
Comparison of Heart and Lung Doses According to Tumor Bed Boost Techniques in Early-Stage Left-Sided Breast Cancer: Simultaneous Integrated Boost versus Sequential Boost


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment Planning and Target Volume Delineation
2.3. Assessment of Plan Quality
2.4. Statistical Analysis
3. Results
3.1. Assessment of Plan Quality
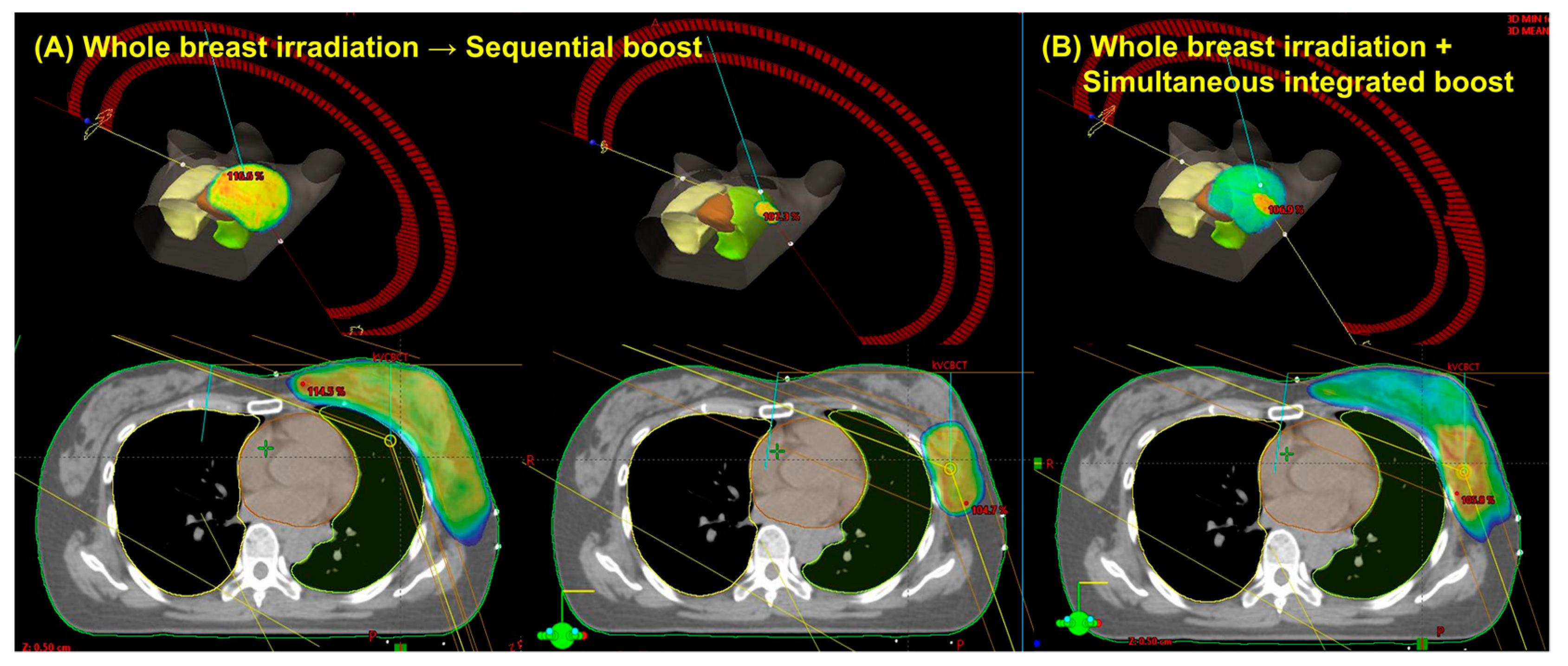
