
Neurophysiological Effects of a Singing Bowl Massage


Abstract
1. Introduction
2. Materials and Methods
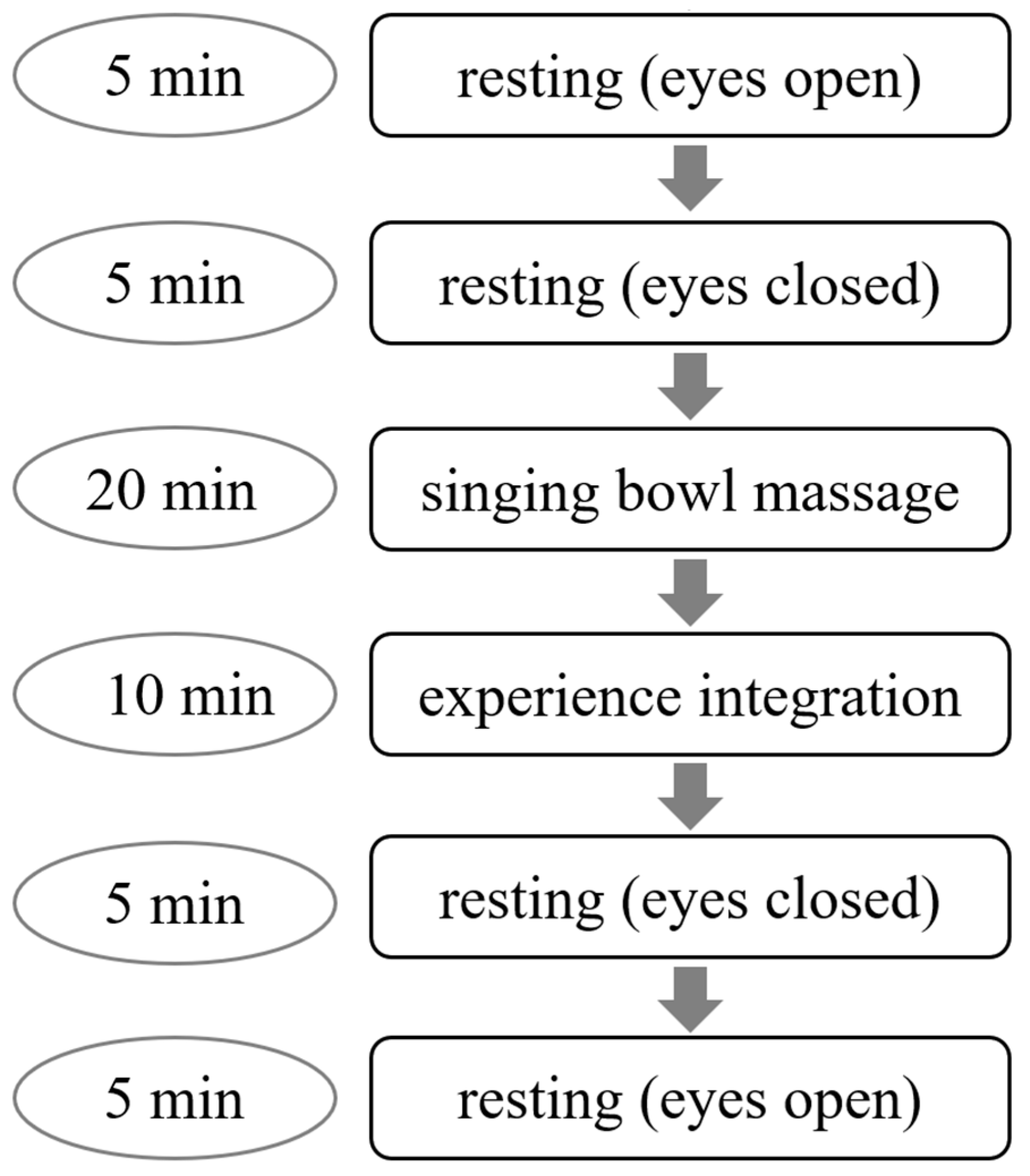
2.1. Data Acquisition and Participants
2.2. Data Processing
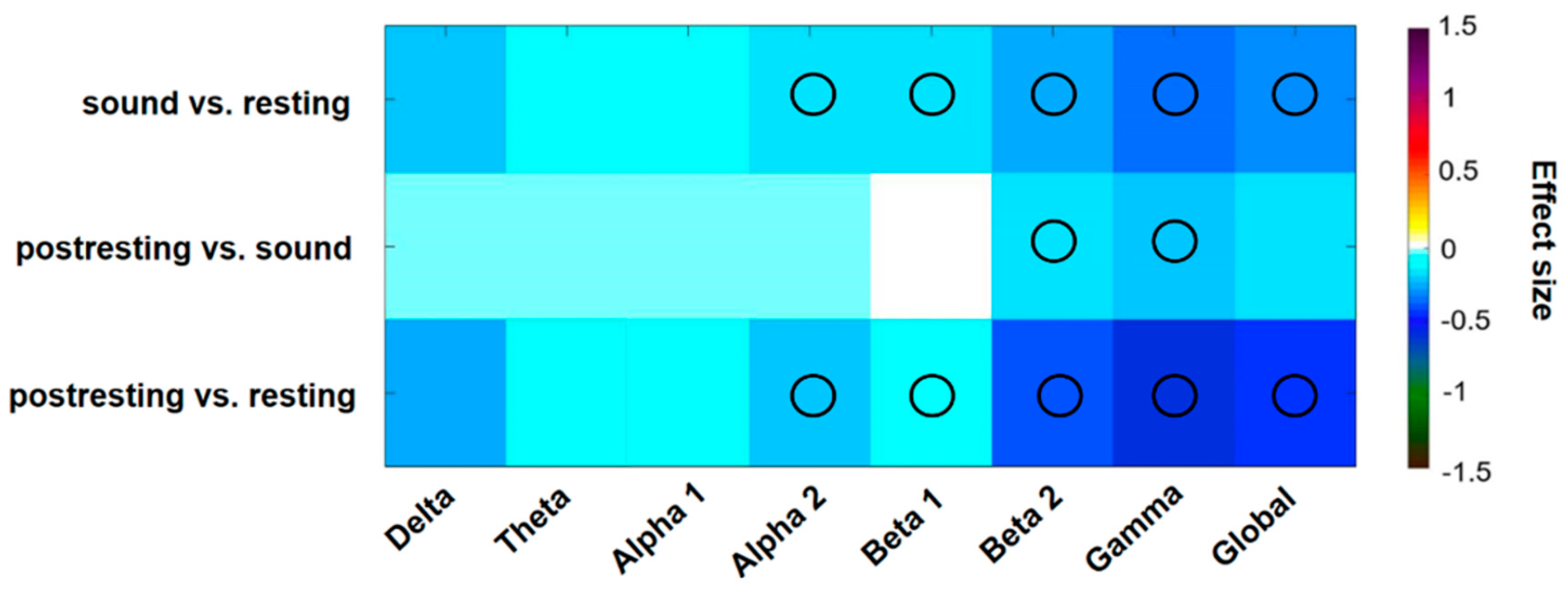
- sound vs. resting (eyes closed)
- postresting (eyes closed) vs. sound
- postresting (eyes closed) vs. resting (eyes closed)
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldsby, T.L.; Goldsby, M.E. Eastern Integrative Medicine and Ancient Sound Healing Treatments for Stress: Recent Research Advances. Integr. Med. 2020, 19, 24–30. [Google Scholar]
- Stegemann, T.; Geretsegger, M.; Phan Quoc, E.; Riedl, H.; Smetana, M. Music Therapy and Other Music-Based Interventions in Pediatric Health Care: An Overview. Medicines 2019, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Aalbers, S.; Fusar-Poli, L.; Freeman, R.E.; Spreen, M.; Ket, J.C.; Vink, A.C.; Maratos, A.; Crawford, M.; Chen, X.-J.; Gold, C. Music therapy for depression. Cochrane Database Syst. Rev. 2017, 11, CD004517. [Google Scholar] [CrossRef] [PubMed]
- Leubner, D.; Hinterberger, T. Reviewing the Effectiveness of Music Interventions in Treating Depression. Front. Psychol. 2017, 8, 1109. [Google Scholar] [CrossRef]
