
Assessment of Salvage Surgery in Persistent Cervical Cancer after Definitive Radiochemotherapy: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
1. Introduction
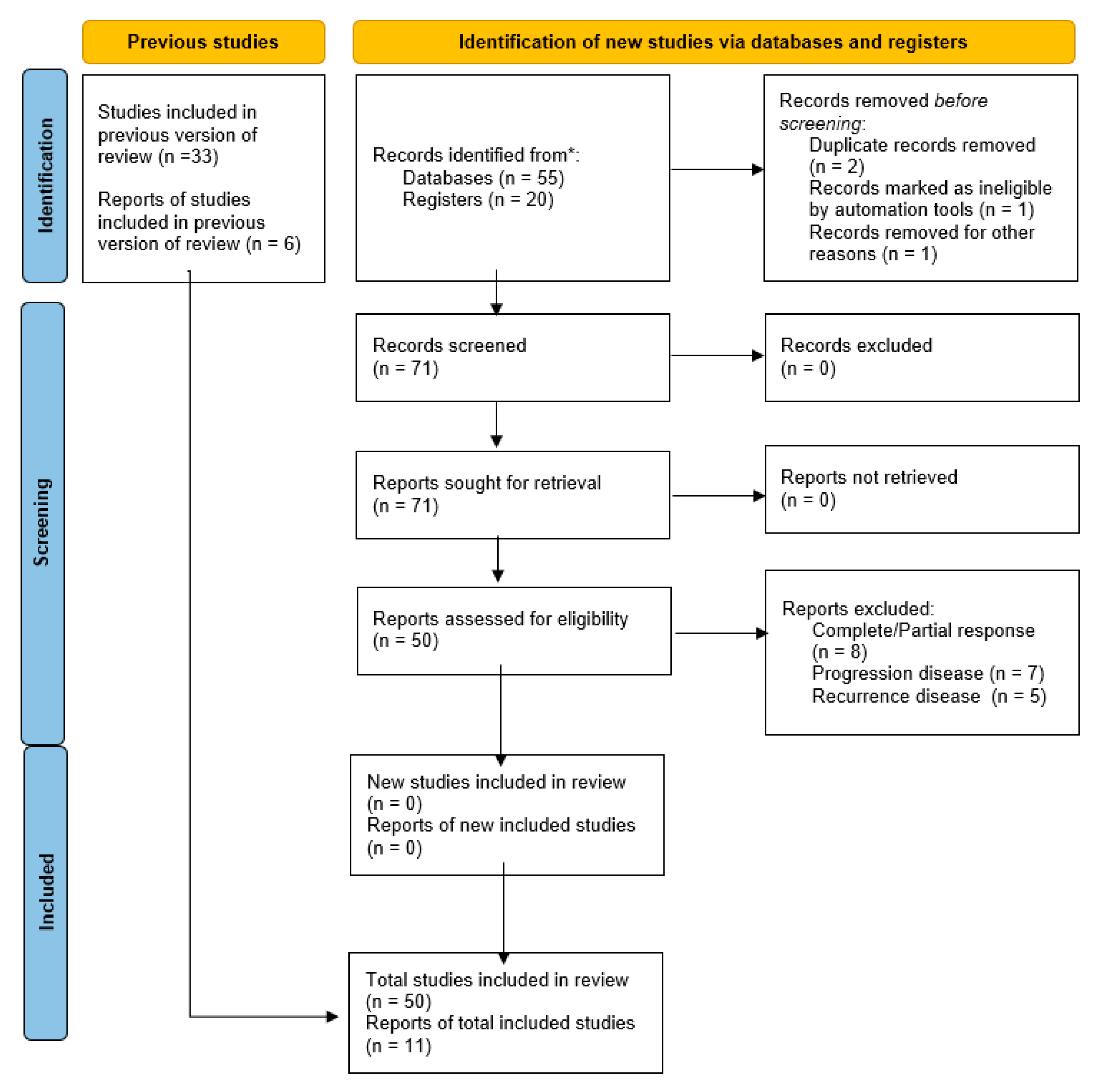
2. Material and Methods
2.1. Search Method
2.2. Study Selection
2.3. Statistical Analysis
2.4. Quality Assessment
3. Results
3.1. Studies’ Characteristics
3.2. Pathological Findings
3.3. Survival
3.4. Postoperative Complications
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, Second Edition: Use of mRNA Tests for Human Papillomavirus (HPV). 2021. Available online: https://www.who.int/publications/i/item/9789240040434 (accessed on 5 November 2022).
- Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (CCCMAC). Reducing analysis. Cochrane Database Syst. Rev. 2010, 1, CD8285. [Google Scholar]
- Rose, P.G.; Bundy, B.N.; Watkins, E.B.; Thigpen, J.T.; Deppe, G.; Maiman, M.A.; Clarke-Pearson, D.L.; Insalaco, S. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N. Engl. J. Med. 1999, 340, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic radiation with concurrent chemotherapy compared with pelvic and paraaortic radiation for high-risk cervical cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Whitney, C.W.; Sause, W.; Bundy, B.N.; Malfetano, J.H.; Hannigan, E.V.; Fowler, W.C.; Clarke-Pearson, D.L.; Liao, S.Y. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stages IIB--IVA carcinoma of the cervix with negative paraaortic lymph nodes. A Gynecologic Oncology Group and Southwest Oncology Group Study. J. Clin. Oncol. 1999, 17, 1339–1348. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie, M.C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother. Oncol. 2018, 127, 404–416. [Google Scholar] [CrossRef]
- NCCN: National Comprensive Cancer Network Cervical Cancer Versione 1. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 5 November 2022).
- Barbera, L.; Thomas, G. Management of early and locally advanced cervical cancer. Semin. Oncol. 2009, 36, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Touboul, C.; Uzan, C.; Mauguen, A.; Gouy, S.; Pautier, P.; Lhommé, C.; Duvillard, P.; Haie-Meder, C.; Morice, P. Prognostic factors and morbidities after completion surgery in patients undergoing initial chemoradiation therapy for locally advanced cervical cancer. Oncologist 2010, 15, 405–415. [Google Scholar] [CrossRef]
- Zannoni, G.F.; Vellone, V.G.; Carbone, A. Morphological effects of radiochemotherapy on cervical carcinoma: A morphological study of 50 cases of hysterectomy specimens after neoadjuvant treatment. Int. J. Gynecol. Pathol. 2008, 27, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Rouanet, P.; Rey, A.; Romestaing, P.; Houvenaeghel, G.; Boulanger, J.C.; Leveque, J.; Cowen, D.; Mathevet, P.; Malhaire, J.P.; et al. Results of the GYNECO 02 study, an FNCLCC phase III trial comparing hysterectomy with no hysterectomy in patients with a (clinical and radiological) complete response after chemoradiation therapy for stage IB2 or II cervical cancer. Oncologist 2012, 17, 64–71. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Azria, E.; Morice, P.; Haie-Meder, C.; Thoury, A.; Pautier, P.; Lhomme, C.; Duvillard, P.; Castaigne, D. Results of hysterectomy in patients with bulky residual disease at the end of chemoradiotherapy for stage IB2/II cervical carcinoma. Ann. Surg. Oncol. 2005, 12, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, E.R.; van der Zee, A.G.; in ‘t Hout, B.A.; Boomgaard, J.J.; de Hullu, J.A.; Pras, E.; Hollema, H.; Aalders, J.G.; Nijman, H.W.; Willemse, P.H.; et al. Gynecologic examination and cervical biopsies after (chemo) radiation for cervical cancer to identify patients eligible for salvage surgery. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Boers, A.; Arts, H.J.; Klip, H.; Nijhuis, E.R.; Pras, E.; Hollema, H.; Wisman, G.B.; Nijman, H.W.; Mourits, M.J.; Reyners, A.K.; et al. Radical surgery in patients with residual disease after (chemo)radiation for cervical cancer. Int. J. Gynecol. Cancer. 2014, 24, 1276–1285. [Google Scholar] [CrossRef]
