Abstract
Background and Objectives: Due to a lack of long-term clinical studies that would clarify whether the insertion of three mini-implants (MDIs) can be as successful treatment as the insertion of four MDIs for the retention of mandibular overdentures (ODs), this 5-year prospective cohort study was set up. Materials and Methods: Participants (n = 83) randomly received either four or three MDIs and a mandibular OD. Clinical examinations were performed at the baseline, as well as after one, three, and five years, respectively. A total of 73 participants (38 in the four-MDI and 35 in the three-MDI groups) partook in the study. The marginal bone level change, success and survival rates, and prosthodontic maintenance were assessed. Results: Repeated measures showed that the mean peri-implant bone loss increased progressively at a small amount over five years in both groups (four-MDI group = −0.36 ± 0.74; three-MDI group = −0.33 ± 0.27 mm; p < 0.05). However, an ANCOVA revealed no significant effects of the group (no significant difference between the three- and the four-MDI groups; F = 0.085; p = 0.771), gender (F = 0.023; p = 0.88), or covariate age (F = 1.95; p = 0.167) on the dependent variable: the 5-year MBL change. The success rate (together with successful survival) was 93.8% in the four-MDI group and 91.7% in the three-MDI group. The log-rank (Mantel–Cox) test revealed no significant differences between them (X2 = 0.373; p = 0.541). Conclusions: In patients with narrow ridges, the insertion of three MDIs in the mandible for overdenture retention can be equally as successful as the insertion of four MDIs.
1. Introduction
Mini dental implants (MDIs) with an active surface for osseointegration have been on the dental market for over 20 years as an alternative to standard-sized implants, because their reduced diameter enables their insertion into alveolar ridges with a reduced buccolingual width without the need for bone augmentation [1,2,3,4,5]. They are mostly made from the Ti-6Al-4V titanium alloy and have grade 5 mechanical properties. Although MDIs were once considered to be implants with a diameter less than 3.0 mm [6], the newest classification defines them as one-piece category 1 narrow implants with a diameter ranging from 1.8 to 2.5 mm [7]. The insertion of MDIs can often be performed without raising a flap, thus decreasing the duration of postsurgical recovery [8,9]. The insertion of four MDIs in the mandible for complete overdenture (OD) retention has been verified as an excellent clinical treatment option in subjects with narrow alveolar ridges, due to the very good survival and success rates of implants accompanied by increased patient satisfaction [3,4,5,10,11,12,13,14]. Even the insertion of four short MDIs (length ≤ 8 mm) and a mandibular OD was a successful treatment option in extreme mandibular atrophy [15,16]. The fixed-type MDIs have proved to be successful in the retention of crowns or short bridges in the mandibular incisor region [17]. Furthermore, the insertion of two or more MDIs for the retention of partial removable dentures was also confirmed as a successful treatment modality [18,19,20].
The question raised in this study was whether the retention of a mandibular OD with three MDIs can be as successful as with four MDIs. No prospective clinical studies have been conducted to test whether three MDIs can sufficiently retain and support mandibular ODs over a longer period. Therefore, the aim of this randomized, controlled prospective clinical trial was to assess the success of using only three MDIs for mandibular OD retention and comparing them with four MDIs. This study measured peri-implant marginal bone level (MBL) change and success and survival rates, comparing the three-MDI group with the control subjects, which were in fact, the cohort of patients with four MDIs (four-MDI group) over the period of five years.
Marginal bone loss refers to the gradual reduction in bone height around the implant site. While some degree of bone remodeling is natural, excessive marginal bone loss can impact the long-term success of dental implants. Various factors contribute to this phenomenon including surgical techniques, implant design, infection, loading protocol, extent of chewing forces, and other individual patient characteristics [21,22,23,24] The null hypothesis was that no significant differences in MBL changes and success and survival rates would be found between the three- and four-MDI groups.
2. Materials and Methods
2.1. Study Design
This prospective randomized clinical cohort study was performed between September 2015 and October 2022 at the School of Dental Medicine, University of Zagreb, Croatia, with the approval of the institution’s ethical committee (No. 05-PA-26-6/2015). The study protocol was in compliance with the Declaration of Helsinki. Before obtaining signed informed consent documentation, all procedures and possible complications, risks, and benefits were explained in detail to each participant.
2.2. Inclusion and Exclusion Criteria
An edentulous mandibular alveolar ridge width < 5.5 mm in the interforaminal region was the determining factor for inclusion in this study. Participants with wider ridges were excluded, as they could receive standard-sized implants. The available bone volume and length were measured on preoperative CBCT scans and digital panoramic radiographs. All participants were also required to have a eugnathic jaw relationship in their centric position. General exclusion criteria were not different from those accepted for any implant placement and were based on general health issues [25]. Local exclusion criteria were as follows: attached mucosa of a denture-bearing area thicker than 4.0 mm, flabby ridge, mandibular bone height less than 16 mm in the interforaminal region, participants having dysgnathia, and a history of radiotherapy in the mandible or neighboring regions.
Randomization in assigning edentulous participants into the 3- or 4-MDI groups was completed by assigning odd and even numbers to the participants. The first participant was assigned an odd number, the second an even number, and so on. Each participant assigned an odd number received 4 MDIs, while each participant assigned an even number received 3 MDIs in the mandible.
