
Diagnostic and Prognostic Value of IL-10, FABP2 and LPS Levels in HCC Patients

 and
and
Abstract
:1. Introduction
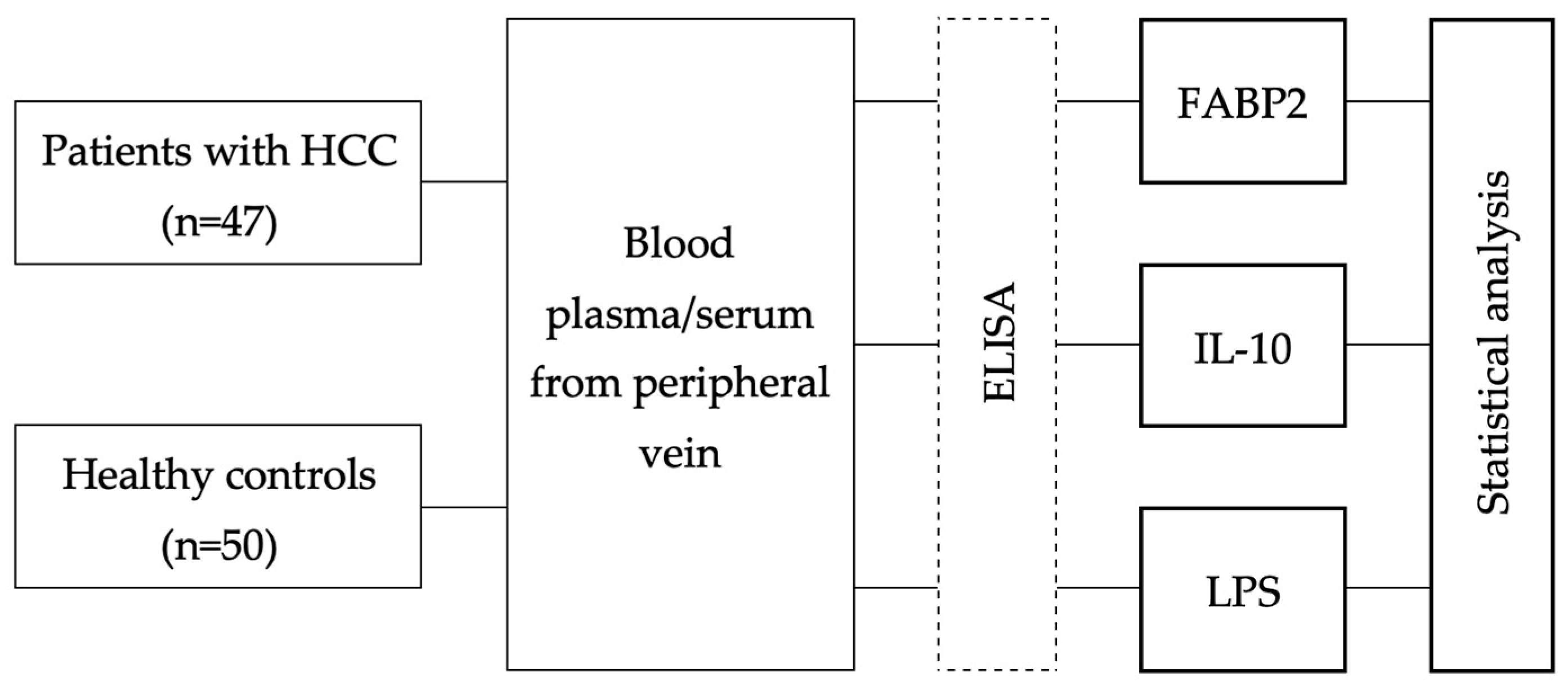
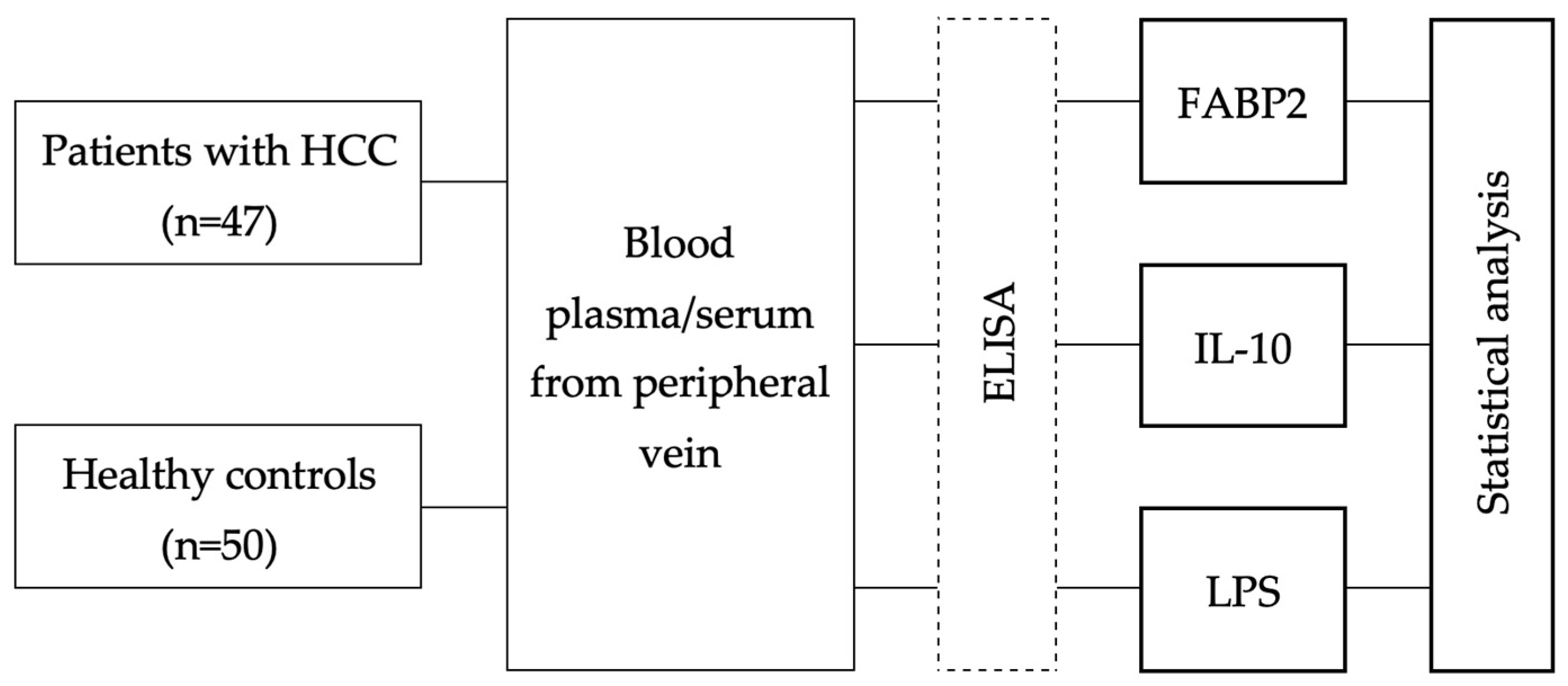
2. Materials and Methods
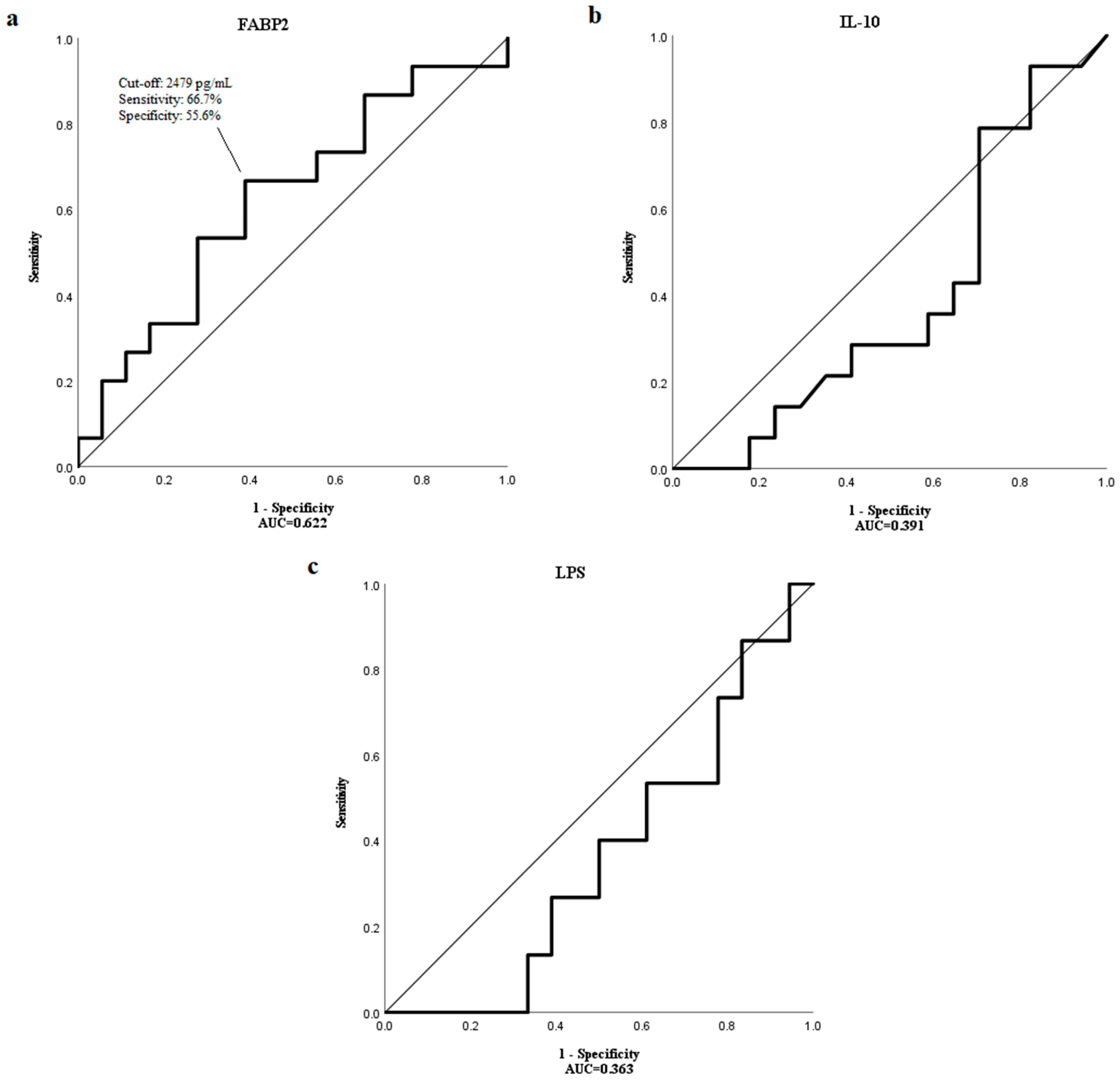
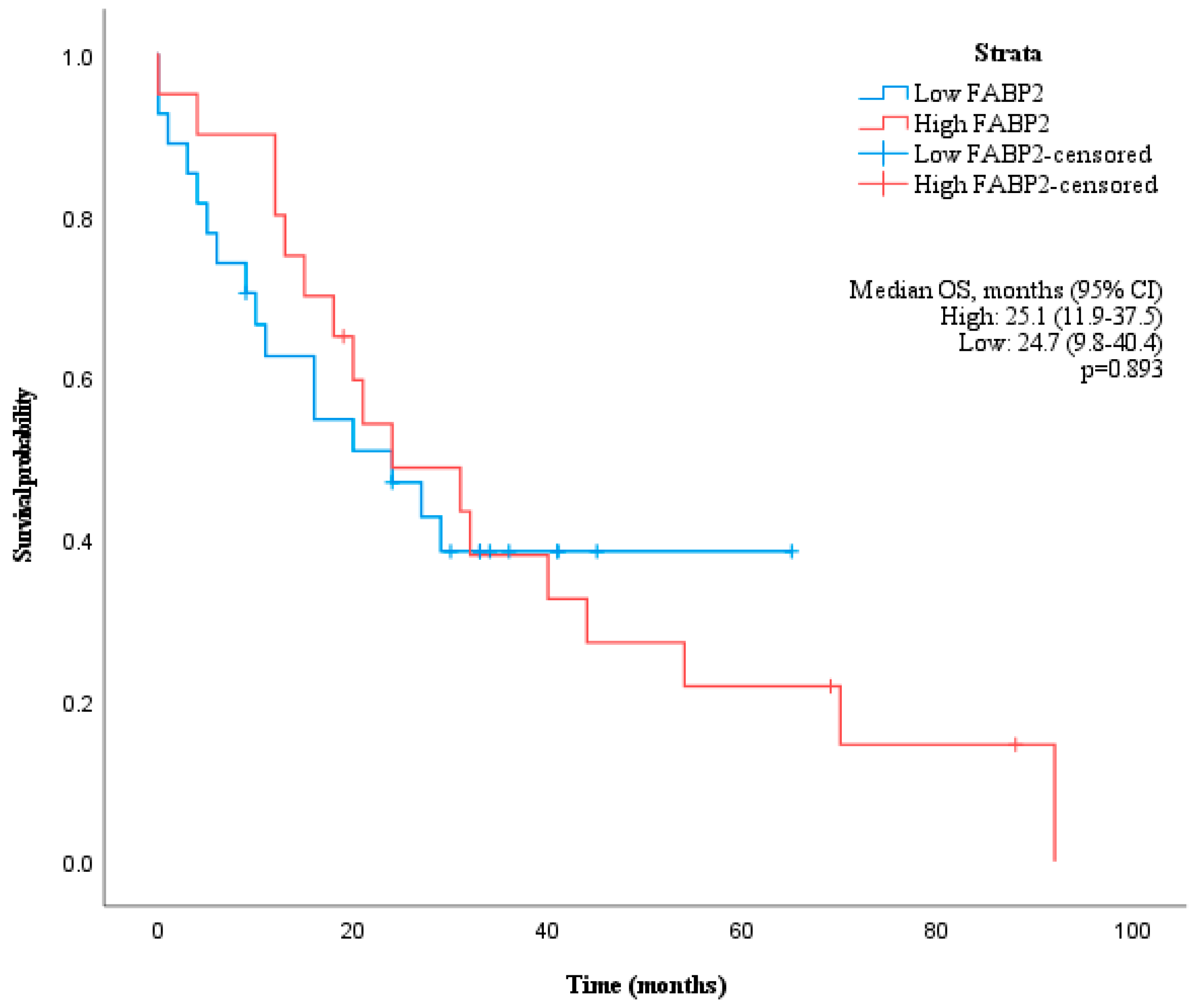
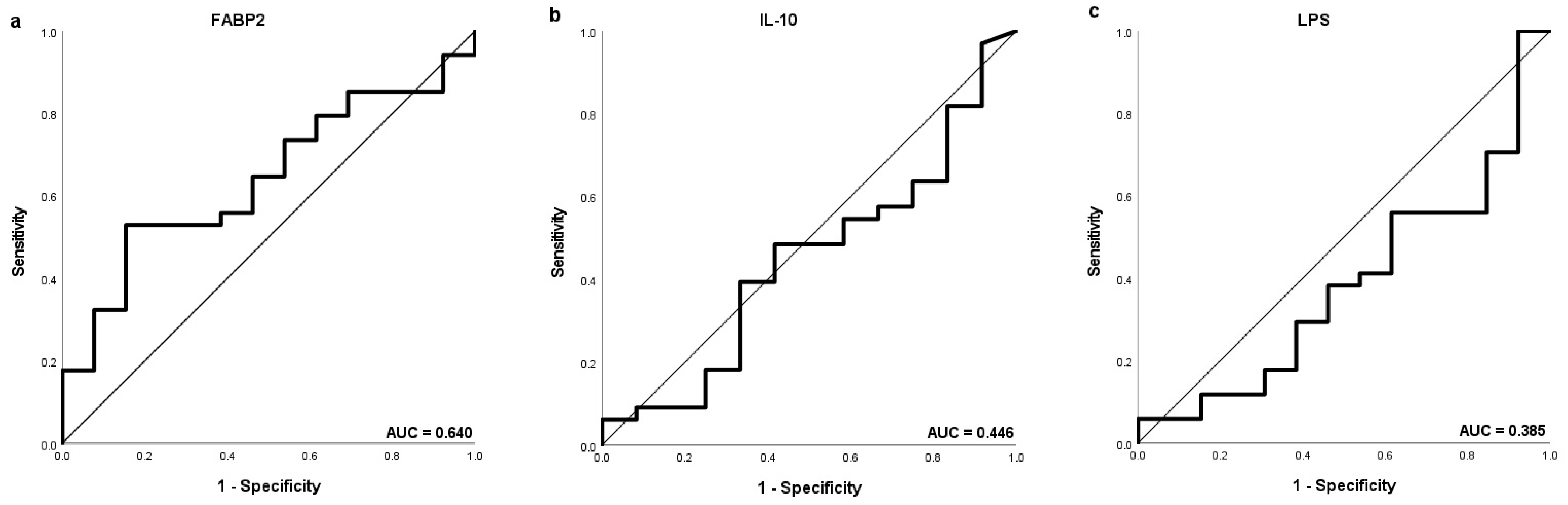
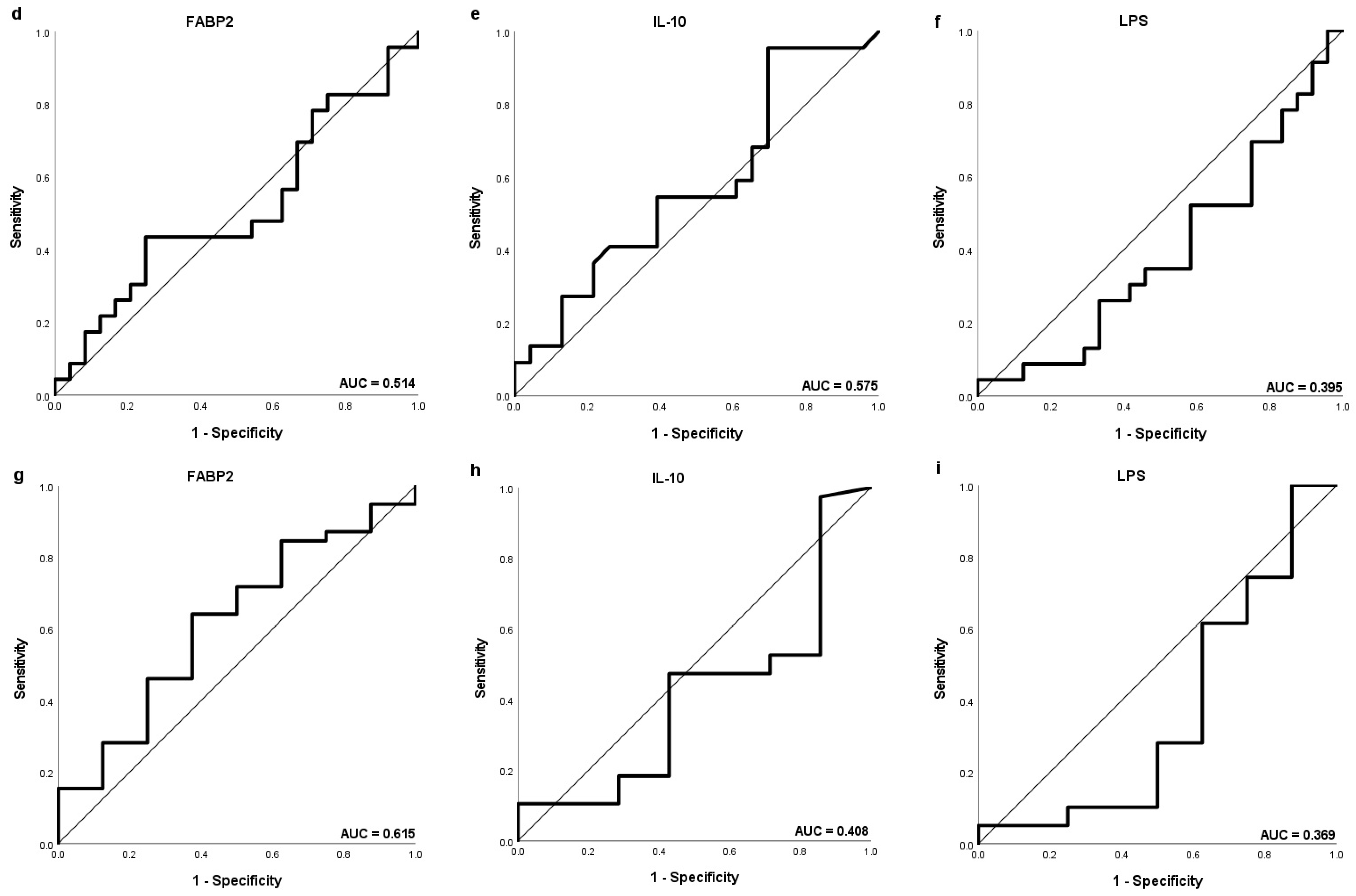
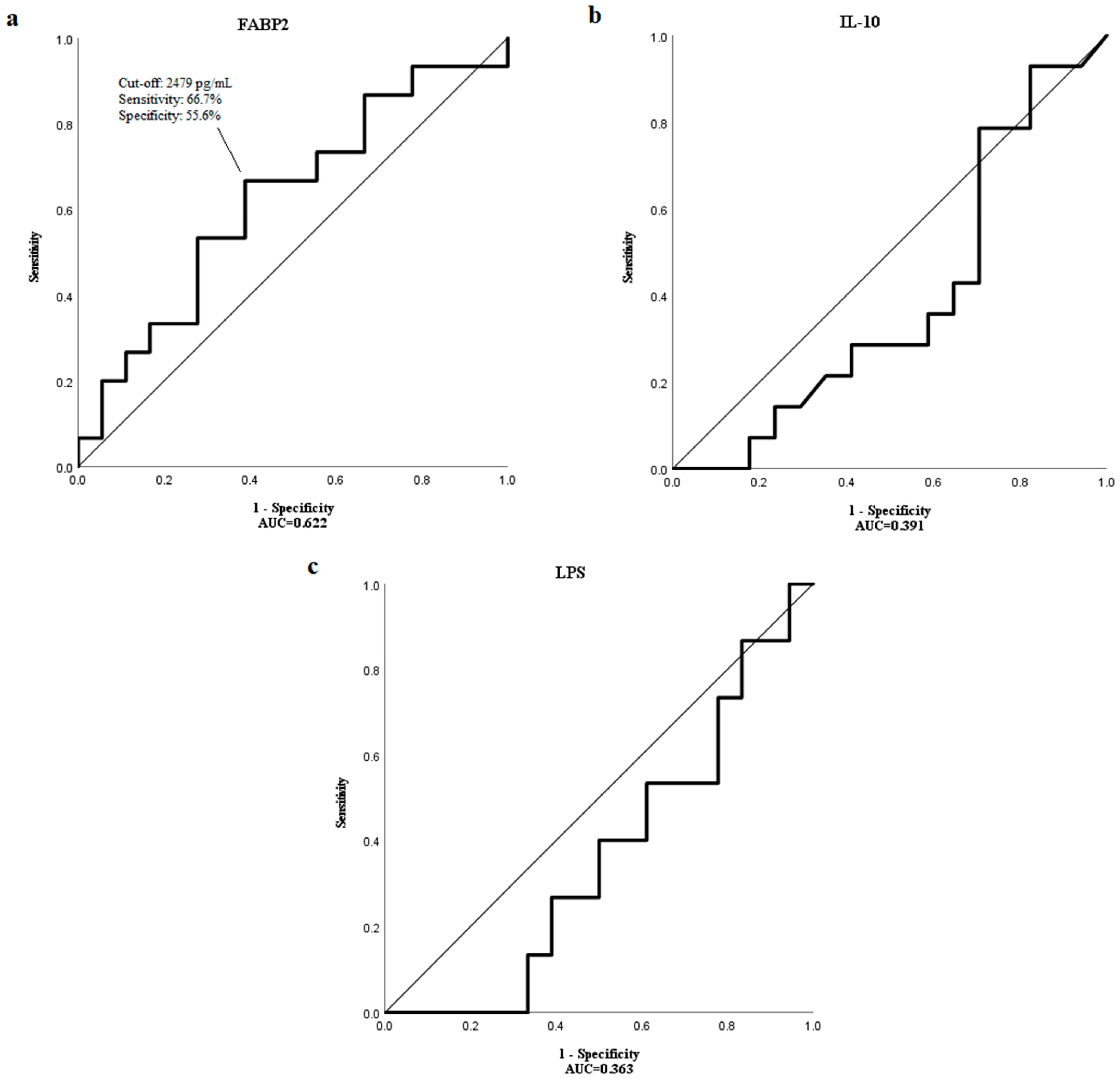
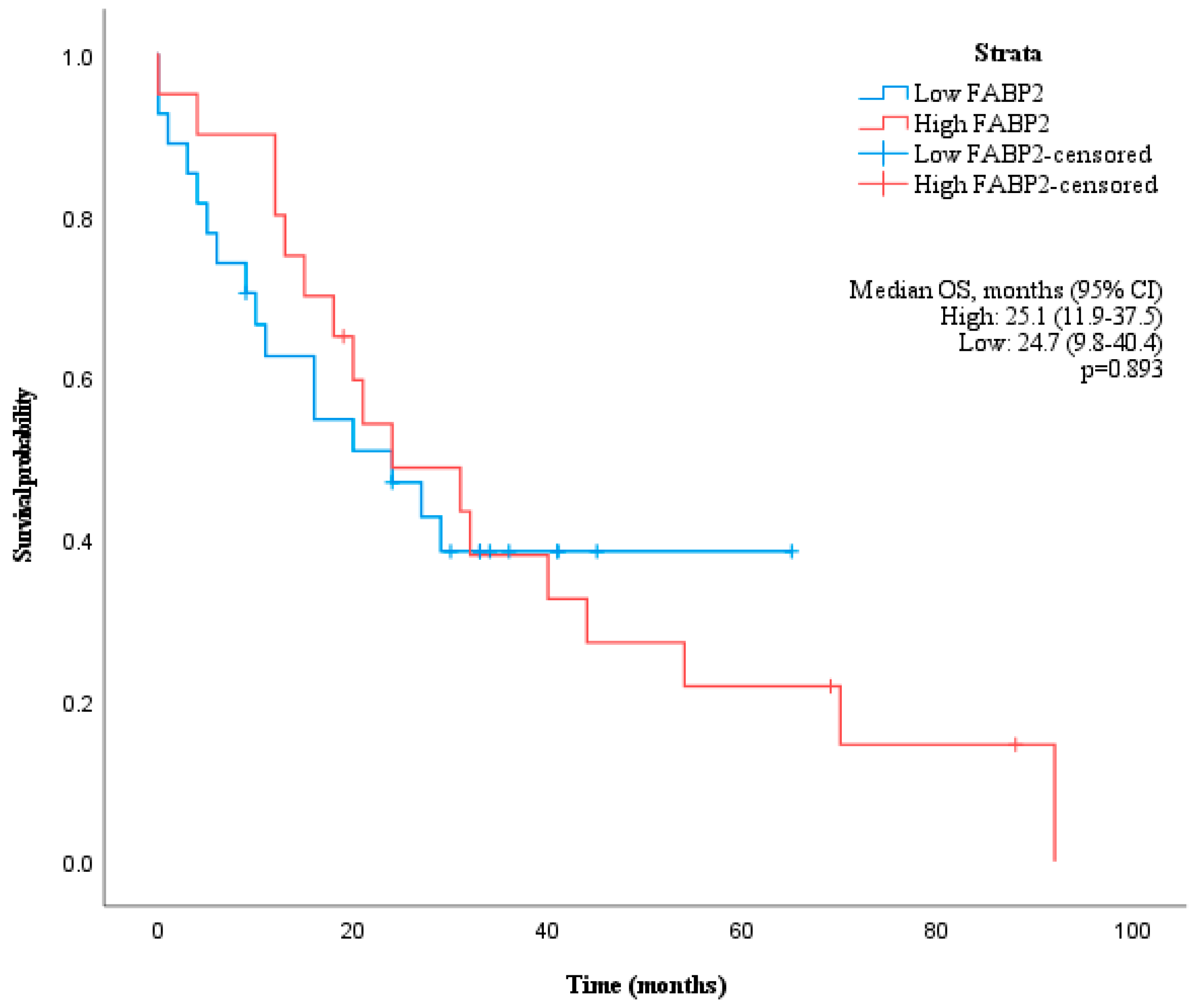
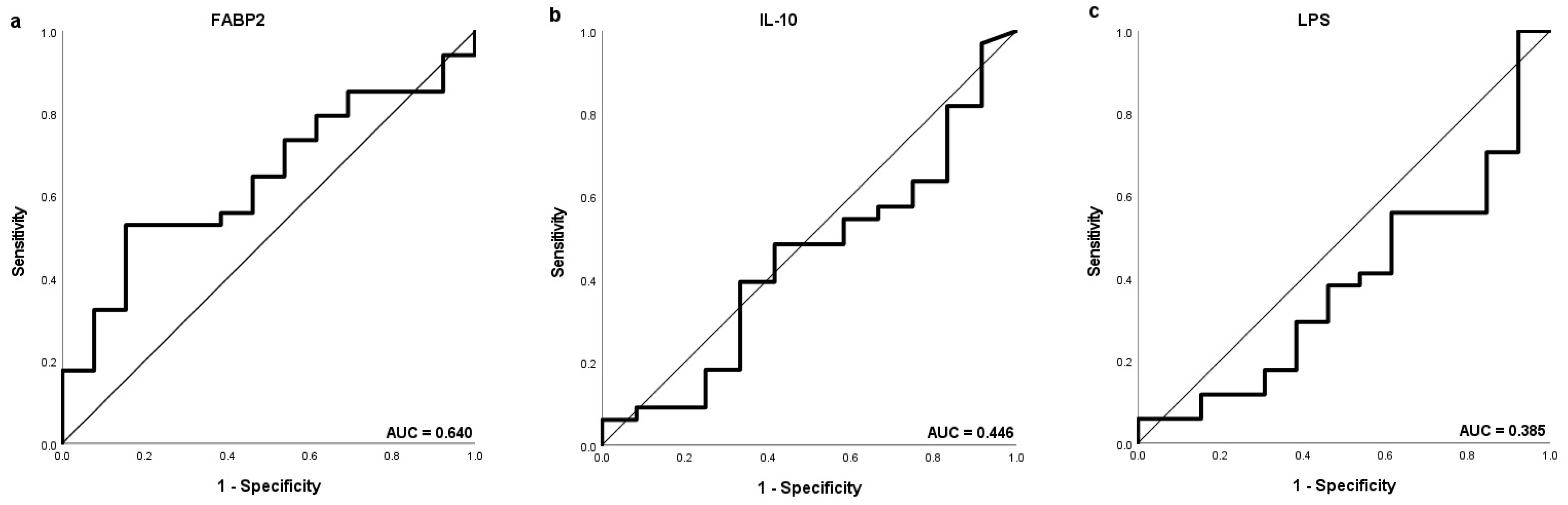
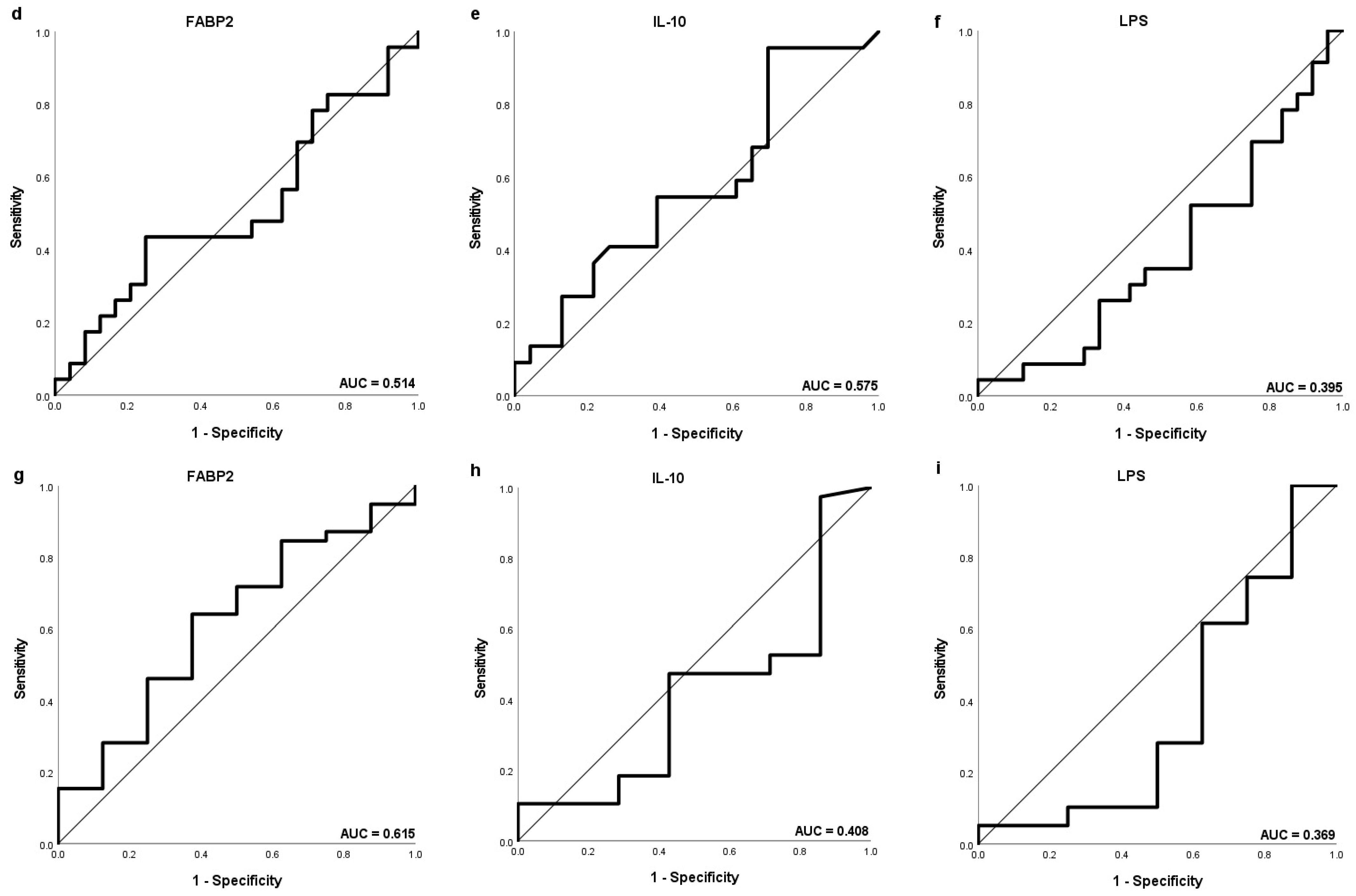
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, P.; Hu, K.; Dai, G.; Li, J.; Zheng, D.; Yuan, H.; He, L.; Xie, P.; Tu, M.; et al. Inflammatory microenvironment of fibrotic liver promotes hepatocellular carcinoma growth, metastasis and sorafenib resistance through STAT3 activation. J. Cell Mol. Med. 2021, 25, 1568–1582. [Google Scholar] [CrossRef] [PubMed]
- Bishayee, A. The role of inflammation and liver cancer. Adv. Exp. Med. Biol. 2014, 816, 401–435. [Google Scholar]
- Ceni, E.; Mello, T.; Galli, A. Pathogenesis of alcoholic liver disease: Role of oxidative metabolism. World J. Gastroenterol. 2014, 20, 17756–17772. [Google Scholar] [CrossRef]
