
Multipronged Programmatic Strategy for Preventing Secondary Fracture and Facilitating Functional Recovery in Older Patients after Hip Fractures: Our Experience in Taipei Municipal Wanfang Hospital

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
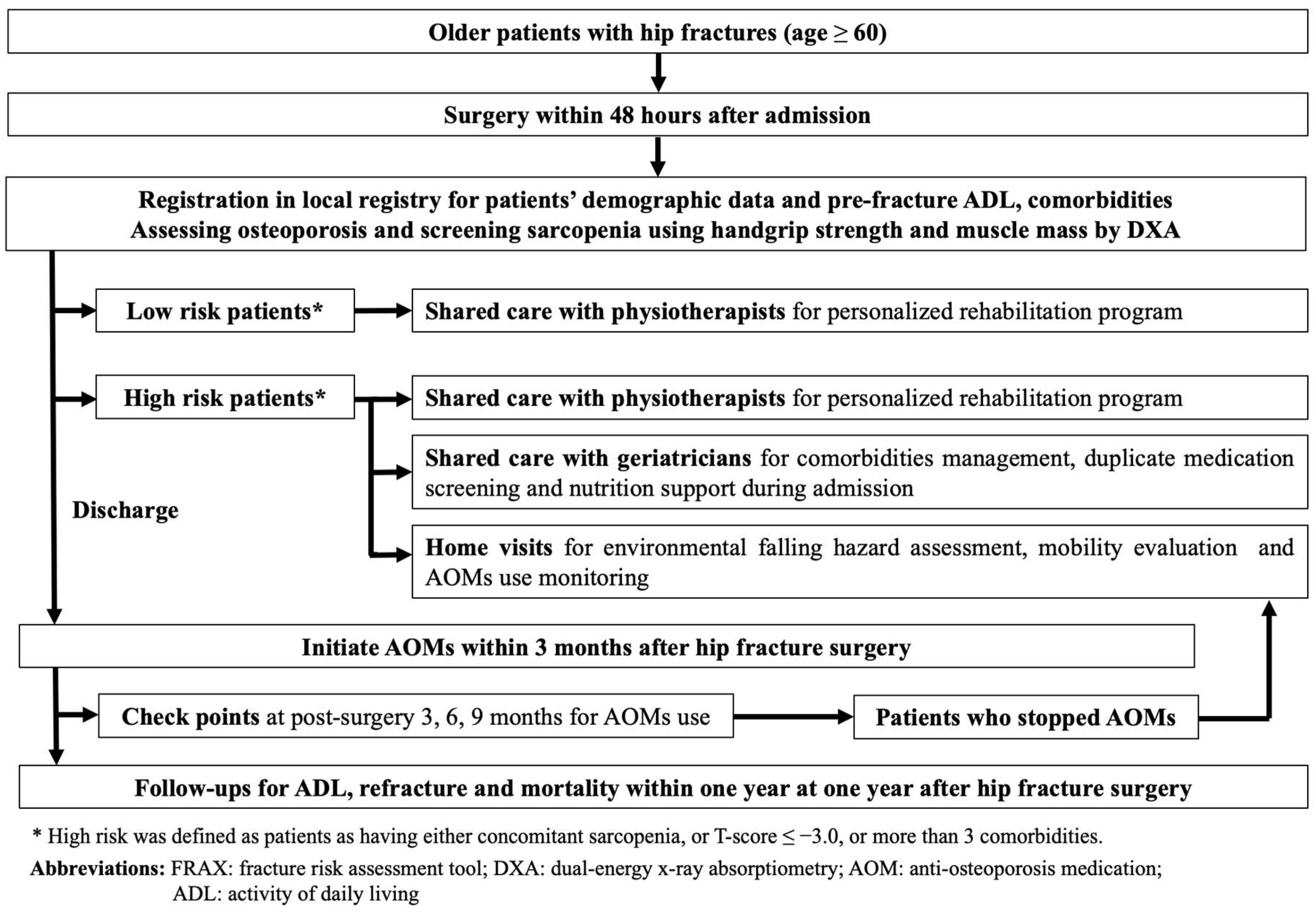
2.1. Program Description
2.2. Data Collection
2.3. Key Performance Indicators for FLS
2.4. Environmental Evaluation in Home Visits
2.5. Definition of Sarcopenia
2.6. Instruments for Functional Outcomes
2.7. Statistics
3. Results
3.1. Demographic Data
3.2. KPIs for Quality Control in FLS
3.3. Findings on Home Visits and Changes Thereafter
3.4. Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lesic, A.; Jarebinski, M.; Pekmezovic, T.; Bumbasirevic, M.; Spasovski, D.; Atkinson, H.D. Epidemiology of Hip Fractures in Belgrade, Serbia Montenegro, 1990–2000. Arch. Orthop. Trauma Surg. 2007, 127, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J., 3rd. Epidemiology of Hip Fractures: Implications of the Exponential Increase with Age. Bone 1996, 18, S121–S125. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Bin Ang, S.; Chadha, M.; Chow, E.S.-L.; Chung, Y.-S.; Hew, F.L.; Jaisamrarn, U.; Ng, H.; Takeuchi, Y.; Wu, C.-H.; et al. An updated hip fracture projection in Asia: The Asian Federation of Osteoporosis Societies study. Osteoporos. Sarcopenia 2018, 4, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-C.; Ho, P.-S.; Lin, H.-T.; Ho, M.-L.; Huang, H.-T.; Chang, J.-K. One-Year Readmission Risk and Mortality after Hip Fracture Surgery: A National Population-Based Study in Taiwan. Aging Dis. 2017, 8, 402–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-B.; Lin, C.-F.J.; Liang, W.-M.; Cheng, C.-F.; Chang, Y.-J.; Wu, H.-C.; Wu, T.-N.; Leu, T.-H. Excess mortality after hip fracture among the elderly in Taiwan: A nationwide population-based cohort study. Bone 2013, 56, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Hu, H.; Lin, S.; Chie, W.-C.; Yang, R.-S.; Liaw, C. Trends in hip fracture rates in Taiwan: A nationwide study from 1996 to 2010. Osteoporos. Int. 2016, 28, 653–665. [Google Scholar] [CrossRef]
- Abrahamsen, B.; van Staa, T.; Ariely, R.; Olson, M.; Cooper, C. Excess mortality following hip fracture: A systematic epidemiological review. Osteoporos. Int. 2009, 20, 1633–1650. [Google Scholar] [CrossRef]
- Chen, Y.-P.; Kuo, Y.-J.; Liu, C.-H.; Chien, P.-C.; Chang, W.-C.; Lin, C.-Y.; Pakpour, A.H. Prognostic factors for 1-year functional outcome, quality of life, care demands, and mortality after surgery in Taiwanese geriatric patients with a hip fracture: A prospective cohort study. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211028360. [Google Scholar] [CrossRef]