However, the surgeons who inserted the implants were not blinded to the procedure; neither were the prosthodontists who manufactured and loaded the overdentures. The costs of MDIs were covered by the research grant No. 1218/2014 (Croatian Science Foundation), and the costs of mandibular ODs were covered by the health insurance of each participant. All MDIs were inserted and all new ODs were manufactured during the first two years of the study (from October 2014 to December 2016).
2.3. Sample Size Calculation
The sample size calculation was made based on the primary outcome, i.e., peri-implant MBL change. Assuming that the mean MBL change may differ up to one mm between the groups with a standard deviation of one mm in each group and accounting for even 30% of possible dropouts during the observation period (five years), the calculation showed that 26 participants should be included in each group, with the type I probability error alpha set at p < 0.05 and the power at 80%. However, at the baseline of the study, a total of 83 participants were included: 42 in the 4-MDI group and 41 in the 3-MDI group.
2.4. Surgical Procedures
The inserted MDIs were ball-type (Dentium, South Korea) and 2.0 or 2.5 mm wide and 10–14 mm long, depending on the available bone volume assessed on the preoperative CBCT scans. The two experienced specialists in oral surgery, both with >10 years of experience, inserted the MDIs.
Participants in the 3-MDI group received 3 ball-type MDIs. Two posterior MDIs were inserted in the approximate region previously occupied by the distal surfaces of the canines. The third MDI was inserted at the midline, or as close as possible to the midline of the mandible (Figure 1a). Participants in the 4-MDI group received 4 ball-type MDIs in the sites of their previous first premolars (two posterior MDIs) and second incisors (two anterior MDIs) (Figure 1b).

Figure 1.
Participants with three (a) or four mini dental implants (MDIs) (b) inserted in the mandible for retention of mandibular overdentures.
Surgical procedures were performed by two experienced surgeons after consulting a specialist in prosthodontics. The surgical techniques performed were the flapless or the open flap techniques, depending on the morphology and volume of the available bone. The open-flap technique was utilized when a pointed narrow ridge had to be leveled, or the mucosa of a denture-bearing area needed alterations. In cases when the flapless method was used, the first step was to punch a small amount of oral mucosa into the preparation site to ensure a stable drill position. A physiodispenser (W&H Implantmed, GmbH, Salzburg, Austria) and an external drill cooled by a saline solution were used. The bone was prepared using the pilot and final drill (Dentium drilling set); however, the final drill diameter was always smaller than the MDI diameter (1.3–1.8 mm for 2.0 mm wide MDIs; 1.8–2.3 mm for 2.5 mm wide MDIs). The depth of preparation was determined depending on the bone quality. The preparations were made one, two, or three mm shorter than the implant length (longer preparations were performed in a denser bone). The only exception was when the MDI had to end in the dense lower mandibular cortex; in that case, the whole mini-implant length had to be prepared, as the tip of the MDI could not advance into the dense D1 bone. Antibiotics were administered one hour before surgery for prophylactic reasons (2 g amoxicillin with clavulanic acid or 600 mg clindamycin). Local anesthesia was administered prior to the surgery (Ubistesine forte 4% or Mepivastesin 3%, 3M). Each MDI was inserted into the preparation site and rotated clockwise, exerting a downward pressure (self-tapping insertion technique). The implants were transferred into the preparation hole with a plastic carrier from the original package and rotated until the plastic carrier broke; then, the thumb wrench was used and finally, the torque wrench. The whole roughened threaded MDI surface had to be inserted into the bone. The transmucosal part of the smooth MDI profile emerged from the attached mucosa into the oral cavity with the platform and the ball-type head for OD retention. The final MDI insertion torque values varied between 30 and 55 Ncm in both groups (3-MDI and 4-MDI groups, respectively).
All patients were given the following postsurgical instructions: no alcohol or smoking for two days, no hot beverages, ice packs for cooling, antiseptic mouth rinse (chlorhexidine gluconate 0.12%), and analgesics when necessary (nonsteroid anti-inflammatory drugs). Detailed instructions on how to maintain oral hygiene were also provided.
2.5. Prosthodontic Protocol
All new mandibular ODs were made by two trained specialists in prosthodontics and were delivered two to three months after the MDI insertions. The procedure was as follows: After obtaining alginate impressions, custom trays were made to obtain custom impressions for each participant. They were made using a thermoplastic border material and an additive low-viscosity silicone. The occlusal rims were made in the laboratory. The vertical jaw dimension of the lower jaw was recorded at the centric jaw relation for each participant and transferred into a semi-adjustable articulator. Semi-anatomical artificial teeth (lingualized occlusion scheme) were set up in the laboratory. After testing a trial denture to verify satisfactory esthetics and antagonistic contacts in the centric relation, new dentures were processed. All mandibular ODs were strengthened with a CoCr metal framework to prevent fractures. One to two days after the OD delivery and trial wearing (without MDI loading), metal housings with O-rings were mounted chairside using blockout shims and a self-curing acrylic resin (GC Reline, GC America Inc., Alsip, IL, USA). The occlusion was again checked and adjusted. During the adaptation period (fifteen days), the oral mucosa was inspected for soreness, and the denture was trimmed off if necessary.
2.6. Radiographic Evaluation
Preoperative CBCT scans and digital panoramic radiographs were obtained to determine mini-implant dimensions. Panoramic radiographs were obtained again after the MDI insertions to check their parallelism and positions. In some participants, panoramic radiographs were also obtained at the follow-up examinations (Figure 2a–e).
