
Hypermagnesemia in Clinical Practice

 , and
, and 
Abstract
1. Introduction
2. Mg Transporters in the Human Body
3. Mg Absorption in the Human Body
4. Mg Storage and Renal Regulation
5. Determinants of Renal Mg Absorption
5.1. Hormonal
5.2. Non-Hormonal
6. The Role of Mg in Cellular Processes
7. Epidemiology of Hypermagnesemia
8. Assessment of Mg Status
9. Causes of Hypermagnesemia
9.1. Reduced Renal Excretion
9.2. Increased Intake of Mg
9.3. Mg Leak to the Extracellular Fluid
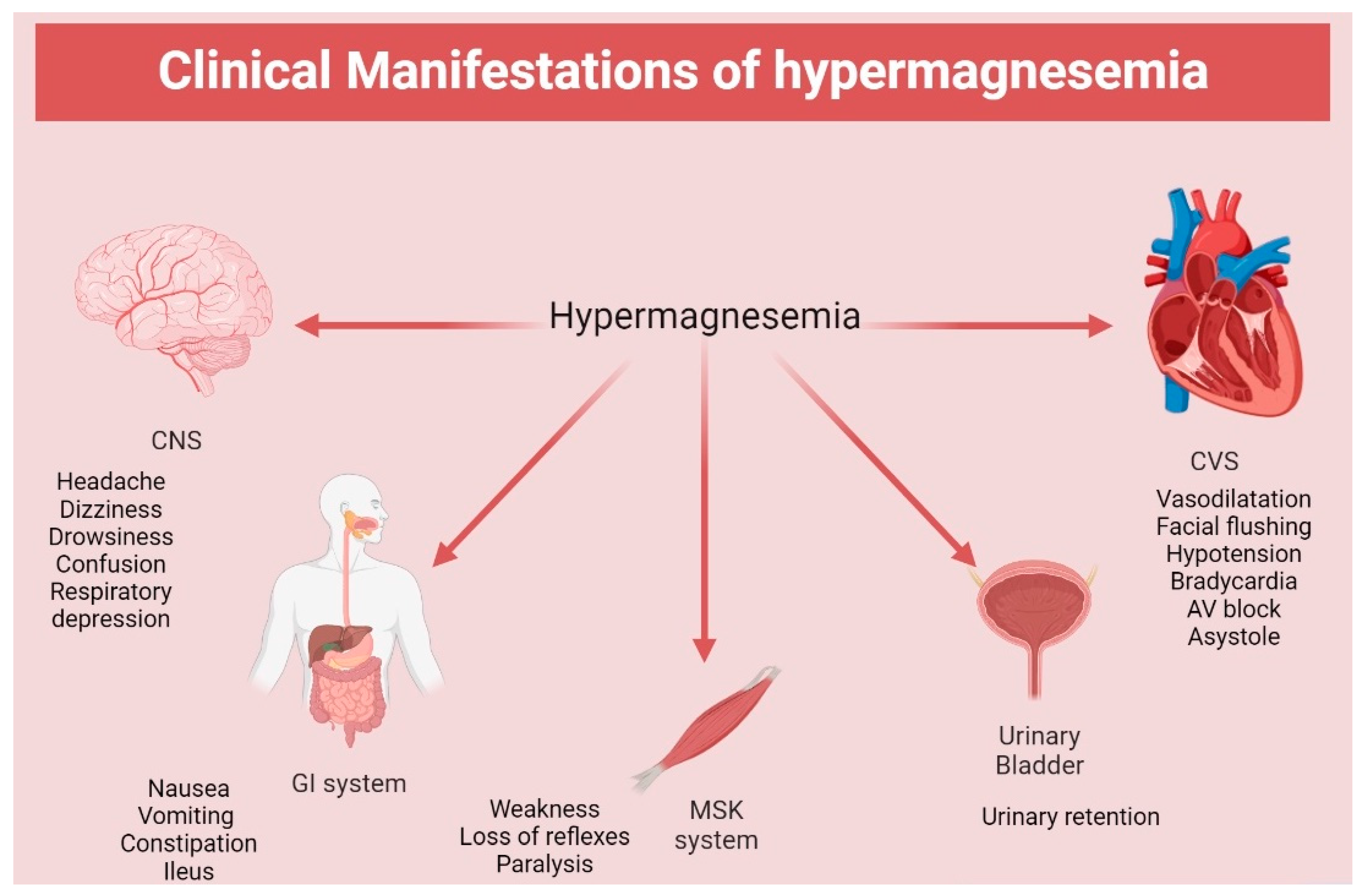
10. Clinical Manifestations of Hypermagnesemia
11. Clinical Assessment of Hypermagnesemia
12. Management of Hypermagnesemia
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al Alawi, A.M.; Majoni, S.W.; Falhammar, H. Magnesium and Human Health: Perspectives and Research Directions. Int. J. Endocrinol. 2018, 2018, 9041694. [Google Scholar] [CrossRef]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef]
- Al Alawi, A.M.; Berhane, T.; Majoni, S.W.; Falhammar, H. Characteristics and health outcomes of patients hospitalised with hypomagnesaemia: A retrospective study from a single centre in the Northern Territory of Australia. Intern. Med. J. 2022, 52, 1544–1553. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Qian, Q. Dysmagnesemia in Hospitalized Patients: Prevalence and Prognostic Importance. Mayo Clin. Proc. 2015, 90, 1001–1010. [Google Scholar] [CrossRef]
- Sontia, B.; Touyz, R.M. Role of magnesium in hypertension. Arch. Biochem. Biophys. 2007, 458, 33–39. [Google Scholar] [CrossRef]
- Monteilh-Zoller, M.K.; Hermosura, M.; Nadler, M.J.; Scharenberg, A.M.; Penner, R.; Fleig, A. TRPM7 provides an ion channel mechanism for cellular entry of trace metal ions. J. Gen. Physiol. 2003, 121, 49–60. [Google Scholar] [CrossRef]
- Schlingmann, K.P.; Gudermann, T. A critical role of TRPM channel-kinase for human magnesium transport. J. Physiol. 2005, 566, 301–308. [Google Scholar] [CrossRef]
- Romani, A.M.P. Cellular magnesium homeostasis. Arch. Biochem. Biophys. 2011, 512, 1–23. [Google Scholar] [CrossRef]
- Rondon, L.J.; Groenestege, W.M.; Rayssiguier, Y.; Mazur, A. Relationship between low magnesium status and TRPM6 expression in the kidney and large intestine. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, R2001–R2007. [Google Scholar] [CrossRef]
- Gold, M.E.; Buga, G.M.; Wood, K.S.; Byrns, R.E.; Chaudhuri, G.; Ignarro, L.J. Antagonistic modulatory roles of magnesium and calcium on release of endothelium-derived relaxing factor and smooth muscle tone. Circ. Res. 1990, 66, 355–366. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium-An Update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef]
