
Hand Grip Strength, Osteoporosis, and Quality of Life in Middle-Aged and Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Measurement of HGS
2.4. Assessment of HRQoL
2.5. Definition of Covariates
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Total Participants
3.2. HGS in Participants with or without Osteoporosis
3.3. The Comparison of EQ-5D Index by Subgroup Analysis
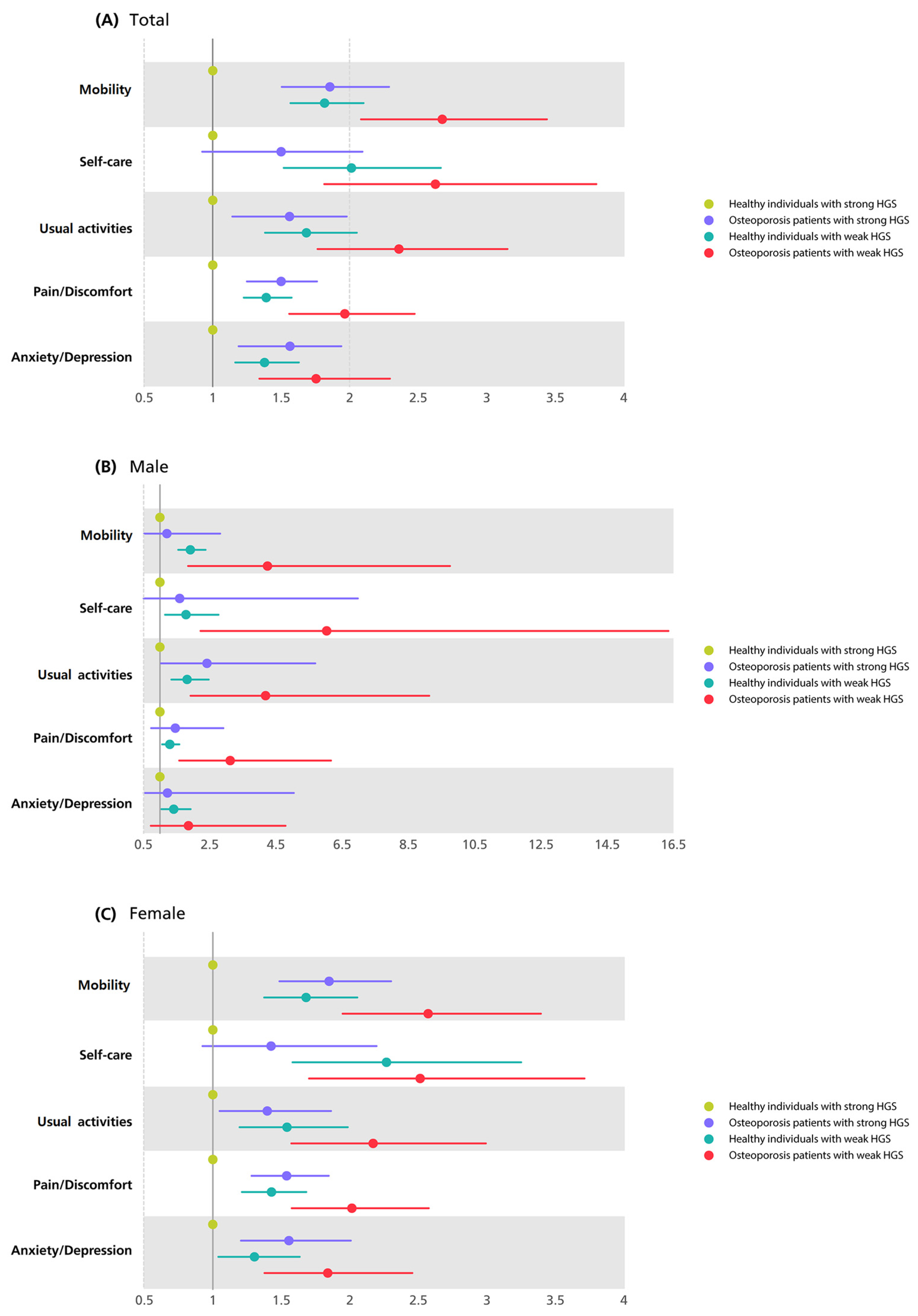
3.4. The Comparison of HRQoL by the Presence of Osteoporosis and HGS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker For Older Adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef]
- Yoo, J.I.; Choi, H.; Ha, Y.C. Mean Hand Grip Strength and Cut-off Value for Sarcopenia in Korean Adults Using KNHANES VI. J. Korean Med. Sci. 2017, 32, 868–872. [Google Scholar] [CrossRef]
- Vancini, R.L.; dos Santos Andrade, M.; Andre Barbosa de Lira, C.; Theodoros Nikolaidis, P.; Knechtle, B. Is It Possible to Age Healthy Performing Ultra-endurance Exercises? Int. J. Sport Stud. Health 2022, 4, e122900. [Google Scholar] [CrossRef]
- Pacholek, M. The Effects of Various Stimuli on Motivation and Physical Fitness of Physically Active and Non-Active Students. Ann. Appl. Sport Sci. 2021, 9, e954. [Google Scholar] [CrossRef]
- Cheung, C.L.; Tan, K.C.; Bow, C.H.; Soong, C.S.; Loong, C.H.; Kung, A.W. Low handgrip strength is a predictor of osteoporotic fractures: Cross-sectional and prospective evidence from the Hong Kong Osteoporosis Study. Age 2012, 34, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Hurst, C.; Demurtas, J.; Firth, J.; Howden, R.; Yang, L.; Tully, M.A.; Koyanagi, A.; Ilie, P.C.; Lopez-Sanchez, G.F.; et al. Handgrip strength and health outcomes: Umbrella review of systematic reviews with meta-analyses of observational studies. J. Sport Health Sci. 2021, 10, 290–295. [Google Scholar] [CrossRef]
- Norman, K.; Stobaus, N.; Gonzalez, M.C.; Schulzke, J.D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Luna-Heredia, E.; Martin-Pena, G.; Ruiz-Galiana, J. Handgrip dynamometry in healthy adults. Clin. Nutr. 2005, 24, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Choi, H.Y.; Ki, M. Association between levels of physical activity and low handgrip strength: Korea National Health and Nutrition Examination Survey 2014-2019. Epidemiol. Health 2022, 44, e2022027. [Google Scholar] [CrossRef]
- Wang, Y.C.; Bohannon, R.W.; Li, X.; Sindhu, B.; Kapellusch, J. Hand-Grip Strength: Normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. J. Orthop. Sports Phys. Ther. 2018, 48, 685–693. [Google Scholar] [CrossRef]