- Barooah, P.; Saikia, S.; Kalita, M.J.; Bharadwaj, R.; Sarmah, P.; Bhattacharyya, M.; Goswami, B.; Medhi, S. IL-10 Polymorphisms and Haplotypes Predict Susceptibility to Hepatocellular Carcinoma Occurrence in Patients with Hepatitis C Virus Infection from Northeast India. Viral Immunol. 2020, 33, 457–467. [Google Scholar] [CrossRef]
- Bellot, P.; Francés, R.; Such, J. Pathological bacterial translocation in cirrhosis: Pathophysiology, diagnosis and clinical implications. Liver Int. 2013, 33, 31–39. [Google Scholar] [CrossRef]
- Loosen, S.H.; Schulze-Hagen, M.; Leyh, C.; Benz, F.; Vucur, M.; Kuhl, C.; Trautwein, C.; Tacke, F.; Bruners, P.; Roderburg, C.; et al. IL-6 and IL-8 Serum Levels Predict Tumor Response and Overall Survival after TACE for Primary and Secondary Hepatic Malignancies. Int. J. Mol. Sci. 2018, 19, 1766. [Google Scholar] [CrossRef]
- Seidensticker, M.; Powerski, M.; Seidensticker, R.; Damm, R.; Mohnike, K.; Garlipp, B.; Klopffleisch, M.; Amthauer, H.; Ricke, J.; Pech, M. Cytokines and (90)Y-Radioembolization: Relation to Liver Function and Overall Survival. Cardiovasc. Intervent. Radiol. 2017, 40, 1185–1195. [Google Scholar] [CrossRef]
- Öcal, O.; Kupčinskas, J.; Morkunas, E.; Amthauer, H.; Schütte, K.; Malfertheiner, P.; Klümpen, H.J.; Sengel, C.; Benckert, J.; Seidensticker, R.; et al. Prognostic value of baseline interleukin 6 levels in liver decompensation and survival in HCC patients undergoing radioembolization. EJNMMI Res. 2021, 11, 51. [Google Scholar] [CrossRef] [PubMed]
