
Prevention of Compression Fracture in Osteoporosis Patients under Minimally Invasive Trans-Foraminal Lumbar Interbody Fusion with Assistance of Bone-Mounted Robotic System in Two-Level Degenerative Lumbar Disease

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
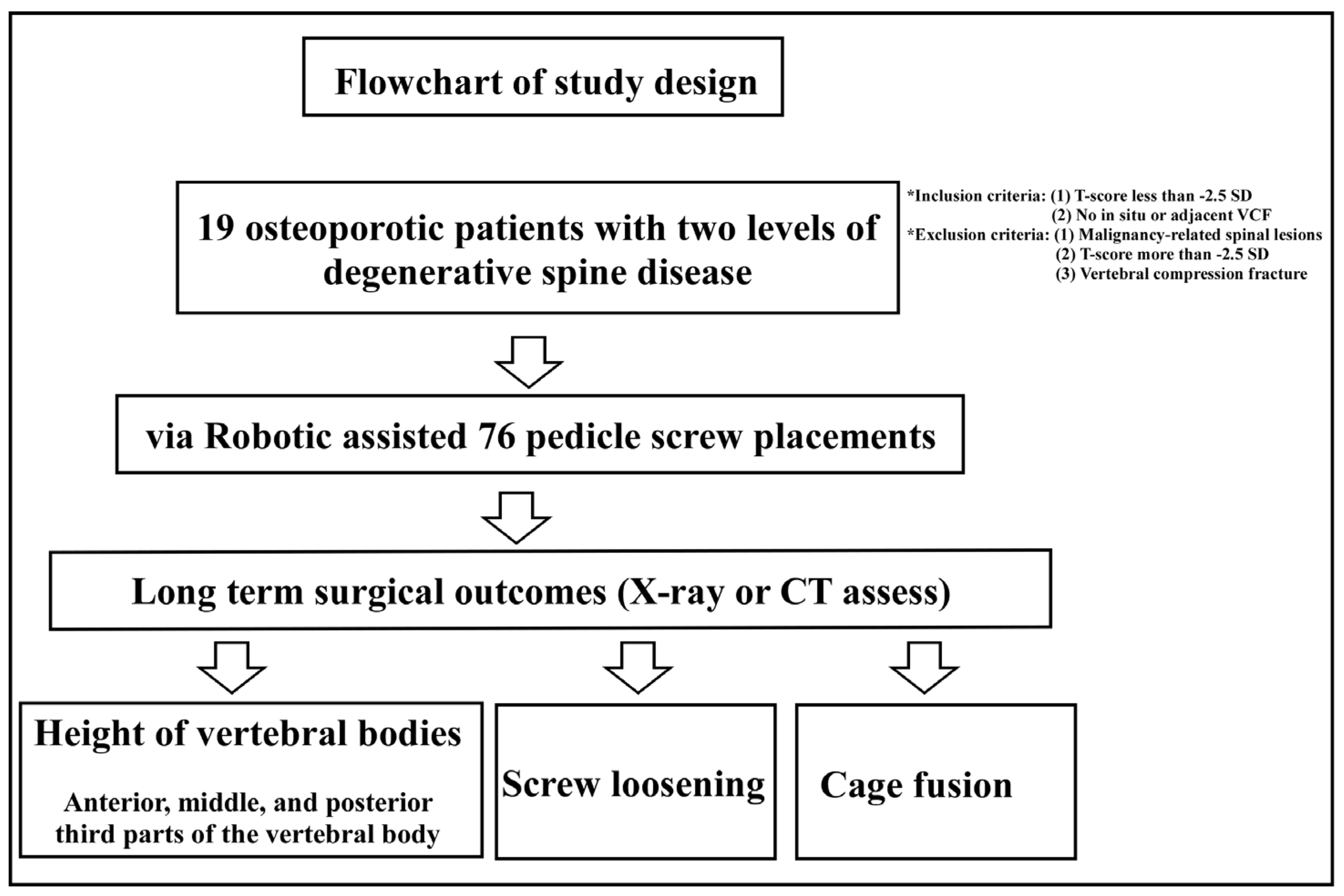
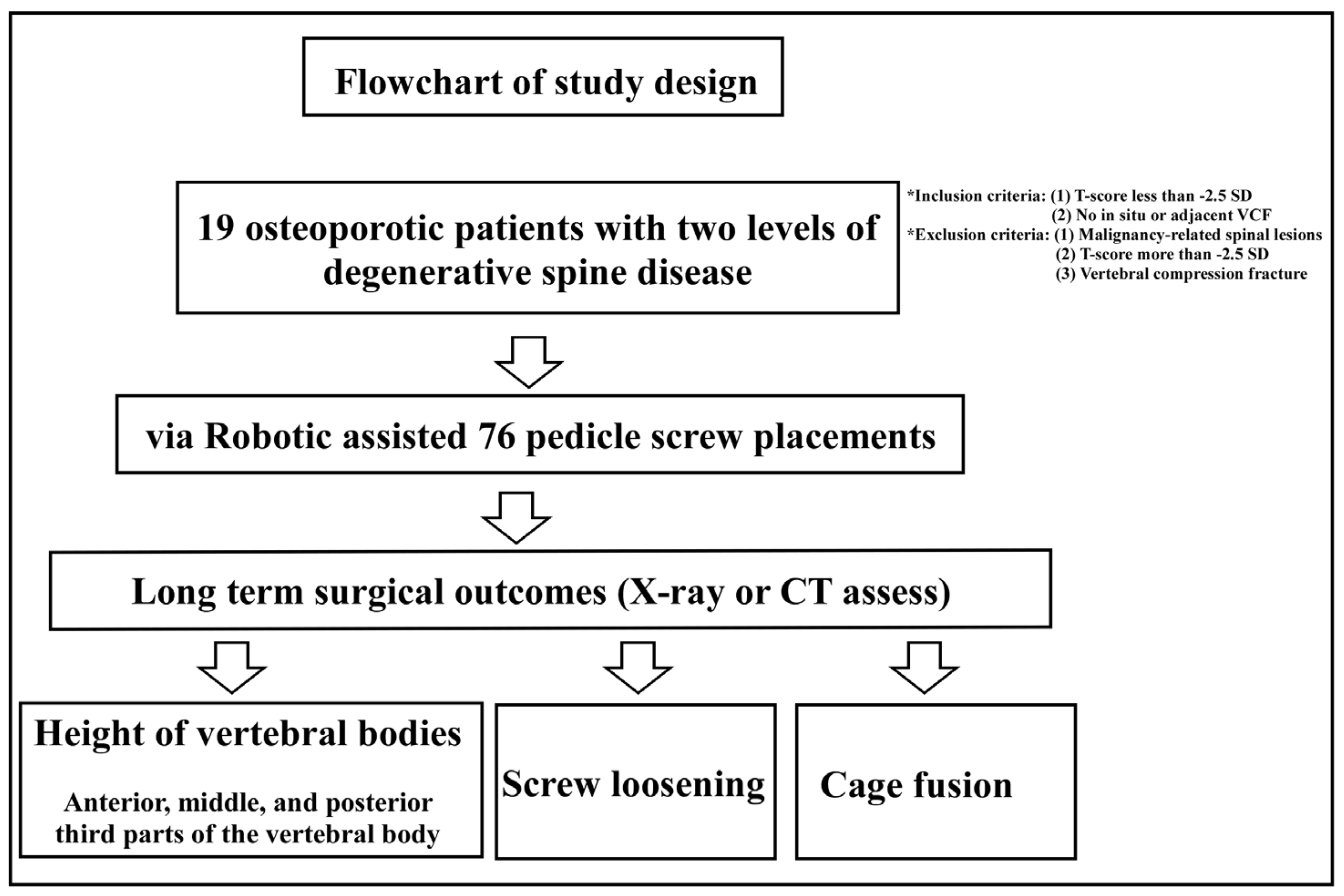
2.1. Study Patients
2.2. Inclusion and Exclusion Criteria
2.3. Radiological Assessment
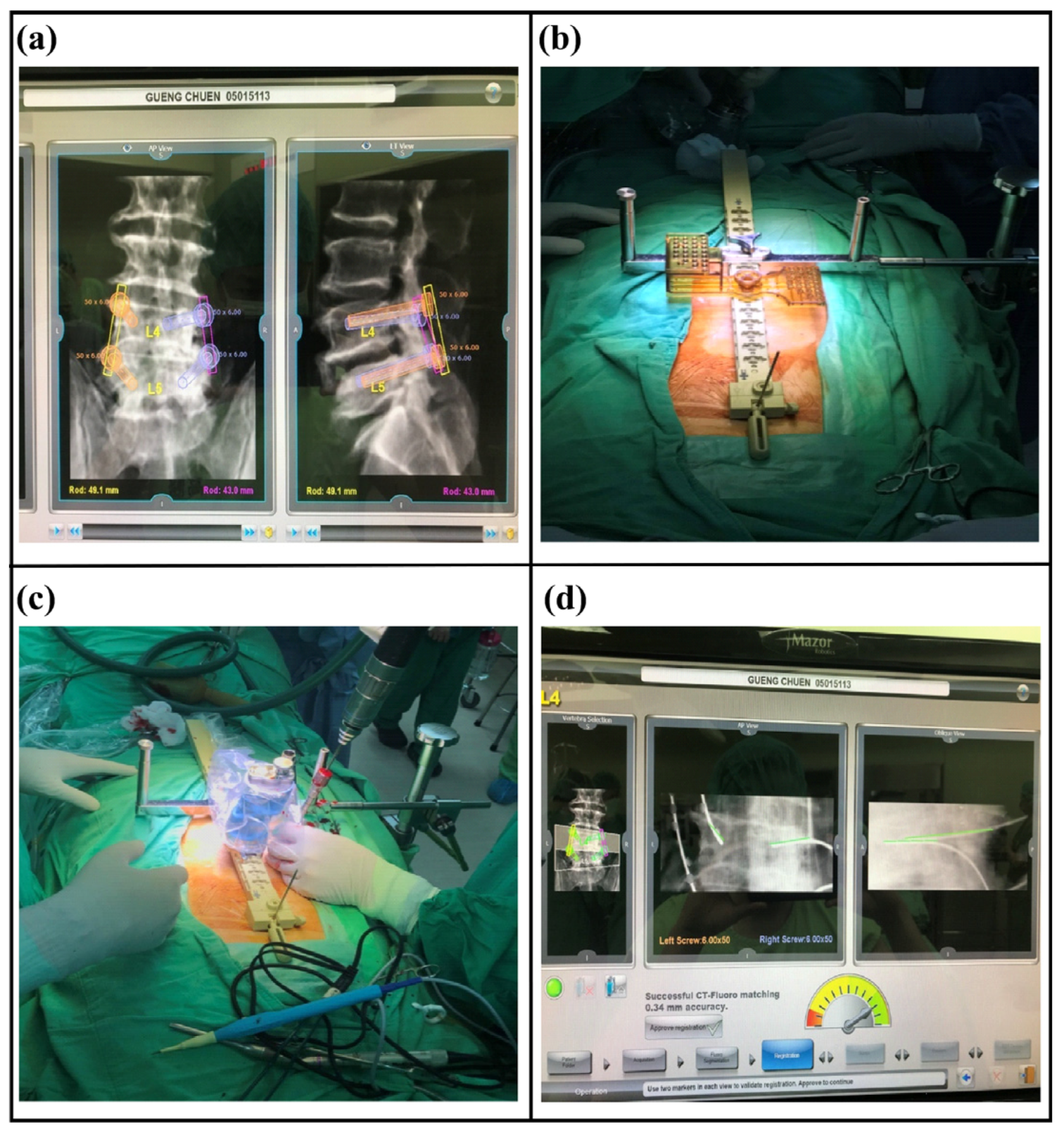
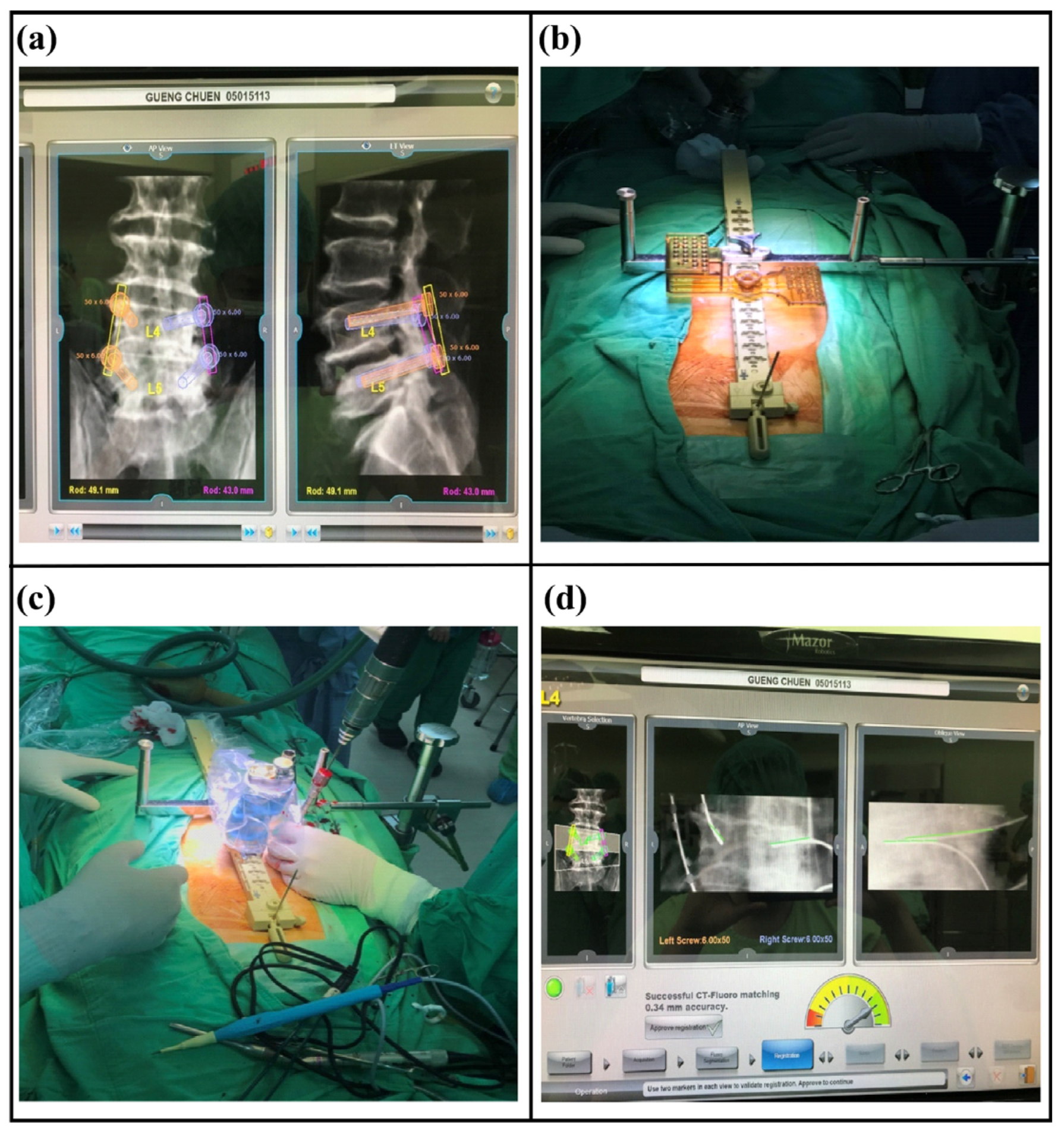
2.4. Surgical Technique
2.5. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tandon, V.; Franke, J.; Kalidindi, K.K.V. Advancements in osteoporotic spine fixation. J. Clin. Orthop. Trauma 2020, 11, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Weng, F.; Wang, J.; Yang, L.; Zeng, J.; Chu, Y.; Tian, Z. Application value of expansive pedicle screw in the lumbar short-segment fixation and fusion for osteoporosis patients. Exp. Ther. Med. 2018, 16, 665–670. [Google Scholar] [CrossRef]
- Oh, K.W.; Lee, J.H.; Lee, J.H.; Lee, D.Y.; Shim, H.J. The correlation between cage subsidence, bone mineral density, and clinical results in posterior lumbar interbody fusion. Clin. Spine Surg. 2017, 30, E683–E689. