

Bleeding Events Associated with Rivaroxaban Therapy in Naive Patients with Nonvalvular Atrial Fibrillation: A Longitudinal Study from a Genetic Perspective with INR Follow-Up



Abstract
1. Introduction
2. Results
2.1. Plasma Level of Rivaroxaban and SNPs of ABCB1 and CYP3A5 Genes
2.2. Effect of ABCB1 Gene Polymorphism on Coagulation Parameters
2.3. Clinical Outcomes and Frequency of ADRs and SNPs
2.3.1. Clinical Outcomes/Clinical Success
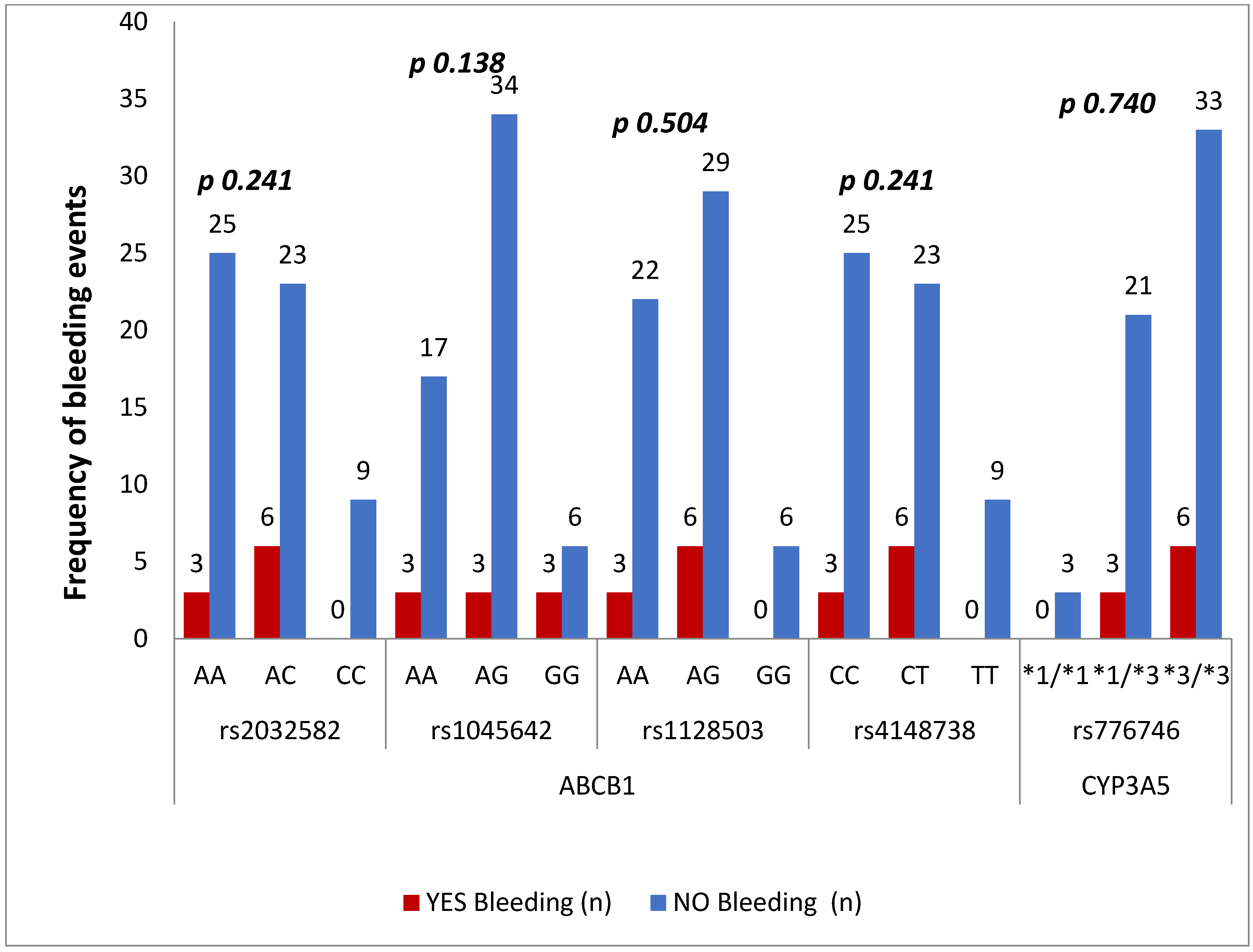
2.3.2. Frequency of ADRs
3. Discussions
4. Materials and Methods
4.1. Participant Recruitment
4.1.1. Inclusion Criteria
4.1.2. Exclusion Criteria
4.2. Study Design
4.3. Analysis of Plasma Concentrations
4.4. Extraction of Genomic DNA
4.5. Sanger Sequencing
4.6. Statistical Analysis
5. Conclusions
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Nattel, S. New ideas about atrial fibrillation 50 years on. Nature 2002, 415, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Amit, G.; Field, T.S. Atrial fibrillation and stroke: How much atrial fibrillation is enough to cause a stroke? Curr. Opin. Neurol. 2020, 33, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Pritchett, E.L. Management of atrial fibrillation. N. Engl. J. Med. 1992, 326, 1264–1271. [Google Scholar] [PubMed]
- Kanuri, S.H.; Kreutz, R.P. Pharmacogenomics of Novel Direct Oral Anticoagulants: Newly Identified Genes and Genetic Variants. J. Pers. Med. 2019, 9, 7. [Google Scholar] [CrossRef]
- Dimatteo, C.; D’Andrea, G.; Vecchione, G.; Paoletti, O.; Tiscia, G.L.; Santacroce, R.; Correale, M.; Brunetti, N.; Grandone, E.; Testa, S.; et al. ABCB1 SNP rs4148738 modulation of apixaban interindividual variability. Thromb. Res. 2016, 145, 24–26. [Google Scholar] [CrossRef]
- Ueshima, S.; Hira, D.; Kimura, Y.; Fujii, R.; Tomitsuka, C.; Yamane, T.; Tabuchi, Y.; Ozawa, T.; Itoh, H.; Ohno, S.; et al. Population pharmacokinetics and pharmacogenomics of apixaban in Japanese adult patients with atrial fibrillation. Br. J. Clin. Pharmacol. 2018, 84, 1301–1312. [Google Scholar] [CrossRef]
- Lorenzini, K.I.; Daali, Y.; Fontana, P.; Desmeules, J.; Samer, C. Rivaroxaban-Induced Hemorrhage Associated with ABCB1 Genetic Defect. Front. Pharmacol. 2016, 7, 494. [Google Scholar] [CrossRef]