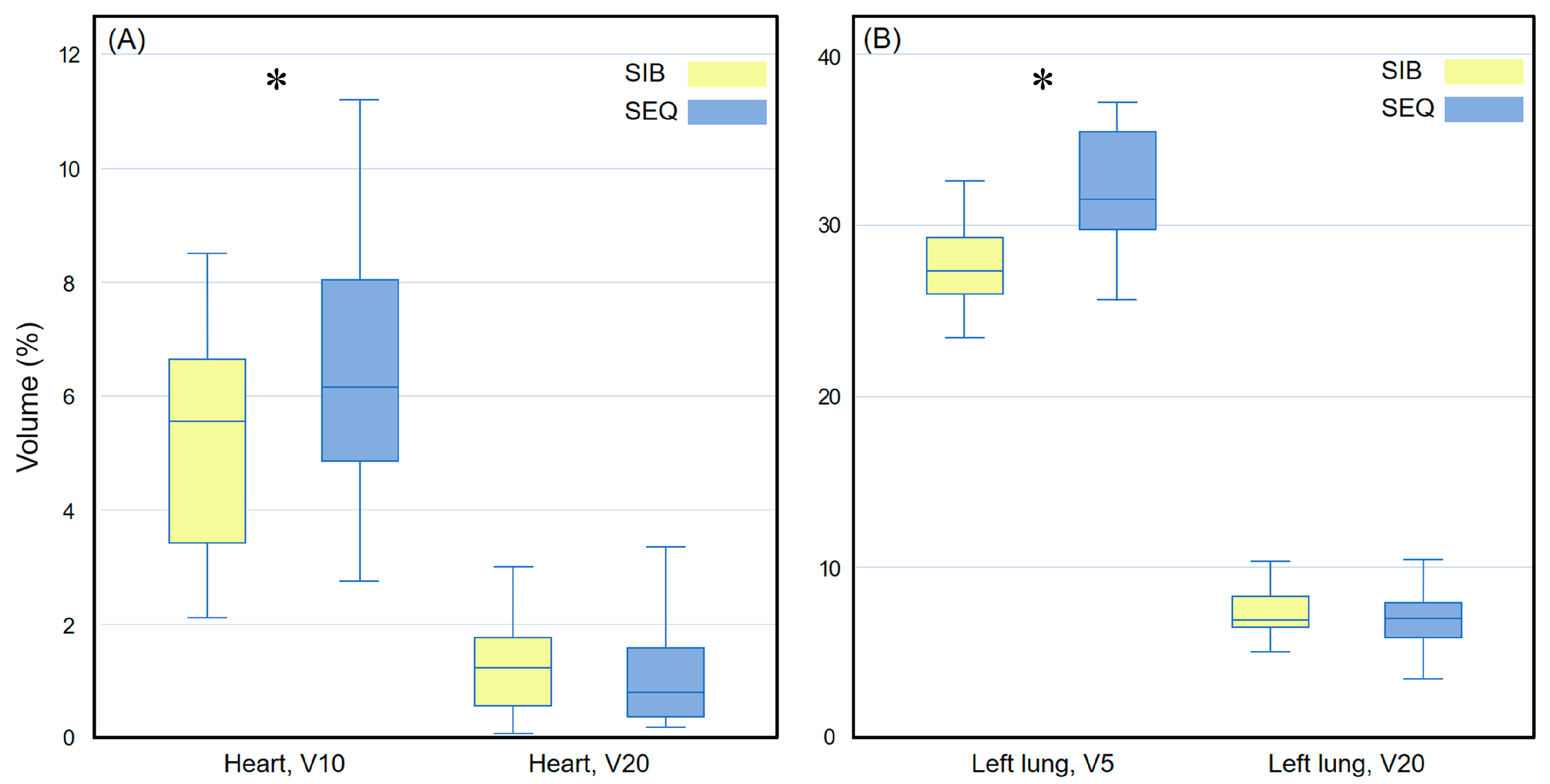
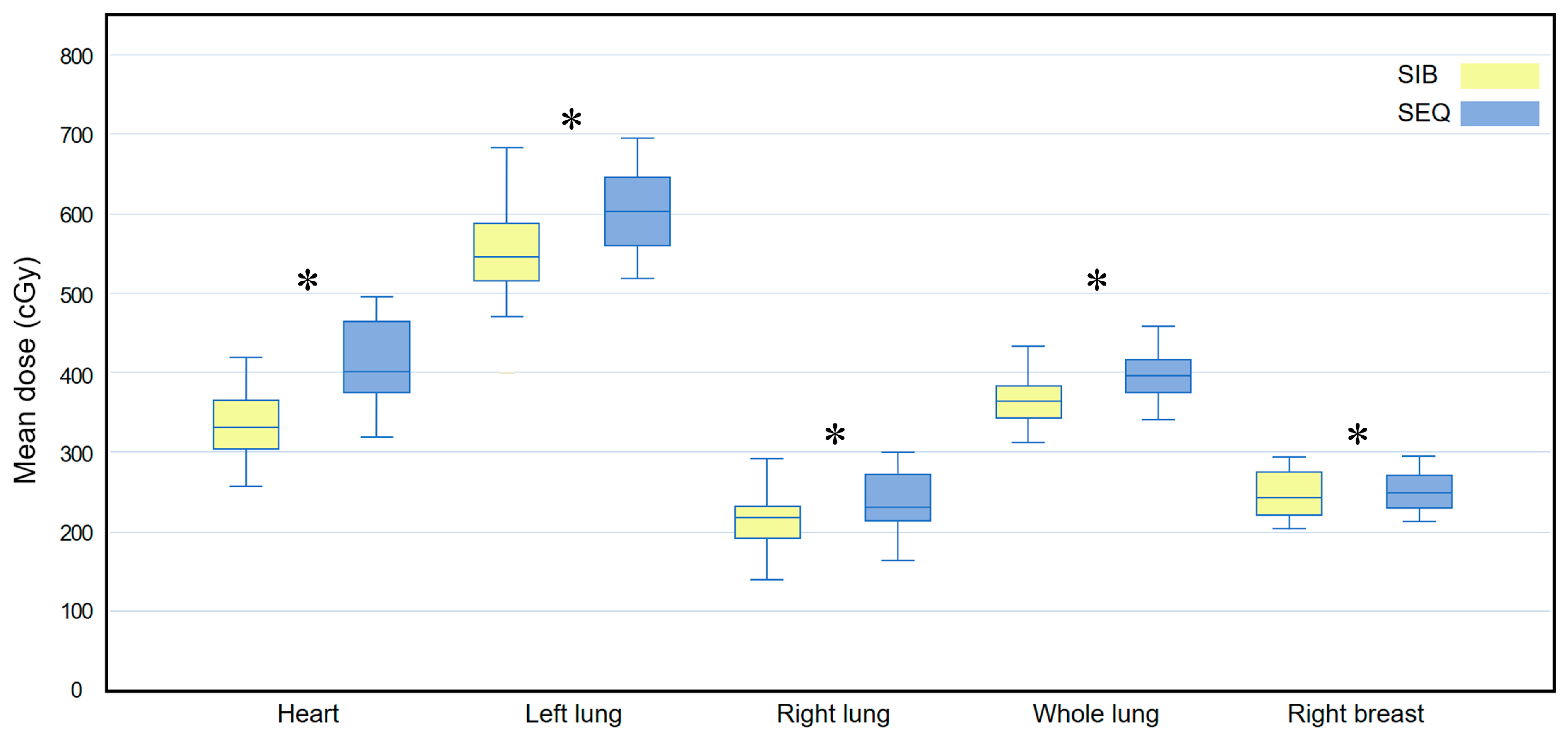
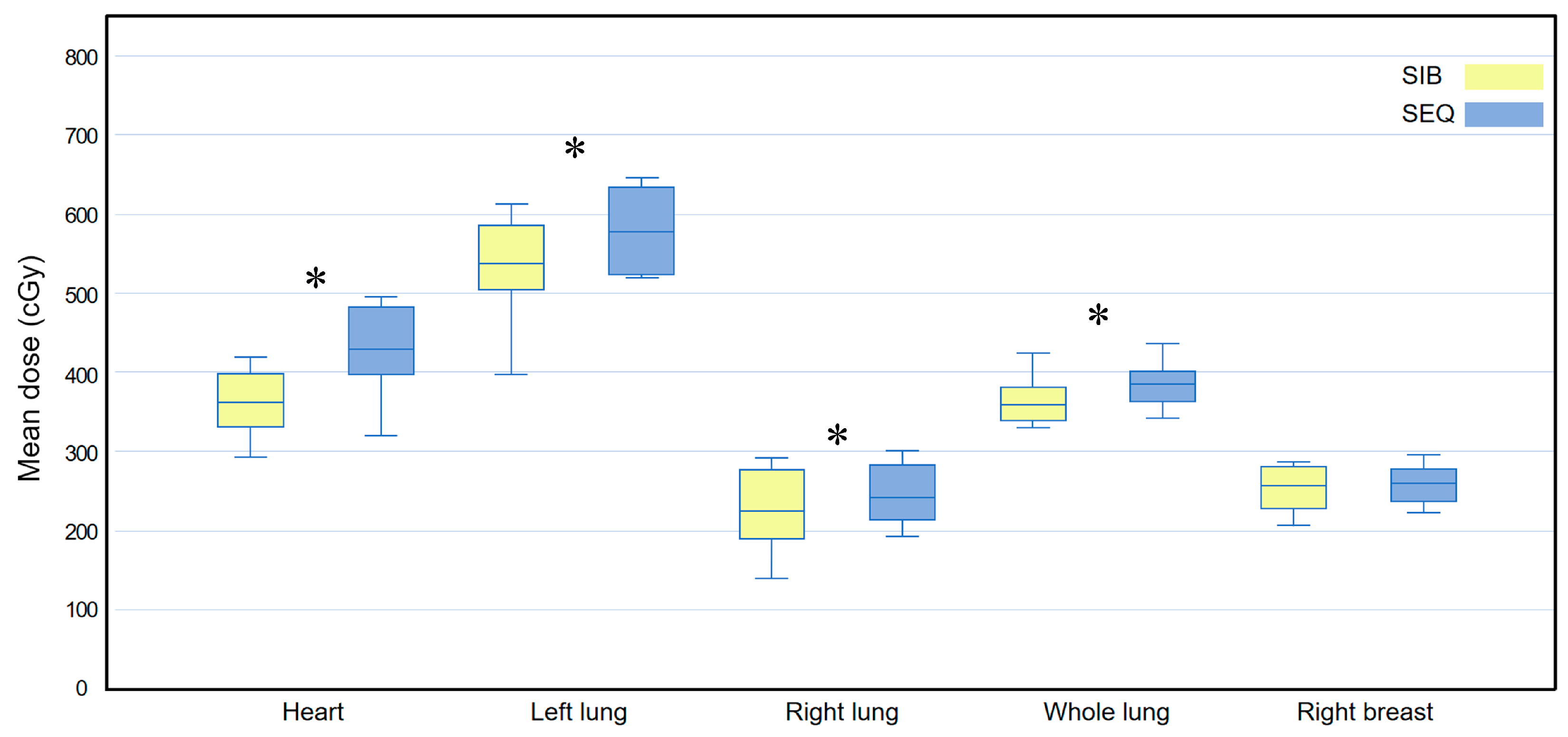
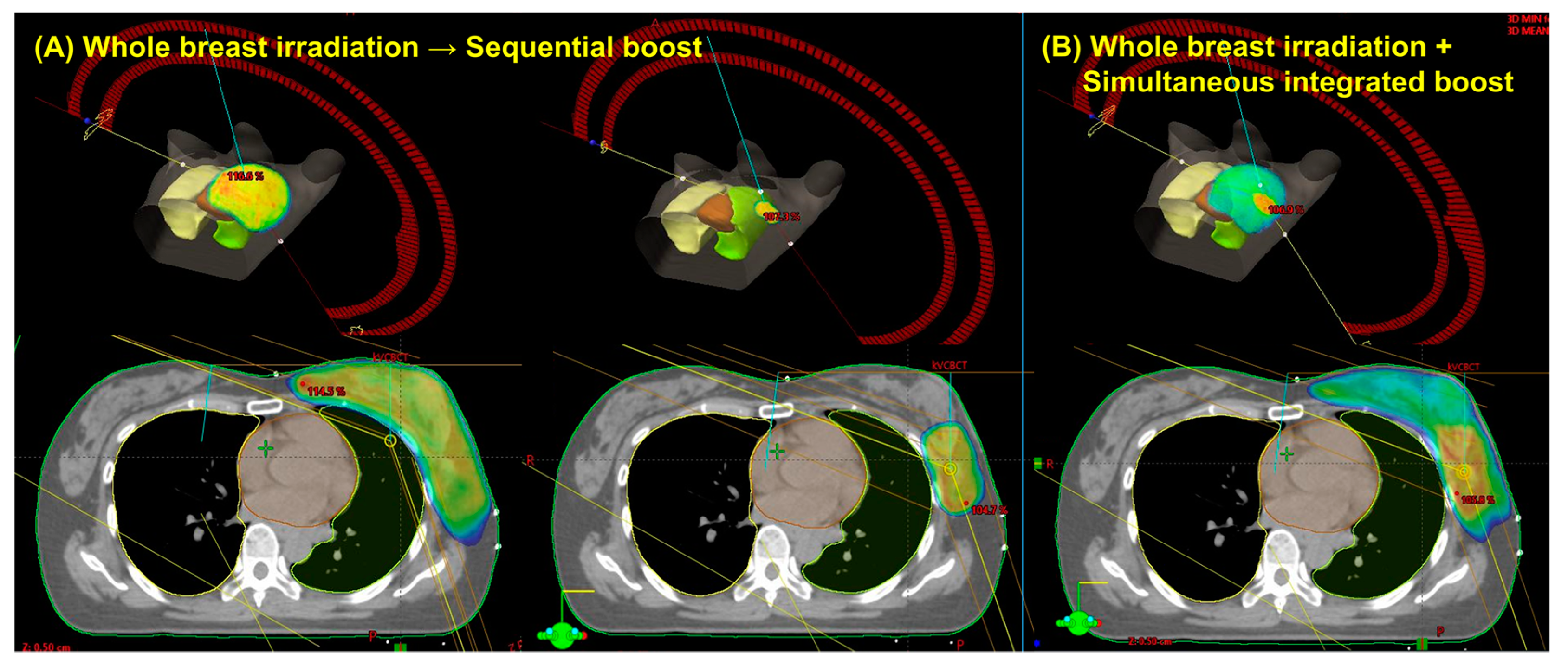
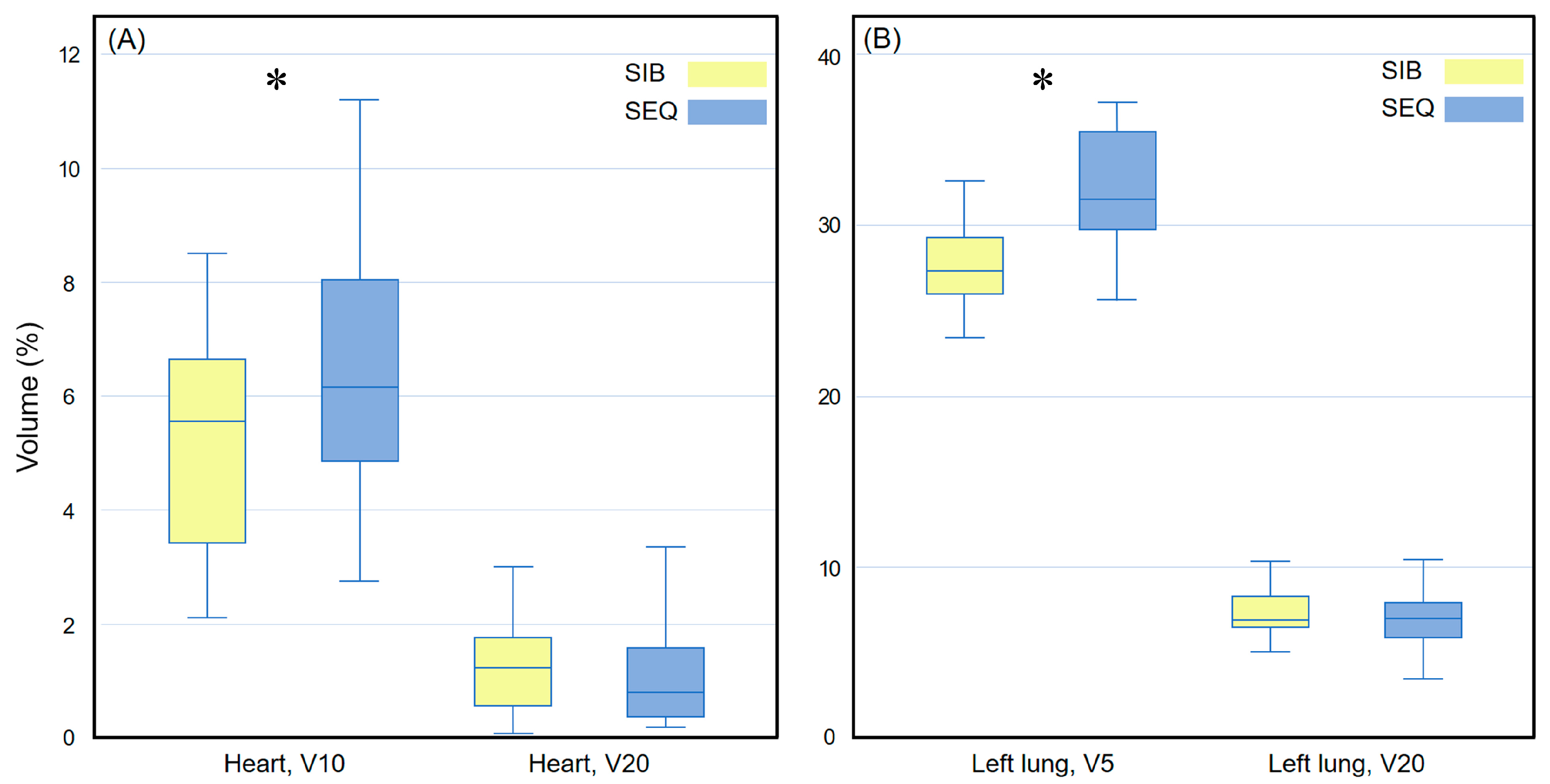
