


Right Axillary Artery Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Postcardiotomy Patients: A Single-Center Experience

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
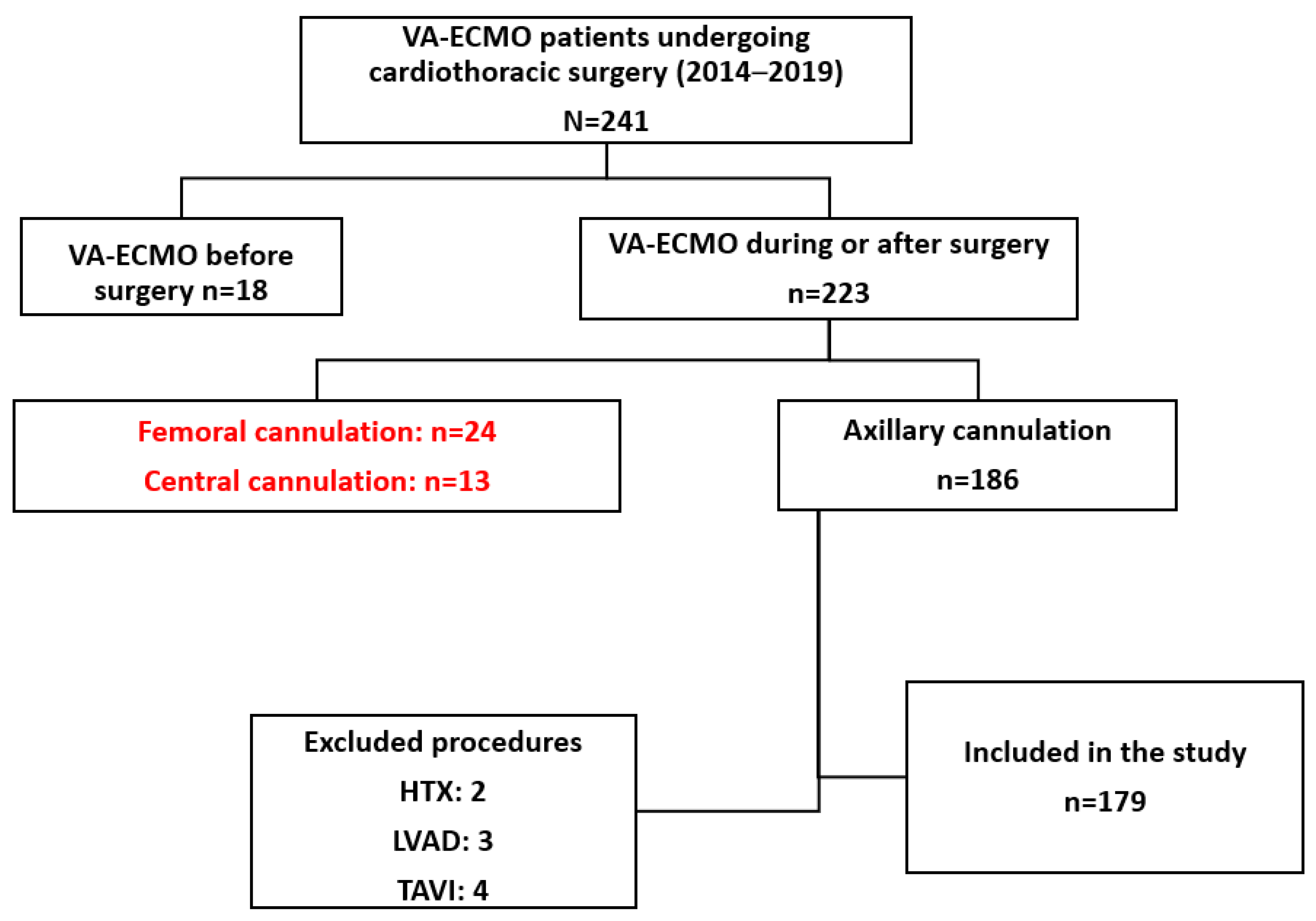
2.1. Patient Selection
2.2. ECMO Implantation
2.3. Management and Weaning Protocol
2.4. VA-ECMO Complications
- Cannulation-related complications, including local bleeding, infection, and limb ischemia at the arterial cannulation site.
- VA-ECMO-related complications, including systemic hemorrhagic complications, VA-ECMO membrane thrombosis, and pulmonary edema.
- Systemic complications: pulmonary infection and sepsis.