- Hajatnia, B.; Tajeri, B.; Haji-Alizadeh, K. Comparing the Effectiveness of Spirituality Therapy and Acceptance and Commitment Therapy on Sleep Quality, Resilience, and Death Anxiety in the Elderly: Spirituality therapy and ACT in the elderly. Int. J. Body Mind Cult. 2023, 10, 207–215. [Google Scholar] [CrossRef]
- Leboime, A.; Confavreux, C.B.; Mehsen, N.; Paccou, J.; David, C.; Roux, C. Osteoporosis and mortality. Jt. Bone Spine 2010, 77, S107–S112. [Google Scholar] [CrossRef] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Bergland, A. Associations between health-related quality of life, physical function and pain in older women with osteoporosis and vertebral fracture. BMC Geriatr. 2019, 19, 298. [Google Scholar] [CrossRef] [PubMed]
- Alawi, M.; Begum, A.; Harraz, M.; Alawi, H.; Bamagos, S.; Yaghmour, A.; Hafiz, L. Dual-Energy X-Ray Absorptiometry (DEXA) Scan Versus Computed Tomography for Bone Density Assessment. Cureus 2021, 13, e13261. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Jiang, K.; He, M. Association between grip strength and bone mineral density in general US population of NHANES 2013–2014. Arch. Osteoporos. 2020, 15, 47. [Google Scholar] [CrossRef]
- Siris, E.S.; Adler, R.; Bilezikian, J.; Bolognese, M.; Dawson-Hughes, B.; Favus, M.J.; Harris, S.T.; Jan de Beur, S.M.; Khosla, S.; Lane, N.E.; et al. The clinical diagnosis of osteoporosis: A position statement from the National Bone Health Alliance Working Group. Osteoporos. Int. 2014, 25, 1439–1443. [Google Scholar] [CrossRef]
- Musalek, C.; Kirchengast, S. Grip Strength as an Indicator of Health-Related Quality of Life in Old Age-A Pilot Study. Int. J. Environ. Res. Public Health 2017, 14, 1447. [Google Scholar] [CrossRef]
- Yun, I.; Park, Y.S.; Park, E.C.; Jang, S.I. Association between changes in working status and hand-grip strength among Korean middle-aged and older adults: A longitudinal panel study. Sci. Rep. 2022, 12, 12897. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.E.; Martin, H.J.; Dennison, E.M.; Roberts, H.C.; Cooper, C. Is grip strength associated with health-related quality of life? Findings from the Hertfordshire Cohort Study. Age Ageing 2006, 35, 409–415. [Google Scholar] [CrossRef]
- Wang, M.T.; Yao, S.H.; Wong, P.; Trinh, A.; Ebeling, P.R.; Tran, T.; Milat, F.; Mutalima, N. Hip fractures in young adults: A retrospective cross-sectional study of characteristics, injury mechanism, risk factors, complications and follow-up. Arch. Osteoporos. 2017, 12, 46. [Google Scholar] [CrossRef]
- Herath, M.; Cohen, A.; Ebeling, P.R.; Milat, F. Dilemmas in the Management of Osteoporosis in Younger Adults. JBMR Plus 2022, 6, e10594. [Google Scholar] [CrossRef]