- Öcal, O.; Schütte, K.; Kupčinskas, J.; Morkunas, E.; Jurkeviciute, G.; de Toni, E.N.; Ben Khaled, N.; Berg, T.; Malfertheiner, P.; Klümpen, H.J.; et al. Baseline Interleukin-6 and -8 predict response and survival in patients with advanced hepatocellular carcinoma treated with sorafenib monotherapy: An exploratory post hoc analysis of the SORAMIC trial. J. Cancer Res. Clin. Oncol. 2022, 148, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Galun, E. Liver inflammation and cancer: The role of tissue microenvironment in generating the tumor-promoting niche (TPN) in the development of hepatocellular carcinoma. Hepatology 2016, 63, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Ge, W.; Zhou, J.; Gao, B.; Qian, X.; Wang, W. The Role of Tumor Associated Macrophages in Hepatocellular Carcinoma. J. Cancer 2021, 12, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Saviano, A.; Roehlen, N.; Virzì, A.; Roca Suarez, A.A.; Hoshida, Y.; Lupberger, J.; Baumert, T.F. Stromal and Immune Drivers of Hepatocarcinogenesis; Hoshida, Y., Ed.; Springer: Cham, Switzerland, 2019; pp. 317–331. [Google Scholar]
- Ge, Z.; Ding, S. The Crosstalk Between Tumor-Associated Macrophages (TAMs) and Tumor Cells and the Corresponding Targeted Therapy. Front. Oncol. 2020, 10, 590941. [Google Scholar] [CrossRef] [PubMed]