- Lee, S.-H.; Chen, I.; Li, Y.; Chiang, C.F.; Chang, C.; Hsieh, P. Incidence of Second Hip Fractures and Associated Mortality in Taiwan: A Nationwide Population-Based Study of 95,484 Patients During 2006–2010. Acta Orthop. Traumatol. Turc. 2016, 50, 437–442. [Google Scholar] [CrossRef] [Green Version]
- Åkesson, K.; Marsh, D.; Mitchell, P.J.; McLellan, A.R.; Stenmark, J.; Pierroz, D.D.; Kyer, C.; Cooper, C. Capture the Fracture: A Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos. Int. 2013, 24, 2135–2152. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.-H.; Tu, S.-T.; Chang, Y.-F.; Chan, D.-C.; Chien, J.-T.; Lin, C.-H.; Singh, S.; Dasari, M.; Chen, J.-F.; Tsai, K.-S. Fracture liaison services improve outcomes of patients with osteoporosis-related fractures: A systematic literature review and meta-analysis. Bone 2018, 111, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Chien, L.-N.; Li, Y.-F.; Yang, R.-S.; Yang, T.-H.; Chen, Y.-H.; Huang, W.-J.; Tsai, H.-Y.; Li, C.-Y.; Chan, D.-C. Real-world cost-effectiveness analysis of the fracture liaison services model of care for hip fracture in Taiwan. J. Formos. Med. Assoc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Amphansap, T.; Stitkitti, N.; Arirachakaran, A. The effectiveness of Police General Hospital’s fracture liaison service (PGH’s FLS) implementation after 5 years: A prospective cohort study. Osteoporos. Sarcopenia 2020, 6, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Sami, A.; Lems, W.; Mitchell, P.; Thomas, T.; Singer, A.; Speerin, R.; Fujita, M.; Pierroz, D.D.; Akesson, K.; et al. A Patient-Level Key Performance Indicator Set to Measure the Effectiveness of Fracture Liaison Services and Guide Quality Improvement: A Position Paper of the Iof Capture the Fracture Working Group, National Osteoporosis Foundation and Fragility Fracture Network. Osteoporos. Int. 2020, 31, 1193–1204. [Google Scholar]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Unnanuntana, A.; Jarusriwanna, A.; Nepal, S. Validity and responsiveness of Barthel index for measuring functional recovery after hemiarthroplasty for femoral neck fracture. Arch. Orthop. Trauma Surg. 2018, 138, 1671–1677. [Google Scholar] [CrossRef]
- Bauer, D.C. Osteoporosis Treatment After Hip Fracture: Bad News and Getting Worse. JAMA Netw. Open 2018, 1, e180844. [Google Scholar] [CrossRef]