- Tsuji, S.; Tsunoda, N.; Yata, H.; Katsukawa, F.; Onishi, S.; Yamazaki, H. Relation Between Grip Strength and Radial Bone Mineral Density in Young Athletes. Arch. Phys. Med. Rehabil. 1995, 76, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Chang, S.Y.; Han, B.D.; Han, K.D.; Park, H.J.; Kang, S. Relation between Handgrip Strength and Quality of Life in Patients with Arthritis in Korea: The Korea National Health and Nutrition Examination Survey, 2015–2018. Medicina 2022, 58, 172. [Google Scholar] [CrossRef]
- Son, D.H.; Yoo, J.W.; Cho, M.R.; Lee, Y.J. Relationship Between Handgrip Strength and Pulmonary Function in Apparently Healthy Older Women. J. Am. Geriatr. Soc. 2018, 66, 1367–1371. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Emrani, Z.; Akbari Sari, A.; Zeraati, H.; Olyaeemanesh, A.; Daroudi, R. Health-related quality of life measured using the EQ-5D-5 L: Population norms for the capital of Iran. Health Qual. Life Outcomes 2020, 18, 108. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Ock, M.; Lee, H.A.; Lee, S.; Han, H.; Jo, M.W.; Park, H. Multimorbidity and health-related quality of life in Koreans aged 50 or older using KNHANES 2013-2014. Health Qual. Life Outcomes 2018, 16, 186. [Google Scholar] [CrossRef]
- Lee, Y.-h.; Choi, J.-s.; Rhee, J.-a.; Ryu, S.-y.; Shin, M.-h.; Kim, J.-h. A Study on the Application of the Korean Valuation Weights for EuroQoL-5 Dimension. J. Korean Soc. Health Educ. Promot. 2009, 26, 1–13. [Google Scholar]
- Kim, C.R.; Jeon, Y.J.; Kim, M.C.; Jeong, T.; Koo, W.R. Reference values for hand grip strength in the South Korean population. PLoS ONE 2018, 13, e0195485. [Google Scholar] [CrossRef]
- Li, Y.Z.; Zhuang, H.F.; Cai, S.Q.; Lin, C.K.; Wang, P.W.; Yan, L.S.; Lin, J.K.; Yu, H.M. Low Grip Strength is a Strong Risk Factor of Osteoporosis in Postmenopausal Women. Orthop. Surg. 2018, 10, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H. Nutrition for Sarcopenia. J. Clin. Med. Res. 2015, 7, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Eleni, A.; Andrea, M.; Johanna, D. Nutrition and Quality of Life in Older Adults. J. Gerontol. 2001, 56, 54–64. [Google Scholar]
- Sakazaki, T.; Koike, T.; Yanagimoto, Y.; Oshida, Y. Association between gait speed and bone strength in community-dwelling postmenopausal Japanese women. Environ. Health Prev. Med. 2012, 17, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation between muscle strength and muscle mass, and their association with walking speed, in community-dwelling elderly Japanese individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef]
- Cooper, R.; Hardy, R.; Aihie Sayer, A.; Ben-Shlomo, Y.; Birnie, K.; Cooper, C.; Craig, L.; Deary, I.J.; Demakakos, P.; Gallacher, J.; et al. Age and gender differences in physical capability levels from mid-life onwards: The harmonisation and meta-analysis of data from eight UK cohort studies. PLoS ONE 2011, 6, e27899. [Google Scholar] [CrossRef]