- Greig, S.L.; Garnock-Jones, K.P. Apixaban: A Review in Venous Thromboembolism. Drugs 2016, 76, 1493–1504. [Google Scholar] [CrossRef]
- Picard, N.; Boyer, J.-C.; Etienne-Grimaldi, M.-C.; Guellec, C.B.-L.; Thomas, F.; Loriot, M.-A. Pharmacogenetics-based personalized therapy: Levels of evidence and recommendations from the French Network of Pharmacogenetics (RNPGx). Therapies 2017, 72, 185–192. [Google Scholar] [CrossRef]
- Leschziner, G.D.; Andrew, T.; Pirmohamed, M.; Johnson, M.R. ABCB1 genotype and PGP expression, function and therapeutic drug response: A critical review and recommendations for future research. Pharmacogenom. J. 2007, 7, 154–179. [Google Scholar] [CrossRef]
- Ganoci, L.; Božina, T.; Skvrce, N.M.; Lovrić, M.; Mas, P.; Božina, N. Genetic polymorphisms of cytochrome P450 enzymes: CYP2C9, CYP2C19, CYP2D6, CYP3A4, and CYP3A5 in the Croatian population. Drug Metab. Pers. Ther. 2017, 32, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Xiang, Q.; Mu, G.; Ma, L.; Chen, S.; Zhou, S.; Hu, K.; Zhang, Z.; Cui, Y.; Jiang, J. Effect of ABCB1 Genotypes on the Pharmacokinetics and Clinical Outcomes of New Oral Anticoagulants: A Systematic Review and Meta-analysis. Curr. Pharm. Des. 2018, 24, 3558–3565. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, M.; Chen, H.; Wang, F. Influence of ABCB1 Gene Polymorphism on Rivaroxaban Blood Concentration and Hemorrhagic Events in Patients with Atrial Fibrillation. Front. Pharmacol. 2021, 12, 639854. [Google Scholar] [CrossRef] [PubMed]
- Shnayder, N.A.; Petrova, M.M.; Bochanova, E.N.; Zimnitskaya, O.V.; Savinova, A.; Pozhilenkova, E.; Nasyrova, R. Pharmacogenetics of Direct Oral Anticoagulants. In Pharmacogenetics; InTech Open: London, UK, 2021. [Google Scholar]
- Lund, M.; Petersen, T.S.; Dalhoff, K.P. Clinical Implications of P-Glycoprotein Modulation in Drug–Drug Interactions. Drugs 2017, 77, 859–883. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, B.; Salomone, L.; Cini, M.; Guazzaloca, G.; Legnani, C. Observational Study of the Inter-Individual Variability of the Plasma Concentrations of Direct Oral Anticoagulants (Dabigatran, Rivaroxaban, Apixaban) and the Effect of rs4148738 Polymorphism of ABCB1. J. Cardiol. Ther. 2019, 7, 8–14. [Google Scholar] [CrossRef]