- Chiantera, V.; Rossi, M.; De Iaco, P.; Koehler, C.; Marnitz, S.; Ferrandina, G.; Legge, F.; Parazzini, F.; Scambia, G.; Schneider, A.; et al. Survival after curative pelvic exenteration for primary or recurrent cervical cancer: A retrospective multicentric study of 167 patients. Int. J. Gynecol. Cancer. 2014, 24, 916–922. [Google Scholar] [CrossRef]
- Mabuchi, S.; Matsumoto, Y.; Komura, N.; Sawada, M.; Tanaka, M.; Yokoi, E.; Kozasa, K.; Yoshimura, A.; Kuroda, H.; Kimura, T. The efficacy of surgical treatment of recurrent or persistent cervical cancer that develops in a previously irradiated field: A monoinstitutional experience. Int. J. Clin. Oncol. 2017, 22, 927–936. [Google Scholar] [CrossRef]
- Platt, S.L.; Patel, A.; Humphrey, P.J.; Al-Booz, H.; Bailey, J. Completion surgery after chemoradiotherapy for cervical cancer–is there a role? UK Cancer Centre experience of hysterectomy post chemo-radiotherapy treatment for cervical cancer. J. Obstet. Gynaecol. 2018, 39, 68–73. [Google Scholar] [CrossRef]
- Gosset, M.; Chargari, C.; Bentivegna, E.; Leary, A.; Genestie, C.; Maulard, A.; Morice, P.; Gouy, S. Should We Cease to Perform Salvage Hysterectomy After Chemoradiation and Brachytherapy in Locally Advanced Cervical Cancer? Anticancer Res. 2019, 39, 2919–2926. [Google Scholar] [CrossRef]
- Pervin, S.; Ruma, F.I.; Rahman, K. Ferdous, J.; Ara, R.; Abu Syed, M.M.; Goodman, A. Adjuvant Hysterectomy in Patients With Residual Disease After Radiation for Locally Advanced Cervical Cancer: A Prospective Longitudinal Study. J. Glob. Oncol. 2019, 5, 1–7. [Google Scholar] [CrossRef]
- Topuz, S.; Kaban, A.; Küçücük, S.; Salihoglu, Y. Is Surgical Treatment an Option for Locally Advanced Cervical Cancer in the Presence of Central Residual Tumor after Chemoradiotherapy? Rev. Bras. Ginecol. Obstet. 2020, 42, 35–42. [Google Scholar] [CrossRef]
- Stanca, M.; Căpîlna, D.M.; Căpîlna, M.E. Long-Term Survival, Prognostic Factors, and Quality of Life of Patients Undergoing Pelvic Exenteration for Cervical Cancer. Cancers 2022, 14, 2346. [Google Scholar] [CrossRef] [PubMed]
- Vizzielli, G.; Tortorella, L.; Conte, C.; Chiantera, V.; Gallotta, V.; Foschi, N.; Arcieri, M.; Ferrandina, G.; Fagotti, A.; Zattoni, F.; et al. Is a Vaginectomy Enough or is a Pelvic Exenteration Always Required for Surgical Treatment of Recurrent Cervical Cancer? A Propensity-Matched Study. Ann. Surg. Oncol. 2021, 28, 3281–3290. [Google Scholar] [CrossRef]