- Henriksen, M.; Rosager, S.; Aaboe, J.; Graven-Nielsen, T.; Bliddal, H. Experimental knee pain reduces muscle strength. J. Pain 2011, 12, 460–467. [Google Scholar] [CrossRef]
- Friden, C.; Thoors, U.; Glenmark, B.; Kosek, E.; Nordmark, B.; Lundberg, I.E.; Opava, C.H. Higher pain sensitivity and lower muscle strength in postmenonpausal women with early rheumatoid arthritis compared with age-matched healthy women--a pilot study. Disabil. Rehabil. 2013, 35, 1350–1356. [Google Scholar] [CrossRef]
- Zasadzka, E.; Pieczynska, A.; Trzmiel, T.; Kleka, P.; Pawlaczyk, M. Correlation between Handgrip Strength and Depression in Older Adults-A Systematic Review and a Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4823. [Google Scholar] [CrossRef]
- Noh, H.M.; Park, Y.S. Handgrip strength, dynapenia, and mental health in older Koreans. Sci. Rep. 2020, 10, 4004. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. Effect of grip strength on mental health. J. Affect Disord. 2019, 245, 371–376. [Google Scholar] [CrossRef]
- Shaughnessy, K.A.; Hackney, K.J.; Clark, B.C.; Kraemer, W.J.; Terbizan, D.J.; Bailey, R.R.; McGrath, R. A Narrative Review of Handgrip Strength and Cognitive Functioning: Bringing a New Characteristic to Muscle Memory. J. Alzheimer’s Dis. 2020, 73, 1265–1278. [Google Scholar] [CrossRef]
- Fukumori, N.; Yamamoto, Y.; Takegami, M.; Yamazaki, S.; Onishi, Y.; Sekiguchi, M.; Otani, K.; Konno, S.; Kikuchi, S.; Fukuhara, S. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing 2015, 44, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K. Muscle as a secretory organ. Compr. Physiol. 2013, 3, 1337–1362. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Total | Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Strong HGS | Weak HGS | p-Value | Strong HGS | Weak HGS | p-Value | Strong HGS | Weak HGS | p-Value | |
| N | 10,450 | 3516 | 4652 | 1547 | 5798 | 1969 | |||
| Osteoporotic patients | 6.27 (0.24) | 16.15 (0.76) | <0.001 | 0.73(0.14) | 2.54 (0.47) | <0.001 | 11.91 (0.46) | 27.13 (1.26) | <0.001 |
| HGS (kg) | 34 ± 0.1 | 21.82 ± 0.15 | <0.001 | 42.32 ± 0.11 | 28.46 ± 0.12 | <0.001 | 25.48 ± 0.06 | 16.39 ± 0.07 | <0.001 |
| Age | 54.1 ± 0.2 | 64.4 ± 0.29 | <0.001 | 53.68 ± 0.17 | 64.73 ± 0.37 | <0.001 | 54.54 ± 0.17 | 64.13 ± 0.37 | <0.001 |
| Low income | 316 | 34.34 (1.21) | <0.001 | 10.73 (0.56) | 31.46 (1.45) | <0.001 | 15.47 (0.63) | 36.69 (1.53) | <0.001 |
| Education ≥10 years | 72.39 (0.71) | 44.15 (1.24) | <0.001 | 78.26 (0.79) | 52.29 (1.63) | <0.001 | 66.39 (0.84) | 37.48 (1.46) | <0.001 |