- Fordtran, J.S.; Rector, F.C., Jr.; Carter, N.W. The mechanisms of sodium absorption in the human small intestine. J. Clin. Investig. 1968, 47, 884–900. [Google Scholar] [CrossRef]
- Pham, P.C.; Pham, P.; Pham, S.V.; Pham, P.T.; Pham, P.M.; Pham, P.T. Hypomagnesemia: A clinical perspective. Int. J. Nephrol. Renovasc Dis. 2014, 7, 219–230. [Google Scholar] [CrossRef]
- Schlingmann, K.P.; Weber, S.; Peters, M.; Niemann Nejsum, L.; Vitzthum, H.; Klingel, K.; Kratz, M.; Haddad, E.; Ristoff, E.; Dinour, D.; et al. Hypomagnesemia with secondary hypocalcemia is caused by mutations in TRPM6, a new member of the TRPM gene family. Nat. Genet. 2002, 31, 166–170. [Google Scholar] [CrossRef]
- de Baaij, J.H.; Hoenderop, J.; Bindels, R.J. Regulation of magnesium balance: Lessons learned from human genetic disease. Clin. Kidney J. 2012, 5, i15–i24. [Google Scholar] [CrossRef]
- Maruani, G.; Hertig, A.; Paillard, M.; Houillier, P. Normocalcemic primary hyperparathyroidism: Evidence for a generalized target-tissue resistance to parathyroid hormone. J. Clin. Endocrinol. Metab. 2003, 88, 4641–4648. [Google Scholar] [CrossRef]
- Di Stefano, A.; Roinel, N.; de Rouffignac, C.; Wittner, M. Transepithelial Ca2+ and Mg2+ transport in the cortical thick ascending limb of Henle’s loop of the mouse is a voltage-dependent process. Ren. Physiol. Biochem. 1993, 16, 157–166. [Google Scholar]
- Petrelli, F.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Barni, S. Risk of anti-EGFR monoclonal antibody-related hypomagnesemia: Systematic review and pooled analysis of randomized studies. Expert. Opin. Drug. Saf. 2012, 11, S9–S19. [Google Scholar] [CrossRef]
- Meij, I.C.; Koenderink, J.B.; van Bokhoven, H.; Assink, K.F.; Groenestege, W.T.; de Pont, J.J.; Bindels, R.J.; Monnens, L.A.; van den Heuvel, L.P.; Knoers, N.V. Dominant isolated renal magnesium loss is caused by misrouting of the Na(+),K(+)-ATPase gamma-subunit. Nat. Genet. 2000, 26, 265–266. [Google Scholar] [CrossRef]
- Wong, N.L.; Quamme, G.; Dirks, J.H. Effects of acid-base disturbances on renal handling of magnesium in the dog. Clin. Sci. 1986, 70, 277–278. [Google Scholar] [CrossRef]
- de Baaij, J.H.; Hoenderop, J.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Ahmed, F.; Mohammed, A. Magnesium: The Forgotten Electrolyte-A Review on Hypomagnesemia. Med. Sci. 2019, 7, 56. [Google Scholar] [CrossRef] [PubMed]
- Workinger, J.L.; Doyle, R.P.; Bortz, J. Challenges in the Diagnosis of Magnesium Status. Nutrients 2018, 10, 1202. [Google Scholar] [CrossRef] [PubMed]