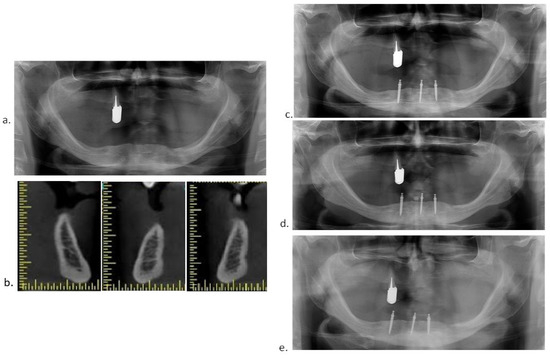
Figure 2.
(a) Preoperative panoramic radiograph; (b) preoperative CBCT; (c) panoramic radiograph after insertion of 3 MDIs; (d) panoramic radiograph obtained at the 3-year follow-up examination; (e) panoramic radiograph obtained at the 5-year follow-up examination.
At the MDI loading (mounting of metal housings with O-rings), digital retroalveolar radiographs were obtained to determine the marginal bone level (Minray Soredex Intraoral, Tuusula, Finland, 70 kV, 0.16 mAs; the long-cone paralleling technique). The digital retroalveolar radiographs were also obtained at the 1-, 3-, and 5-year clinical follow-up examinations. A film holder (X-ray holder, Super-Bite®, Kerr USA, Orange, CA, USA) with a customized silicone index for each patient was used for reproducibility (Figure 3a–c).
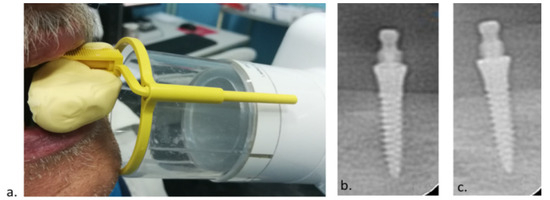
Figure 3.
(a) Silicone index and the long-cone paralleling technique; (b) postoperative radiogram; (c) 5-year follow-up radiogram.
The MBL change was measured at the mesial and distal sites of each MDI using ScanoraTM software 5.1. (Soredex, Tuusula, Finland) at a 10× magnification. The values were rounded to the nearest 0.1 mm. In cases where a part of the smooth MDI surface was submerged into the bone during insertion, bone loss, until it reached the roughened threaded surface, was considered as bone remodeling, not as bone loss. Radiographic evaluation was performed by two experienced specialists in prosthodontics who were not aware of the group classification.
2.7. Implant Success and Survival Rates
Implant success, survival, or failure rates were also assessed at the 1-, 3-, and 5-year follow-up examinations. The assessments were based on the Consensus Conference of the International Congress of Oral Implantology held in Pisa in 2007 [26]. Implants were categorized into successful, survival, or failure groups. Implant survival was categorized either as satisfactory or compromised survival. Successful implants were those where participants had no ongoing pain (or a history of pain), no dysesthesia or a foreign body sensation, no peri-implant infection, and no mobility when the peri-implant radiolucency was less than 2 mm and when the implant was suitable for a prosthodontic restoration. Satisfactory survival was described as a peri-implant marginal bone loss slightly > 2 mm either at the mesial or distal site, but not requiring any clinical management. Any implants requiring serious clinical treatment to reduce the risk of failure were listed in the compromised survival category. The MDIs were listed in the failure category when they required removal or had been lost already.
2.8. Prosthetic Complications and Maintenance
Mandibular OD base fractures, a need for relining, loosening of metal housings, or artificial teeth detachment were considered as complications, while the replacement of retentive elements (“O”-rings) was considered as maintenance.
2.9. Statistical Analysis
Statistical analysis was performed by using SPSS 20.0 software. A one-sample Kolmogorov–Smirnov test was used to test the normality of the MBL change distribution. An X2 test was used to test the significance of gender differences between the 3- and 4-MDI groups. An independent sample t-test was used to test the significance of the differences between the 3- and 4-MDI groups at each time point of observation (1, 3, and 5 years). The repeated-measures analysis was performed for the MBL changes between the three time points (1, 3, and 5 years, respectively) in both groups (the 3- and the 4-MDI groups). An ANCOVA was performed to test the significance of the differences for the variable MBL change, with fixed factors: the group (3 or 4 MDIs), gender (female or male), and age as covariates.
Kaplan–Meier curves were utilized for the survival analysis (MDI failures and compromised survivals were counted as one category, while successful implants and satisfactory survivals were counted together as another category). A comparison of the 4-MDI and 3-MDI groups was made using the Log-rank Mantel–Cox test.
3. Results
From the baseline of 83 participants in both groups, a total of 73 subjects completed the 5-year observation. The flow diagram of the participants is shown in Figure 4. The participants who responded to the 5-year recall clinical examination consisted of 38 subjects in the four-MDI group and 35 subjects in the three-MDI group. The four-MDI group comprised 24 females, and the three-MDI group comprised 17 females; no gender difference was found (X2 = 1.57, df = 1, p = 0.21). The groups were also not different according to the age of the participants (t = 0.52, df = 75; p = 0.61). The mean age ± standard deviation in the four-MDI group was 68.3 ± 9.97 years, while the mean age in the three-MDI group was 69.35 ± 7.71 years. Two participants were lost to follow-up in the four-MDI group after one year, and four participants were in the three-MDI group, so seventy-seven participants remained after one year. Furthermore, in the four-MDI group, one participant lost one MDI, and another participant lost two MDIs during the first year (two MDIs were 2.0 mm wide, one was 2.5 mm wide), while in the three-MDI group, one participant lost all three MDIs (two MDIs were 2.0 mm wide, one was 2.5 mm wide). At the 3-year examination, no more implants were lost in the four-MDI group (38 participants), while one implant fractured in the three-MDI group (2.0 mm wide) (35 participants remained). After 5 years, one participant lost all four implants in the four-MDI group (two were 2.0 mm wide; two were 2.5 mm wide) (they were so movable that they required removal and were categorized as failures), and one participant lost all three mini-implants in the three-MDI group (two of them fractured (2.0 mm wide) and the third one was movable (2.5 mm wide)). Finally, after the 5 years of mandibular OD-wearing, a total of 37 participants remained in the four-MDI group, and 34 remained in the three-MDI group.