- Behary, J.; Raposo, A.E.; Amorim, N.M.L.; Zheng, H.; Gong, L.; McGovern, E.; Chen, J.; Liu, K.; Beretov, J.; Theocharous, C.; et al. Defining the temporal evolution of gut dysbiosis and inflammatory responses leading to hepatocellular carcinoma in Mdr2 −/− mouse model. BMC Microbiol. 2021, 21, 113. [Google Scholar] [CrossRef] [PubMed]
- Compare, D.; Coccoli, P.; Rocco, A.; Nardone, O.M.; De Maria, S.; Cartenì, M. Nardone G. Gut-liver axis: The impact of gut microbiota on non alcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 471–476. [Google Scholar] [CrossRef]
- Miao, E.A.; Andersen-Nissen, E.; Warren, S.E.; Aderem, A. TLR5 and Ipaf: Dual sensors of bacterial flagellin in the innate immune system. Semin. Immunopathol. 2007, 29, 275–288. [Google Scholar] [CrossRef]
- Ni, J.; Huang, R.; Zhou, H.; Xu, X.; Li, Y.; Cao, P.; Zhong, K.; Ge, M.; Chen, X.; Hou, B.; et al. Analysis of the Relationship Between the Degree of Dysbiosis in Gut Microbiota and Prognosis at Different Stages of Primary Hepatocellular Carcinoma. Front. Microbiol. 2019, 10, 1458. [Google Scholar] [CrossRef]
- Zhou, A.; Tang, L.; Zeng, S.; Lei, Y.; Yang, S.; Tang, B. Gut microbiota: A new piece in understanding hepatocarcinogenesis. Cancer Lett. 2020, 474, 15–22. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, J.-X.; Wang, H.; Wang, G.-L.; Hu, Q.-G.; Zheng, Q.