2.5. Statistical Analysis
2.6. International Review Board
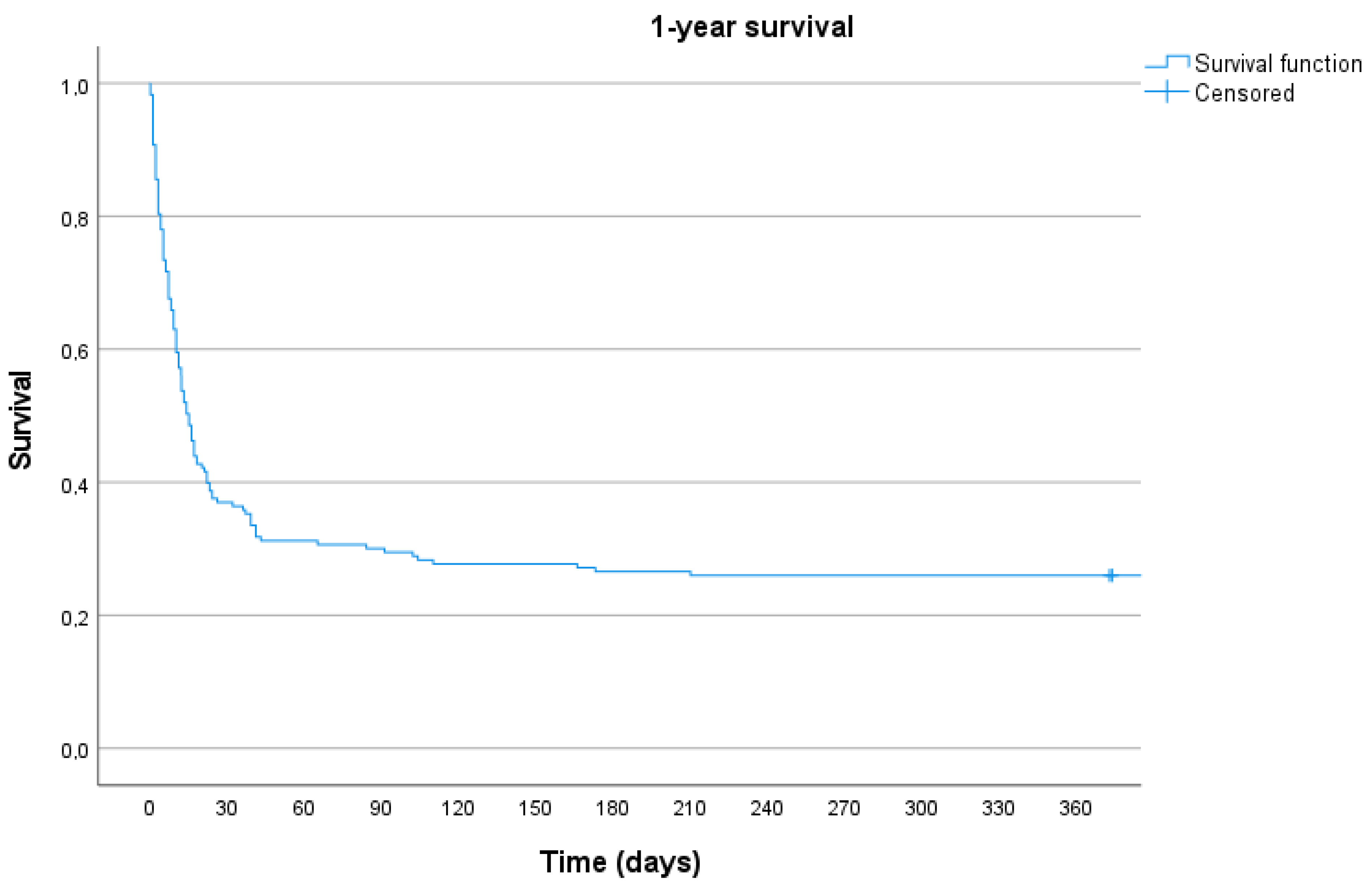
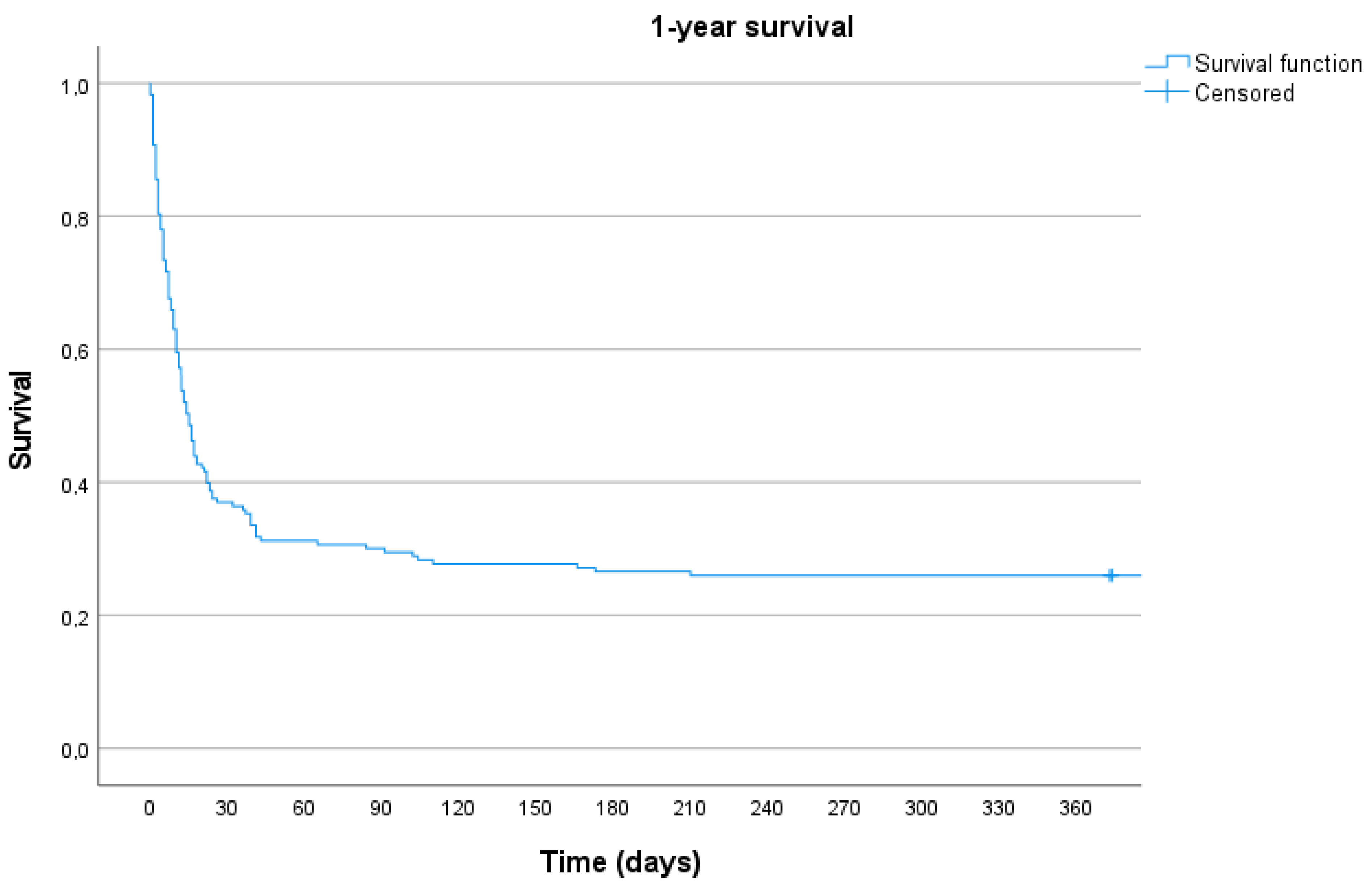
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paul, S.; Leacche, M.; Unic, D.; Couper, G.S.; Macgillivray, T.E.; Agnihotri, A.K.; Cohn, L.H.; Byrne, J.G. Determinants of outcomes for postcardiotomy VAD placement: An 11-year, two-institution study. J. Card. Surg. 2006, 21, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Navia, J.L.; Atik, F.A.; Beyer, E.A.; Ruda Vega, P. Extracorporeal membrane oxygenation with right axillary artery perfusion. Ann. Thorac. Surg. 2005, 79, 2163–5216. [Google Scholar] [CrossRef] [PubMed]
- Madershahian, N.; Weber, C.; Scherner, M.; Langebartels, G.; Slottosch, I.; Wahlers, T. Thrombosis of the aortic root and ascending aorta during extracorporeal membrane oxygenation. Intensive Care Med. 2014, 40, 432–433. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, L.; Flörchinger, B.; Schopka, S.; Schmid, C.; Philipp, A.; Lunz, D.; Müller, T.; Camboni, D. Cardiac decompression on extracorporeal life support: A review and discussion of the literature. ASAIO J. 2013, 59, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Javidfar, J.; Brodie, D.; Costa, J.; Miller, J.; Jurrado, J.; LaVelle, M.; Newmark, A.; Takayama, H.; Sonett, J.R.; Bacchetta, M. Subclavian artery cannulation for venoarterial extracorporeal membrane oxygenation. ASAIO J. 2012, 58, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; Mateo-Sidron, J.A.R.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Ariyaratnam, P.; McLean, L.A.; Cale, A.R.J.; Loubani, M. Extra-corporeal membrane oxygenation for the post-cardiotomy patient. Heart Fail. Rev. 2014, 19, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Meuwese, C.L.; Ramjankhan, F.Z.; Braithwaite, S.A.; De Jonge, N.; De Jong, M.; Buijsrogge, M.P.; Janssen, J.G.D.; Klöpping, C.; Kirkels, J.H.; Donker, D.W. Extracorporeal life support in cardiogenic shock: Indications and management in current practice. Neth. Heart J. 2018, 26, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Khorsandi, M.; Dougherty, S.; Bouamra, O.; Pai, V.; Curry, P.; Tsui, S.; Clark, S.; Westaby, S.; Al-Attar, N.; Zamvar, V. Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2017, 12, 55. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.; Nemeth, A.; Sandoval Boburg, R.; Vöhringer, L.; Lausberg, H.F.; Acharya, M.; Schlensak, C.; Popov, A.F. Long-Term Follow-Up of Survivors of Extracorporeal Life Support Therapy for Cardiogenic Shock: Are They Really Survivors? Medicina 2022, 58, 427. [Google Scholar] [CrossRef] [PubMed]
- Hysi, I.; Renaut, C.; Fabre, O. Direct axillary artery cannulation in cardiac surgery: Clinical outcomes. Asian Cardiovasc. Thorac. Ann. 2017, 25, 502–503. [Google Scholar] [CrossRef]
- Pisani, A.; Braham, W.; Brega, C.; Lajmi, M.; Provenchere, S.; Danial, P.; Alkhoder, S.; Para, M.; Ghodbane, W.; Nataf, P. Right axillary artery cannulation for venoarterial extracorporeal membrane oxygenation: A retrospective single centre observational study. Eur. J. Cardiothorac. Surg. 2021, 59, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Ohira, S.; Malekan, R.; Goldberg, J.B.; Lansman, S.L.; Spielvogel, D.; Kai, M. Axillary artery cannulation for veno-arterial extracorporeal membrane oxygenation support in cardiogenic shock. JTCVS Tech. 2021, 5, 62–71. [Google Scholar] [CrossRef]
- Wang, L.; Yang, F.; Zhang, S.; Li, C.; Du, Z.; Rycus, P.; Tonna, J.E.; Alexander, P.; Lorusso, R.; Fan, E.; et al. Percutaneous versus surgical cannulation for femoro-femoral VA-ECMO in patients with cardiogenic shock: Results from the Extracorporeal Life Support Organization Registry. J. Heart Lung Transplant. 2022, 41, 470–481. [Google Scholar] [CrossRef]
- Sanfilippo, F.; Currò, J.M.; La Via, L.; Dezio, V.; Martucci, G.; Brancati, S.; Murabito, P.; Pappalardo, F.; Astuto, M. Use of nafamostat mesilate for anticoagulation during extracorporeal membrane oxygenation: A systematic review. Artif. Organs 2022, 46, 2371–2381. [Google Scholar] [CrossRef] [PubMed]