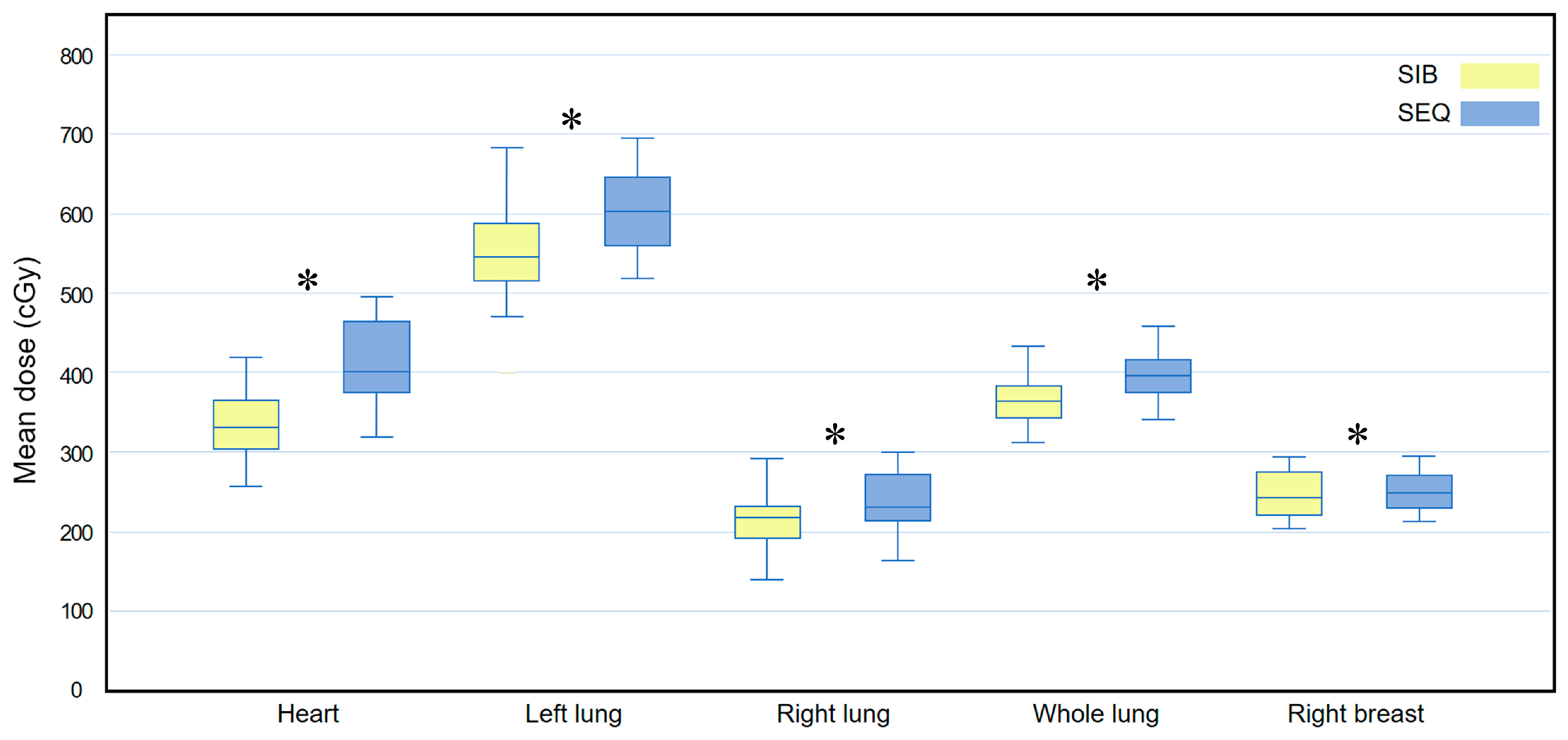
3.2. WBI-SIB versus WBI-SEQ Plan
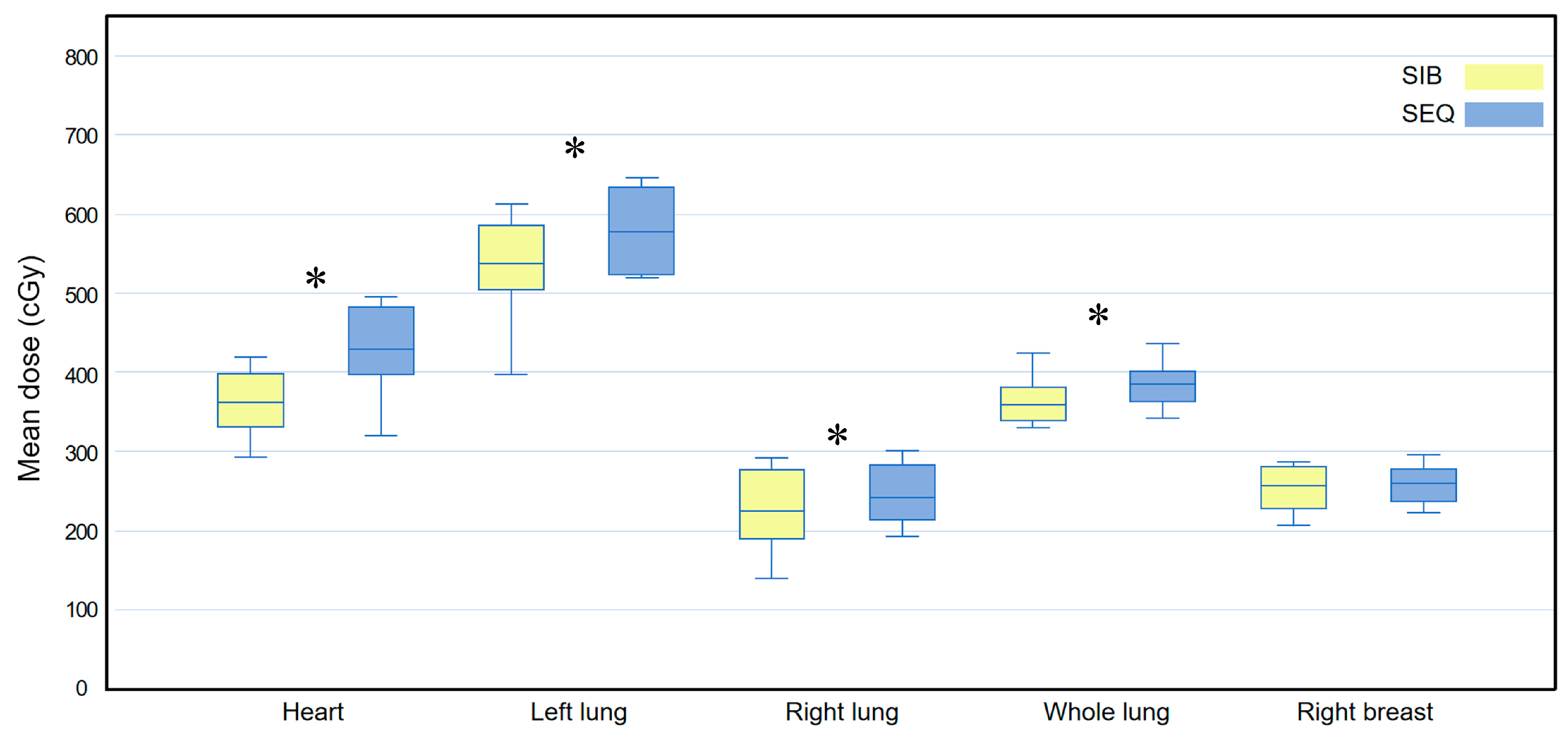
3.3. Subgroup Analysis: Inner Quadrant
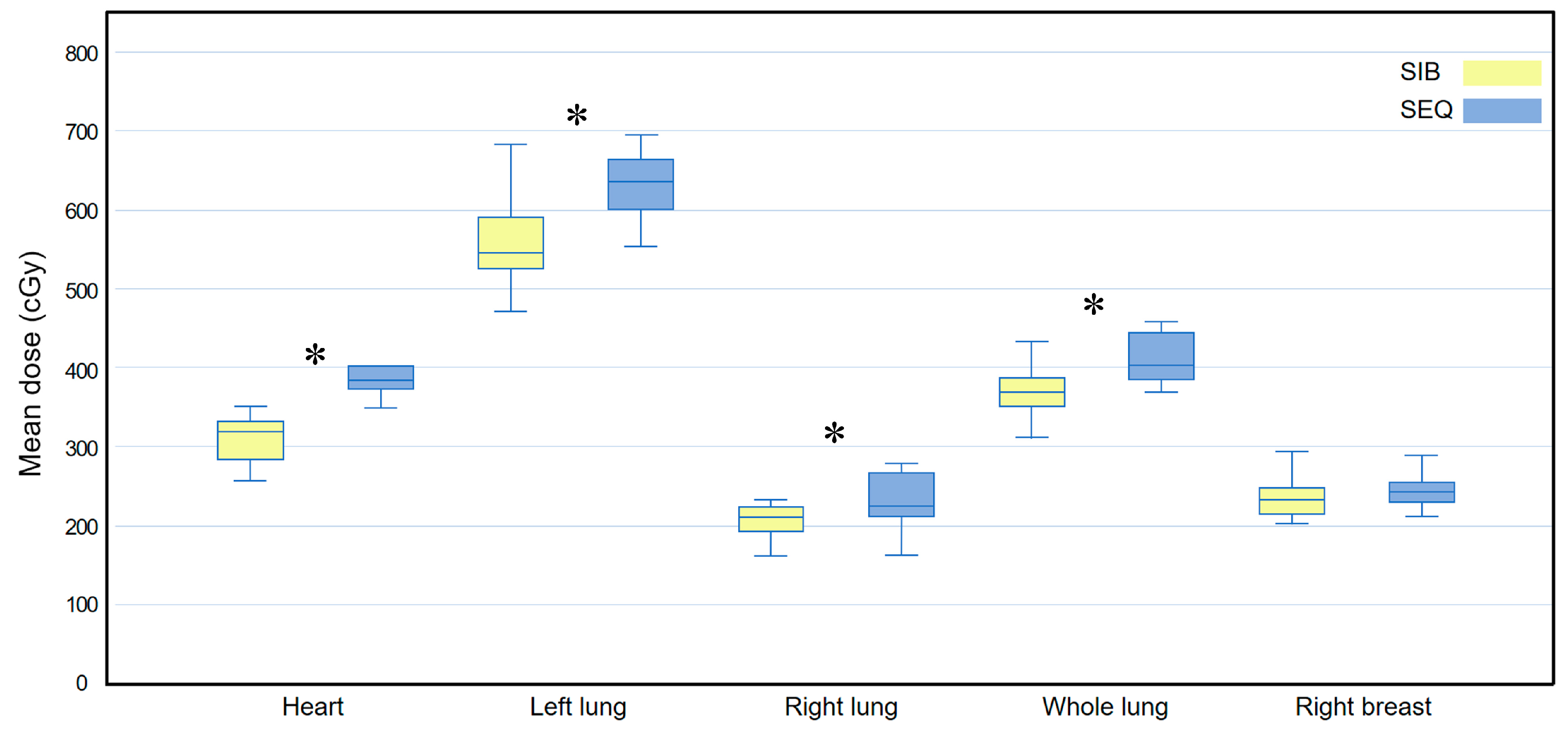
3.4. Subgroup Analysis: Outer Quadrant
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. Breast Cancer (Version 2.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 30 April 2022).
