
Minimally Invasive Trans-Axillary versus Full Sternotomy Mitral Valve Repair: A Propensity Score-Matched Analysis on Mid-Term Outcomes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
2.2. Population
2.3. Definitions
2.4. Echocardiographic Assessment
2.5. Surgical Techniques
2.5.1. Trans-Axillary Access
2.5.2. Full Sternotomy Access
2.6. Statistical Analysis
3. Results
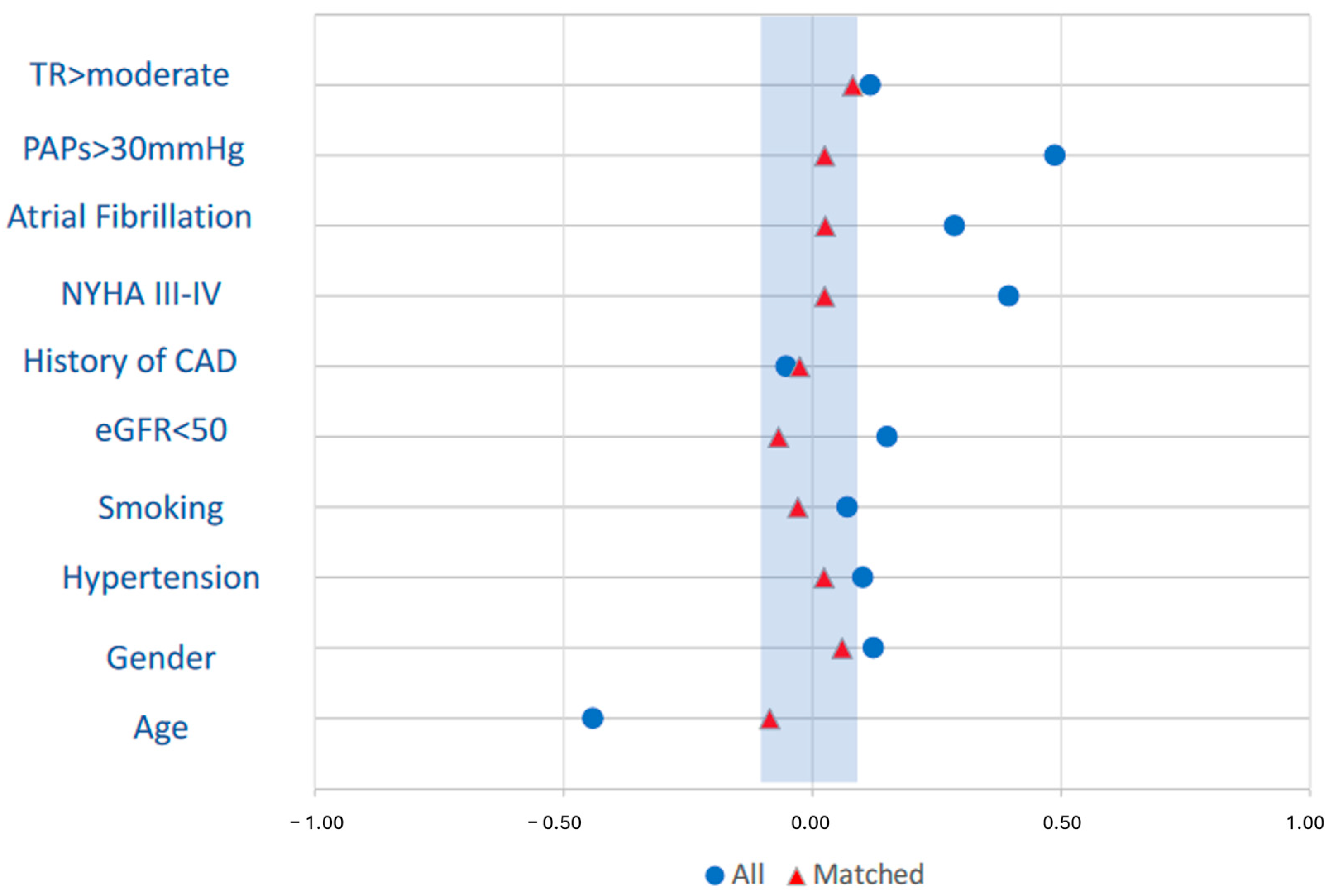
3.1. Baseline Characteristics
3.2. Operative Data in TAxA and FS Matched Cohorts
3.3. Postoperative Outcomes in TAxA and FS Matched Cohorts
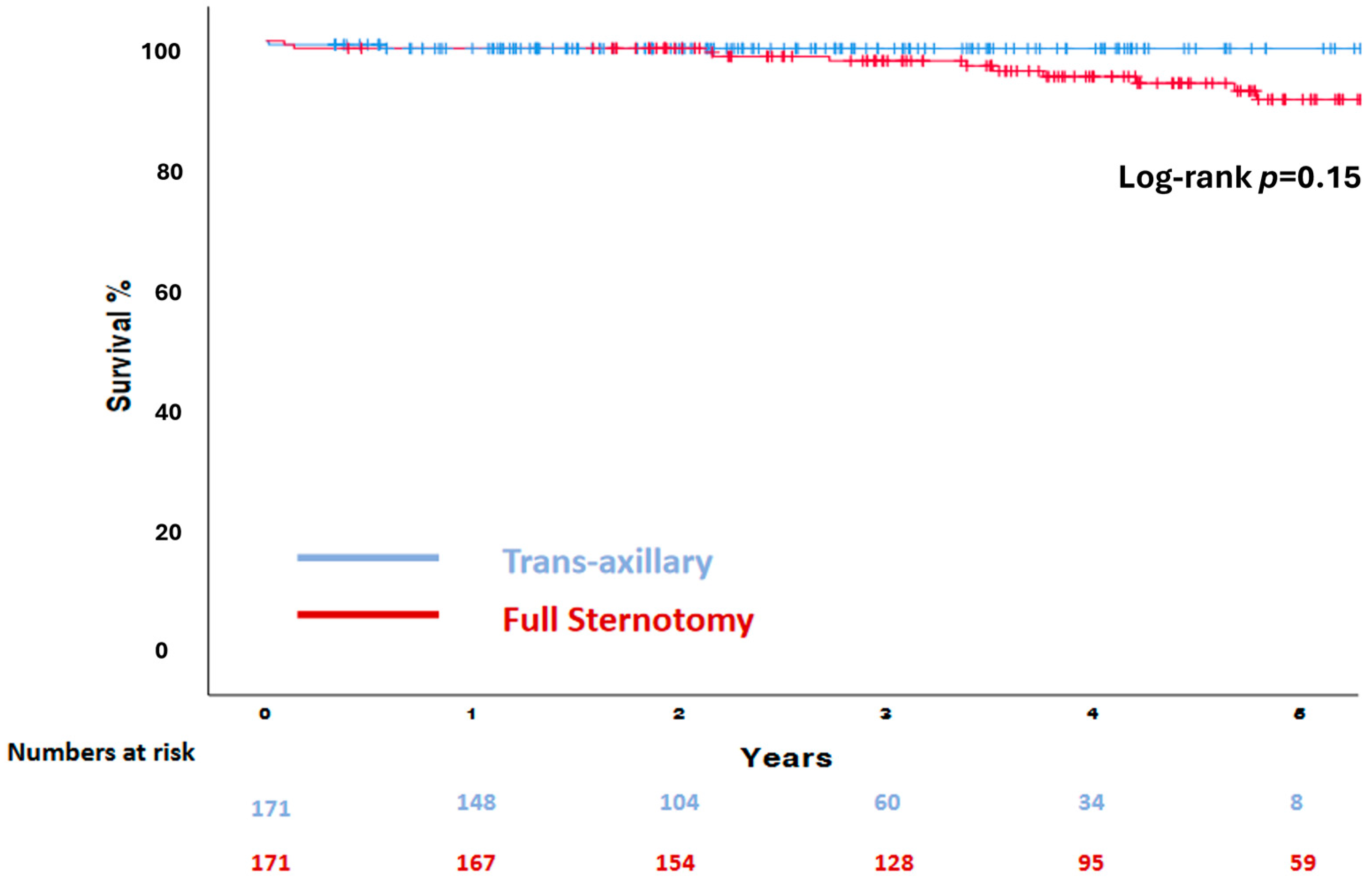
3.4. Mid-Term Outcomes in TAxA and FS Matched Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sá, M.P.B.O.; Eynde, J.V.D.; Cavalcanti, L.R.P.; Kadyraliev, B.; Enginoev, S.; Zhigalov, K.; Ruhparwar, A.; Weymann, A.; Dreyfus, G. Mitral valve repair with minimally invasive approaches vs. sternotomy: A meta-analysis of early and late results in randomized and matched observational studies. J. Card. Surg. 2020, 35, 2307–2323. [Google Scholar] [CrossRef]
- Eqbal, A.J.; Gupta, S.; Basha, A.; Qiu, Y.; Wu, N.; Rega, F.; Chu, F.V.; Belley-Cote, E.P.; Whitlock, R.P. Minimally invasive mitral valve surgery versus conventional sternotomy mitral valve surgery: A systematic review and meta-analysis of 119 studies. J. Card. Surg. 2022, 37, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh-Waghefi, A.; Arzt, S.; De Angelis, V.; Schiffarth, J.; Petrov, A.; Tomko, M.; Alexiou, K.; Matschke, K.; Kappert, U.; Wilbring, M. Safety and Efficacy of the Transaxillary Access for Minimally Invasive Mitral Valve Surgery—A Propensity Matched Competitive Analysis. Medicina 2022, 58, 1850. [Google Scholar] [CrossRef] [PubMed]
- Olsthoorn, J.R.; Heuts, S.; Houterman, S.; Maessen, J.G.; Sardari Nia, P.; Cardiothoracic Surgery Registration Committee of the Netherlands Heart Registration. Effect of minimally invasive mitral valve surgery compared to sternotomy on short- and long-term outcomes: A retrospective multicentre interventional cohort study based on Netherlands Heart Registration. Eur. J. Cardiothorac. Surg. 2022, 61, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Badhwar, V.; Vemulapalli, S.; Mack, M.A.; Gillinov, A.M.; Chikwe, J.; Dearani, J.A.; Grau-Sepulveda, M.V.; Habib, R.; Rankin, J.S.; Jacobs, J.P.; et al. Volume-Outcome Association of Mitral Valve Surgery in the United States. JAMA Cardiol. 