
Predictive Values of Hematological Parameters for Determining Imminent Brain Death: A Retrospective Study


Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arsava, E.M.; Demirkaya, Ş.; Dora, B.; Giray, S.; Gökçe, M.; Güler, A. Turkish Neurological Society—Diagnostic Guidelines for Brain Death. Turk. J. Neurol. 2014, 20, 101–104. [Google Scholar]
- De Groot, Y.J.; Jansen, N.E.; Bakker, J.; Kuiper, M.A.; Aerdts, S.; Maas, A.I.; Wijdicks, E.F.; van Leiden, H.A.; Hoitsma, A.J.; Kremer, B.H.; et al. Imminent brain death: Point of departure for potential heart-beating organ donor recognition. Intensive Care Med. 2010, 36, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.L.; Bayraktutan, U. Oxidative stress and its role in the pathogenesis of ischaemic stroke. Int. J. Stroke 2009, 4, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Caceres, J.A.; Goldstein, J.N. Intracranial hemorrhage. Emerg. Med. Clin. N. Am. 2012, 30, 771–794. [Google Scholar] [CrossRef] [PubMed]
- Keep, R.F.; Hua, Y.; Xi, G. Intracerebral haemorrhage: Mechanisms of injury and therapeutic targets. Lancet Neurol. 2012, 11, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Ye, F.; Garton, H.J.L.; Hua, Y.; Keep, R.F.; Xi, G. The Role of Thrombin in Brain Injury After Hemorrhagic and Ischemic Stroke. Transl. Stroke Res. 2021, 12, 496–511. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Huang, K.; Ji, Z.; Wang, S.; Bai, M.; Pan, S.; Lin, Z.; Wu, Y. High neutrophil-to-lymphocyte ratio is associated with poor clinical outcome in patients with critically ill stroke. Minerva Anestesiol. 2020, 86, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, N.M.; Peker, T.T.; Soyal, Ö.B.; Akçaboy, Z.N.; Akçaboy, E.Y.; Titiz, A.P.; Çiftçi, A.; Göğüş, N. Red Cell Distribution Width in Diagnosis of Brain Death. Transplant. Proc. 2019, 51, 2189–2191. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Zheng, J.; Guo, R.; Ma, L.; You, C.; Li, H. Prognostic impact of leukocytosis in intracerebral hemorrhage: A PRISMA-compliant systematic review and meta-analysis. Medicine 2019, 98, e16281. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, M.H.; Kim, C.H.; Kim, J.M.; Cheong, J.H.; Ryu, J.I. Increased Short-Term Mortality in Patients with Spontaneous Intracerebral Hemorrhage and its Association with Admission Glucose Levels and Leukocytosis. World Neurosurg. 2017, 98, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, H.; Feng, G.L. Neutrophil-to-Lymphocyte Ratio Predicts in-Hospital Mortality in Intracerebral Hemorrhage. J. Stroke Cerebrovasc. Dis. 2022, 31, 106611. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Arima, H.; Heeley, E.; Delcourt, C.; Krause, M.; Peng, B.; Yang, J.; Wu, G.; Chen, X.; Chalmers, J.; et al. White blood cell count and clinical outcomes after intracerebral hemorrhage: The INTERACT2 trial. J. Neurol Sci. 2016, 361, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Uzunkaya, F.; İdil Soylu, A. Predictors of full functional recovery in endovascularly treated patients with aneurysmal subarachnoid hemorrhage. Turk. J. Med. Sci. 2021, 51, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.J.; Dowlati, E.; Triano, M.; Kalegha, E.; Krishnan, R.; Kasturiarachi, B.M.; Gachechiladze, L.; Pandhi, A.; Themistocleous, M.; Katsanos, A.H.; et al. Admission Neutrophil to Lymphocyte Ratio for Predicting Outcome in Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2021, 30, 105936. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Hu, X.; Wang, J.; Ma, J.; Li, H.; You, C. Admission neutrophil count and neutrophil to lymphocyte ratio predict 90-day outcome in intracerebral hemorrhage. Biomark. Med. 2017, 11, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, L.; Jia, L.; Li, T.; Di, Y.; Wang, P.; Deng, H.; Fan, H.; Li, Y.; Cheng, X.; et al. Neutrophil Counts as Promising Marker for Predicting In-Hospital Mortality in Aneurysmal Subarachnoid Hemorrhage. Stroke 2021, 52, 3266–3275. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, S.; Cagnetti, C.; Provinciali, L.; Silvestrini, M. Neutrophil-to-lymphocyte ratio and neurological deterioration following acute cerebral hemorrhage. Oncotarget 2017, 8, 57489–57494. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Jun Yi, H.; Hoon Lee, D.; Hoon Sung, J. Clinical significance of platelet to neutrophil ratio and platelet to lymphocyte ratio in patients with aneurysmal subarachnoid hemorrhage. J. Clin. Neurosci. 2021, 92, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Shen, Y. Platelet-to-Lymphocyte Ratio as a New Predictive Index of Neurological Outcomes in Patients with Acute Intracranial Hemorrhage: A Retrospective Study. Med. Sci. Monit. 2018, 27, 4413–4420. [Google Scholar] [CrossRef] [PubMed]
- Ozgen, E.; Guzel, M.; Akpinar, C.K.; Yucel, M.; Demir, M.T.; Baydin, A. The relationship between neutrophil/lymphocyte, monocyte/ /lymphocyte, platelet/lymphocyte ratios and clinical outcomes after ninety days in patients who were diagnosed as having acute ischemic stroke in the emergency room and underwent a mechanical thro. Bratisl. Lek. Listy 2020, 121, 634–639. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | Brain Death | n | Hemorrhage | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 128 | 63.50 (19:94) | 153 | 66 (18:91) | 0.271 a |
| Gender | |||||
| Female | 128 | 61 (47.70%) | 153 | 75 (49%) | 0.820 b |