- Tang, Q.; Huang, Z.; Zhou, H.; Ye, P. Effects of music therapy on depression: A meta-analysis of randomized controlled trials. PLoS ONE 2020, 15, e0240862. [Google Scholar] [CrossRef]
- Kamioka, H.; Tsutani, K.; Yamada, M.; Park, H.; Okuizumi, H.; Tsuruoka, K.; Honda, T.; Okada, S.; Park, S.-J.; Kitayuguchi, J.; et al. Effectiveness of music therapy: A summary of systematic reviews based on randomized controlled trials of music interventions. Patient Prefer. Adherence 2014, 8, 727–754. [Google Scholar] [CrossRef]
- Raglio, A.; Attardo, L.; Gontero, G.; Rollino, S.; Groppo, E.; Granieri, E. Effects of music and music therapy on mood in neurological patients. World J. Psychiatry 2015, 5, 68–78. [Google Scholar] [CrossRef]
- van Criekinge, T.; D’Août, K.; O’Brien, J.; Coutinho, E. The Influence of Sound-Based Interventions on Motor Behavior After Stroke: A Systematic Review. Front. Neurol. 2019, 10, 1141. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Lipworth, L.; Burney, R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J. Behav. Med. 1985, 8, 163–190. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr. Clin. North Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Stanhope, J.; Weinstein, P. The human health effects of singing bowls: A systematic review. Complement. Ther. Med. 2020, 51, 102412. [Google Scholar] [CrossRef] [PubMed]