| Smoking | <0.001 | <0.001 | 0.304 | ||||||
| Non-smoker | 56.01 (0.53) | 60.59 (0.97) | 20.5 (0.7) | 20.33 (1.18) | 92.3 (0.43) | 93.54 (0.69) | |||
| Ex-smoker | 24.07 (0.48) | 24.18(0.77) | 44.36 (0.87) | 50.43 (1.44) | 3.34 (0.27) | 2.68 (0.4) | |||
| Current-smoker | 19.92 (0.51) | 15.24 (0.82) | 35.14 (0.88) | 29.24 (1.49) | 4.36 (0.35) | 3.78 (0.56) | |||
| Drinking | <0.001 | <0.001 | <0.001 | ||||||
| Non | 23.85 (0.53) | 41.82 (1) | 14.92 (0.62) | 28.28 (1.42) | 32.97 (0.77) | 52.9 (1.37) | |||
| Mild | 66.41 (0.58) | 51.89 (1.05) | 67.61 (0.82) | 59.16 (1.51) | 65.18 (0.78) | 45.94 (1.36) | |||
| Heavy | 9.74 (0.34) | 6.29 (0.51) | 17.47 (0.63) | 12.56 (1.09) | 1.84 (0.23) | 1.16 (0.27) | |||
| Aerobic physical activity | 45.5 (0.7) | 33.03 (1.01) | <0.001 | 47.21 (0.9) | 37.6 (1.61) | <0.001 | 43.79 (0.8) | 29.3 (1.17) | <0.001 |
| Diabetes mellitus | 12.9 (0.4) | 21.43 (0.83) | <0.001 | 15.19 (0.59) | 23.6 (1.27) | <0.001 | 10.47 (0.48) | 19.66 (1.05) | <0.001 |
| Hypertension | 34.7 (0.6) | 48.42 (1.15) | <0.001 | 39.64 (0.83) | 47.66 (1.55) | <0.001 | 29.71 (0.72) | 49.04 (1.49) | <0.001 |
| Hypercholesterolemia | 25.16 (0.51) | 28.68 (0.9) | <0.001 | 22.84 (0.68) | 21.48 (1.22) | 0.317 | 27.54 (0.66) | 34.58 (1.22) | <0.001 |
| BMI (kg/m2) | 24.32 ± 0.04 | 23.68 ± 0.07 | <0.001 | 24.74 ± 0.05 | 23.42 ± 0.09 | <0.001 | 23.89 ± 0.06 | 23.88 ± 0.09 | 0.990 |
| WC (cm) | 83.75 ± 0.12 | 83.22 ± 0.2 | 0.014 | 87.23 ± 0.14 | 85.33 ± 0.27 | <0.001 | 80.2 ± 0.16 | 81.49 ± 0.26 | <0.001 |
| SBP (mmHg) | 120.13 ± 0.22 | 123.82 ± 0.41 | <0.001 | 121.88 ± 0.28 | 123.18 ± 0.52 | 0.019 | 118.34 ± 0.29 | 124.34 ± 0.56 | <0.001 |
| DBP (mmHg) | 77.85 ± 0.13 | 73.96 ± 0.23 | <0.001 | 80.25 ± 0.18 | 74.24 ± 0.33 | <0.001 | 75.4 ± 0.16 | 73.72 ± 0.27 | <0.001 |
| Fasting glucose (mg/dL) | 103.02 ± 0.28 | 106.22 ± 0.55 | <0.001 | 106.25 ± 0.45 | 109.17 ± 0.9 | 0.003 | 99.72 ± 0.34 | 103.81 ± 0.68 | <0.001 |
| Total cholesterol (mg/dL) | 197.56 ± 0.45 | 189.96 ± 0.75 | <0.001 | 195.75 ± 0.66 | 184.1 ± 1.22 | <0.001 | 199.4 ± 0.53 | 194.76 ± 0.98 | <0.001 |
| HDL-C (mg/dL) | 50.39 ± 0.15 | 49.1 ± 0.26 | <0.001 | 46.73 ± 0.19 | 46.58 ± 0.36 | 0.711 | 54.14 ± 0.2 | 51.16 ± 0.37 | <0.001 |
| EQ-5D index | 0.96 ± 0 | 0.9 ± 0 | <0.001 | 0.97 ± 0 | 0.92 ± 0 | <0.001 | 0.95 ± 0 | 0.88 ± 0 | <0.001 |
| N | HGS (kg) | ||||
|---|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 3 c | |||
| Total | Healthy individuals | 12,465 | 32.31 ± 0.12 | 29.88 ± 0.08 | 29.88 ± 0.08 |
| Osteoporotic patients | 1501 | 21.59 ± 0.22 | 30.28 ± 0.17 | 30.25 ± 0.18 | |
| p-value | <0.001 | 0.028 | 0.049 | ||