- Eichelbaum, M.; Fromm, M.F.; Schwab, M. Clinical Aspects of the MDR1 (ABCB1) Gene Polymorphism. Ther. Drug Monit. 2004, 26, 180–185. [Google Scholar] [CrossRef]
- Wu, T.; Wu, S.; Li, L.; Xiang, J.; Wang, N.; Chen, W.; Zhang, J. The impact of ABCB1, CYP3A4/5 and ABCG2 gene polymorphisms on rivaroxaban trough concentrations and bleeding events in patients with non-valvular atrial fibrillation. Hum. Genom. 2023, 17, 59. [Google Scholar] [CrossRef]
- Sychev, D.; Minnigulov, R.; Bochkov, P.; Ryzhikova, K.; Yudina, I.; Lychagin, A.; Morozova, T. Effect of CYP3A4, CYP3A5, ABCB1 Gene Polymorphisms on Rivaroxaban Pharmacokinetics in Patients Undergoing Total Hip and Knee Replacement Surgery. High Blood Press. Cardiovasc. Prev. 2019, 26, 413–420. [Google Scholar] [CrossRef]
- Nakagawa, J.; Kinjo, T.; Iizuka, M.; Ueno, K.; Tomita, H.; Niioka, T. Impact of gene polymorphisms in drug-metabolizing enzymes and transporters on trough concentrations of rivaroxaban in patients with atrial fibrillation. Basic Clin. Pharmacol. Toxicol. 2021, 128, 297–304. [Google Scholar] [CrossRef]
- Sennesael, A.-L.; Panin, N.; Vancraeynest, C.; Pochet, L.; Spinewine, A.; Haufroid, V.; Elens, L. Effect of ABCB1 genetic polymorphisms on the transport of rivaroxaban in HEK293 recombinant cell lines. Sci. Rep. 2018, 8, 10514. [Google Scholar] [CrossRef]
- Park, J.-Y.; Cha, Y.-J.; Kim, K.-A. CYP3A5* 3 polymorphism and its clinical implications and pharmacokinetic role. Transl. Clin. Pharmacol. 2014, 22, 3–7. [Google Scholar] [CrossRef]
- Sychev, D.A.; Minnigulov, R.; Ryzhikova, K.A.; Yudina, I.Y.; Lychagin, A.V.; Morozova, T. Evaluation of the rivaroxaban-influenced effect of abcb1 and CYP3A5 gene polymorphisms on prothrombin time in patients after total hip or knee replacement surgery. Bull. Russ. State Med. Univ. 2018, 4, 105–109. [Google Scholar] [CrossRef]
