

Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Statement
2.2. Semen Analysis
2.3. Study Groups
2.4. Statistical Analysis
3. Results
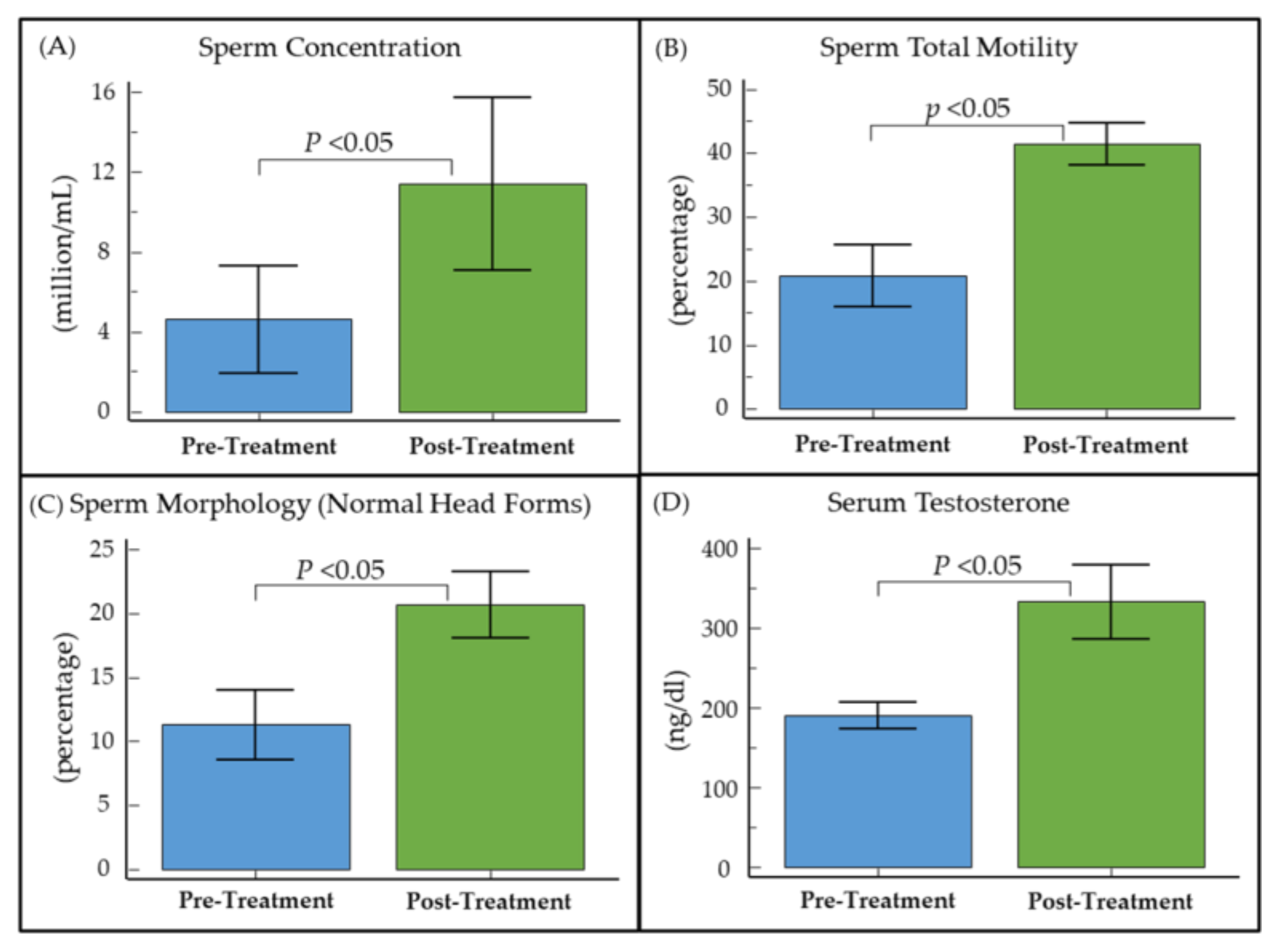
3.1. Effect of CC on Semen Parameters and Testosterone Levels in Oligozoospermic Obese Men
3.2. Effect of CC on Semen Parameters and Testosterone Levels in Oligozoospermic Hypogonadal Obese Men
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef]
- Levine, H.; Jørgensen, N.; Martino-Andrade, A.; Mendiola, J.; Weksler-Derri, D.; Mindlis, I.; Pinotti, R.; Swan, S.H. Temporal trends in sperm count: A systematic review and meta-regression analysis. Hum. Reprod. Update 2017, 23, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Dixon, T.; Waters, A.-M.; Dixon, T. A Growing Problem: Trends and Patterns in Overweight and Obesity among Adults in Australia, 1980 to 2001; Australian Institute of Health and Welfare: Canberra, Australia, 2003. [Google Scholar]
- Sallmén, M.; Sandler, D.P.; Hoppin, J.A.; Blair, A.; Baird, D.D. Reduced fertility among overweight and obese men. Epidemiology 2006, 17, 520–523. [Google Scholar] [CrossRef] [PubMed]
- Sermondade, N.; Faure, C.; Fezeu, L.; Lévy, R.; Czernichow, S. Obesity and increased risk for oligozoospermia and azoospermia. Arch. Intern. Med. 2012, 172, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Katib, A. Mechanisms linking obesity to male infertility. Cent. Eur. J. Urol. 2015, 68, 79–85. [Google Scholar] [CrossRef]
- Leisegang, K.; Sengupta, P.; Agarwal, A.; Henkel, R. Obesity and male infertility: Mechanisms and management. Andrologia 2021, 53, e13617. [Google Scholar] [CrossRef]
- Fernandez, C.J.; Chacko, E.C.; Pappachan, J.M. Male Obesity-related Secondary Hypogonadism—Pathophysiology, Clinical Implications and Management. Eur. Endocrinol. 2019, 15, 83–90. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Trost, L.W.; Brannigan, R.E.; Kurtz, E.G.; Redmon, J.B.; Chiles, K.A.; Lightner, D.J.; Miner, M.M.; Murad, M.H.; Nelson, C.J.; et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J. Urol. 2018, 200, 423–432. [Google Scholar] [CrossRef]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef]
- MacIndoe, J.H.; Perry, P.J.; Yates, W.R.; Holman, T.L.; Ellingrod, V.L.; Scott, S.D. Testosterone suppression of the HPT axis. J. Investig. Med. 1997, 45, 441–447. [Google Scholar]
- Wheeler, K.M.; Sharma, D.; Kavoussi, P.K.; Smith, R.P.; Costabile, R. Clomiphene Citrate for the Treatment of Hypogonadism. Sex. Med. Rev. 2019, 7, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.H.; Horie, N.C.; Chiang, L.A.P.; Caramelli, B.; Matheus, M.G.; Campos, A.H.; Marti, L.C.; Rocha, F.A.; Mancini, M.C.; Costa, E.M.F.; et al. Effects of clomiphene citrate on male obesity-associated hypogonadism: A randomized, double-blind, placebo-controlled study. Int. J. Obes. (Lond.) 2018, 42, 953–963. [Google Scholar] [CrossRef]