| Male | Healthy individuals | 6102 | 39.7 ± 0.13 | 38.46 ± 0.11 | 38.46 ± 0.11 |
| Osteoporotic patients | 97 | 34.18 ± 1.19 | 37.56 ± 0.96 | 37.52 ± 0.96 | |
| p-value | <0.001 | 0.355 | 0.336 | ||
| Female | Healthy individuals | 6363 | 23.87 ± 0.09 | 23.11 ± 0.08 | 23.11 ± 0.08 |
| Osteoporotic patients | 1404 | 20.68 ± 0.17 | 22.63 ± 0.16 | 22.62 ± 0.16 | |
| p-value | <0.001 | 0.008 | 0.006 | ||
| N | EQ-5D Index | ||||
|---|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 3 c | |||
| Total | Healthy individuals with strong HGS | 9588 | 0.97 ± 0.00 | 0.95 ± 0.00 | 0.95 ± 0.00 |
| Osteoporotic patients with strong HGS | 862 | 0.90 ± 0.01 | 0.93 ± 0.01 | 0.93 ± 0.01 | |
| Healthy individuals with weak HGS | 2877 | 0.92 ± 0.00 | 0.93 ± 0.00 | 0.93 ± 0.00 | |
| Osteoporotic patients with weak HGS | 639 | 0.83 ± 0.01 | 0.87 ± 0.01 | 0.87 ± 0.01 | |
| p-value | <0.001 | <0.001 | <0.001 | ||
| Male | Healthy individuals with strong HGS | 4602 | 0.97 ± 0.00 | 0.96 ± 0.00 | 0.96 ± 0.00 |
| Osteoporotic patients with strong HGS | 50 | 0.94 ± 0.2 | 0.95 ± 0.01 | 0.95 ± 0.01 | |
| Healthy individuals with weak HGS | 1500 | 0.93 ± 0.00 | 0.94 ± 0.00 | 0.94 ± 0.00 | |
| Osteoporotic patients with weak HGS | 47 | 0.78 ± 0.05 | 0.82 ± 0.05 | 0.82 ± 0.05 | |
| p-value | <0.001 | <0.001 | <0.001 | ||
| Female | Healthy individuals with strong HGS | 4986 | 0.96 ± 0.00 | 0.94 ± 0.00 | 0.94 ± 0.00 |
| Osteoporotic patients with strong HGS | 812 | 0.90 ± 0.01 | 0.92 ± 0.01 | 0.92 ± 0.01 | |
| Healthy individuals with weak HGS | 1377 | 0.90 ± 0.00 | 0.91 ± 0.00 | 0.92 ± 0.00 | |
| Osteoporotic patients with weak HGS | 592 | 0.83 ± 0.01 | 0.87 ± 0.01 | 0.87 ± 0.01 | |
| p-value | <0.001 | <0.001 | <0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.J.; Han, B.; Chang, S.-y.; Kang, S.H.; Lee, D.W.; Kang, S. Hand Grip Strength, Osteoporosis, and Quality of Life in Middle-Aged and Older Adults. Medicina 2023, 59, 2148. https://doi.org/10.3390/medicina59122148
Park HJ, Han B, Chang S-y, Kang SH, Lee DW, Kang S. Hand Grip Strength, Osteoporosis, and Quality of Life in Middle-Aged and Older Adults. Medicina. 2023; 59(12):2148. https://doi.org/10.3390/medicina59122148
Chicago/Turabian StylePark, Hyo Jin, Byoungduck Han, So-youn Chang, Seung Ho Kang, Dae Wook Lee, and Seok Kang. 2023. "Hand Grip Strength, Osteoporosis, and Quality of Life in Middle-Aged and Older Adults" Medicina 59, no. 12: 2148. https://doi.org/10.3390/medicina59122148
APA StylePark, H. J., Han, B., Chang, S.-y., Kang, S. H., Lee, D. W., & Kang, S. (2023). Hand Grip Strength, Osteoporosis, and Quality of Life in Middle-Aged and Older Adults. Medicina, 59(12), 2148. https://doi.org/10.3390/medicina59122148