-C. Hepatocellular carcinoma and macrophage interaction induced tumor immunosuppression via Treg requires TLR4 signaling. World J. Gastroenterol. 2012, 18, 2938–2947. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.W. Tumour-educated macrophages promote tumour progression and metastasis. Nat. Rev. Cancer Engl. 2004, 4, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.S.; Lee, F.Y.; Lee, S.D.; Tsai, Y.T.; Lin, H.C.; Lu, R.H.; Hsu, W.C.; Huang, C.C.; Wang, S.S.; Lo, K.J. Endotoxemia in patients with chronic liver diseases: Relationship to severity of liver diseases, presence of esophageal varices, and hyperdynamic circulation. J. Hepatol. 1995, 22, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Gajda, A.M.; Storch, J. Enterocyte fatty acid-binding proteins (FABPs): Different functions of liver and intestinal FABPs in the intestine. Prostaglandins Leukot Essent Fat. Acids 2015, 93, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Pelsers, M.M.A.L.; Namiot, Z.; Kisielewski, W.; Namiot, A.; Januszkiewicz, M.; Hermens, W.T.; Glatz, J.F.C. Intestinal-type and liver-type fatty acid-binding protein in the intestine. Tissue distribution and clinical utility. Clin. Biochem. 2003, 36, 529–535. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Jiang, X. Diagnostic Value of Intestinal Fatty-Acid-Binding Protein in Necrotizing Enterocolitis: A Systematic Review and Meta-Analysis. Indian J. Pediatr. 2016, 83, 1410–1419. [Google Scholar] [CrossRef]