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Bronnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darby, S.C.; McGale, P.; Taylor, C.W.; Peto, R. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005, 6, 557–565. [Google Scholar] [CrossRef]
- Henson, K.E.; McGale, P.; Taylor, C.; Darby, S.C. Radiation-related mortality from heart disease and lung cancer more than 20 years after radiotherapy for breast cancer. Br. J. Cancer 2013, 108, 179–182. [Google Scholar] [CrossRef] [Green Version]
- Otto, K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med. Phys. 2008, 35, 310–317. [Google Scholar] [CrossRef]
- Guerrero, M.; Li, X.A.; Earl, M.A.; Sarfaraz, M.; Kiggundu, E. Simultaneous integrated boost for breast cancer using IMRT: A radiobiological and treatment planning study. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 1513–1522. [Google Scholar] [CrossRef]
- Hurkmans, C.W.; Meijer, G.J.; van Vliet-Vroegindeweij, C.; van der Sangen, M.J.; Cassee, J. High-dose simultaneously integrated breast boost using intensity-modulated radiotherapy and inverse optimization. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 923–930. [Google Scholar] [CrossRef]
- Hijal, T.; Fournier-Bidoz, N.; Castro-Pena, P.; Kirova, Y.M.; Zefkili, S.; Bollet, M.A.; Dendale, R.; Campana, F.; Fourquet, A. Simultaneous integrated boost in breast conserving treatment of breast cancer: A dosimetric comparison of helical tomotherapy and three-dimensional conformal radiotherapy. Radiother. Oncol. 2010, 94, 300–306. [Google Scholar] [CrossRef]
- Alford, S.L.; Prassas, G.N.; Vogelesang, C.R.; Leggett, H.J.; Hamilton, C.S. Adjuvant breast radiotherapy using a simultaneous integrated boost: Clinical and dosimetric perspectives. J. Med. Imaging Radiat. Oncol. 2013, 57, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Aly, M.M.; Abo-Madyan, Y.; Jahnke, L.; Wenz, F.; Glatting, G. Comparison of breast sequential and simultaneous integrated boost using the biologically effective dose volume histogram (BEDVH). Radiat. Oncol. 2016, 11, 16. [Google Scholar] [CrossRef] [Green Version]
- Van Parijs, H.; Reynders, T.; Heuninckx, K.; Verellen, D.; Storme, G.; De Ridder, M. Breast conserving treatment for breast cancer: Dosimetric comparison of sequential versus simultaneous integrated photon boost. Biomed. Res. Int. 2014, 2014, 827475. [Google Scholar] [CrossRef]
- Onal, C.; Efe, E.; Guler, O.C.; Yildirim, B.A. Dosimetric comparison of sequential versus simultaneous-integrated boost in early-stage breast cancer patients treated with breast-conserving surgery. In Vivo 2019, 33, 2181–2189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offersen, B.V.; Boersma, L.J.; Kirkove, C.; Hol, S.; Aznar, M.C.; Biete Sola, A.; Kirova, Y.M.; Pignol, J.P.; Remouchamps, V.; Verhoeven, K.; et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother. Oncol. 2015, 114, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Kline, R.; Gillin, M.; Souhami, L.; Hirschfeld, A.; Dinapoli, R.; Martin, L. Radiation Therapy Oncology Group: Radiosurgery quality assurance guidelines. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 1231–1239. [Google Scholar] [CrossRef]
- Feuvret, L.; Noel, G.; Mazeron, J.J.; Bey, P. Conformity index: A review. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Lomax, N.J.; Scheib, S.G. Quantifying the degree of conformity in radiosurgery treatment planning. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 1409–1419. [Google Scholar] [CrossRef]