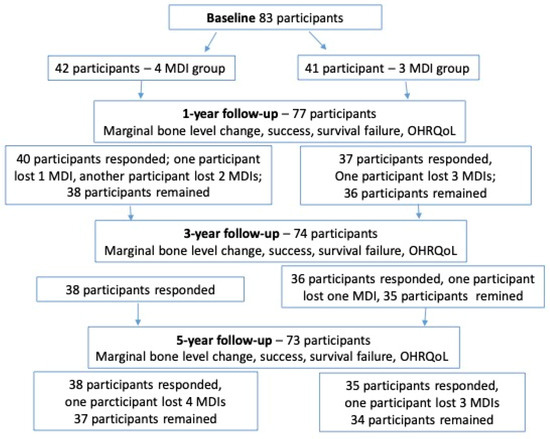
Figure 4.
Flow diagram of the study.
3.1. Marginal Bone Level (MBL) Change
There was no significant difference in the mean marginal bone loss between the two posterior and two anterior implants in the four-MDI group at the 5-year follow-up examination (t = 1.88; p = 0.07). Also, there was no significant difference in the mean marginal bone loss between the two posterior and midline implants (t = 1.34; p = 0.19) in the three-MDI group. Mean values of the MBL changes after the first, third, and fifth year of OD wearing, together with the significance of the differences between the three- and the four-MDI groups are presented in Table 1. Levene’s test for equality of variances showed equal variances, and the t-test for independent samples showed no significant difference in the MBL change between the three- and the four-MDI groups at any of the observation stages (p > 0.05).

Table 1.
Mean marginal bone level change (in mm) in the 3- and 4-MDI groups with the significance of the differences between the groups.
In the three-MDI group (Wilks’ lambda = 0.517; F(2.32) = 15.4; p < 0.001; η2 = 0.233) as well as in the four-MDI group (Wilks’ lambda = 0.807; F(2.35) = 4.3; p = 0.021; η2 = 0.483), the peri-implant MBL change decreased progressively (for a small amount) over the observation period.
The ANCOVA (dependent variable = marginal bone change at the 5-year follow-up) revealed that the model was not significant (F = 0.68, p = 0.61), the group (three- or four-MDI) had no significant effects (F = 0.085; p = 0.771), nor did the gender (F = 0.023, p = 0.88) or the covariate age (F = 1.95; p = 0.167) on the rate of the 5-year marginal bone loss. The mutual effect of belonging to either the three- or the four-MDI group, or a different gender group was also not significant (F = 0.077; p = 0.78). Although not statistically significant (p > 0.05), at the 5-year observation stage, the mean MBL decrease was slightly negatively correlated with the age in the four-MDI (r = −0.15, p = 0.34) as well as in the three-MDI groups (r = −0.24, p = 0.19).
3.2. Success, Survival, and Failure Rates
Success and satisfactory survival rates were analyzed together as one category, while failure and compromised survival were analyzed together as another category. The survival analysis comparing the four-MDI and the three-MDI groups throughout five years at the implant level is presented in Table 2 and Table 3. The survival analysis comparing the four-MDI and the three-MDI groups at the patient level throughout the same period of observation is presented in Table 4 and Table 5. The log-rank (Mantel–Cox) showed no significant difference between the three- and the four-MDI groups (p > 0.05). The Kaplan–Meier curves are presented in Figure 5 (MDI level) and Figure 6 (patient level).
Table 2.
Survival analysis comparing the 3-MDI and 4-MDI groups throughout five years of supporting mandibular overdentures (implant level).
Table 3.
Comparison of the 3-MDI and 4-MDI groups (implant level).
Table 4.
Survival analysis comparing the 3-MDI and 4-MDI groups throughout five years of supporting mandibular overdentures at the patient level.
Table 5.
Comparison of the 3-MDI and 4-MDI groups (patient level).
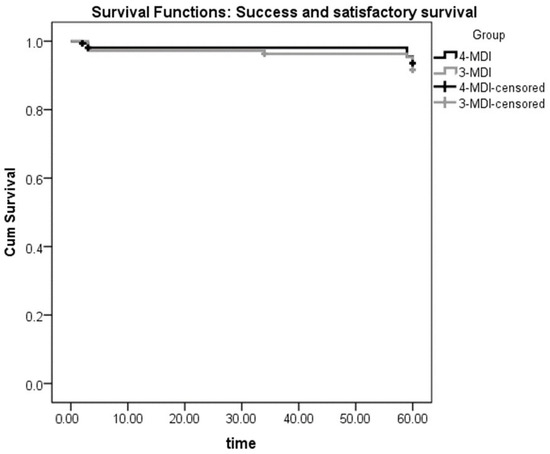
Figure 5.