- Bizzarri, N.; Chiantera, V.; Ercoli, A.; Fagotti, A.; Tortorella, L.; Conte, C.; Cappuccio, S.; Di Donna, M.C.; Gallotta, V.; Scambia, G.; et al. Minimally Invasive Pelvic Exenteration for Gynecologic Malignancies: A Multi-Institutional Case Series and Review of the Literature. J. Minim. Invasive Gynecol. 2019, 26, 1316–1326. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Gallotta, V.; Foschi, N.; Costantini, B.; Conte, C.; Pinto, F.; Ercoli, A.; Ferrandina, G.; Dal Moro, F.; Bassi, P.; et al. Surgical outcomes of segmental ureteral resection with ureteroneocystostomy after major gynecologic surgery. Eur. J. Surg. Oncol. 2020, 46, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Gallotta, V.; Chiantera, V.; Conte, C.; Vizzielli, G.; Fagotti, A.; Nero, C.; Costantini, B.; Lucidi, A.; Cicero, C.; Scambia, G.; et al. Robotic Radical Hysterectomy After Concomitant Chemoradiation in Locally Advanced Cervical Cancer: A Prospective Phase II Study. J. Minim. Invasive Gynecol. 2017, 24, 133–139. [Google Scholar] [CrossRef]
- Fagotti, A.; Conte, C.; Stollagli, F.; Gallotta, V.; Salutari, V.; Bottoni, C.; Bruno, M.; Zannoni, G.F.; Scambia, G. Radical Surgery in Advanced Cervical Cancer Patients Receiving Bevacizumab-Containing Chemotherapy: A “Real Life Experience”. Int. J. Gynecol. Cancer. 2018, 28, 1569–1575. [Google Scholar] [CrossRef]
- Gaballa, K.; Denewer, A.; Khater, A.; Gallotta, V.; Conte, C.; Federico, A.; Elfeki, H.; Scambia, G. Feasibility of early postoperative bladder catheter removal without prior bladder-training exercises after laparoscopic nerve sparing radical hysterectomy. J. Obstet. Gynaecol. 2019, 39, 788–792. [Google Scholar] [CrossRef]
- Tinelli, G.; Cappuccio, S.; Parente, E.; Fagotti, A.; Gallotta, V.; Conte, C.; Costantini, B.; Gueli Alletti, S.; Scambia, G.; Vizzielli, G. Resectability and Vascular Management of Retroperitoneal Gynecological Malignancies: A Large Single-institution Case-Series. Anticancer. Res. 2017, 37, 6899–6906. [Google Scholar] [CrossRef]
- Ferrandina, G.; Distefano, M.G.; De Vincenzo, R.; Salutari, V.; Petrillo, M.; Scarciglia, M.L.; Pietragalla, A.; Conte, C.; Scambia, G. Paclitaxel, epirubicin, and cisplatin (TEP) regimen as neoadjuvant treatment in locally advanced cervical cancer: Long-term results. Gynecol. Oncol. 2013, 128, 518–523. [Google Scholar] [CrossRef]
- Cetina, L.; González-Enciso, A.; Cantú, D.; Coronel, J.; Pérez-Montiel, D.; Hinojosa, J.; Serrano, A.; Rivera, L.; Poitevin, A.; Mota, A.; et al. Brachytherapy versus radical hysterectomy after external beam chemoradiation with gemcitabine plus cisplatin: A randomized, phase III study in IB2–IIB cervical cancer patients. Ann. Oncol. 2013, 24, 2043–2047. [Google Scholar] [CrossRef]
- Ferrandina, G.; Margariti, P.A.; Smaniotto, D.; Petrillo, M.; Salerno, M.G.; Fagotti, A.; Macchia, G.; Morganti, A.G.; Cellini, N.; Scam-bia, G. Long-term analysis of clinical outcome and complications in locally advanced cervical cancer patients administered concomitant chemoradiation followed by radical surgery. Gynecol. Oncol. 2010, 119, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Sardain, H.; Lavoue, V.; Redpath, M.; Bertheuil, N.; Foucher, F.; Levêque, J. Curative pelvic exenteration for recurrent cervical carcinoma in the era of concurrent chemotherapy and radiation therapy. A systematic review. Eur. J. Surg. Oncol. 2015, 41, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Marnitz, S.; Köhler, C.; Müller, M.; Behrens, K.; Hasenbein, K.; Schneider, A. Indications for primary and secondary exenterations in patients with cervical cancer. Gynecol. Oncol. 2006, 103, 1023–1030. [Google Scholar] [CrossRef]