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.J.; Tang, Y.C.; Zhou, T.P.; Guo, H.Z.; Guo, D.Q.; Mo, G.Y.; Ma, Y.H.; Liu, P.J.; Zhang, S.C.; Liang, D. Risk factor analysis of the incidence of subsequent adjacent vertebral fracture after lumbar spinal fusion surgery with instrumentation. World Neurosurg. 2020, 135, e87–e93. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.-J.; Chen, W.-C.; Lu, M.-L.; Cheng, C.-H.; Niu, C.-C. Comparison of paraspinal muscle degeneration and decompression effect between conventional open and minimal invasive approaches for posterior lumbar spine surgery. Sci. Rep. 2020, 10, 14635. [Google Scholar] [CrossRef] [PubMed]
- Meng, B.; Bunch, J.; Burton, D.; Wang, J. Lumbar interbody fusion: Recent advances in surgical techniques and bone healing strategies. Eur. Spine J. 2020, 30, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.R.; Smith, B.W.; Liu, X.; Park, P. Current applications of robotics in spine surgery: A systematic review of the litera-ture. Neurosurg. Focus 2017, 42, E2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbusera, F.; Volkheimer, D.; Reitmaier, S.; Berger-Roscher, N.; Kienle, A.; Wilke, H.J. Pedicle screw loosening: A clinically relevant complication? Eur. Spine J. 2015, 24, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, C.L.; Brodke, D.S.; Choma, T.J. Surgical Management of Spinal Conditions in the Elderly Osteoporotic Spine. Neurosurgery 2015, 77, S98–S107. [Google Scholar] [CrossRef] [PubMed]
- Rometsch, E.; Spruit, M.; Zigler, J.E.; Menon, V.K.; Ouellet, J.A.; Mazel, C.; Härtl, R.; Espinoza, K.; Kandziora, F. Screw-related complications after instrumentation of the osteoporotic spine: A systematic literature review with me-ta-analysis. Glob. Spine J. 2020, 10, 69–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.H.; Hwang, C.J.; Kim, H.; Joo, Y.-S.; Lee, D.-H.; Lee, C.S. Effect of osteoporosis on the clinical and radiological outcomes following one-level posterior lumbar interbody fusion. J. Orthop. Sci. 2018, 23, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Chung, C.K. Strategies of Spinal Fusion on Osteoporotic Spine. J. Korean Neurosurg. Soc. 2011, 49, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Mo, G.; Guo, H.; Guo, D.; Tang, Y.; Li, Y.; Yuan, K.; Luo, P.; Zhou, T.; Zhang, S.; Liang, D. Augmented pedicle trajectory applied on the osteoporotic spine with lumbar degenerative dis-ease: Mid-term outcome. J. Orthop. Surg. Res. 2019, 14, 170. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.; Su, Y.; Kuo, K.; Ko, H.; Su, H.; Wu, C.; Chou, Y.; Lin, C.; Tsai, T. Minimally Invasive Transforaminal Lumbar Interbody Fusion for 2-Level Degenerative Lumbar Disease in Pa-tients With Osteoporosis: Long-Term Clinical and Radiographic Outcomes. Oper. Neurosurg. 2021, 20, 535–540. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| No. | Age (Years) | Sex | T-Score | BMI | Follow-Up (Months) | Screw- Loosening | Cage Fusion |
|---|---|---|---|---|---|---|---|
| 1 | 73 | F | −2.9 | 27.2 | 87 | − | + |
| 2 | 57 | F | −4 | 20.9 | 14 | − | + |
| 3 | 71 | F | −4.3 | 23.8 | 59 | − | + |
| 4 | 62 | F | −3.7 | 26.6 | 53 | − | + |
| 5 | 78 | F | −3 | 25.1 | 55 | − | + |
| 6 | 63 | F | −3.9 | 21 | 20 | − | + |
| 7 | 78 | F | −3.1 | 31 | 50 | − | + |
| 8 | 77 | F | −3.6 | 20.9 | 11.5 | − | + |
| 9 | 61 | F | −4 | 28 | 54 | − | + |
| 10 | 70 | M | −3.5 | 20.3 | 57 | 3 screws | + |
| 11 | 64 | F | −2.9 | 19.3 | 73 | − | + |
| 12 | 72 | F | −3.1 | 39.9 | 13 | 2 screws | − |
| 13 | 74 | F | −3.7 | 35.1 | 40 | − | + |
| 14 | 62 | M | −3 | 24.6 | 46 | − | + |
| 15 | 62 | M | −3.2 | 23.2 | 12 | − | + |
| 16 | 81 | F | −2.8 | 21.2 | 18 | 2 screws | − |
| 17 | 68 | F | −2.6 | 22.2 | 69 | 4 screws | + |