- Nakayama, M.; Miyagawa, H.; Kuranami, Y.; Tsunooka-Ota, M.; Yamaguchi, Y.; Kojima-Aikawa, K. Annexin A4 inhibits sulfatide-induced activation of coagulation factor XII. J. Thromb. Haemost. 2020, 18, 1357–1369. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, M.A.; Kong, X.; Haymart, B.; Kaatz, S.; Krol, G.; Kozlowski, J.; Dahu, M.; Ali, M.; Almany, S.; Alexandris-Souphis, T.; et al. Comparison of temporary interruption with continuation of direct oral anticoagulants for low bleeding risk procedures. Thromb. Res. 2021, 203, 27–32. [Google Scholar] [CrossRef]
- Johnson, J.A.; Cavallari, L.H. Pharmacogenetics and Cardiovascular Disease—Implications for Personalized Medicine. Pharmacol. Rev. 2013, 65, 987–1009. [Google Scholar] [CrossRef]
- Cascorbi, I. Role of pharmacogenetics of ATP-binding cassette transporters in the pharmacokinetics of drugs. Pharmacol. Ther. 2006, 112, 457–473. [Google Scholar] [CrossRef]
- Kryukov, A.V.; Sychev, D.A.; Andreev, D.A.; Ryzhikova, K.A.; Grishina, E.A.; Ryabova, A.V.; Loskutnikov, M.A.; Smirnov, V.V.; Konova, O.D.; Matsneva, I.A.; et al. Influence of ABCB1 and CYP3A5 gene polymorphisms on pharmacokinetics of apixaban in patients with atrial fibrillation and acute stroke. Pharmacogenom. Pers. Med. 2018, 11, 43–49. [Google Scholar] [CrossRef]
- Li, X.; Gu, Z.; Wang, Z.; Xu, Q.; Ma, C.; Lv, Q. Mutant CYP3A4/5 correlated with clinical outcomes by affecting rivaroxaban pharmacokinetics and pharmacodynamics in patients with atrial fibrillation. Cardiovasc. Drugs Ther. 2023, 37, 1–11. [Google Scholar] [CrossRef]
- Ingason, A.B.; Hreinsson, J.P.; Agustsson, A.S.; Lund, S.H.; Rumba, E.; Palsson, D.A.; Reynisson, I.E.; Gudmundsdottir, B.R.; Onundarson, P.T.; Bjornsson, E.S. Comparison of the effectiveness and safety of direct oral anticoagulants: A nationwide propensity score–weighted study. Blood Adv. 2023, 7, 2564–2572. [Google Scholar] [CrossRef]
- Wells, G.; Coyle, D.; Cameron, C.; Steiner, S.; Coyle, K.; Kelly, S.; Tang, A.; Healey, J.; Hsieh, S.C.; van Berkom, J. Safety, Effectiveness, and Cost-Effectiveness of New Oral Anticoagulants Compared with Warfarin in Preventing Stroke and Other Cardiovascular Events in Patients with Atrial Fibrillation; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2013. [Google Scholar]