Implant-level Kaplan–Meier curves for success and satisfactory survival of 4 or 3 mini dental implants (MDIs) supporting mandibular overdentures over 5 years of follow-ups.
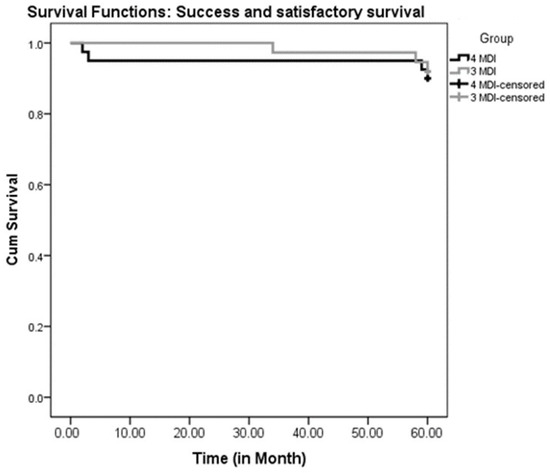
Figure 6.
Patient-level Kaplan–Meier curves for success and satisfactory survival of 4 or 3 mini dental implants (MDIs) supporting mandibular overdentures over 5 years of follow-ups.
3.3. Prosthetic Complications and Maintenance
No OD fracture was registered either in the three- or the four-MDI group. The complications and the need for maintenance registered with mandibular ODs are presented in Table 6. At the 1-year observation stage, two ODs required relining: one in the three- and another in the four-MDI group, respectively. The same occurred after three years, while at the 5-year examination stage, three ODs required relining in the four-MDI group, and four ODs required relining in the three-MDI group. Seven “O”-rings were lost or needed to be changed in the three-MDI group and another three “O”-rings in the four-MDI group during the first year. During the second and third years, an additional 34 “O”-rings had to be changed in the three-MDI group and 24 in the four-MDI group. Up to the fifth year of observation, an additional 30 “O”-rings had to be changed in the three-MDI group and 24 in the four-MDI group, respectively. At the 5-year observation stage, all “O”-rings were changed in both groups.
Table 6.
Overdenture complications and maintenance registered through the 5-year observation period.
4. Discussion
Due to a lack of clinical evidence on whether the insertion of only three MDIs can be as equally successful of a treatment as the insertion of four MDIs for the retention of mandibular ODs over a longer period of time, this cohort study was set up. The 5-year results revealed small rates of peri-implant bone loss in both the three- and four-MDI groups, with no significant difference between them. The 5-year success and survival rates were also not different between the groups and were acceptable in both groups. Thus, the hypothesis was accepted.
The short time of clinical evidence (one year) showed that either two or four MDIs led to better oral health-related quality of life (OHRQoL), compared with two standard implants [5]. However, the costs were the least for the two mini-implant OD options [27]. One study (limited sample size) pointed towards increased patient satisfaction during the 7-year clinical observation with two MDIs [28]. However, the rate of MBL change was not presented. Another study (11 patients) showed a 1-year satisfactory masticatory efficiency with two MDIs [29]. On the other hand, Jofre et al. [30] showed a high amount of marginal bone loss in two unsplinted MDIs retaining a mandibular OD during the 15 months of clinical follow-up (1.40 +/− 1.02 mm), compared with the two MDIs splinted with a prefabricated bar (0.84 +/− 0.66 mm). Therefore, they recommended the splitting of two mini-implants for better clinical success or the insertion of four MDIs as single units. Also, a lack of data exists about the aftercare costs and survival rates of two mini-implants for mandibular OD retention [31]. The study of Misfud et al. [32] described an MBL change in two MDIs, but they used category 2 narrow implants (diameter = 2.9 mm, with locator system for the retention of ODs). As opposed to the insertion of only two MDIs as the less expensive treatment modality, Mangano et al. [33] reported that the insertion of either three or four MDIs in 62 patients was satisfactory in the 4-year prospective study (overall cumulative survival rate was 96.9%, and there were only 6% biologic complications). However, Magnano et al. [33] did not compare the outcomes of the three and the four MDIs.
Our previous clinical experience showed that patients with four MDIs, even when they lost one implant, continued to wear dentures retained on only three MDIs. Therefore, as the less expensive treatment than the four MDIs, we chose to follow-up prospectively the option of inserting only three MDIs. The insertion of four MDIs is the standard of care for mandibular OD retention in edentulous subjects with narrow ridges [2,3,4,5,6,10,11,12,13,14,15,16,27,33,34,35,36,37,38,39,40,41,42]. The present 5-year cohort study compared clinical outcomes of the insertion of three MDIs with the outcomes of four MDIs for mandibular OD retention. No statistically significant differences were found between the groups over the intermediate-term clinical observation period of five years in mean peri-implant MBL change (−0.36 mm in the three-MDI group vs. −0.33 mm in the four-MDI group) and the success and satisfactory survival rates (93.8% in the four-MDI, and 91.7% in the three-MDI group, respectively). One study based on the review of the literature (1–7 years) reported that the mean survival rate of patients with four MDIs was 92.32% [34], while another similar study reported that the mean survival rate of four MDIs (category 1 narrow implants) was 94.7 ± 5% [35]. One study reported survival rates of 95.63% over the mean period of 28 months [10]. The overall survival rate (for four MDIs) after 5 years of treatment was 90.7% in the study of Hussein and Alruthea [36]. Enkling et al. [11] reported the 100% survival rate of four MDIs and ascribed it to the open-flap surgical approach at the baseline. The present study revealed similar (sometimes even better) survival rates to those listed in the literature [10,34,35,36] both for the 3- and the 4-MDI option. The study of Mundt et al. [37] reported 0.5 mm of peri-implant bone loss over the mean observation time of 2.2 ± 1.0 years with mandibular ODs loading four MDIs. Zygogiannis et al. [34] reported a one-year mean MBL change of −0.42 ± 0.56 mm in the mandibles with four MDIs. Another study [36] reported a mean peri-implant vertical bone loss of 1.61 ± 0.371 after 5 years. Our 5-year study revealed less bone loss in both groups (−0.33 ± 0.27 mm in the three-MDI group and −0.36 ± 0.74 in the four-MDI group). The lower amount of peri-implant vertical bone loss recorded in the present study can be attributed to the fact that bone loss in the submerged MDIs around the polished surface was considered as bone remodeling [15,17,19]. Only a decrease in the bone below the roughened, threaded surface was considered as bone loss. In this study, the MDIs were inserted during the open-flap surgery whenever it was necessary (the morphology of the available bone required bone leveling), which is in compliance with the study of Enkling et al., who reported a 100% success rate over five years when MDIs were inserted through open-flap surgery [11,39].