- Thomas, J.; Suarez Arbelaez, M.C.; Narasimman, M.; Weber, A.R.; Blachman-Braun, R.; White, J.T.; Ledesma, B.; Ghomeshi, A.; Jara-Palacios, M.A.; Ramasamy, R. Efficacy of Clomiphene Citrate Versus Enclomiphene Citrate for Male Infertility Treatment: A Retrospective Study. Cureus 2023, 15, e41476. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Wu, L.; Zhou, Y.; Zhang, H.; Xiong, C.; Peng, Z.; Bao, W.; Meng, T.; Liu, Y. Association between BMI and semen quality: An observational study of 3966 sperm donors. Hum. Reprod. 2019, 34, 155–162. [Google Scholar] [CrossRef]
- Sekhavat, L.; Moein, M.R. The effect of male body mass index on sperm parameters. Aging Male 2010, 13, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Palmer, N.O.; Bakos, H.W.; Fullston, T.; Lane, M. Impact of obesity on male fertility, sperm function and molecular composition. Spermatogenesis 2012, 2, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, M.; Thomas, M.C.; Panagiotopoulos, S.; Sharpe, K.; Macisaac, R.J.; Clarke, S.; Zajac, J.D.; Jerums, G. Low testosterone levels are common and associated with insulin resistance in men with diabetes. J. Clin. Endocrinol. Metab. 2008, 93, 1834–1840. [Google Scholar] [CrossRef]
- Stárka, L.; Hill, M.; Pospíšilová, H.; Dušková, M. Estradiol, obesity and hypogonadism. Physiol. Res. 2020, 69, S273–S278. [Google Scholar] [CrossRef]
- Khanna, D.; Khanna, S.; Khanna, P.; Kahar, P.; Patel, B.M. Obesity: A Chronic Low-Grade Inflammation and Its Markers. Cureus 2022, 14, e22711. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.L.; Mantzoros, C.S. Leptin and the hypothalamic-pituitary regulation of the gonadotropin-gonadal axis. Pituitary 2001, 4, 87–92. [Google Scholar] [CrossRef]
- Janssen, J. New Insights into the Role of Insulin and Hypothalamic-Pituitary-Adrenal (HPA) Axis in the Metabolic Syndrome. Int. J. Mol. Sci. 2022, 23, 8178. [Google Scholar] [CrossRef]
- Sharma, D.; Zillioux, J.; Khourdaji, I.; Reines, K.; Wheeler, K.; Costabile, R.; Kavoussi, P.; Smith, R. Improvements in semen parameters in men treated with clomiphene citrate—A retrospective analysis. Andrologia 2019, 51, e13257. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Sigalos, J.T.; Osadchiy, V.; Santamaria, A.; Zheng, M.H.; Modiri, N.; Regets, K.V.; Mills, J.N.; Eleswarapu, S.V. Temporal Changes of Clomiphene on Testosterone Levels and Semen Parameters in Subfertile Men. World J. Men’s Health 2023, 41, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Huijben, M.; Huijsmans, R.L.N.; Lock, M.; de Kemp, V.F.; de Kort, L.M.O.; van Breda, J. Clomiphene citrate for male infertility: A systematic review and meta-analysis. Andrology 2023, 11, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Bendre, S.V.; Murray, P.J.; Basaria, S. Clomiphene Citrate Effectively Increases Testosterone in Obese, Young, Hypogonadal Men. Reprod. Syst. Sex. Disord. 2015, 4, 155. [Google Scholar] [CrossRef] [PubMed]