- Cini, M.; Legnani, C.; Padrini, R.; Cosmi, B.; Dellanoce, C.; De Rosa, G.; Marcucci, R.; Pengo, V.; Poli, D.; Testa, S.; et al. DOAC plasma levels measured by chromogenic anti-Xa assays and HPLC-UV in apixaban-and rivaroxaban-treated patients from the START-Register. Int. J. Lab. Hematol. 2020, 42, 214–222. [Google Scholar] [CrossRef]
- Gouveia, F.; Bicker, J.; Santos, J.; Rocha, M.; Alves, G.; Falcão, A.; Fortuna, A. Development, validation and application of a new HPLC-DAD method for simultaneous quantification of apixaban, dabigatran, edoxaban and rivaroxaban in human plasma. J. Pharm. Biomed. Anal. 2020, 181, 113109. [Google Scholar] [CrossRef] [PubMed]
- El-Shair, S.; Al Shhab, M.; Zayed, K.; Alsmady, M.; Zihlif, M. Association between CYP3A4 and CYP3A5 genotypes and cyclosporine’s blood levels and doses among Jordanian kidney transplanted patients. Curr. Drug Metab. 2019, 20, 682–694. [Google Scholar] [CrossRef] [PubMed]
- Zmorzynski, S.; Wojcierowska-Litwin, M.; Popek-Marciniec, S.; Szudy-Szczyrek, A.; Styk, W.; Chocholska, S.; Filip, A.A. The relationship of ABCB1/MDR1 and CYP1A1 variants with the risk of disease development and shortening of overall survival in patients with multiple myeloma. J. Clin. Med. 2021, 10, 5276. [Google Scholar] [CrossRef]
- Riemann, K.; Adamzik, M.; Frauenrath, S.; Egensperger, R.; Schmid, K.W.; Brockmeyer, N.H.; Siffert, W. Comparison of manual and automated nucleic acid extraction from whole-blood samples. J. Clin. Lab. Anal. 2007, 21, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Jamil, A.; Saleh Faisal, M.; Zaman, G.; Khan, M. Decoding the genome: Cyp3a5 rs15524 polymorphism and how it affects plasma carbamazepine levels in patients with epilepsy in Khyber Pakhtunkhwa. Afr. J. Biomed. Res. 2024, 31, 1187–1194. [Google Scholar]
- Faisal, M.S.; Jamil, A.; Ali, N.; Alshahrani, A.M.; Almarshad, F. Distribution pattern of UGT1A6 and UGT2B7 gene polymorphism and its impact on the pharmacokinetics of valproic acid and carbamazepine: Prospective genetic association study conducted in Pakistani patients with epilepsy. Gene 2024, 892, 147886. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
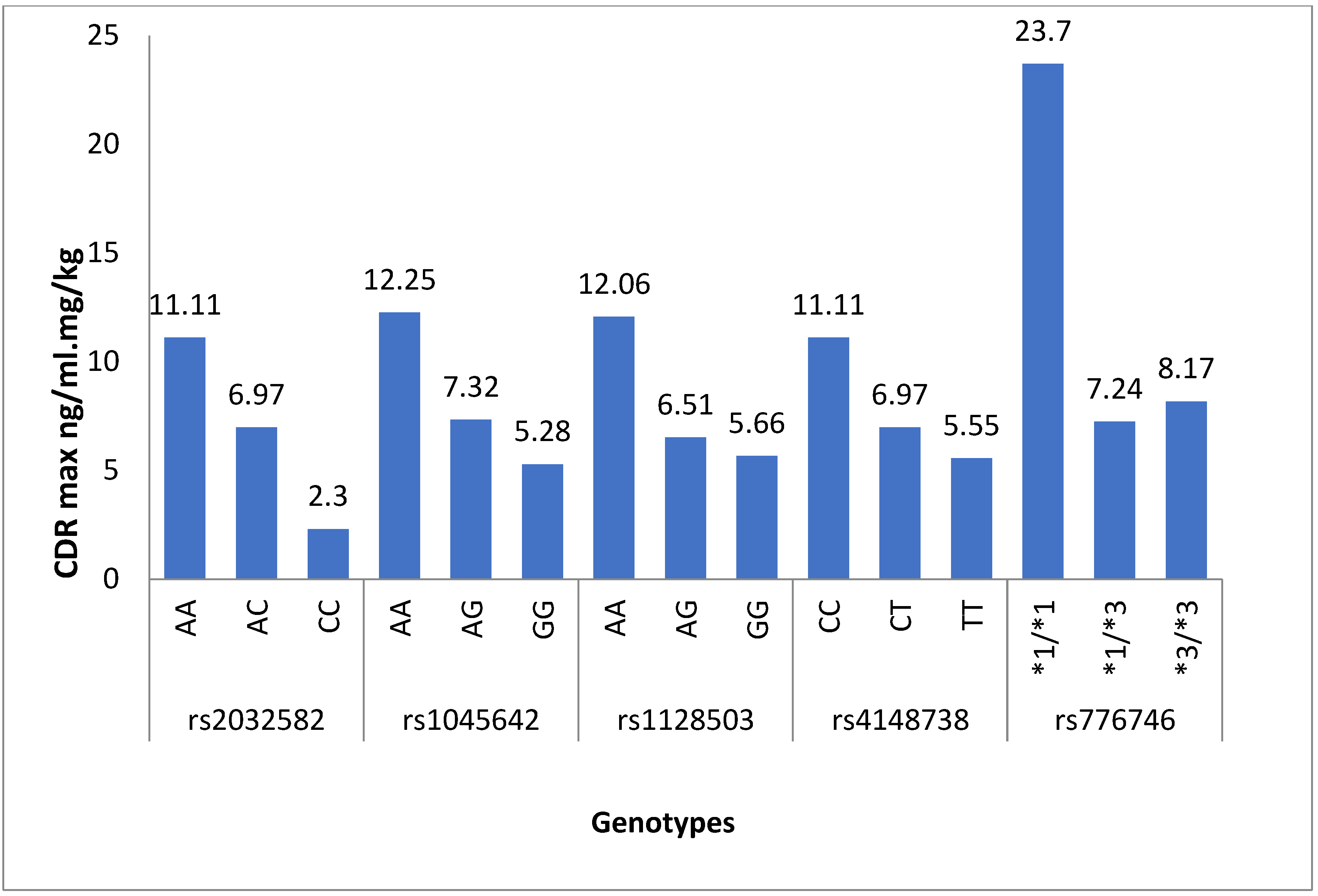