- Carlson, L.E.; Watt, G.P.; Tonorezos, E.S.; Chow, E.J.; Yu, A.F.; Woods, M.; Lynch, C.F.; John, E.M.; Mellemkjr, L.; Brooks, J.D.; et al. Coronary artery disease in young women after radiation therapy for breast cancer: The WECARE study. JACC Cardio Oncol. 2021, 3, 381–392. [Google Scholar] [CrossRef]
- Duma, M.N.; Baumann, R.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Harms, W.; Hehr, T.; Krug, D.; et al. Heart-sparing radiotherapy techniques in breast cancer patients: A recommendation of the breast cancer expert panel of the German society of radiation oncology (DEGRO). Strahlenther. Onkol. 2019, 195, 861–871. [Google Scholar] [CrossRef]
- Viren, T.; Heikkila, J.; Myllyoja, K.; Koskela, K.; Lahtinen, T.; Seppala, J. Tangential volumetric modulated arc therapy technique for left-sided breast cancer radiotherapy. Radiat. Oncol. 2015, 10, 79. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Zhang, Y.; Yang, Z.; Liang, F.; Wu, J.; Wang, R. A comparison of clinical outcomes between simultaneous integrated boost (SIB) versus sequential boost (SEQ) intensity modulated radiation therapy (IMRT) for head and neck cancer: A meta-analysis. Medicine 2019, 98, e16942. [Google Scholar] [CrossRef]
- Zwicker, F.; Hoefel, S.; Kirchner, C.; Huber, P.E.; Debus, J.; Schempp, M. Hypofractionated radiotherapy with simultaneous-integrated boost after breast-conserving surgery compared to standard boost-applications using helical tomotherapy with TomoEdge. Anticancer Res. 2021, 41, 1909–1920. [Google Scholar] [CrossRef]
- Yarnold, J.; Ashton, A.; Bliss, J.; Homewood, J.; Harper, C.; Hanson, J.; Haviland, J.; Bentzen, S.; Owen, R. Fractionation sensitivity and dose response of late adverse effects in the breast after radiotherapy for early breast cancer: Long-term results of a randomised trial. Radiother. Oncol. 2005, 75, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Owen, J.R.; Ashton, A.; Bliss, J.M.; Homewood, J.; Harper, C.; Hanson, J.; Haviland, J.; Bentzen, S.M.; Yarnold, J.R. Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: Long-term results of a randomised trial. Lancet Oncol. 2006, 7, 467–471. [Google Scholar] [CrossRef] [Green Version]
- Group, S.T.; Bentzen, S.M.; Agrawal, R.K.; Aird, E.G.; Barrett, J.M.; Barrett-Lee, P.J.; Bliss, J.M.; Brown, J.; Dewar, J.A.; Dobbs, H.J.; et al. The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: A randomised trial. Lancet Oncol. 2008, 9, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Group, S.T.; Bentzen, S.M.; Agrawal, R.K.; Aird, E.G.; Barrett, J.M.; Barrett-Lee, P.J.; Bentzen, S.M.; Bliss, J.M.; Brown, J.; Dewar, J.A.; et al. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: A randomised trial. Lancet 2008, 371, 1098–1107. [Google Scholar] [CrossRef] [Green Version]
- Haviland, J.S.; Owen, J.R.; Dewar, J.A.; Agrawal, R.K.; Barrett, J.; Barrett-Lee, P.J.; Dobbs, H.J.; Hopwood, P.; Lawton, P.A.; Magee, B.J.; et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013, 14, 1086–1094. [Google Scholar] [CrossRef]
- Whelan, T.J.; Pignol, J.P.; Levine, M.N.; Julian, J.A.; MacKenzie, R.; Parpia, S.; Shelley, W.; Grimard, L.; Bowen, J.; Lukka, H.; et al. Long-term results of hypofractionated radiation therapy for breast cancer. N. Engl. J. Med. 2010, 362, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Li, Y.; Sun, T.; Xu, M.; Wang, W.; Shao, Q.; Zhang, Y.; Li, J.; Yu, J. A comparative study on hypofractionated whole-breast irradiation with sequential or simultaneous integrated boost on different positions after breast-conserving surgery. Sci. Rep. 2021, 11, 18017. [Google Scholar] [CrossRef]