- Rockall, A.G.; Ghosh, S.; Alexander-Sefre, F.; Babar, S.; Younis, M.T.; Naz, S.; Jacobs, I.J.; Reznek, R.H. Can MRI rule out bladder and rectal invasion in cervical cancer to help select patients for limited EUA? Gynecol. Oncol. 2006, 101, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Ahn, H.S.; Kim, Y.S.; Lee, E.J.; Ryu, H.S.; Chang, K.H.; Kim, S.J. The value of cystoscopy and intravenous urography after magnetic resonance imaging or computed tomography in the staging of cervical carcinoma. Yonsei Med. J. 2001, 42, 527–531. [Google Scholar] [CrossRef]
- Hertel, H.; Köhler, C.; Elhawary, T.; Michels, W.; Possover, M.; Schneider, A. Laparoscopic staging compared with imaging techniques in the staging of advanced cervical cancer. Gynecol. Oncol. 2002, 87, 46–51. [Google Scholar] [CrossRef]
- Manganaro, L.; Lakhman, Y.; Bharwani, N.; Gui, B.; Gigli, S.; Vinci, V.; Rizzo, S.; Kido, A.; Cunha, T.M.; Sala, E.; et al. Staging, recurrence and follow-up of uterine cervical cancer using MRI: Updated Guidelines of the European Society of Urogenital Radiology after revised FIGO staging 2018. Eur. Radiol. 2021, 31, 7802–7816. [Google Scholar] [CrossRef]
- Vincens, E.; Balleyguier, C.; Rey, A.; Uzan, C.; Zareski, E.; Gouy, S.; Pautier, P.; Duvillard, P.; Haie-Meder, C.; Morice, P. Accuracy of magnetic resonance imaging in predicting residual disease in patients treated for stage IB2/II cervical carcinoma with chemoradiation therapy: Correlation of radiologic findings with surgicopathologic results. Cancer 2008, 113, 2158–2165. [Google Scholar] [CrossRef]
- Sala, E.; Rockall, A.G.; Freeman, S.J.; Mitchell, D.G.; Reinhold, C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: What the radiologist needs to know. Radiology 2013, 266, 717–740. [Google Scholar] [CrossRef]
- Balcacer, P.; Shergill, A.; Litkouhi, B. MRI of cervical cancer with a surgical perspective: Staging, prognostic implications and pitfalls. Abdom. Radiol. 2019, 44, 2557–2571. [Google Scholar] [CrossRef]
- Jalaguier-Coudray, A.; Villard-Mahjoub, R.; Delouche, A. Value of dynamic contrastenhanced and diffusion weighted MR imaging in the detection of pathologic complete response in cervical cancer after neoadjuvant therapy: A retrospective observational study. Radiology 2017, 284, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Gillies, J.R.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. 2018, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Autorino, R.; Gui, B.; Panza, G.; Boldrini, L.; Cusumano, D.; Russo, L.; Nardangeli, A.; Persiani, S.; Campitelli, M.; Ferrandina, G.; et al. Radiomics-based prediction of two-year clinical outcome in locally advanced cervical cancer patients undergoing neoadjuvant chemoradiotherapy. Radiol. Med. 2022, 127, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Sodeikat, P.; Lia, M.; Martin, M.; Horn, L.C.; Höckel, M.; Aktas, B.; Wolf, B. The Importance of Clinical Examination under General Anesthesia: Improving Parametrial Assessment in Cervical Cancer Patients. Cancers 2021, 13, 2961. [Google Scholar] [CrossRef]