2020, 5, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Wilbring, M.; Arzt, S.; Alexiou, K.; Matschke, K.; Kappert, U. Surgery without visible scars-double valve surgery using the right lateral access. Ann. Cardiothorac. Surg. 2020, 9, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Malvindi, P.G.; Wilbring, M.; De Angelis, V.; Bifulco, O.; Berretta, P.; Kappert, U.; Di Eusanio, M. Transaxillary approach enhances postoperative recovery after mitral valve surgery. Eur. J. Cardiothorac. Surg. 2023, 64, ezad207. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardiothorac. Surg. 2012, 41, 734–744. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Am. Coll. Cardiol. 2012, 60, 1438–1454. [Google Scholar] [CrossRef]
- Wilbring, M.; Alexiou, K.; Schmidt, T.; Petrov, A.; Taghizadeh-Waghefi, A.; Charitos, E.; Matschke, K.; Arzt, S.; Kappert, U. Safety and Efficacy of the Transaxillary Access for Minimally Invasive Aortic Valve Surgery. Medicina 2023, 59, 160. [Google Scholar] [CrossRef] [PubMed]
- Wilbring, M.; Matschke, K.E.; Alexiou, K.; Di Eusanio, M.; Kappert, U. Surgery without Scars: Right Lateral Access for Minimally Invasive Aortic Valve Replacement. Thorac. Cardiovasc. Surg. 2021, 69, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Malvindi, P.G.; Bifulco, O.; Berretta, P.; Silvano, R.; Alfonsi, J.; Cefarelli, M.; Zingaro, C.; Di Eusanio, M. del Nido and Histidine-Tryptophan-Ketoglutarate cardioplegia in minimally invasive mitral valve surgery: A propensity-Match study. Perfusion 2023, 7, 2676591231161920. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, A.; Meyer, R.; Lewandowski, J.; Markewitz, A.; Blaßfeld, D.; Böning, A. German Heart Surgery Report. 2021: The Annual Updated Registry of the German Society for Thoracic and Cardiovascular Surgery. Thorac. Cardiovasc. Surg. 2022, 70, 362–376. [Google Scholar] [CrossRef] [PubMed]
- Gammie, J.S.; Chikwe, J.; Badhwar, V.; Thibault, D.P.; Vemulapalli, S.; Thourani, V.H.; Gillinov, M.; Adams, D.H.; Rankin, J.S.; Ghoreishi, M.; et al. Isolated Mitral Valve Surgery: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis. Ann. Thorac. Surg. 2018, 106, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Downs, E.A.; Johnston, L.E.; LaPar, D.J.; Ghanta, R.K.; Kron, I.L.; Speir, A.M.; Fonner, C.E.; Kern, J.A.; Ailawadi, G. Minimally