- Huey, C.G.; Chan, K.M.; Wong, E.T.; Nelson, J.M.; Durand, M. Los Angeles County-University of Southern California Medical Center clinical pathology case conference: Extreme hypermagnesemia in a neonate. Clin. Chem. 1995, 41, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Oren, S.; Rapoport, J.; Zlotnik, M.; Brami, J.L.; Heimer, D.; Chaimovitz, C. Extreme hypermagnesemia due to ingestion of Dead Sea water. Nephron 1987, 47, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Syedmoradi, L.; Ghasemi, A.; Zahediasl, S.; Azizi, F. Prevalence of hypo- and hypermagnesemia in an Iranian urban population. Ann. Hum. Biol. 2011, 38, 150–155. [Google Scholar] [CrossRef]
- Smith, J.M.; Lowe, R.F.; Fullerton, J.; Currie, S.M.; Harris, L.; Felker-Kantor, E. An integrative review of the side effects related to the use of magnesium sulfate for pre-eclampsia and eclampsia management. BMC Pregnancy Childbirth 2013, 13, 34. [Google Scholar] [CrossRef]
- Altman, D.; Carroli, G.; Duley, L.; Farrell, B.; Moodley, J.; Neilson, J.; Smith, D. Magpie Trial Collaboration Group. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: A randomised placebo-controlled trial. Lancet 2002, 359, 1877–1890. [Google Scholar]
- Whang, R.; Ryder, K.W. Frequency of hypomagnesemia and hypermagnesemia. Requested vs routine. JAMA 1990, 263, 3063–3064. [Google Scholar] [CrossRef]
- Felsenfeld, A.J.; Levine, B.S.; Rodriguez, M. Pathophysiology of Calcium, Phosphorus, and Magnesium Dysregulation in Chronic Kidney Disease. Semin. Dial. 2015, 28, 564–577. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Bathini, T.; Hansrivijit, P.; Vaitla, P.; Medaura, J.; Vallabhajosyula, S.; Chewcharat, A.; Mao, M.A.; Erickson, S.B. Impact of admission serum magnesium levels on long-term mortality in hospitalized patients. Hosp. Pract. 2020, 48, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Haider, D.G.; Lindner, G.; Ahmad, S.S.; Sauter, T.; Wolzt, M.; Leichtle, A.B.; Fiedler, G.M.; Exadaktylos, A.K.; Fuhrmann, V. Hypermagnesemia is a strong independent risk factor for mortality in critically ill patients: Results from a cross-sectional study. Eur. J. Intern. Med. 2015, 26, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Xu, Q.; Li, C.; Liu, J.; Shi, R. High-Normal Serum Magnesium and Hypermagnesemia Are Associated With Increased 30-Day In-Hospital Mortality: A Retrospective Cohort Study. Front. Cardiovasc. Med. 2021, 8, 625133. [Google Scholar] [CrossRef]
- Li, J.; Imtiaz, M.S.; Beard, N.A.; Dulhunty, A.F.; Thorne, R.; vanHelden, D.F.; Laver, D.R. ß-Adrenergic stimulation increases RyR2 activity via intracellular Ca2+ and Mg2+ regulation. PLoS ONE 2013, 8, e58334. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Del Canale, S.; Coffrini, E.; Melej, R.; Vitali, P.; Guariglia, A.; Borghetti, A. Muscle and serum magnesium in pulmonary intensive care unit patients. Crit. Care Med. 1988, 16, 751–760. [Google Scholar] [CrossRef]