- Lavoué, V.; Voguet, L.; Bertel, C.; Mesbah, H.; Williaume, D.; Laguerre, B.; Porée, P.; Foucher, F.; Montpetit, E.; Leblanc, M.; et al. Place of surgery before and after concurrent chemoradiotherapy for locally advanced cervical carcinoma: A retrospective study of 102 cases. J. Gynecol. Obstet. Biol. Reprod 2011, 40, 11–21. [Google Scholar] [CrossRef]
- Fanfani, F.; Fagotti, A.; Ferrandina, G.; Raspagliesi, F.; Ditto, A.; Cerrotta, A.M.; Morganti, A.; Smaniotto, D.; Scambia, G. Neoadjuvant chemoradiation followed by radical hysterectomy in FIGO stage IIIB cervical cancer: Feasibility, complications, and clinical outcome. Int. J. Gynecol. Cancer 2009, 19, 1119–1124. [Google Scholar] [CrossRef]
- van Kol, K.G.G.; Ebisch, R.M.F.; Piek, J.M.J.; Zusterzeel, P.L.M.; Vergeldt, T.F.M.; Bekkers, R.L.M. Salvage surgery for patients with residual disease after chemoradiation therapy for locally advanced cervical cancer: A systematic review on indication, complications, and survival. Acta. Obstet. Gynecol. Scand. 2021, 100, 1176–1185. [Google Scholar] [CrossRef]
- Mascilini, F.; Quagliozzi, L.; Moro, F.; Moruzzi, M.C.; De Blasis, I.; Paris, V.; Scambia, G.; Fagotti, A.; Testa, A.C. Role of transvaginal ultrasound-guided biopsy in gynecology. Int. J. Gynecol. Cancer. 2020, 30, 128–132. [Google Scholar] [CrossRef]
- Hoeijmakers, Y.M.; Zusterzeel, P.L.M.; Snyers, A.; Ham, M.A.P.C.v.; Bekkers, R.L.M. Cervical biopsy after chemoradiation for locally advanced cervical cancer to identify residual disease: A retrospective cohort study. J. Surg. Oncol. 2019, 2, 2–6. [Google Scholar]
- Mabuchi, S.; Komura, N.; Kodama, M.; Matsuzaki, S.; Matsumoto, Y.; Kamiura, S.; Kimura, T. Impact of lymphadenectomy in patients with locally recurrent or persistent cervical cancer treated with salvage hysterectomy. J. Obstet. Gynaecol. Res. 2022. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort a | Selection of the Non-Exposed Cohort | Ascertainment of Exposure b | Demonstration That Outcome of Interest Was not Present at Start of Study | Comparability of Cohorts | Assessment of Outcome c | FUP d | Adequacy of FUP | Quality | |
| Azria (2005) [14] | NA | NA | 22 (range 1–37) | 1 patient lost to FUP | Good | ||||
| Nijhuis (2006) [15] | 62.4 (range 46.8–105.6) | No lost to FUP | Good | ||||||
| Boers (2014) [16] | 27.6 (IQR, 15.6–56.4) | No lost to FUP | Good | ||||||
| Chiantera (2014) [17] | 68 (range 47–94) | No lost to FUP | Good | ||||||
| Mabuchi (2017) [18] | 41.5 (mean) | No statement about lost to FUP | Good | ||||||
| Platt (2018) [19] | NA | NA | 31 (range 12–60) | No lost to FUP | Good | ||||