- Huijben, M.; Lock, M.; de Kemp, V.F.; Beck, J.J.H.; De Kort, L.M.O.; van Breda, H.M.K. Clomiphene citrate: A potential alternative for testosterone therapy in hypogonadal males. Endocrinol. Diabetes Metab. 2023, 6, e416. [Google Scholar] [CrossRef] [PubMed]
- Herzog, B.J.; Nguyen, H.M.T.; Soubra, A.; Hellstrom, W.J. Clomiphene citrate for male hypogonadism and infertility: An updated review. Androg. Clin. Res. Ther. 2020, 1, 62–69. [Google Scholar] [CrossRef]


{kind=link}
| Patient Characteristics | |
|---|---|
| Age (years) | |
| Obese group (n = 31) | 36.9 ± 1.5 |
| Non-obese group (n = 22) | 34.0 ± 1.2 |
| Body Mass Index (kg/m2) | |
| Obese group (n = 31) | 37.3 ± 1.2 |
| Non-obese group (n = 22) | 26.3 ± 0.6 |
| Total Testosterone (ng/dL) | |
| Obese group (n = 26) | 304.9 ± 31.6 |
| Non-obese group (n = 22) | 369.6 ± 42.9 |
| Race | |
| White | 30 (56.6%) |
| African American | 19 (35.8%) |
| Hispanic | 4 (7.5%) |
| Semen parameters | |
| Semen volume (mL) | 2.9 ± 0.2 |
| pH | 7.6 ± 0.1 |
| Sperm concentration (×106/mL) | 3.7 ± 0.8 |
| Total sperm count (×106) | 11.9 ± 4.2 |
| Total motility (%) | 30.3 ± 2.8 |
| Sperm morphology (normal heads) (%) | 14.8 ± 1.4 |
| White blood cells (WBC) (×106/mL) | 0.9 ± 0.2 |
| Parameters | Pre-Treatment | Post-Treatment | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Sperm Concentration (×106/mL) | 4.5 ± 6.8 | 11.4 ± 15.5 | <0.05 |
| Total Sperm Count (×106) | 13.8 ± 38.5 | 31.5 ± 43.9 | <0.05 |
| Motility (%) | 31.5 ± 21.5 | 42.6 ± 14.7 | <0.05 |
| Normal Head Forms (%) | 16.1 ± 10.9 | 20.3 ± 9.0 | 0.07 |
| Testosterone (ng/dL) | 349.8 ± 174.5 | 404.9 ± 157.9 | 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panner Selvam, M.K.; Baskaran, S.; Tannenbaum, J.; Greenberg, J.; Shalaby, H.Y.; Hellstrom, W.J.G.; Sikka, S.C. Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study. Medicina 2023, 59, 1902. https://doi.org/10.3390/medicina59111902
Panner Selvam MK, Baskaran S, Tannenbaum J, Greenberg J, Shalaby HY, Hellstrom WJG, Sikka SC. Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study. Medicina. 2023; 59(11):1902. https://doi.org/10.3390/medicina59111902
Chicago/Turabian StylePanner Selvam, Manesh Kumar, Saradha Baskaran, Jacob Tannenbaum, Jacob Greenberg, Hosam Y. Shalaby, Wayne J. G. Hellstrom, and Suresh C. Sikka. 2023. "Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study" Medicina 59, no. 11: 1902. https://doi.org/10.3390/medicina59111902
APA StylePanner Selvam, M. K., Baskaran, S., Tannenbaum, J., Greenberg, J., Shalaby, H. Y., Hellstrom, W. J. G., & Sikka, S. C. (2023). Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study. Medicina, 59(11), 1902. https://doi.org/10.3390/medicina59111902