- Kung, A.W.; Fan, T.; Xu, L.; Xia, W.B.; Park, I.H.; Kim, H.S.; Chan, S.P.; Lee, J.K.; Koh, L.; Soong, Y.K.; et al. Factors influencing diagnosis and treatment of osteoporosis after a fragility fracture among postmenopausal women in Asian countries: A retrospective study. BMC Women’s Health 2013, 13, 7. [Google Scholar] [CrossRef] [Green Version]
- González-Quevedo, D.; Bautista-Enrique, D.; Pérez-Del-Río, V.; Bravo-Bardají, M.; García-de-Quevedo, D.; Tamimi, I. Fracture Liaison Service and Mortality in Elderly Hip Fracture Patients: A Prospective Cohort Study. Osteoporos. Int. 2020, 31, 77–84. [Google Scholar] [CrossRef]
- Amphansap, T.; Stitkitti, N.; Dumrongwanich, P. Evaluation of Police General Hospital’s Fracture Liaison Service (Pgh’s Fls): The First Study of a Fracture Liaison Service in Thailand. Osteoporos Sarcopenia 2016, 2, 238–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baroni, M.; Zampi, E.; Rinonapoli, G.; Serra, R.; Zengarini, E.; Duranti, G.; Ercolani, S.; Conti, F.; Caraffa, A.; Mecocci, P.; et al. Fracture prevention service to bridge the osteoporosis care gap. Clin. Interv. Aging 2015, 10, 1035–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.-Y.; Tsai, K.-S.; Peng, J.-K.; Chen, C.-H.; Lin, G.-T.; Lin, C.-H.; Tu, S.-T.; Mao, I.-C.; Gau, Y.-L.; Liu, H.-C.; et al. The development of Taiwan Fracture Liaison Service network. Osteoporos. Sarcopenia 2018, 4, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Warriner, A.H.; Curtis, J.R. Adherence to osteoporosis treatments: Room for improvement. Curr. Opin. Rheumatol. 2009, 21, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Chiang, M.-H.; Huang, Y.-Y.; Kuo, Y.-J.; Huang, S.-W.; Jang, Y.-C.; Chu, F.-L.; Chen, Y.-P. Prognostic Factors for Mortality, Activity of Daily Living, and Quality of Life in Taiwanese Older Patients within 1 Year Following Hip Fracture Surgery. J. Pers. Med. 2022, 12, 102. [Google Scholar] [CrossRef]
- Senay, A.; Fernandes, J.C.; Delisle, J.; Morin, S.N.; Perreault, S. Persistence and compliance to osteoporosis therapy in a fracture liaison service: A prospective cohort study. Arch. Osteoporos. 2019, 14, 87. [Google Scholar] [CrossRef]
- Penrod, J.D.; Litke, A.; Hawkes, W.G.; Magaziner, J.; Koval, K.J.; Doucette, J.T.; Silberzweig, S.B.; Siu, A.L. Heterogeneity in Hip Fracture Patients: Age, Functional Status, and Comorbidity. J. Am. Geriatr. Soc. 2007, 55, 407–413. [Google Scholar] [CrossRef]