- Sharma, R.; Heidari, A.; Johnson, R.H.; Advani, S.; Petersen, G. Serum magnesium levels in hospitalized patients with SARS-CoV-2. J. Investig. Med. 2022, 70, 409–414. [Google Scholar] [CrossRef]
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5, i3–i14. [Google Scholar] [CrossRef]
- Bouillon-Minois, J.B.; Khaled, L.; Vitte, F.; Miraillet, L.; Eschalier, R.; Jabaudon, M.; Sapin, V.; Derault, L.; Kahouadji, S.; Brailova, M.; et al. Ionized Magnesium: Interpretation and Interest in Atrial Fibrillation. Nutrients 2023, 15, 236. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Park, T.J. Magnesium metabolism. Electrolyte Blood Press. 2008, 6, 86–95. [Google Scholar] [CrossRef]
- Nishikawa, M.; Shimada, N.; Kanzaki, M.; Ikegami, T.; Fukuoka, T.; Fukushima, M.; Asano, K. The characteristics of patients with hypermagnesemia who underwent emergency hemodialysis. Acute Med. Surg. 2018, 5, 222–229. [Google Scholar] [CrossRef]
- Cascella, M.; Vaqar, S. Hypermagnesemia; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Riccardi, D.; Brown, E.M. Physiology and pathophysiology of the calcium-sensing receptor in the kidney. Am. J. Physiol. Renal Physiol. 2010, 298, F485–F499. [Google Scholar] [CrossRef]
- Iglesias, P.; Bajo, M.A.; Selgas, R.; Díez, J.J. Thyroid dysfunction and kidney disease: An update. Rev. Endocr. Metab. Disord. 2017, 18, 131–144. [Google Scholar] [CrossRef]
- Woodward, A.; McCann, S.; Al-Jubouri, M. The relationship between estimated glomerular filtration rate and thyroid function: An observational study. Ann. Clin. Biochem. 2008, 45, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Brent, G.A. The molecular basis of thyroid hormone action. N. Engl. J. Med. 1994, 331, 847–853. [Google Scholar] [PubMed]
- Wu, Y.; Koenig, R.J. Gene regulation by thyroid hormone. Trends Endocrinol. Metab. 2000, 11, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Yen, P.M. Physiological and molecular basis of thyroid hormone action. Physiol. Rev. 2001, 81, 1097–1142. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Shimada, H.; Yoshita, K.; Tsubata, Y.; Ikarashi, K.; Morioka, T.; Saito, N.; Sakai, S.; Narita, I. Severe hypermagnesemia induced by magnesium oxide ingestion: A case series. CEN Case Rep. 2019, 8, 31–37. [Google Scholar] [CrossRef]
- Shoaib Khan, M.; Zahid, S.; Ishaq, M. Fatal Hypermagnesemia: An acute ingestion of Epsom Salt in a patient with normal renal function. Caspian J. Intern. Med. 2018, 9, 413–415. [Google Scholar] [PubMed]
- Mori, H.; Suzuki, H.; Hirai, Y.; Okuzawa, A.; Kayashima, A.; Kubosawa, Y.; Kinoshita, S.; Fujimoto, A.; Nakazato, Y.; Nishizawa, T.; et al. Clinical features of hypermagnesemia in patients with functional constipation taking daily magnesium oxide. J. Clin. Biochem. Nutr. 2019, 65, 76–81. [Google Scholar] [CrossRef]