| 18 | 70 | F | −2.7 | 29.8 | 49 | − | + |
| 19 | 68 | F | −2.6 | 27 | 39 | − | + |
| Average (cm) | Average (cm) | |||
|---|---|---|---|---|
| Adjacent anterior 1/3 | Preoperative | 3.1647 | Postoperative | 3.1426 |
| Adjacent middle 1/3 | Preoperative | 3.2058 | Postoperative | 3.15 |
| Adjacent posterior 1/3 | Preoperative | 3.2174 | Postoperative | 3.2237 |
| First fixation segment anterior 1/3 | Preoperative | 3.1532 | Postoperative | 3.1479 |
| First fixation segment middle 1/3 | Preoperative | 3.1774 | Postoperative | 3.0005 |
| First fixation segment posterior 1/3 | Preoperative | 3.1332 | Postoperative | 2.9395 |
| Second fixation segment anterior 1/3 | Preoperative | 3.0974 | Postoperative | 3.0242 |
| Second fixation segment middle 1/3 | Preoperative | 3.0458 | Postoperative | 2.9758 |
| Second fixation segment posterior 1/3 | Preoperative | 2.8668 | Postoperative | 2.8489 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, H.-Y.; Ko, H.-J.; Su, Y.-F.; Lieu, A.-S.; Lin, C.-L.; Chang, C.-H.; Tsai, T.-H.; Tsai, C.-Y. Prevention of Compression Fracture in Osteoporosis Patients under Minimally Invasive Trans-Foraminal Lumbar Interbody Fusion with Assistance of Bone-Mounted Robotic System in Two-Level Degenerative Lumbar Disease. Medicina 2022, 58, 688. https://doi.org/10.3390/medicina58050688