- Landry, J.M. Physiological and psychological effects of a Himalayan singing bowl in meditation practice: A quantitative analysis. Am. J. Health Promot. 2014, 28, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Goldsby, T.L.; Goldsby, M.E.; McWalters, M.; Mills, P.J. Effects of Singing Bowl Sound Meditation on Mood, Tension, and Well-being: An Observational Study. J. Evid. Based Complementary Altern. Med. 2017, 22, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Hess, P. (Ed.) Peter-Hess-Klangmethoden im Kontext von Forschung und Wissenschaft; Hess: Schüttorf, Germany, 2010; ISBN 978-3-938263-19-8. [Google Scholar]
- Tellegen, A.; Atkinson, G. Openness to absorbing and self-altering experiences (“absorption”), a trait related to hypnotic susceptibility. J. Abnorm. Psychol. 1974, 83, 268–277. [Google Scholar] [CrossRef]
- Hinterberger, T.; Walter, N. Rhythmic Mechanical Body Stimulation Improves Physical and Mental Wellbeing and Alters States of Consciousness. AJBSR 2020, 9, 132–136. [Google Scholar] [CrossRef]
- Hinterberger, T.; Kübler, A.; Kaiser, J.; Neumann, N.; Birbaumer, N. A brain–computer interface (BCI) for the locked-in: Comparison of different EEG classifications for the thought translation device. Clin. Neurophysiol. 2003, 114, 416–425. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. ISBN 978113474 2707.