- Riva, A.; Gray, E.H.; Azarian, S.; Zamalloa, A.; McPhail, M.J.W.; Vincent, R.P.; Williams, R.; Chokshi, S.; Patel, V.C.; Edwards, L.A. Faecal cytokine profiling as a marker of intestinal inflammation in acutely decompensated cirrhosis. JHEP Rep. Innov. Hepatol. 2020, 2, 100151. [Google Scholar] [CrossRef]
- Gedgaudas, R.; Bajaj, J.S.; Skieceviciene, J.; Varkalaite, G.; Jurkeviciute, G.; Gelman, S.; Valantiene, I.; Zykus, R.; Pranculis, A.; Bang, C.; et al. Circulating microbiome in patients with portal hypertension. Gut Microbes 2022, 14, 2029674. [Google Scholar] [CrossRef]
- Triantos, C.; Kalafateli, M.; Assimakopoulos, S.F.; Karaivazoglou, K.; Mantaka, A.; Aggeletopoulou, I.; Spantidea, P.I.; Tsiaoussis, G.; Rodi, M.; Kranidioti, H. Endotoxin Translocation and Gut Barrier Dysfunction Are Related to Variceal Bleeding in Patients with Liver Cirrhosis. Front Med. 2022, 9, 836306. [Google Scholar] [CrossRef]
- Heymann, F.; Tacke, F. Immunology in the liver—From homeostasis to disease. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 88–110. [Google Scholar] [CrossRef]