Invasive Mitral Valve Surgery Provides Excellent Outcomes Without Increased Cost: A Multi-Institutional Analysis. Ann. Thorac. Surg. 2016, 102, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Perin, G.; Shaw, M.; Toolan, C.; Palmer, K.; Al-Rawi, O.; Modi, P. Cost Analysis of Minimally Invasive Mitral Valve Surgery in the UK National Health Service. Ann. Thorac. Surg. 2021, 112, 124–131. [Google Scholar] [CrossRef]
- Kastengren, M.; Svenarud, P.; Källner, G.; Franco-Cereceda, A.; Liska, J.; Gran, I.; Dalén, M. Minimally invasive versus sternotomy mitral valve surgery when initiating a minimally invasive programme. Eur. J. Cardiothorac. Surg. 2020, 58, 1168–1174. [Google Scholar] [CrossRef]
- Van Praet, K.M.; Kofler, M.; Hirsch, S.; Akansel, S.; Hommel, M.; Sündermann, S.H.; Meyer, A.; Jacobs, S.; Falk, V.; Kempfert, J. Factors associated with an unsuccessful fast-track course following minimally invasive surgical mitral valve repair. Eur. J. Cardiothorac. Surg. 2022, 62, ezac451. [Google Scholar] [CrossRef]
- Bonaros, N.; Hoefer, D.; Oezpeker, C.; Gollmann-Tepeköylü, C.; Holfeld, J.; Dumfarth, J.; Kilo, J.; Ruttmann-Ulmer, E.; Hangler, H.; Grimm, M.; et al. Predictors of safety and success in minimally invasive surgery for degenerative mitral disease. Eur. J. Cardiothorac. Surg. 2022, 61, 637–644. [Google Scholar] [CrossRef]
- Berretta, P.; De Angelis, V.; Alfonsi, J.; Pierri, M.D.; Malvindi, P.G.; Zahedi, H.M.; Munch, C.; Di Eusanio, M. Enhanced recovery after minimally invasive heart valve surgery: Early and midterm outcomes. Int. J. Cardiol. 2023, 370, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, M.E.; Okoh, A.K.; Chao, J.C.; Soto, C.; Baxi, J.; Salgueiro, L.A.; Olds, A.; Ikegami, H.; Lemaire, A.; Russo, M.J.; et al. Early Discharge After Minimally Invasive Aortic and Mitral Valve Surgery. Ann. Thorac. Surg. 2022, 114, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Kloth, B.; Konertz, J.; Kubitz, J.; Schulte-Uentrop, L.; Ketels, G.; Reichenspurner, H.; Girdauskas, E. Economic impact of enhanced recovery after surgery protocol in minimally invasive cardiac surgery. BMC Health Serv. Res. 2021, 21, 254. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, J.; Gan, T.J.; Qin, G.; Wang, L.; Zhu, M.; Zhang, Z.; Pan, Y.; Ye, Z.; Zhang, F.; et al. Enhanced recovery after surgery pathway for patients undergoing cardiac surgery: A randomized clinical trial. Eur. J. Cardiothorac. Surg. 2018, 54, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Kubitz, J.C.; Schulte-Uentrop, L.; Zoellner, C.; Lemke, M.; Messner-Schmitt, A.; Kalbacher, D.; Sill, B.; Reichenspurner, H.; Koell, B.; Girdauskas, E. Establishment of an enhanced recovery after surgery protocol in minimally invasive heart valve surgery. PLoS ONE 2020, 15, e0231378. [Google Scholar] [CrossRef]
- Grossi, E.A.; Goldman, S.; Wolfe, J.A.; Mehall, J.; Smith, J.M.; Ailawadi, G.; Salemi, A.; Moore, M.; Ward, A.; Gunnarsson, C.; et al. Minithoracotomy for mitral valve repair improves inpatient and postdischarge economic savings. J. Thorac. Cardiovasc. Surg. 2014, 148, 2818–2822. [Google Scholar] [CrossRef]
- Glauber, M.; Miceli, A.; Canarutto, D.; Lio, A.; Murzi, M.; Gilmanov, D.; Ferrarini, M.; Farneti, P.A.; Quaini, E.L.; Solinas, M. Early and long-term outcomes of minimally invasive mitral valve surgery through right minithoracotomy: A 10-year experience in 1604 patients. J. Cardiothorac. Surg. 2015, 10, 181. [Google Scholar] [CrossRef]
- Goldstone, A.B.; Atluri, P.; Szeto, W.Y.; Trubelja, A.; Howard, J.L.; MacArthur, J.W.; Newcomb, C.; Donnelly, J.P.; Kobrin, D.M.; Sheridan, M.A.; et al. Minimally invasive approach provides at least equivalent results for surgical correction of mitral regurgitation: A propensity-matched comparison. J. Thorac. Cardiovasc. Surg. 2013, 145, 748–756. [Google Scholar] [CrossRef]
- Duchnowski, P. The Role of the N-Terminal of the Prohormone Brain Natriuretic Peptide in Predicting Postoperative Multiple Organ Dysfunction Syndrome. J. Clin. Med. 2022, 11, 7217. [Google Scholar] [CrossRef]
- Tatum, J.M.; Bowdish, M.E.; Mack, W.J.; Quinn, A.M.; Cohen, R.G.; Hackmann, A.E.; Barr, M.L.; Starnes, V.A. Outcomes after mitral valve repair: A single-center 16-year experience. J. Thorac. Cardiovasc. Surg. 2017, 154, 822–830. [Google Scholar] [CrossRef]
- Chan, V.; Elmistekawy, E.; Ruel, M.; Hynes, M.; Mesana, T.G. How Does Mitral Valve Repair Fail in Patients with Prolapse?—Insights From Longitudinal Echocardiographic Follow-Up. Ann. Thorac. Surg. 2016, 102, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; David, C.M.; Tsang, W.; Lafreniere-Roula, M.; Manlhiot, C. Long-Term Results of Mitral Valve Repair for Regurgitation Due to Leaflet Prolapse. J. Am. Coll. Cardiol. 