- Seelhammer, T.G.; Bohman, J.K.; Schulte, P.J.; Hanson, A.C.; Aganga, D.O. Comparison of Bivalirudin Versus Heparin for Maintenance Systemic Anticoagulation During Adult and Pediatric Extracorporeal Membrane Oxygenation. Crit. Care Med. 2021, 49, 1481–1492. [Google Scholar] [CrossRef] [PubMed]
- Radakovic, D.; Hamouda, K.; Penov, K.; Bening, C.; Sayed, S.; Gietzen, C.; Leyh, R.G.; Aleksic, I. Central Versus Peripheral Arterial Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Post-Cardiotomy Patients. ASAIO J. 2021, 67, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Smood, B.; Fowler, C.; Rao, S.D.; Genuardi, M.V.; Sperry, A.E.; Goel, N.; Acker, A.M.; Olia, S.E.; Iyengar, A.; Han, J.J.; et al. Subacute groin complications related to ECMO cannulation are associated with longer hospitalizations. J. Artif. Organs 2022, 26, 119–126. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| N | Percentage | |
|---|---|---|
| Sex | ||
| Male | 119 | 66.48% |
| Female | 60 | 33.52% |
| Age (y) | 67.05 ± 10.9 | |
| BMI (kg/m2) | 33.18 ± 48.61 | |
| Indication | ||
| CABG | 72 | 40.22% |
| Valvular Pathology | 52 | 29.05% |
| Combined CABG and Valvular Pathology | 28 | 15.64% |
| Thoracic Aorta | 20 | 11.17% |
| Other | 7 | 3.91% |
| Chronic Atrial Fibrillation | 33 | 17.74% |
| Hypertension | 121 | 67.60% |
| Diabetes | 79 | 44.13% |
| Pulmonary Hypertension | 85 | 47.49% |
| Dyslipidemia | 43 | 24.02% |
| LVEF (%) | ||
| >50 | 74 | 41.34% |
| 50–31 | 48 | 26.82% |
| 30–21 | 23 | 12.85% |
| <20 | 22 | 12.29% |
| NYHA III-IV | 137 | 76.54% |
| Acute MI | 54 | 30.17% |
| CPR | 69 | 38.55% |
| Intubated Admission | 33 | 18.44% |
| Type of Surgery | ||
| Elective | 74 | 41.34% |
| Urgent | 37 | 20.67% |
| Emergency | 64 | 35.75% |
| CPB time (min) | 196.08 | |
| Cross Clamp Time (min) | 101.50 |
| Number | Percentage | |
|---|---|---|
| ECMO Duration (d) | 8.37 ± 5.13 | |
| Implantation during CPR | 32 | 17.88% |