It is known that younger patients develop higher occlusal forces and chew more vigorously, while implants have less proprioception than periodontal ligaments [39]. That may account for a slightly negative (although not significant) correlation between the age and MBL decrease after five years, as found in this study [40]. When we consider maintenance in the three- and four-MDI groups, no fractures of denture bases were registered during the 5-year observation due to reinforcement by a metal Co–Cr framework in all delivered dentures. Most of the “O”-ring replacements had to be completed due to calculus formation (lost elasticity) or wear; only a few “O”-rings fell out of metal housings in both groups. Although the manufacturer recommends changing the “O”-rings once a year, only a few “O”-rings had to be changed after one year, similar to other studies [38,39,41]. A slightly larger number of “O”-rings had to be replaced in the three-MDI group during the 5-year period. All “O”-rings were only changed after five years, which is consistent with another study on MDIs utilized for partial removable denture retention [19].
The keratinized mucosa thickness can influence the amount of marginal bone loss. It was reported that the peri-implant bone loss is lesser in thick than in thin mucosa biotypes [42,43,44]. However, we did not measure the height of the peri-implant mucosa, which is one of the study limitations.
The limitations of the present study are the 2-dimensional assessment of peri-implant bone level, variations in the amount of chewing force between the participants, variations in the diameter (2.0–2.5) and length (10, 12 or 14 mm) of the MDIs, variations in the thickness of the keratinized mucosa around implants, as well as differences in the thickness of the mucosa at the overdenture’s bearing area, which could account to different levels of stress and strain around implants. The strength of this study is the long period of clinical follow-up (5 years) and the controlled cohort prospective study design.
Overall, the findings of the present study point out that a treatment with only three MDIs is a clinically acceptable treatment option: the same as treatment with four MDIs [2,3,4,5,6,10,11,12,13,14,15,16,33,34,35,36,37,38,39,40,41,45].
5. Conclusions
Within the limitation of this 5-year prospective cohort study, the results revealed no significant differences between the three- and four-MDI groups in terms of the peri-implant marginal bone loss and success and survival rates. Therefore, treatment with three MDIs retaining the mandibular OD (as a less expensive option) is equally as successful as treatment with four MDIs.
Author Contributions
A.C. conceptualized and designed the work, acquired and analyzed data, interpreted data, drafted, and finally approved the manuscript; I.K. drafted the manuscript and performed the literature and data acquisition, data analysis, and clinical follow-up; N.P. performed the literature and data acquisition, drafted the manuscript, and interpreted data; M.N.A. was involved in conceptualization, data interpretation and analysis, and final manuscript approval; J.T. drafted the manuscript, acquired data, and partook in clinical follow-up; L.J. was involved in statistical analysis and data interpretation; S.P.-K. was involved in conceptualization, clinical follow-up, and final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Croatian Science Foundation, grant number 1218, which covered expenses for mini-implants.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the School of Dental Medicine, University of Zagreb (protocol code 05-PA-26-6/2015, approved date June 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Acknowledgments
We thank the Croatian Science Foundation for funding the expense of mini-implants in project 1218.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bulard, R.A.; Vance, J.B. Multi-clinic evaluation using mini-dental implants for long-term denture stabilization: A preliminary biometric evaluation. Compend. Contin. Educ. Dent. 2005, 26, 892–897. [Google Scholar] [PubMed]
- Griffitts, T.M.; Collins, C.P.; Collins, P.C. Mini dental implants: An adjunct for retention, stability, and comfort for the edentulous patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, e81–e84. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, D. Rationale for Mini Dental Implant Treatment. J. Oral Implantol. 2021, 47, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Topić, J.; Poljak-Guberina, R.; Persic-Kirsic, S.; Kovacic, I.; Petricevic, N.; Popovac, A.; Čelebić, A. Adaptation to New Dentures and 5 Years of Clinical Use: A Comparison between Complete Denture and Mini-implant Mandibular Overdenture Patients based on Oral Health-Related Quality of Life (OHRQoL) and Orofacial Esthetics. Acta Stomatol. Croat. 2022, 56, 132–142. [Google Scholar] [CrossRef] [PubMed]