Su H-Y, Ko H-J, Su Y-F, Lieu A-S, Lin C-L, Chang C-H, Tsai T-H, Tsai C-Y. Prevention of Compression Fracture in Osteoporosis Patients under Minimally Invasive Trans-Foraminal Lumbar Interbody Fusion with Assistance of Bone-Mounted Robotic System in Two-Level Degenerative Lumbar Disease. Medicina. 2022; 58(5):688. https://doi.org/10.3390/medicina58050688
Chicago/Turabian StyleSu, Hui-Yuan, Huey-Jiun Ko, Yu-Feng Su, Ann-Shung Lieu, Chih-Lung Lin, Chih-Hui Chang, Tai-Hsin Tsai, and Cheng-Yu Tsai. 2022. "Prevention of Compression Fracture in Osteoporosis Patients under Minimally Invasive Trans-Foraminal Lumbar Interbody Fusion with Assistance of Bone-Mounted Robotic System in Two-Level Degenerative Lumbar Disease" Medicina 58, no. 5: 688. https://doi.org/10.3390/medicina58050688
APA StyleSu, H.-Y., Ko, H.-J., Su, Y.-F., Lieu, A.-S., Lin, C.-L., Chang, C.-H., Tsai, T.-H., & Tsai, C.-Y. (2022). Prevention of Compression Fracture in Osteoporosis Patients under Minimally Invasive Trans-Foraminal Lumbar Interbody Fusion with Assistance of Bone-Mounted Robotic System in Two-Level Degenerative Lumbar Disease. Medicina, 58(5), 688. https://doi.org/10.3390/medicina58050688