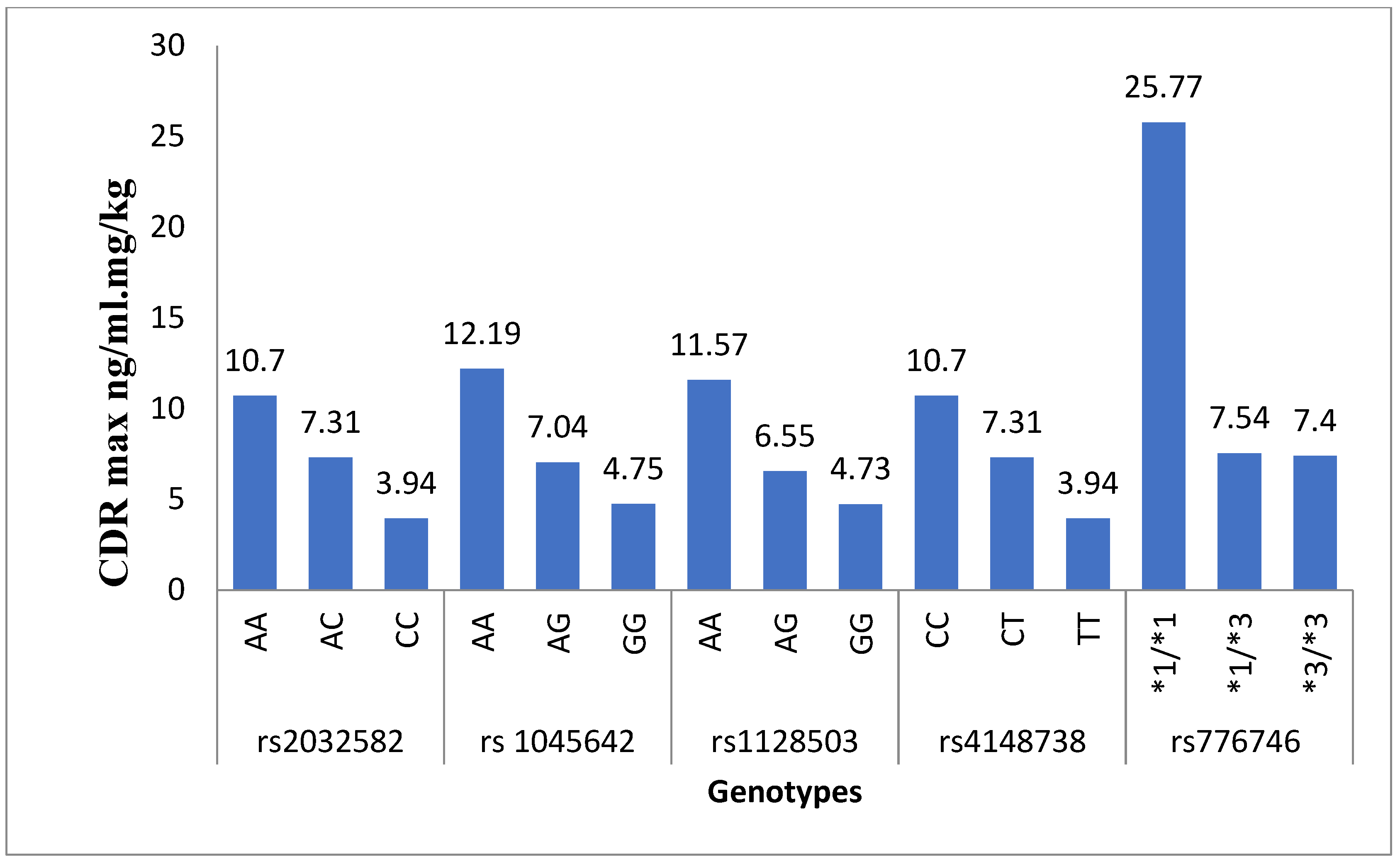
| GENES | SNPs | Genotypes | CDR Max (3 h) | p-Values | CDR Steady State (1 Month) | p-Values |
|---|---|---|---|---|---|---|
| ABCB1 | rs1128503 | AA | 12.06 ± 7.31 | - | 11.57 ± 8.24 | - |
| AG | 6.51 ± 4.15 | 0.001 * | 6.55 ± 3.56 | 0.004 * | ||
| GG | 5.66 ± 2.42 | 0.034 * | 4.73 ± 0.74 | 0.029 * | ||
| rs1045642 | AA | 12.25 ± 8.24 | - | 12.19 ± 9.05 | - | |
| AG | 7.32 ± 4.17 | 0.007 * | 7.04 ± 3.62 | 0.005 * | ||
| GG | 5.28± 2.69 | 0.008 * | 4.75 ± 1.19 | 0.005 * | ||
| rs2032582 | AA | 11.11 ± 7.43 | - | 10.70 ± 8.18 | - | |
| AC | 6.97 ± 4.35 | 0.022 * | 7.31 ± 3.48 | 0.081 | ||
| CC | 2.30 ± 0.76 | 0.036 * | 3.94 ± 1.10 | 0.010 * | ||
| rs4148738 | CC | 11.11 ± 7.43 | - | 10.70 ± 8.18 | - | |
| CT | 6.97 ± 4.35 | 0.022 * | 7.31 ± 3.48 | 0.081 | ||
| TT | 5.55 ± 2.30 | 0.036 * | 3.94 ± 1.10 | 0.010 * | ||
| CYP3A5 | rs776746 | *1/*1 | 23.70 ± 4.32 | - | 25.77 ± 3.31 | - |
| *1/*3 | 7.24 ± 6.16 | 0.001 * | 7.54 ± 6.37 | 0.001 * | ||
| *3/*3 | 8.17 ± 4.57 | 0.001 * | 7.40 ± 4.05 | 0.001 * |
| CYP3A5 rs776746 | ABCB1 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rs2032582 | rs1045642 | rs1128503 | rs4148738 | |||||||||
| AA | AC | CC | AA | AG | GG | AA | AG | GG | CC | CT | TT | |
| *1/*1 | 237.03 ± 0.12 | - | - | 237.03 ± 0.12 | - | - | 237.03 ± 0.12 | - | - | 237.03 ± 0.12 | - | - |
| *1/*3 | 132.79 ± 62.39 | 121.27 ± 85.96 | 53.00 ± 0.14 | 137.56 ± 79.81 | 127.28 ± 66.52 | 36.48 ± 0.14 | 155.49 ± 55.08 | 96.30 ± 72.38 | - | 132.79 ± 62.39232 | 121.27 ± 85.96 | 53.00 ± 0.13 |
| *3/*3 | 167.64 ± 86.83 | 110.44 ± 39.66 | 120.50 ± 2.63 | 147.40 ± 78.24 | 125.75 ± 62.29 | 36.48 ± 0.14 | 167.64 ± 86.83 | 118.52 ± 35.46 | 93.54 ± 26.89 | 167.64 ± 86.83 | 110.44 ± 39.66 | 120.50 ± 2.63 |
| CYP3A5 rs776746 | ABCB1 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rs2032582 | rs1045642 | rs1128503 | rs4148738 | |||||||||
| AA | AC | CC | AA | AG | GG | AA | AG | GG | CC | CT | TT | |
| *1/*1 | 257.75 ± 0.23 | - | - | 257.75 ± 0.23 | - | - | 257.75 ± 0.23 | - | - | 257.7588 ± 0.23 | - | - |