- de Souza, R.F.; Ribeiro, A.B.; Della Vecchia, M.P.; Costa, L.; Cunha, T.R.; Reis, A.C.; Albuquerque, R.F., Jr. Mini vs. Standard Implants for Mandibular Overdentures: A Randomized Trial. J. Dent. Res. 2015, 94, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Shin, S.W.; Lee, J.Y. Mini-implant mandibular overdentures under a two-step immediate loading protocol: A 4–6-year retrospective study. Gerodontology 2023, 40, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI Consensus Report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kovačić, I.; Peršić, S.; Disha, V.; Rener-Sitar, K.; Čelebić, A. Short-Term Postoperative Pain and Swelling Associated with Mini and Standard-Size Implants in the Same Patients. Int. J. Prosthodont. 2018, 31, 117–119. [Google Scholar] [CrossRef]
- Kahn, A.; Masri, D.; Shalev, T.; Meir, H.; Sebaoun, A.; Chaushu, L. Patients’ Perception of Recovery after Dental Implant Placement. Medicina 2021, 57, 1111. [Google Scholar] [CrossRef]
- Jawad, S.; Clarke, P.T. Survival of Mini Dental Implants Used to Retain Mandibular Complete Overdentures: Systematic Review. Int. J. Oral Maxillofac. Implants 2019, 34, 343–356. [Google Scholar] [CrossRef]
- Enkling, N.; Haueter, M.; Worni, A.; Müller, F.; Leles, C.R.; Schimmel, M. A prospective cohort study on survival and success of one-piece mini-implants with associated changes in oral function: Five-year outcomes. Clin. Oral Implants Res. 2019, 30, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Čelebić, A.; Peršić, S.; Kovačić, I.; Buković, D.; Lešić, N.; Rener-Sitar, K. Comparison of Three Prosthodontic Treatment Modalities for Patients with Periodontally Compromised Anterior Mandibular Teeth: A 2-year follow-up study. Acta Stomatol. Croat. 2019, 53, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Peršić, S.; Ćelić, R.; Vojvodić, D.; Petričević, N.; Kranjčić, J.; Zlatarić, D.K.; Čelebić, A. Oral Health-Related Quality of Life in Different Types of Mandibular Implant Overdentures in Function Longer Than 3 Years. Int. J. Prosthodont. 2016, 29, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.A.; Codello, D.J.; Del Rio Silva, L.; Dini, C.; Barão, V.A.R.; Mesquita, M.F. Factors and clinical outcomes for standard and mini-implants retaining mandibular overdentures: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 130, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Kovačić, I.; Peršić, S.; Kranjčić, J.; Celebic, A. A cohort study on short mini-implants for mandibular overdentures compared to those of standard length. Clin. Oral Implants Res. 2020, 31, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Kovacic, I.; Persic, S.; Kranjcic, J.; Lesic, N.; Celebic, A. Rehabilitation of an Extremely Resorbed Edentulous Mandible by Short and Narrow Dental Implants. Case Rep. Dent. 2018, 2018, 7597851. [Google Scholar] [CrossRef] [PubMed]
- Ćorić, A.; Kovačić, I.; Kiršić, S.P.; Čelebić, A. Are Mini Dental Implants Suitable for Support of Crowns or Small Bridges in the Mandibular Incisor Region? A 5-year Longitudinal Study. J. Oral Maxillofac. Surg. 2022, 80, 1811–1826. [Google Scholar] [CrossRef] [PubMed]
- Mundt, T.; Heinemann, F.; Müller, J.; Schwahn, C.; Al Jaghsi, A. Survival and stability of strategic mini-implants with immediate or delayed loading under removable partial dentures: A 3-year randomized controlled clinical trial. Clin. Oral. Investig. 2023, 27, 1767–1779. [Google Scholar] [CrossRef]
- Celebic, A.; Kovacic, I.; Petricevic, N.; Puljic, D.; Popovac, A.; Kirsic, S.P. Mini-Implants Retaining Removable Partial Dentures in Subjects without Posterior Teeth: A 5-Year Prospective Study Comparing the Maxilla and the Mandible. Medicina 2023, 59, 237. [Google Scholar] [CrossRef]
- Mundt, T.; Schwahn, C.; Heinemann, F.; Schimmel, M.; Lucas, C.; Al Jaghsi, A. Stabilizing Removable Partial Dentures by Immediate or Delayed Loading of Mini-implants: Chewing Efficiency in a Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implants 2020, 35, 178–186. [Google Scholar] [CrossRef]
- Güven, S.Ş.; Cabbar, F.; Güler, N. Local and systemic factors associated with marginal bone loss around dental implants: A retrospective clinical study. Quintessence Int. 2020, 52, 128–141. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Koller, C.D.; Pereira-Cenci, T.; Boscato, N. Parameters Associated with Marginal Bone Loss around Implant after Prosthetic Loading. Braz. Dent J. 2016, 27, 292–297. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Galindo-Moreno, P.; Catena, A.; Lopez-Chaichio, L.; Borges, T.; O’Valle, F.; Torrecillas-Martínez, L.; Padial-Molina, M. The Influence of History of Severe Periodontitis on Estimated Long-Term Marginal Bone Loss around Implants Restored with Fixed Segmented Full-Arch Rehabilitation. J. Clin. Med. 2023, 12, 6665. [Google Scholar] [CrossRef] [PubMed]