| Successful ECMO weaning | 87 | 48.60% |
| Hospital stay (d) | 23.48 ±22.66 | |
| ICU stay (d) | 18.80 ± 15.86 | |
| Discharged | 62 | 36.31% |
| Mortality during ECMO | 92 | 51.40% |
| Mortality after ECMO | 44 | 24.58% |
| Number | Percentage | |
|---|---|---|
| Access site bleeding | 20 | 11.1% |
| Cerebral bleeding | 7 | 3.91% |
| Ischemia | 29 | 16.20% |
| Upper limb | 12 | 6.70% |
| Lower limb | 13 | 7.26% |
| Both | 4 | 2.23% |
| Compartment syndrome | 11 | 6.15% |
| Upper limb | 6 | 3.35% |
| Lower limb | 4 | 2.23% |
| Both | 1 | 0.56% |
| Cannulation site infection | 5 | 4.47% |
| Stroke | 11 | 6.15% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radwan, M.; Baghdadi, K.; Popov, A.F.; Sandoval Boburg, R.; Risteski, P.; Schlensak, C.; Walter, T.; Berger, R.; Emrich, F. Right Axillary Artery Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Postcardiotomy Patients: A Single-Center Experience. Medicina 2023, 59, 2040. https://doi.org/10.3390/medicina59112040
Radwan M, Baghdadi K, Popov AF, Sandoval Boburg R, Risteski P, Schlensak C, Walter T, Berger R, Emrich F. Right Axillary Artery Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Postcardiotomy Patients: A Single-Center Experience. Medicina. 2023; 59(11):2040. https://doi.org/10.3390/medicina59112040
Chicago/Turabian StyleRadwan, Medhat, Karim Baghdadi, Aron Frederik Popov, Rodrigo Sandoval Boburg, Petar Risteski, Christian Schlensak, Thomas Walter, Rafal Berger, and Fabian Emrich. 2023. "Right Axillary Artery Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Postcardiotomy Patients: A Single-Center Experience" Medicina 59, no. 11: 2040. https://doi.org/10.3390/medicina59112040
APA StyleRadwan, M., Baghdadi, K., Popov, A. F., Sandoval Boburg, R., Risteski, P., Schlensak, C., Walter, T., Berger, R., & Emrich, F. (2023). Right Axillary Artery Cannulation for Veno-Arterial Extracorporeal Membrane Oxygenation in Postcardiotomy Patients: A Single-Center Experience. Medicina, 59(11), 2040. https://doi.org/10.3390/medicina59112040