| Gosset (2019) [20] | NA | NA | No statement about FUP | No statement about lost to FUP | Fair | ||||
| Pervin (2019) [21] | NA | NA | 93.6 (mean) | No statement about lost to FUP | Fair | ||||
| Topuz (2020) [22] | NA | 20 (range 6–118) | 1 patient lost to FUP | Good | |||||
| Touboul (2020) [9] | 43.2 (range 2.4–127.2) | 4 patients lost to FUP | Good | ||||||
| Stanca (2022) [23] | NA | NA | 44.5 (1–88) | Good | |||||
| Authors (Year of Publication) | Total Number of Pts Included in the Study (Pts with Persistent Disease) | FIGO Stage at Diagnosis | Histology | RTCT Treatment | Total Number of Patients with Salvage Surgery (H and PE) | Lymphadenectomy(P and AO) | Median Tumor Size, mm (Range) |
|---|---|---|---|---|---|---|---|
| Azria (2005) [14] | 10 (10) | IIA = 2 IIB = 8 | SCC = 8 AC = 2 | EBRT 45 Gy with concomitant cisplatin 40 mg/m2) with 15 GyBRT | 10 (H = 9) (PE = 1) | P = 8 AO = 8 | 60 (40–90) |
| Nijhuis (2006) [15] | 165 (21) | NA | NA | EBRT 45 Gy with concomitant carboplatin and 5-FU (before 1999) and cisplatin 40 mg/m2 (after 1999) with 35 Gy BRT | 13 (H = 12) (PE = 1) | 0 | NA |
| Boers (2014) [16] | 491 (84) | IB1 = 4 IB2 = 16 IIA = 8 IIB = 29 IIIA = 2 IIIB = 2 | SCC = 35 AC = 20 ACS = 2 | EBRT 45 Gy in fractions of 1.8 Gy, from 1994 additional BRT total dose 34.8 Gy. Before 1999 carboplatin (300 mg/m2) and 5 FU (600 mg/m2). After 1999 cisplatin 40 mg/m2) | 61 (H = 56) (PE = 5) | 0 | NA |
| Chiantera (2014) [17] | 167 (34) | NA | SCC = 144 AC = 22 Other = 1 | NA | 167 (PE = 167) | P = 83 PA = 46 | NA |
| Mabuchi (2017) [18] | 51 (34) | IB2-IIA = 10 IIB-IVA = 39 IVB = 2 | SCC = 29 AC = 19 Other = 3 | EBRT 45 Gy with/without concomitant weekly cisplatin 40 mg/m2 with 3 doses of BRT | 46 (H = 37) (PE = 9) | P and/or PA = 36 | 30 (5–70) |
| Platt (2018) [19] | 15 (15) | IB2 = 2 IIA = 1 IIB = 9 IIIB = 3 | SCC = 8 AC = 7 | EBRT 45 Gy with concomitant weekly cisplatin 40 mg/m2 with 3 doses of BRT | 15 (H = 15) | 0 | 44 (23–53) |
| Gosset (2019) [20] | 31 (29) | IB2 = 8 IIA = 2 IIB = 18 III = 1 | SCC = 22 AC = 7 | EBRT 45–50.4 Gy in 25–28 fractions of 1.8 Gy over 5 weeks with concomitant cisplatin (40 mg/m2) with 15 Gy BRT | 29 (H = 29) | P = 1 PA = 19 P and PA = 1 | 19 (6–40) |
| Pervin (2019) [21] | 55 (40) | IIB = 25 IIIB = 7 At least IIB = 8 | SCC = 32 AC = 7 ACS = 1 | EBRT 50 Gy in 25fractions of 2 Gy for25 days with or without3 × 7 Gy BT. 23 patients received 3 doses cisplatin | 40 (H = 40) | P and PA = 40 | >2 cm (30%) <2 cm (70%) |
| Topuz (2020) [22] | 25 (23) | At least IB2 = 23 | SCC = 16 AC = 7 | EBRT, 1.8–2 Gy per fraction, Total 45–50 Gy with cisplatin 40 mg/m2/week and BT 5 Gy once weekly for 5 weeks | 23 (H = 21) (PE = 2) | 0 | NA |
| Touboul (2020) [9] | 150 (78) | IB2 = 48 II = 91 III = 10 IV = 1 | SCC = 108 AC = 26 Other = 16 | EBRT 45 Gy with concomitant weekly cisplatin 40 mg/m2 with BRT 15 Gy | 150 (H = 150) | P = 5 PA = 82 P & PA = 49 | NA |