- O’Garra, A.; Barrat, F.J.; Castro, A.G.; Vicari, A.; Hawrylowicz, C. Strategies for use of IL-10 or its antagonists in human disease. Immunol. Rev. 2008, 223, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Wills-Karp, M.; Nathan, A.; Page, K.; Karp, C.L. New insights into innate immune mechanisms underlying allergenicity. Mucosal. Immunol. 2010, 3, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Rajasingh, J.; Bord, E.; Luedemann, C.; Asai, J.; Hamada, H.; Thorne, T.; Qin, G.; Goukassian, D.; Zhu, Y.; Losordo, D.W.; et al. IL-10-induced TNF-alpha mRNA destabilization is mediated via IL-10 suppression of p38 MAP kinase activation and inhibition of HuR expression. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2006, 20, 2112–2114. [Google Scholar] [CrossRef] [PubMed]
- Basyte-Bacevice, V.; Skieceviciene, J.; Valantiene, I.; Sumskiene, J.; Petrenkiene, V.; Kondrackiene, J.; Petrauskas, D.; Lammert, F.; Kupcinskas, J. SERPINA1 and HSD17B13 Gene Variants in Patients with Liver Fibrosis and Cirrhosis. J. Gastrointestin. Liver Dis. 2019, 28, 297–302. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls (n = 50) | HCC Patients (n = 47) | p Value | |
|---|---|---|---|
| Age, mean ± SD | 58.8 ± 4.9 | 61.3 ± 9.3 | 0.101 |
| Gender (male) | 25 (50%) | 39 (83.0%) | <0.001 |
| Liver cirrhosis (yes) | 45 (95.7%) | ||
| HCC etiology | |||
| Hepatitis B | 7 (14.9%) | ||
| Hepatitis C | 21 (44.7%) | ||
| Other (alcohol) | 19 (40.4%) | ||
| BCLC stage | |||
| 0 | 2 (4.3%) | ||
| A | 15 (31.9%) | ||
| B | 17 (36.2%) | ||