- Bouchardy, C.; Rapiti, E.; Usel, M.; Majno, S.B.; Vlastos, G.; Benhamou, S.; Miralbell, R.; Neyroud-Caspar, I.; Verkooijen, H.M.; Vinh-Hung, V. Excess of cardiovascular mortality among node-negative breast cancer patients irradiated for inner-quadrant tumors. Ann. Oncol. 2010, 21, 459–465. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
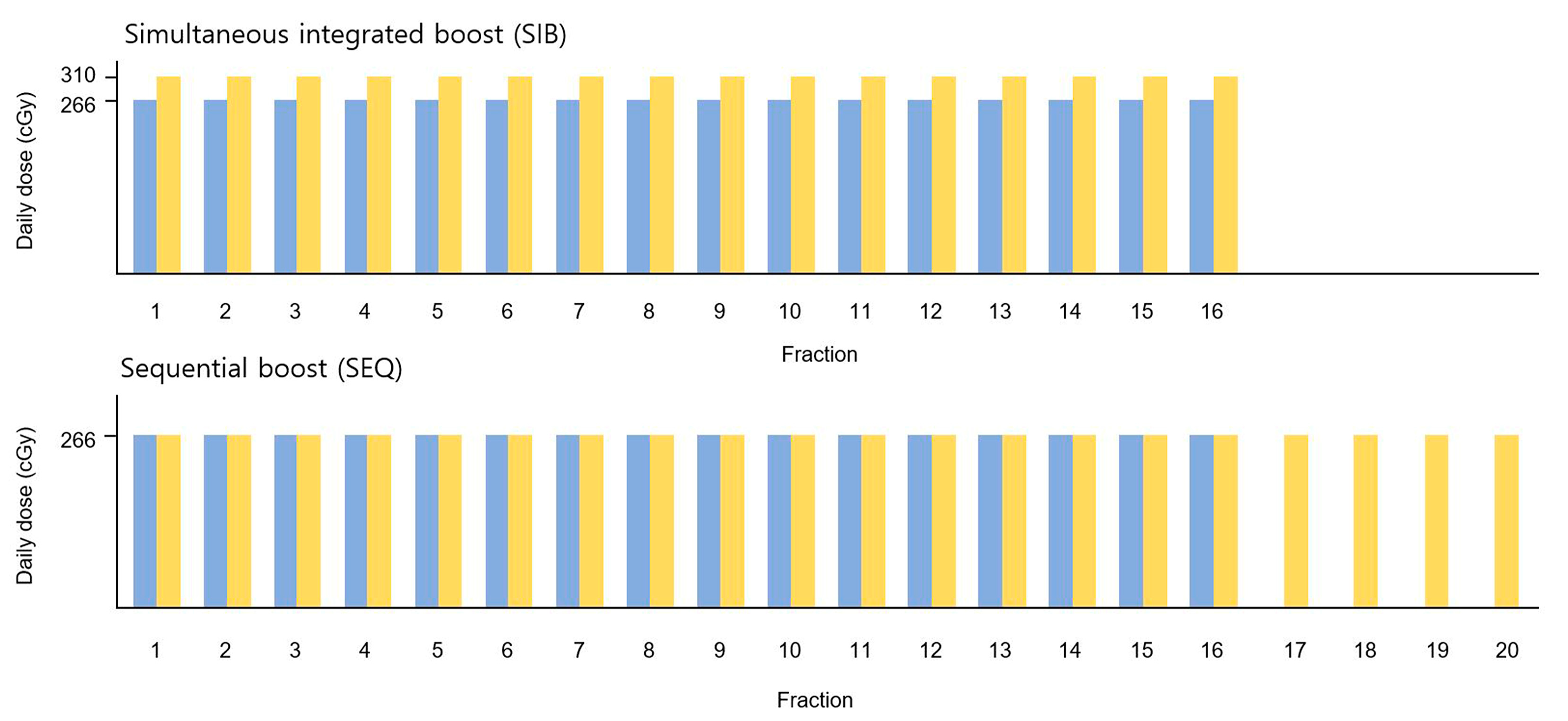
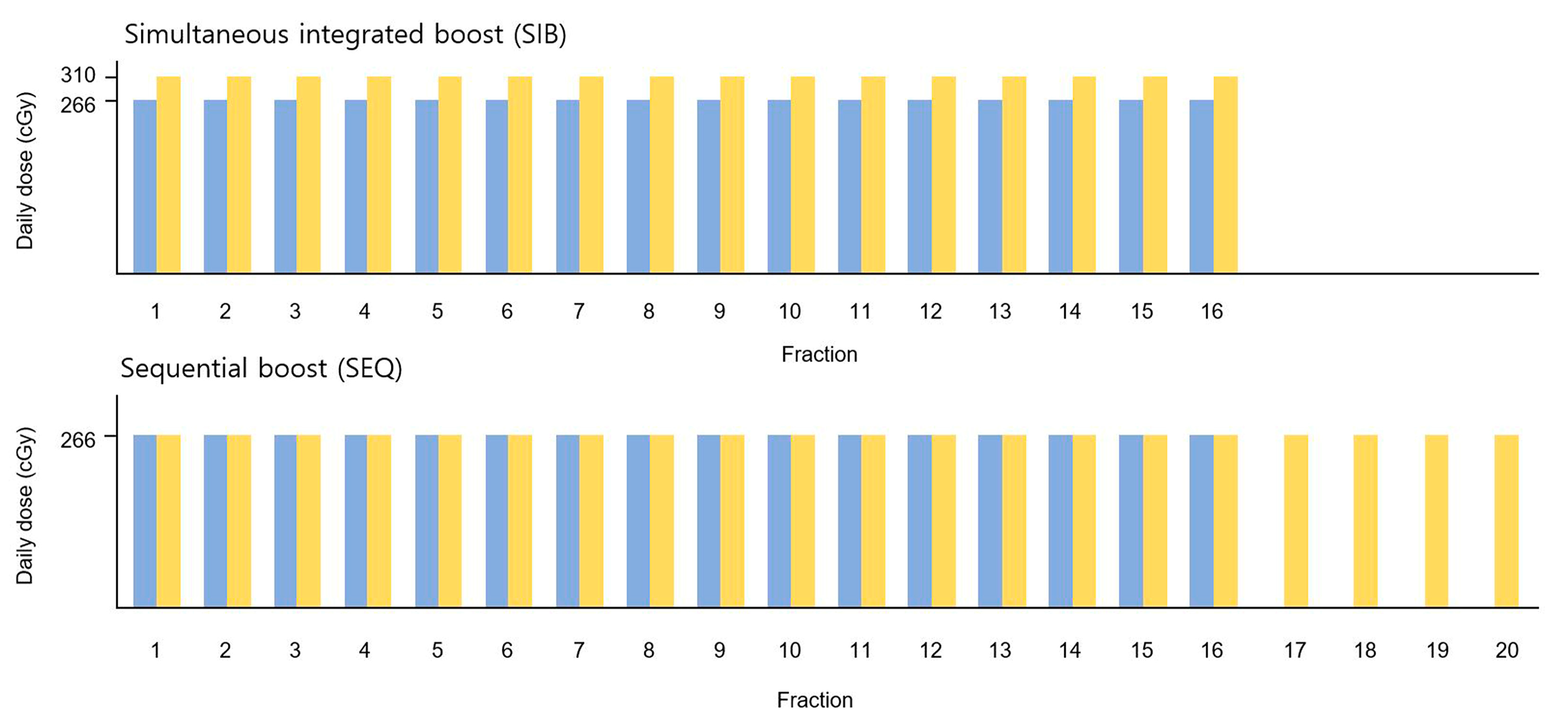
| Prescription | BED3 (Gy) | |
|---|---|---|
| Simultaneous integrated boost (SIB) SIB-PTVWB SIB-PTVBoost | 42.56 Gy in 16 fractions 49.60 Gy in 16 fractions | 80.30 100.85 |
| Sequential boost (SEQ) SEQ-PTVWB SEQ-PTVBoost | 42.56 Gy in 16 fractions 10.64 Gy in 4 fractions | 80.30 100.37 |
| Organ at Risk | Dose Constraints |
|---|---|
| Heart | V30 < 5% |
| Dmean < 5 Gy | |
| Ipsilateral lung | V20 < 20% |
| Dmean < 7 Gy | |
| Contralateral lung | Dmean < 3 Gy |
| Whole lungs | V20 < 10% |
| Dmean < 5 Gy | |
| Contralateral breast | Dmean < 3 Gy |
| Index for PTV | Formula | Reference Value |
|---|---|---|
| Homogeneity index | Imax/RI | ≤2: per protocol >2.0 and ≤2.5: minor deviation >2.5: major deviation |
| Conformity index | VRI/TV | 1: ideal value 1.0–2.0: per protocol 0.9–1.0 or 2.0–2.5: minor deviation <0.9 or >2.5: major deviation |
| Quality of coverage | Imin/RI | 1: ideal value ≥0.9 and <1.0: per protocol ≥0.8 and <0.9: minor deviation <0.8: major deviation |
| Characteristic | Classification | Number of Patients (%) |
|---|---|---|
| Age (years) | Median (range) | 54 (39–79) * |
| Histology | Invasive ductal carcinoma Metaplastic carcinoma | 19 (95.0) 1 (5.0) |
| Histologic grade | I II III | 4 (20.0) 9 (45.0) 7 (35.0) |
| Tumor location | Left inner quadrant Left outer quadrant | 10 (50.0) 10 (50.0) |
| T classification | T1mi T1 T2 | 2 (10.0) 11 (55.0) 7 (35.0) |
| Hormone receptor status | ER- or PR-positive ER- and PR-negative | 14 (70.0) 6 (30.0) |
| HER2/neu † receptor | Positive Negative | 0 (00.0) 20 (100.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Lee, N.K.; Lee, S.; Hwang, J. Comparison of Heart and Lung Doses According to Tumor Bed Boost Techniques in Early-Stage Left-Sided Breast Cancer: Simultaneous Integrated Boost versus Sequential Boost. Medicina 2022, 58, 873. https://doi.org/10.3390/medicina58070873
Kim M, Lee NK, Lee S, Hwang J. Comparison of Heart and Lung Doses According to Tumor Bed Boost Techniques in Early-Stage Left-Sided Breast Cancer: Simultaneous Integrated Boost versus Sequential Boost. Medicina. 2022; 58(7):873. https://doi.org/10.3390/medicina58070873
Chicago/Turabian StyleKim, Myungsoo, Nam Kwon Lee, Suk Lee, and Jinho Hwang. 2022. "Comparison of Heart and Lung Doses According to Tumor Bed Boost Techniques in Early-Stage Left-Sided Breast Cancer: Simultaneous Integrated Boost versus Sequential Boost" Medicina 58, no. 7: 873. https://doi.org/10.3390/medicina58070873
APA StyleKim, M., Lee, N. K., Lee, S., & Hwang, J. (2022). Comparison of Heart and Lung Doses According to Tumor Bed Boost Techniques in Early-Stage Left-Sided Breast Cancer: Simultaneous Integrated Boost versus Sequential Boost. Medicina, 58(7), 873. https://doi.org/10.3390/medicina58070873