2019, 74, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Armstrong, S.; McCrindle, B.W.; Manlhiot, C. Late outcomes of mitral valve repair for mitral regurgitation due to degenerative disease. Circulation 2013, 127, 1485–1492. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Unmatched | Matched | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Overall n = 528 | FS n = 220 | TAxA n = 308 | Absolute SMD | FS n = 171 | TAxA n = 171 | Absolute SMD |
| Mean ± SD n (%) | Mean ± SD n (%) | Mean ± SD n (%) | Mean ± SD n (%) | Mean ± SD n (%) | |||
| Age (years) | 64 ± 11 | 67.2 ± 11 | 62 ± 11 | 0.44 | 66 ± 10 | 65 ± 11 | 0.09 |
| Gender (M/F) | 194/334 | 88/132 | 106/202 | 0.13 | 105/66 | 110/61 | 0.06 |
| BMI (kg/m2) | 25.1 ± 4.1 | 25.5 ± 4.2 | 24.9 ± 3.9 | 0.15 | 25.4 ± 4.2 | 24.9 ± 4.3 | 0.12 |
| BSA (m2) | 1.85 ± 0.22 | 1.84 ± 0.21 | 1.86 ± 0.22 | 0.09 | 1.83 ± 0.21 | 1.84 ± 0.22 | 0.05 |
| Hypertension | 288 (54.5) | 127 (57.7) | 161 (52.3) | 0.10 | 97 (56.7) | 95 (55.6) | 0.02 |
| Diabetes Mellitus | 35 (6.6) | 14 (6.4) | 21 (6.8) | 0.02 | 11 (6.4) | 11 (6.4) | 0 |
| Dyslipidemia | 161 (30.5) | 77 (35) | 84 (27.3) | 0.16 | 55 (32.2) | 51 (29.8) | 0.05 |
| Smoking history | 99 (18.8) | 45 (20.5) | 54 (17.5) | 0.07 | 34 (19.9) | 36 (21.1) | 0.03 |
| CKD (eGFR < 50 mL/min/1.73 m2) | 68 (12.9) | 35 (15.9) | 33 (10.8) | 0.15 | 22 (12.9) | 26 (15.2) | 0.07 |
| Previous cerebral stroke | 9 (1.7) | 4 (1.8) | 5 (1.6) | 0.02 | 2 (1.2) | 2 (1.2) | 0 |
| Previous CAD | 30 (5.7) | 11 (5) | 19 (6.2) | 0.05 | 9 (5.3) | 10 (5.8) | 0.03 |
| Previous PCI | 18 (3.4) | 9 (4.1) | 9 (2.9) | 0.07 | 6 (3.5) | 5 (2.9) | 0.03 |
| NYHA class ≥ III | 207 (39.2) | 111 (50.5) | 96 (31.2) | 0.39 | 76 (44.4) | 74 (43.3) | 0.02 |
| Permanent pacemaker | 11(2.1) | 7 (3.2) | 4 (1.3) | 0.13 | 3 (1.8) | 3 (1.8) | 0 |
| History of AF | 148 (28) | 78 (35.5) | 70 (22.7) | 0.29 | 51 (29.8) | 49 (28.7) | 0.03 |
| Preoperative AF | 148 (28) | 79 (36) | 69 (22.4) | 0.3 | 50 (29.2) | 49 (28.7) | 0.01 |
| Hemoglobin (g/dL) | 13.6 ± 1.5 | 13.5 ± 1.6 | 13.7 ± 1.5 | 0.13 | 13.6 ± 1.5 | 13.5 ± 1.5 | 0.07 |
| Hematocrit (%) | 41.1 ± 4.4 | 40.9 ± 4.5 | 41.3 ± 4.4 | 0.09 | 41.3 ± 4.3 | 41 ± 4.2 | 0.07 |
| Preoperative ventricular arrhythmia | 10 (1.9) | 2 (0.9) | 8 (2.6) | 0.13 | 2 (1.2) | 4 (2.3) | 0.08 |