| C | 7 (14.9%) | ||
| D | 6 (12.8%) | ||
| Cytokine levels, median (min-max) (pg/mL) | |||
| FABP2 | 1327 (518.5–8388) | 2345 (326.3–4587) | 0.026 |
| IL-10 | 4.89 (0.036–53) * | 9.94 (0.04–564.1) * | <0.001 |
| LPS | 56.38 (4.74–436.4) | 51.95 (12.37–148.8) | 0.263 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morkunas, E.; Vaitkeviciute, E.; Varkalaite, G.; Pilvinis, V.; Skieceviciene, J.; Kupcinskas, J. Diagnostic and Prognostic Value of IL-10, FABP2 and LPS Levels in HCC Patients. Medicina 2023, 59, 2191. https://doi.org/10.3390/medicina59122191
Morkunas E, Vaitkeviciute E, Varkalaite G, Pilvinis V, Skieceviciene J, Kupcinskas J. Diagnostic and Prognostic Value of IL-10, FABP2 and LPS Levels in HCC Patients. Medicina. 2023; 59(12):2191. https://doi.org/10.3390/medicina59122191
Chicago/Turabian StyleMorkunas, Egidijus, Evelina Vaitkeviciute, Greta Varkalaite, Vidas Pilvinis, Jurgita Skieceviciene, and Juozas Kupcinskas. 2023. "Diagnostic and Prognostic Value of IL-10, FABP2 and LPS Levels in HCC Patients" Medicina 59, no. 12: 2191. https://doi.org/10.3390/medicina59122191
APA StyleMorkunas, E., Vaitkeviciute, E., Varkalaite, G., Pilvinis, V., Skieceviciene, J., & Kupcinskas, J. (2023). Diagnostic and Prognostic Value of IL-10, FABP2 and LPS Levels in HCC Patients. Medicina, 59(12), 2191. https://doi.org/10.3390/medicina59122191