- Cope, C.L. Base changes in the alkalosis produced by the treatment of gastric ulcer with alkalies. Clin. Sci. 1936, 2, 287–300. [Google Scholar]
- Medarov, B.I. Milk-alkali syndrome. Mayo Clin. Proc. 2009, 84, 261–267. [Google Scholar] [CrossRef]
- Chakurkar, V.V.; Gade, P.S.; Godbole, A.V.; Wadia, F.F.; Lobo, V.A. Inadvertently high dialysate magnesium causing weakness and nausea in hemodialysis patients. Hemodial. Int. 2019, 23, E106–E110. [Google Scholar] [CrossRef]
- Thompson, I.M.; Mora, R.V. Hypermagnesemia associated with hemiacidrin irrigation. J. Urol. 1984, 132, 741–742. [Google Scholar] [CrossRef]
- Al Alawi, A.M.; Al Badi, A.; Al Huraizi, A.; Falhammar, H. Magnesium: The recent research and developments. Adv. Food Nutr. Res. 2021, 96, 193–218. [Google Scholar] [CrossRef]
- Razzaque, M.S. Magnesium: Are We Consuming Enough? Nutrients 2018, 10, 1863. [Google Scholar] [CrossRef]
- Wibe, E.; Kvaløy, S.; Nome, O.; Abrahamsen, A.F.; Bjørgo, S. Tumor lysis syndrome. A life-threatening complication during cytostatic treatment of chemosensitive types of cancer. Tidsskr. Nor. Laegeforen 1991, 111, 2435–2437. [Google Scholar] [PubMed]
- Swaminathan, R. Magnesium metabolism and its disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar] [PubMed]
- Saris, N.E.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium. An update on physiological, clinical and analytical aspects. Clin. Chim. Acta. 2000, 294, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Caballero, B.; Allen, L.; Prentice, A. Encyclopedia of Human Nutrition; Elsevier Science: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Chang, W.T.; Radin, B.; McCurdy, M.T. Calcium, magnesium, and phosphate abnormalities in the emergency department. Emerg. Med. Clin. N. Am. 2014, 32, 349–366. [Google Scholar] [CrossRef]
- Onishi, S.; Yoshino, S. Cathartic-induced fatal hypermagnesemia in the elderly. Intern. Med. 2006, 45, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Kazama, I. High-magnesium exposure to bullfrog heart causes ST segment elevation. J. Vet. Med. Sci. 2021, 83, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Jhang, W.K.; Lee, Y.J.; Kim, Y.A.; Park, S.J.; Park, Y.S. Severe hypermagnesemia presenting with abnormal electrocardiographic findings similar to those of hyperkalemia in a child undergoing peritoneal dialysis. Korean J. Pediatr. 2013, 56, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.S.L.Y.A. Hypermagnesemia: Causes, Symptoms, and Treatment; UpToDate: Waltham, MA, USA, 2023. [Google Scholar]
- DynaMed. Hypermagnesemia-Approach to the Patient. Available online: https://www.dynamed.com/approach-to/hypermagnesemia-approach-to-the-patient#GUID-90892592-B90F-48C6-ACF1-D53C3D5648E4 (accessed on 1 May 2023).
