Res. Public Health 2022, 19, 12665. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. RAPID RISK ASSESSMENT Local Transmission of Dengue Fever in France and Spain—2018—22 October 2018. Stockholm: ECDC. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/08-10-2018-RRA-Dengue-France.pdf (accessed on 25 February 2024).
- Getahun, A.; Batikawai, A.; Nand, D.; Khan, S.; Sahukhan, A.; Faktaufon, D. Dengue in Fiji: Epidemiology of the 2014 DENV-3 outbreak. West. Pac. Surveill. Response J. 2019, 10, 31–38. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Vaccines and Immunization: Dengue; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/news-room/questions-and-answers/item/dengue-vaccines (accessed on 25 February 2024).
- European Medicines Agency (EMA). Qdenga, Dengue Tetravalent Vaccine (Live, Attenuated). Amsterdam: The Netherlands. 2022. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/qdenga (accessed on 25 February 2024).
- La Ruche, G.; Souarès, Y.; Armengaud, A.; Peloux-Petiot, F.; Delaunay, P.; Desprès, P.; Lenglet, A.; Jourdain, F.; Leparc-Goffart, I.; Charlet, F.; et al. First two autochthonous dengue virus infections in metropolitan France, September 2010. Euro Surveill. 2010, 15, 19676. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Dengue Outbreak in Madeira, Portugal. Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/dengue-madeira-ECDC-mission-2013.pdf (accessed on 25 February 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Males | Females | ||||
|---|---|---|---|---|---|---|
| Age-Specific Rates | AAPC (95% CI) | Age-Specific Rates | AAPC (95% CI) | |||
| 1990 | 2019 | 1990 | 2019 | |||
| Incidence | ||||||
| 0–9 | 573.18 | 638.94 | +0.5 * (0.2 to 0.7) | 642.01 | 699.92 | +0.4 * (0.1 to 0.7) |
| 10–24 | 673.84 | 944.35 | +1.4 * (1.2 to 1.5) | 744.05 | 1004.60 | +1.2 * (1.1 to 1.4) |
| 25–49 | 476.92 | 680.25 | +1.5 * (1.4 to 1.7) | 538.00 | 738.80 | +1.4 * (1.2 to 1.6) |
| 50–69 | 409.88 | 530.57 | +1.0 * (0.9 to 1.1) | 435.99 | 599.59 | +1.2 * (1.1 to 1.3) |
| 70+ | 425.57 | 607.24 | +1.4 * (1.3 to 1.5) | 381.84 | 631.87 | +2.1 * (1.9 to 2.2) |
| Age-standardized rates | ||||||
| All ages | 532.12 | 712.21 | +1.2 * (1.0 to 1.4) | 584.29 | 769.95 | +1.2 * (1.0 to 1.4) |
| Mortality | ||||||
| 0–9 | 1.19 | 0.70 | −1.4 * (−1.6 to −1.2) | 1.83 | 0.71 | −3.1 * (−3.2 to −2.9) |
| 10–24 | 0.21 | 0.29 | +1.2 * (1.0 to 1.4) | 0.20 | 0.21 | +0.2 * (0.1 to 0.3) |
| 25–49 | 0.20 | 0.32 | +2.1 * (1.9 to 2.2) | 0.17 | 0.24 | +1.5 * (1.2 to 1.7) |
| 50–69 | 0.34 | 0.54 | +2.0 * (1.8 to 2.3) | 0.27 | 0.46 | +2.3 * (1.9 to 2.6) |
| 70+ | 0.94 | 1.65 | +2.3 * (2.0 to 2.6) | 0.66 | 1.61 | +3.5 * (3.2 to 3.9) |
| Age-standardized rates | ||||||
| All ages | 0.47 | 0.52 | +0.6 * (0.5 to 0.8) | 0.54 | 0.44 | −0.5 * (−0.7 to −0.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilic, I.; Ilic, M. Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study. Medicina 2024, 60, 425. https://doi.org/10.3390/medicina60030425
Ilic I, Ilic M. Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study. Medicina. 2024; 60(3):425. https://doi.org/10.3390/medicina60030425
Chicago/Turabian StyleIlic, Irena, and Milena Ilic. 2024. "Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study" Medicina 60, no. 3: 425. https://doi.org/10.3390/medicina60030425
APA StyleIlic, I., & Ilic, M. (2024). Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study. Medicina, 60(3), 425. https://doi.org/10.3390/medicina60030425