- Chen, Y.P.; Wong, P.K.; Tsai, M.J.; Chang, W.C.; Hsieh, T.S.; Leu, T.H.; Lin, C.F.J.; Lee, C.H.; Kuo, Y.J.; Lin, C.Y. The High Prevalence of Sarcopenia and Its Associated Outcomes Following Hip Surgery in Taiwanese Geriatric Patients with a Hip Fracture. J. Formos. Med. Assoc. 2020, 119, 1807–1816. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 2021, CD007146. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Zhang, J.; Chen, L.; Wenkert, D.; Daigle, S.G.; Grauer, A.; Curtis, J.R. Risk of Subsequent Fracture after Prior Fracture among Older Women. Osteoporos. Int. 2019, 30, 79–92. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Variable | Pre-FLS (n = 110) | Post-FLS (n = 117) | p Value |
|---|---|---|---|
| Age | 82.98 ± 8.20 | 80.67 ± 9.76 | 0.071 |
| Gender | 0.66 | ||
| Female | 81 (73.6%) | 83 (70.9%) | |
| Male | 27 (26.4%) | 34 (29.1%) | |
| BMI | 22.31 ± 3.74 | 21.58 ± 3.46 | 0.063 |
| Fracture type | 0.349 | ||
| Femoral neck fracture | 66 (60.0%) | 62 (53.0%) | |
| Peritrochanteric fracture | 44 (40.0%) | 55 (47.0%) | |
| Lesion side | 0.233 | ||
| Left | 52 (47.3%) | 65 (55.6%) | |
| Right | 58 (52.7%) | 52 (44.4%) | |
| CCI | 5.05 ± 1.74 | 4.87 ± 1.80 | 0.475 |
| Preoperative serum tests | |||
| Hemoglobin (g/dL) | 12.05 ±1.78 | 12.18 ± 1.74 | 0.924 |
| Creatinine (mg/dL) | 1.36 ±1.70 | 1.07 ± 0.96 | 0.477 |
| Sodium (mmol/L) | 137.01 ±3.77 | 136.62 ± 4.29 | 0.475 |
| Potassium (mmol/L) | 3.94 ±0.51 | 3.90 ± 0.46 | 0.617 |
| Surgical methods | 0.173 | ||
| Joint replacement | 48 (43.6%) | 40 (34.2%) | |
| Internal fixation | 62 (56.4%) | 77 (65.8%) | |
| Surgical delay from admission | 0.982 | ||
| Within 24 h | 66 (60%) | 70 (59.8%) | |
| 24–48 h | 32 (29.1%) | 35 (29.9%) | |
| >48 h | 12 (10.9%) | 12 (10.2%) | |
| Surgical time (h) | 71.61 ± 26.23 | 85.92 ± 54.62 | 0.073 |
| Surgical blood loss | 102.00 ± 91.95 | 106.39 ± 110.84 | 0.851 |
| Pre-fracture ADL | 82.36 ± 24.23 | 83.25 ± 23.78 | 0.959 |
| KPIs | Pre-FLS (n = 110) | Post-FLS (n = 117) | p Value |
|---|---|---|---|
| Assessment with DXA within 12 weeks after surgery | 92 (83.6%) | 102 (90.9%) | 0.449 |
| T-score | −3.93 ± 1.10 | −3.90 ± 1.12 | 0.84 |
| Sarcopenia screening | |||
| Handgrip strength (kg) | 14.52 ± 7.93 | 14.42 ± 12.50 | 0.382 |
| Muscle mass assessment with DXA | 80 (72.7%) | 96 (82.1%) | 0.093 |
| Muscle mass (ASMI, kg/m2) | 5.67 ± 1.04 | 5.70 ± 1.12 | 0.84 |
| Diagnosis of sarcopenia | 42 (53.2%) | 49 (51.3%) | 0.873 |
| Post-surgery physiotherapy consultation | 32 (29.1%) | 117(100%) | 0.000 |
| AOM use | |||
| Initiating treatment with AOMs | 32 (22.8%) | 74 (72.3%) | 0.000 |
| Prescription within 3 months after surgery | 24/32 (75%) | 67/74 (90.5%) | 0.071 |
| Denosumab | 10 (31.3%) | 46 (62.3%) | |
| Bisphosphonate | 11 (34.3%) | 19 (25.7%) | |
| Selective estrogen-receptor modulators | 7 (21.9%) | 2 (2.7%) | |
| Teriparatide | 4 (12.5%) | 7 (9.5%) | |