- Moe, S.M. Disorders involving calcium, phosphorus, and magnesium. Prim. Care 2008, 35, 215–237. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Category | Sub-Category | Causes | Mechanisms |
|---|---|---|---|
| Reduced Renal Excretion | Kidney Disease | Acute kidney injury Chronic kidney disease | Reduced ability of the kidneys to excrete Mg |
| Endocrinological Conditions | Hyperparathyroidism Adrenal insufficiency Hypothyroidism | Abnormalities in calcium metabolism or renal blood flow/filtration rate | |
| Certain Drugs | Lithium, angiotensin-converting enzyme inhibitors, non-steroidal anti-inflammatory drugs | Alteration of renal endothelial vessels and angiotensin system | |
| Increased Intake of Mg | Bowel Conditions | Elderly patients with bowel conditions | Enhanced absorption or reduced gut motility |
| Medications | Anticholinergics, laxatives, and medications containing Mg | Increased intake or absorption of Mg | |
| Other Causes | Milk alkali syndrome, increased dialysate Mg, post-urethral irrigation with hemiacidrin, excessive infusion of Mg sulfate | Various mechanisms | |
| Mg Leak to Extracellular Fluid | Hemolysis | Tumor lysis syndrome | Movement of Mg from intracellular to extracellular space |
| Metabolic Acidosis | Diabetic ketoacidosis | Movement of Mg from intracellular to extracellular space | |
| Other Causes | Chronic low-grade metabolic acidosis | Various mechanisms |
| Symptoms | Magnesium Concentration |
|---|---|
| Non-specific symptoms, wide variability | <2.2 mmol/L (<5.35 mg/dL) |
| Nausea, dizziness, weakness, confusion | 2.2–3.5 mmol/L (5.35–8.5 mg/dL) |
| Worsening confusion, drowsiness, depressed reflexes, headache, flushing, urinary complications, gastrointestinal symptoms, blurred vision | >3.5 mmol/L (>8.5 mg/dL) |
| Mild decrease in blood pressure | >3.5 mmol/L (>8.5 mg/dL) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aal-Hamad, A.H.; Al-Alawi, A.M.; Kashoub, M.S.; Falhammar, H. Hypermagnesemia in Clinical Practice. Medicina 2023, 59, 1190. https://doi.org/10.3390/medicina59071190
Aal-Hamad AH, Al-Alawi AM, Kashoub MS, Falhammar H. Hypermagnesemia in Clinical Practice. Medicina. 2023; 59(7):1190. https://doi.org/10.3390/medicina59071190
Chicago/Turabian StyleAal-Hamad, Aya Hasan, Abdullah M. Al-Alawi, Masoud Salim Kashoub, and Henrik Falhammar. 2023. "Hypermagnesemia in Clinical Practice" Medicina 59, no. 7: 1190. https://doi.org/10.3390/medicina59071190
APA StyleAal-Hamad, A. H., Al-Alawi, A. M., Kashoub, M. S., & Falhammar, H. (2023). Hypermagnesemia in Clinical Practice. Medicina, 59(7), 1190. https://doi.org/10.3390/medicina59071190