| LVEF (%) | 61.2 ± 7.9 | 60.9 ± 9.3 | 61.4 ± 6.7 | 0.06 | 61.2 ± 9 | 61 ± 8 | 0.02 |
| PAPs ≥ 30 mmHg | 230 (43.6) | 126 (57.3) | 104 (33.9) | 0.48 | 85 (49.7) | 83 (48.5) | 0.02 |
| TVR ≥ moderate | 129 (24.4) | 60 (27.3) | 69 (22.4) | 0.11 | 48 (28.1) | 42 (24.6) | 0.08 |
| EuroSCORE II (%) | 1.24 ± 1.1 | 1.4 ± 1.1 | 1.13 ± 0.9 | 0.12 | 1.29 ± 1.2 | 1.23 ± 0.9 | 0.08 |
| Variables | Matched | ||
|---|---|---|---|
| FS n = 171 | TAxA n = 171 | p | |
| Median [IQR] n (%) | Median [IQR] n (%) | ||
| Mitral repair for PMVL prolapse | 82 (48) | 103 (60.2) | 0.03 |
| Mitral repair for AMVL prolapse | 19 (11.1) | 10 (5.8) | 0.1 |
| Mitral repair for bileaflets disease | 35 (20.5) | 35 (20.5) | 1.0 |
| Neochordae | 55 (32.2) | 123 (71.9) | <0.001 |
| Leaflet(s) resection | 48 (28.1) | 16 (9.4) | <0.001 |
| Edge-to-edge | 43 (25.1) | 20 (11.7) | <0.001 |
| Concomitant TV repair | 33 (19.3) | 20 (11.7) | 0.08 |
| Concomitant AF surgery | 2 (1.2) | 4 (2.3) | 0.7 |
| Cardiopulmonary bypass time (minutes) | 80 (69–94) | 103 (87–123) | <0.001 |
| Cross-clamp time (minutes) | 64 (55–75) | 62 (51–78) | 0.5 |
| Repeated Cross-clamp | 4 (2.3) | 5 (2.9) | 1.0 |
| Intraoperative SAM | 2 (1.2) | 4 (2.3) | 0.7 |
| Intraoperative LCx occlusion | 0 | 1 (0.6) | 1.0 |
| Intraoperative aortic dissection | 0 | 1 (0.6) | 1.0 |
| Variables | Matched | ||
|---|---|---|---|
| FS n = 171 | TAxA n = 171 | p | |
| Median (IQR) n (%) | Median (IQR) n (%) | ||
| 30-day mortality | 1 (0.6) | 1 (0.6) | 1.0 |
| Cerebral stroke | 0 (0) | 1 (0.6) | 1.0 |
| Post-operative myocardial infarction | 3 (1.8) | 3 (1.8) | 1.0 |
| CVVHD | 1 (0.6) | 1 (0.6) | 1.0 |
| Bleeding re-thoracotomy | 6 (3.5) | 4 (2.4) | 0.6 |
| On table extubation | 14 (8.2) | 83 (48.5) | <0.001 |
| Mechanical ventilation time (hours) | 6 (4–10) 12 ± 39 | 1 (0–6) 5 ± 11 | <0.001 |
| Respiratory failure | 2 (1.2) | 3 (1.8) | 1.0 |
| ICU stay (hours) | 25 (24–48) 43 ± 40 | 24 (20–44) 36 ± 42 | <0.001 |
| New onset AF (preoperative SR) | 35 (28.9) | 31 (25.4) | 0.6 |
| Permanent pacemaker | 12 (7.1) | 8 (4.8) | 0.5 |
| Deep wound complication | 2 (1.2) | 0 (0) | 0.5 |
| Pre-discharge red blood cells transfusion (number of patients) | 34 (20.1) | 26 (15.8) | 0.3 |
| Hospital stay (days) | 7 (6–8) | 7 (6–8) | 0.7 |
| Discharge Home | 23 (13.5) | 86 (50.6) | <0.001 |
| LVEF (%) | 55 (50–60) | 55 (50–60) | 0.6 |