- Kullar, A.S.; Miller, C.S. Are There Contraindications for Placing Dental Implants? Dent. Clin. N. Am. 2019, 63, 345–362. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Della Vecchia, M.P.; Leles, C.R.; Cunha, T.R.; Ribeiro, A.B.; Sorgini, D.B.; Muglia, V.A.; Reis, A.C.; Albuquerque, R.F., Jr.; de Souza, R.F. Mini-Implants for Mandibular Overdentures: Cost-Effectiveness Analysis alongside a Randomized Trial. JDR Clin. Trans. Res. 2018, 3, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Catalán, A.; Martínez, A.; Marchesani, F.; González, U. Mandibular Overdentures Retained by Two Mini-Implants: A Seven-Year Retention and Satisfaction Study. J. Prosthodont. 2016, 25, 364–370. [Google Scholar] [CrossRef]
- Bellia, E.; Boggione, L.; Terzini, M.; Manzella, C.; Menicucci, G. Immediate Loading of Mandibular Overdentures Retained by Two Mini-Implants: A Case Series Preliminary Report. Int. J. Prosthodont. 2018, 31, 558–564. [Google Scholar] [CrossRef]
- Jofré, J.; Hamada, T.; Nishimura, M.; Klattenhoff, C. The effect of maximum bite force on marginal bone loss of mini-implants supporting a mandibular overdenture: A randomized controlled trial. Clin. Oral Implants Res. 2010, 21, 243–249. [Google Scholar] [CrossRef]
- Roy, S.; Maji, S.; Paul, R.; Bhattacharyya, J.; Goel, P. A comparison of cost and cost-effectiveness analysis of two- implant-retained overdentures versus other removable prosthodontic treatment options for edentulous mandible: A systematic review. J. Indian Prosthodont. Soc. 2020, 20, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Mifsud, D.P.; Cortes, A.R.G.; Zarb, M.J.; Attard, N.J. Maintenance and risk factors for fractures of overdentures using immediately loaded conventional diameter or mini implants with Locator abutments: A cohort study. Clin. Implant Dent. Relat. Res. 2020, 22, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Caprioglio, A.; Levrini, L.; Farronato, D.; Zecca, P.A.; Mangano, C. Immediate loading of mandibular overdentures supported by one-piece, direct metal laser sintering mini-implants: A short-term prospective clinical study. J. Periodontol. 2015, 86, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.; Verri, F.R.; Batista, V.E.; Júnior, J.F.; Mello, C.C.; Pellizzer, E.P. Complete overdentures retained by mini implants: A systematic review. J. Dent. 2017, 57, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 21–40. [Google Scholar] [CrossRef]
- Hussein, M.O.; Alruthea, M.S. Marginal Bone Level Changes and Oral Health Impact Profile (14) Score of Smokers Treated by Mandibular Mini Implant Overdentures: A 5-Year Follow-up Study. Eur. J. Dent. 2020, 14, 590–597. [Google Scholar] [CrossRef]
- Mundt, T.; Schwahn, C.; Biffar, R.; Heinemann, F. Changes in Bone Levels Around Mini-Implants in Edentulous Arches. Int. J. Oral Maxillofac. Implants 2015, 30, 1149–1155. [Google Scholar] [CrossRef][Green Version]
- Zygogiannis, K.; Aartman, I.H.; Parsa, A.; Tahmaseb, A.; Wismeijer, D. Implant Mandibular Overdentures Retained by Immediately Loaded Implants: A 1-Year Randomized Trial Comparing the Clinical and Radiographic Outcomes Between Mini Dental Implants and Standard-Sized Implants. Int. J. Oral Maxillofac. Implants 2017, 32, 1377–1388. [Google Scholar] [CrossRef]
- Enkling, N.; Moazzin, R.; Geers, G.; Kokoschka, S.; Abou-Ayash, S.; Schimmel, M. Clinical Outcomes and Bone-Level Alterations around One-Piece Mini Dental Implants Retaining Mandibular Overdentures: 5-Year Follow-up of a Prospective Cohort Study. Clin. Oral Implants Res. 2020, 31, 549–556. [Google Scholar] [CrossRef]
- González-Gil, D.; Dib-Zaitum, I.; Flores-Fraile, J.; López-Marcos, J. Importance of Osseoperception and Tactile Sensibility during Masticatory Function in Different Prosthetic Rehabilitations: A Review. Medicina 2022, 58, 92. [Google Scholar] [CrossRef]
- Elsyad, M.A. Patient Satisfaction and Prosthetic Aspects with Mini-Implants Retained Mandibular Overdentures. A 5-Year Prospective Study. Clin. Oral Implants Res. 2016, 27, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Alkimavicius, J.; Linkevicius, R.; Gineviciute, E.; Linkeviciene, L. Effect of Ti-Base Abutment Gingival Height on Maintenance of Crestal Bone in Thick Biotype Patients: A Randomized Clinical Trial with 1-Year Follow-up. Int. J. Oral Maxillofac. Implants 2022, 37, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Avila-Ortiz, G.; Urban, I.A.; Giannobile, W.V.; Wang, H.L. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: A systematic review and network meta-analysis. J. Periodontol. 2021, 92, 21–44. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.M.; Choi, B.H.; Li, J.; Xuan, F. The effect of thick mucosa on peri-implant tissues: An experimental study in dogs. J. Periodontol. 2008, 79, 2151–2155. [Google Scholar] [CrossRef]
- Peršić, S.; Čelebić, A. Influence of Different Prosthodontic Rehabilitation Options on Oral Health-Related Quality of Life, Orofacial Esthetics and Chewing Function Based on Patient-Reported Outcomes. Qual. Life Res. 2015, 24, 919–926. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).