| *1/*3 | 124.26 ± 64.36 | 139.15 ± 63.43 | 64.74 ± 0.21 | 148.86 ± 87.48 | 113.60 ± 57.59 | 113.49 ± 0.21 | 142.68 ± 64.57 | 110.23 ± 60.37 | - | 124.26 ± 64.36 | 139.15 ± 63.43 | 64.74 ± 0.25 |
| *3/*3 | 167.64 ± 86.83 | 119.19 ± 57.65 | 72.35 ± 9.70 | 128.73 ± 69.11 | 131.89 ± 68.52 | 113.49 ± 0.21 | 148.75 ± 79.80 | 116.57 ± 59.80 | 81.10 ± 0.12 | 148.75 ± 79.80 | 119.19 ± 57.65 | 72.35 ± 9.70 |
| GENES | SNPs | Genotypes | PT at 3 h (s) (11–13.5 s) | p-Values | INR at 3 h (2–3) | p-Values | APTT at 3 h (s) (26–34 s) | p-Values |
|---|---|---|---|---|---|---|---|---|
| ABCB1 | rs1128503 | AA | 18.00 ± 2.57 | - | 1.49 ± 0.24 | - | 34.78 ± 6.48 | - |
| AG | 23.50 ± 9.61 | 0.015 * | 2.05 ± 0.97 | 0.013 * | 34.24 ± 10.46 | 0.972 | ||
| GG | 16.50 ± 3.28 | 0.894 | 1.38 ± 0.26 | 0.941 | 33.00 ± 7.66 | 0.900 | ||
| rs1045642 | AA | 19.41 ± 4.20 | - | 1.60 ± 0.36 | - | 40.25 ± 11.32 | - | |
| AG | 20.85 ± 9.72 | 0.782 | 1.81 ± 0.98 | 0.593 | 31.30 ± 6.09 | 0.001 * | ||
| GG | 23.53 ± 3.09 | 0.389 | 2.06 ± 0.33 | 0.302 | 33.63 ± 5.26 | 0.104 | ||
| rs2032582 | AA | 18.96 ± 3.73 | - | 1.57 ± 0.32 | - | 37.66 ± 10.45 | - | |
| AC | 22.29 ± 10.82 | 0.242 | 1.95 ± 1.08 | 0.152 | 32.46 ± 4.91 | 0.059 * | ||
| CC | 21.56 ± 3.55 | 0.655 | 1.85 ± 0.38 | 0.607 | 30.00 ± 10.21 | 0.053 * | ||
| rs4148738 | CC | 18.96 ± 3.73 | - | 1.57 ± 0.32 | - | 37.66 ± 10.45 | - | |
| CT | 22.29 ± 10.82 | 0.242 | 1.95 ± 1.08 | 0.152 | 32.46 ± 4.91 | 0.059 * | ||
| TT | 21.56 ± 3.55 | 0.655 | 1.85 ± 0.38 | 0.607 | 30.00 ± 10.21 | 0.053 * | ||
| CYP3A5 | rs776746 | *1/*1 | 15.00 ± 3.21 | - | 1.20 ± 1.20 | - | 33.00 ± 4.31 | - |
| *1/*3 | 24.53 ± 10.87 | 0.090 | 2.15 ± 1.10 | 0.095 | 33.31 ± 12.29 | 0.998 | ||
| *3/*3 | 18.91 ± 4.06 | 0.644 | 1.59 ± 0.39 | 0.637 | 35.06 ± 6.31 | 0.920 |
| GENES | SNPs | Genotypes | PT at 1 Month (s) (11–13.5 s) | p-Values | INR at 1 Month (2–3) | p-Values | aPTT at 1 Month (s) (26–34 s) | p-Values |
|---|---|---|---|---|---|---|---|---|
| ABCB1 | rs1128503 | AA | 16.92 ± 3.21 | - | 1.42 ± 0.30 | - | 35.34 ± 4.68 | - |
| AG | 18.94 ± 7.65 | 0.405 | 1.62 ± 0.72 | 0.385 | 36.84 ± 8.42 | 0.681 | ||
| GG | 14.30 ± 1.42 | 0.602 | 1.21 ± 0.12 | 0.690 | 31.20 ± 0.21 | 0.383 | ||
| rs1045642 | AA | 16.77 ± 2.54 | - | 1.40 ± 0.25 | - | 35.47 ± 5.13 | - | |