| Residual moderate MR | 1 (0.6) | 5 (2.9) | 0.1 |
| Redo for early failure | 5 (2.9) | 2 (1.2) | 0.4 |
| Patient | Previous MV Surgical Approach | Type of Repair Technique | Mode of Failure | Interval From Repair, y |
|---|---|---|---|---|
| 1 | FS | AMVL neochordae implantation | New onset of AMVL prolapse | 1.94 |
| 2 | FS | AMVL neochordae implantation | Recurrent AMVL prolapse | 2.49 |
| 3 | FS | PMVL neochordae implantation | Endocarditis: perforation and new onset of PMVL prolapse | 0.48 |
| 4 | FS | PMVL resection | New onset of flail leaflet due to chordal rapture | 3.96 |
| 5 | FS | Edge-to-edge | Recurrent AMVL and PMVL prolapse | 0.49 |
| 6 | FS | Edge-to-edge | New onset of AMVL prolapse | 4.49 |
| 7 | TAxA | PMVL neochordae implantation | Recurrent PMVL prolapse and chordal rapture | 3.36 |
| 8 | TAxA | PMVL neochordae implantation | New onset of PMVL chordal rapture | 1.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bifulco, O.; Malvindi, P.G.; Berretta, P.; Brugiatelli, L.; Cefarelli, M.; Alfonsi, J.; D’Alfonso, A.; Zingaro, C.; Di Eusanio, M. Minimally Invasive Trans-Axillary versus Full Sternotomy Mitral Valve Repair: A Propensity Score-Matched Analysis on Mid-Term Outcomes. Medicina 2024, 60, 29. https://doi.org/10.3390/medicina60010029
Bifulco O, Malvindi PG, Berretta P, Brugiatelli L, Cefarelli M, Alfonsi J, D’Alfonso A, Zingaro C, Di Eusanio M. Minimally Invasive Trans-Axillary versus Full Sternotomy Mitral Valve Repair: A Propensity Score-Matched Analysis on Mid-Term Outcomes. Medicina. 2024; 60(1):29. https://doi.org/10.3390/medicina60010029
Chicago/Turabian StyleBifulco, Olimpia, Pietro Giorgio Malvindi, Paolo Berretta, Leonardo Brugiatelli, Mariano Cefarelli, Jacopo Alfonsi, Alessandro D’Alfonso, Carlo Zingaro, and Marco Di Eusanio. 2024. "Minimally Invasive Trans-Axillary versus Full Sternotomy Mitral Valve Repair: A Propensity Score-Matched Analysis on Mid-Term Outcomes" Medicina 60, no. 1: 29. https://doi.org/10.3390/medicina60010029
APA StyleBifulco, O., Malvindi, P. G., Berretta, P., Brugiatelli, L., Cefarelli, M., Alfonsi, J., D’Alfonso, A., Zingaro, C., & Di Eusanio, M. (2024). Minimally Invasive Trans-Axillary versus Full Sternotomy Mitral Valve Repair: A Propensity Score-Matched Analysis on Mid-Term Outcomes. Medicina, 60(1), 29. https://doi.org/10.3390/medicina60010029