| Stanca (2022) [23] | 47 (5) | NA | SCC = 40 AC = 7 | EBRT 45 Gy with concomitant weekly cisplatin 40 mg/m2 with BRT 15 Gy | 47 (PE = 47) | P = 47 | <4 cm (51.1%) ≥4 cm (48.9%) |
| Authors (Year of Publication) | Positive Pathology after Salvage Surgery (%) | Positive Margins (%) | Patients with at Least One Metastatic Lymph Node (%) | N severe Complications Grade ≥ 3 (%) | Follow-Up Period Median Months (Range) | Recurrence (%) | Median DFS Months (Range) | Death (%) | Median OS Months (Range) |
|---|---|---|---|---|---|---|---|---|---|
| Azria (2005) [14] | 10 (100) | 1 (10) | 5 (50) | 4 (40) | 22 (1–37) | 7 (70) | 18 (6–36) | 4 (40) | 24 (9–37) |
| Nijhuis (2006) [15] | 13 (100) | 2 (15.4) | 0 | NA | NA | 8 (61.5) | NA | 8 (61.5) | 48 (11–105) |
| Boers (2014) [16] | 44 (72) | 8 (13) | 0 | 14 (23) | 27.6 | 31 (50) | NA | 29 (47.5) | NA |
| Chiantera (2014) [17] | 167 (100) | 46 (27.5) | 49 (23) | 58 (34.7) | NA | 41 (33.9) | 13.4 (1.4–114) | 99 (59.3) | 19 (15–239) |
| Mabuchi (2017) [18] | 51 (100) | 14 (27.4) | 20 (39.2) | 11 (21.6) | 41.5 | 23 (45.1) | 23.3 | 19 (37.3) | 29 |
| Platt (2018) [19] | 4 (26.7) | NA | 0 | 3 (20) | 13 (12–60) | 3 (20) | n.r. (10–31) | 1 (6.7) | n.r. |
| Gosset (2019) [20] | 14 (48.3) | 2 (6.9) | 3 (10.3) | 7 (24) | NA | 3 (10.3) | n.r. (9–43) | NA | NA |
| Pervin (2019) [21] | 40 (100) | 0 | 0 | 2 (5) | 93.6 (60–108) | 4 (10) | NA | 1 (2.5) | NA |
| Topuz (2020) [22] | 18 (78.2) | 10 (43.5) | 0 | 12 (52.2) | 20 (6–118) | 14 (60.8) | 15 (6–23) | 9 (39.1) | 20 (in positive margins) 36 (in negative margins) |
| Touboul (2020) [9] | 78 (52) | 9 (7) | 47 (31.3) | 37 (25) * | 43 (2–127) | 41 (27) | 5-ys = 66% | 37 (24.7) | NA (5 ys = 71%) |
| Stanca (2022) [23] | 47 (100) | 17 (36) | 15 (31.9) | 27 (57.5) | 44.5 (1–118) | NA | NA | 22 (46.8) | 49.4 (5 ys = 48.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conte, C.; Della Corte, L.; Pelligra, S.; Bifulco, G.; Abate, B.; Riemma, G.; Palumbo, M.; Cianci, S.; Ercoli, A. Assessment of Salvage Surgery in Persistent Cervical Cancer after Definitive Radiochemotherapy: A Systematic Review. Medicina 2023, 59, 192. https://doi.org/10.3390/medicina59020192
Conte C, Della Corte L, Pelligra S, Bifulco G, Abate B, Riemma G, Palumbo M, Cianci S, Ercoli A. Assessment of Salvage Surgery in Persistent Cervical Cancer after Definitive Radiochemotherapy: A Systematic Review. Medicina. 2023; 59(2):192. https://doi.org/10.3390/medicina59020192
Chicago/Turabian StyleConte, Carmine, Luigi Della Corte, Silvia Pelligra, Giuseppe Bifulco, Biagio Abate, Gaetano Riemma, Marco Palumbo, Stefano Cianci, and Alfredo Ercoli. 2023. "Assessment of Salvage Surgery in Persistent Cervical Cancer after Definitive Radiochemotherapy: A Systematic Review" Medicina 59, no. 2: 192. https://doi.org/10.3390/medicina59020192
APA StyleConte, C., Della Corte, L., Pelligra, S., Bifulco, G., Abate, B., Riemma, G., Palumbo, M., Cianci, S., & Ercoli, A. (2023). Assessment of Salvage Surgery in Persistent Cervical Cancer after Definitive Radiochemotherapy: A Systematic Review. Medicina, 59(2), 192. https://doi.org/10.3390/medicina59020192