| AG | 16.44 ± 5.02 | 0.972 | 1.39 ± 0.48 | 0.998 | 35.37 ± 8.05 | 0.999 | ||
| GG | 25.33 ± 9.73 | 0.001 * | 2.20 ± 0.91 | 0.001 * | 38.00 ± 5.26 | 0.640 | ||
| rs2032582 | AA | 16.80 ± 3.05 | - | 1.41 ± 0.29 | - | 34.66 ± 4.84 | - | |
| AC | 18.55 ± 7.69 | 0.525 | 1.60 ± 0.74 | 0.421 | 36.53 ± 8.98 | 0.569 | ||
| CC | 18.13 ± 7.40 | 0.836 | 1.50 ± 0.59 | 0.909 | 36.66 ± 4.44 | 0.734 | ||
| rs4148738 | CC | 16.80 ± 3.05 | - | 1.41 ± 0.29 | - | 34.66 ± 4.84 | - | |
| CT | 18.55 ± 7.69 | 0.525 | 1.60 ± 0.74 | 0.421 | 36.53 ± 8.98 | 0.569 | ||
| TT | 18.13 ± 7.40 | 0.836 | 1.50 ± 0.59 | 0.909 | 36.66 ± 4.44 | 0.734 | ||
| CYP3A5 | rs776746 | *1/*1 | 14.50 ± 1.21 | - | 1.20 ± 1.02 | - | 32.00 ± 2.21 | - |
| *1/*3 | 18.33 ± 7.05 | 0.563 | 1.57 ± 0.67 | 0.555 | 33.81 ± 4.68 | 0.900 | ||
| *3/*3 | 17.64 ± 5.63 | 0.668 | 1.49 ± 0.51 | 0.684 | 37.24 ± 7.92 | 0.405 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ain, N.U.; Ali, N.; Ullah, A.; Ullah, S.; Ahmad, S. Bleeding Events Associated with Rivaroxaban Therapy in Naive Patients with Nonvalvular Atrial Fibrillation: A Longitudinal Study from a Genetic Perspective with INR Follow-Up. Medicina 2024, 60, 1712. https://doi.org/10.3390/medicina60101712
Ain NU, Ali N, Ullah A, Ullah S, Ahmad S. Bleeding Events Associated with Rivaroxaban Therapy in Naive Patients with Nonvalvular Atrial Fibrillation: A Longitudinal Study from a Genetic Perspective with INR Follow-Up. Medicina. 2024; 60(10):1712. https://doi.org/10.3390/medicina60101712
Chicago/Turabian StyleAin, Nur Ul, Niaz Ali, Abid Ullah, Shakir Ullah, and Shujaat Ahmad. 2024. "Bleeding Events Associated with Rivaroxaban Therapy in Naive Patients with Nonvalvular Atrial Fibrillation: A Longitudinal Study from a Genetic Perspective with INR Follow-Up" Medicina 60, no. 10: 1712. https://doi.org/10.3390/medicina60101712
APA StyleAin, N. U., Ali, N., Ullah, A., Ullah, S., & Ahmad, S. (2024). Bleeding Events Associated with Rivaroxaban Therapy in Naive Patients with Nonvalvular Atrial Fibrillation: A Longitudinal Study from a Genetic Perspective with INR Follow-Up. Medicina, 60(10), 1712. https://doi.org/10.3390/medicina60101712