| Continuing AOMs for 1 year after fracture | 16 (14.5%) | 62 (53.0%) | |
| Nutrition supplements (i.e., calcium or vitamin D) | 16 (14.5%) | 65 (55.6%) | 0.000 |
| Receiving home visits | 0 | 66 (56.4%) | 0.000 |
| Home Visits after Hip Fracture Surgery | n = 66 |
|---|---|
| Mean follow-up time after surgery (months) | 8.26 ± 3.40 |
| Mean age | 79.86 ± 9.52 |
| Environmental evaluation | |
| Indoor environmental hazards of falling | 54 (81.8%) |
| Inadequate light | 16 (24.2%) |
| Tripping hazards | 48 (72.7%) |
| Indoor environmental protection against falling | 26 (39.4%) |
| Antislip rubber mats in the bathroom | 22 (33.3%) |
| Grab bars on the path and in the bathroom | 10 (15.2%) |
| Changing environmental hazards after visits | 23/54 (42.6%) |
| Stop AOM use before home visits | 30 |
| Return to clinics for AOM treatment after home visits | 16/30 (53.3%) |
| Outcomes | Pre-FLS (n = 110) | Post-FLS (n = 117) | p Value |
|---|---|---|---|
| Refracture within the first year of surgery | 13 (11.8%) | 5 (4.9%) | 0.048 |
| Mortality within the first year of surgery | 17 (17.9%) | 12 (11.8%) | 0.225 |
| ADL at 1-year follow-up | 64.19 ± 34.17 | 75.61 ± 30.67 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-P.; Chang, W.-C.; Wen, T.-W.; Chien, P.-C.; Huang, S.-W.; Kuo, Y.-J. Multipronged Programmatic Strategy for Preventing Secondary Fracture and Facilitating Functional Recovery in Older Patients after Hip Fractures: Our Experience in Taipei Municipal Wanfang Hospital. Medicina 2022, 58, 875. https://doi.org/10.3390/medicina58070875
Chen Y-P, Chang W-C, Wen T-W, Chien P-C, Huang S-W, Kuo Y-J. Multipronged Programmatic Strategy for Preventing Secondary Fracture and Facilitating Functional Recovery in Older Patients after Hip Fractures: Our Experience in Taipei Municipal Wanfang Hospital. Medicina. 2022; 58(7):875. https://doi.org/10.3390/medicina58070875
Chicago/Turabian StyleChen, Yu-Pin, Wei-Chun Chang, Tsai-Wei Wen, Pei-Chun Chien, Shu-Wei Huang, and Yi-Jie Kuo. 2022. "Multipronged Programmatic Strategy for Preventing Secondary Fracture and Facilitating Functional Recovery in Older Patients after Hip Fractures: Our Experience in Taipei Municipal Wanfang Hospital" Medicina 58, no. 7: 875. https://doi.org/10.3390/medicina58070875
APA StyleChen, Y.-P., Chang, W.-C., Wen, T.-W., Chien, P.-C., Huang, S.-W., & Kuo, Y.-J. (2022). Multipronged Programmatic Strategy for Preventing Secondary Fracture and Facilitating Functional Recovery in Older Patients after Hip Fractures: Our Experience in Taipei Municipal Wanfang Hospital. Medicina, 58(7), 875. https://doi.org/10.3390/medicina58070875