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Keng, S.-L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef]
- Hinterberger, T.; Schmidt, S.; Kamei, T.; Walach, H. Decreased electrophysiological activity represents the conscious state of emptiness in meditation. Front. Psychol. 2014, 5, 99. [Google Scholar] [CrossRef]
- Chang, K.-M.; Lo, P.-C. Meditation EEG interpretation based on novel fuzzy-merging strategies and wavelet features. Biomed. Eng. Appl. Basis Commun. 2005, 17, 167–175. [Google Scholar] [CrossRef][Green Version]
- Dor-Ziderman, Y.; Berkovich-Ohana, A.; Glicksohn, J.; Goldstein, A. Mindfulness-induced selflessness: A MEG neurophenomenological study. Front. Hum. Neurosci. 2013, 7, 582. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Panchal, S.; Irani, F.; Trivedi, G.Y. Impact of Himalayan Singing Bowls Meditation Session on Mood and Heart Rate Variability—An Observational Study. IJPR 2019, 1, 20–30. [Google Scholar] [CrossRef]
- Bergmann, M.; Riedinger, S.; Stefani, A.; Mitterling, T.; Holzknecht, E.; Grassmayr, P.; Högl, B. Effects of singing bowl exposure on Karolinska sleepiness scale and pupillographic sleepiness test: A randomised crossover study. PLoS ONE 2020, 15, e0233982. [Google Scholar] [CrossRef]
- Cotoia, A.; Dibello, F.; Moscatelli, F.; Sciusco, A.; Polito, P.; Modolo, A.; Gallo, C.; Cibelli, G.; Cinnella, G. Effects of Tibetan Music on Neuroendocrine and Autonomic Functions in Patients Waiting for Surgery: A Randomized, Controlled Study. Anesthesiol. Res. Pract. 2018, 2018, 9683780. [Google Scholar] [CrossRef]
- Trivedi, G.Y.; Saboo, B. A Comparative Study of the Impact of Himalayan Singing Bowls and Supine Silence on Stress Index and Heart Rate Variability. JBTM 2018, 2, 40–50. [Google Scholar] [CrossRef]
- Menzies, V.; Taylor, A.G.; Bourguignon, C. Absorption: An individual difference to consider in mind-body interventions. J. Holist. Nurs. 2008, 26, 297–302. [Google Scholar] [CrossRef]
- Menzies, V.; Taylor, A.G.; Bourguignon, C. Effects of guided imagery on outcomes of pain, functional status, and self-efficacy in persons diagnosed with fibromyalgia. J. Altern. Complement. Med. 2006, 12, 23–30. [Google Scholar] [CrossRef]
- Wepner, F.; Hahne, J.; Teichmann, A.; Berka-Schmid, G.; Hördinger, A.; Friedrich, M. Quarzklangschalentherapie bei Wirbelsäulenbeschwerdenund chronobiologische Vorgänge-eine randomisiertekontrollierte Studie. Forsch. Komplementmed. 2008, 15, 130–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Resting [Mean (SD)] | Sound [Mean (SD)] | Postresting [Mean (SD)] | Comparison (p-Value) |
|---|---|---|---|---|
| HR [bmp] | 75.5 (19.8) | 71.3 (17.0) | 71.5 (17.9) | <0.001 * |
| SDNN [ms] | 68.5 (36.0) | 68.3 (34.5) | 73.0 (43.3) | 0.152 |
| RMSSD [ms] | 52.4 (34.6) | 54.5 (34.6) | 55.7 (38.7) | 0.057 |
| LF power [%] | 41.6 (19.6) | 36.7 (14.1) | 39.0 (18.0) | 0.203 |
| HF power [%] | 21.8 (13.1) | 25.0 (14.1) | 21.9 (13.2) | 0.717 |
| Respiration rate | 13.5 (5.3) | 14.0 (6.5) | 15.2 (6.3) | 0.018 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walter, N.; Hinterberger, T. Neurophysiological Effects of a Singing Bowl Massage. Medicina 2022, 58, 594. https://doi.org/10.3390/medicina58050594
Walter N, Hinterberger T. Neurophysiological Effects of a Singing Bowl Massage. Medicina. 2022; 58(5):594. https://doi.org/10.3390/medicina58050594
Chicago/Turabian StyleWalter, Nike, and Thilo Hinterberger. 2022. "Neurophysiological Effects of a Singing Bowl Massage" Medicina 58, no. 5: 594. https://doi.org/10.3390/medicina58050594
APA StyleWalter, N., & Hinterberger, T. (2022). Neurophysiological Effects of a Singing Bowl Massage. Medicina, 58(5), 594. https://doi.org/10.3390/medicina58050594