| Male | 67 (52.30%) | 78 (51%) | |||
| Comorbidities | |||||
| HT | 128 | 87 (68%) | 153 | 96 (62.70%) | 0.054 b |
| DM | 128 | 28 (21.90%) | 153 | 28 (18.30%) | 0.455 b |
| COPD | 128 | 9 (7%) | 153 | 4 (2.60%) | 0.079 b |
| CRF | 128 | 2 (1.60%) | 153 | 0 | 0.207 c |
| CAD | 128 | 15 (11.70%) | 153 | 14 (9.20%) | 0.481 b |
| AF | 128 | 3 (2.30%) | 153 | 0 | 0.093 c |
| n | Brain Death | n | Hemorrhage | p-Value | |
|---|---|---|---|---|---|
| WBC | 128 | 14,240 (3400:79,800) | 153 | 11,650 (2580:31,310) | 0.002 a |
| PLT | 128 | 216,500 (16,000:480,000) | 153 | 223,000 (9000:500,000) | 0.393 a |
| Neutrophil | 128 | 12,360 (1890:66,540) | 153 | 9940 (1580:29,550) | 0.004 a |
| Lymphocyte | 128 | 980 (0.83:23,550) | 153 | 1180 (220:12,540) | 0.021 a |
| Monocyte | 128 | 395 (0:6180) | 153 | 350 (10:1160) | 0.239 a |
| Neutrophil/Lymphocyte | 128 | 13.77 (0.34:19,542.17) | 153 | 8.66 (0.42:98) | <0.001 a |
| PLT/Neutrophil | 128 | 17.59 (0.24:57.91) | 153 | 22.29 (1.81:143) | 0.002 a |
| PLT/Lymphocyte | 128 | 242.13 (3.33:238,554.22) | 153 | 218 (3.52:925.93) | 0.046 a |
| Lymphocyte/Monocyte | 127 | 2.27 (0.25:142) | 153 | 3.11 (0.64:68) | 0.006 a |
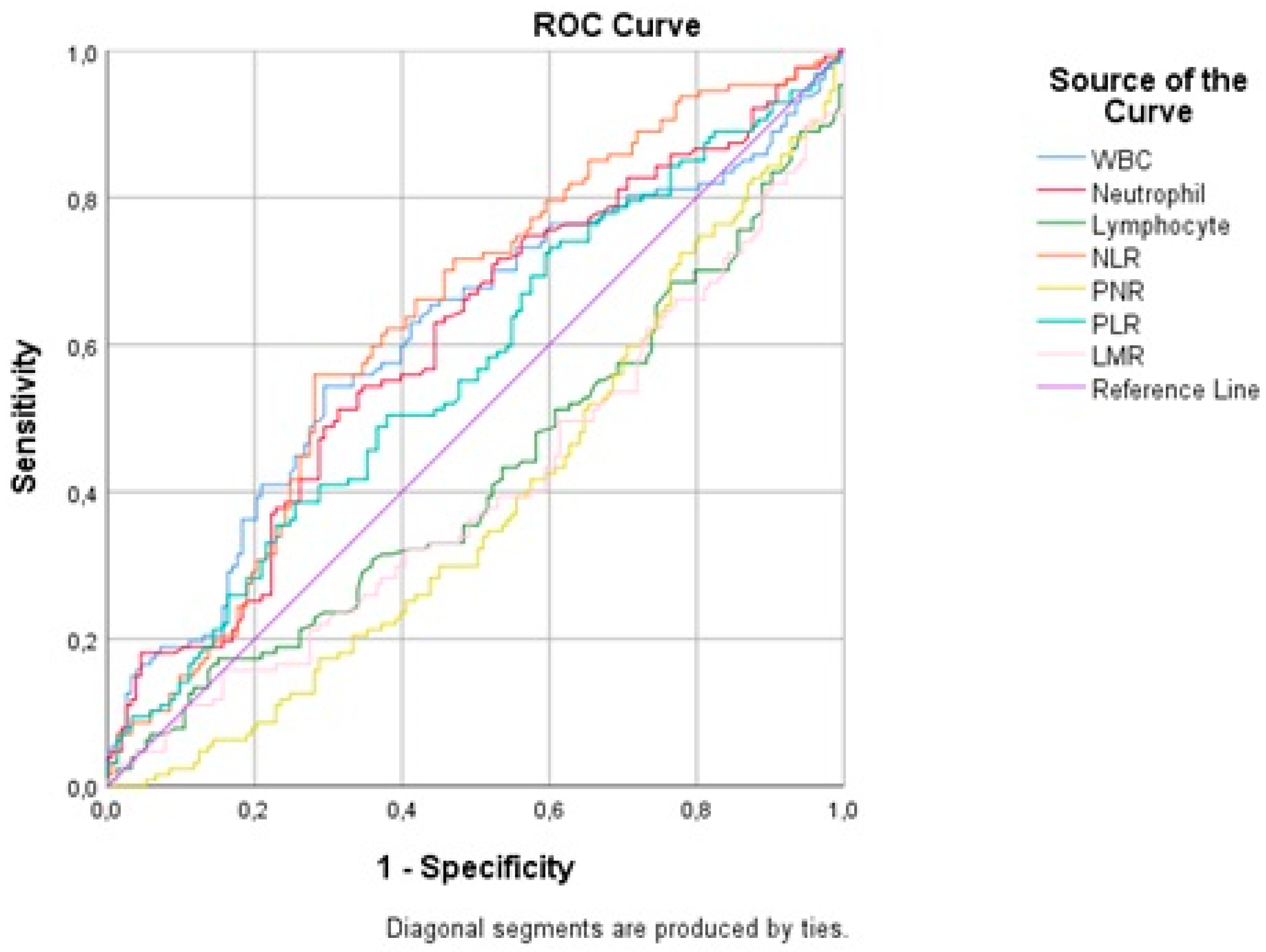
| AUC | 95% (CI) | Optimal Cut-Off Point | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| WBC | 0.60 | (0.551:0.668) | >13,760 | 53.91% | 70.59% |
| Neutrophil | 0.60 | (0.545:0.662) | >12,270 | 50.78% | 68.63% |
| Lymphocyte | 0.58 | (0.517:0.636) | <810 | 42.97% | 73.20% |
| NLR | 0.63 | (0.576:0.692) | >12.9 | 55.47% | 71.90% |
| PLR | 0.56 | (0.507:0.626) | >287.36 | 39.06% | 74.51% |
| LMR | 0.59 | (0.536:0.654) | ≤2.63 | 59.84% | 59.48% |
| PNR | 0.61 | (0.55:0.66) | ≤22.27 | 69.53% | 50.33% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çevikkalp, E.; Taşkapılıoğlu, M.Ö. Predictive Values of Hematological Parameters for Determining Imminent Brain Death: A Retrospective Study. Medicina 2023, 59, 417. https://doi.org/10.3390/medicina59020417
Çevikkalp E, Taşkapılıoğlu MÖ. Predictive Values of Hematological Parameters for Determining Imminent Brain Death: A Retrospective Study. Medicina. 2023; 59(2):417. https://doi.org/10.3390/medicina59020417
Chicago/Turabian StyleÇevikkalp, Eralp, and Mevlüt Özgür Taşkapılıoğlu. 2023. "Predictive Values of Hematological Parameters for Determining Imminent Brain Death: A Retrospective Study" Medicina 59, no. 2: 417. https://doi.org/10.3390/medicina59020417
APA StyleÇevikkalp, E., & Taşkapılıoğlu, M. Ö. (2023). Predictive Values of Hematological Parameters for Determining Imminent Brain Death: A Retrospective Study. Medicina, 59(2), 417. https://doi.org/10.3390/medicina59020417