
The Effects of Exercise Habit on Albuminuria and Metabolic Indices in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Locations
2.2. Research Tools
2.3. Sample Size and Statistical Methods
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.-A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; DCCT/EDIC Research Group. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: Overview. Diabetes Care 2014, 37, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Ley, S.-H.; Hu, F.-B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Ahlqvist, E.; Prasad, R.-B.; Groop, L. 100 years of insulin: Towards improved precision and a new classification of diabetes mellitus. J. Endocrinol. 2021, 252, R59–R70. [Google Scholar] [CrossRef] [PubMed]
- Lee-Ødegård, S.; Olsen, T.; Norheim, F.; Drevon, C.A.; Birkeland, K.I. Potential mechanisms for how long-term physical activity may reduce insulin resistance. Metabolites 2022, 12, 208. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 17. Diabetes advocacy: Standards of medical care in diabetes-2022. Diabetes Care 2022, 45 (Suppl. 1), S254–S255. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2021. Diabetes Care 2021, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 diabetes and its impact on the immune system. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Tu, S.-T.; Sheu, W.-H. 2019 Diabetes Atlas: Achievements and challenges in diabetes care in Taiwan. J Formos Med Assoc. 2019, 118 (Suppl. 2), S130–S134. [Google Scholar] [CrossRef]
- Mooradian, A.-D. Dyslipidemia in type 2 diabetes mellitus. Nat Clin Pract Endocrinol Metab. 2009, 5, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Du, R. Study of the physiological effects of bicycle exercise on the body’s metabolism. J. Des. Environ. 2014, 15, 1–14. [Google Scholar]
- Varghese, R.-T.; Jialal, I. Diabetic nephropathy. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Colberg, S.-R.; Sigal, R.-J.; Yardley, J.-E.; Riddell, M.-C.; Dunstan, D.-W.; Dempsey, P.-C.; Horton, E.-S.; Castorino, K.; Tate, D.-F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care. 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanuso, S.; Jimenez, A.; Pugliese, G.; Corigliano, G.; Balducci, S. Exercise for the management of type 2 diabetes: A review of the evidence. Acta Diabetol. 2010, 47, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Stensvold, D.; Tjønna, A.E.; Skaug, E.A.; Aspenes, S.; Stølen, T.; Wisløff, U.; Slørdahl, S.A. Strength training versus aerobic interval training to modify risk factors of metabolic syndrome. J. Appl. Physiol. 2010, 108, 804–810. [Google Scholar] [CrossRef] [Green Version]
- Larose, J.; Sigal, R.-J.; Khanwala, F.; Prud’homme, D.; Boulé, N.-G.; Kenny, G.-P. Associations between physical fitness and HbA1C in chronic diabetes mellitus. Diabetologia 2011, 54, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Johansen, K.-L.; Painter, P. Exercise in individuals with CKD. Am. J. Kidney Dis. 2012, 59, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wang, Y.; Xiong, L.; Luo, Y.; Huang, Z.; Yi, B. Exercise therapy improves eGFR, and reduces blood pressure and BMI in non-dialysis CKD patients: Evidence from a meta-analysis. BMC Nephrol. 2019, 20, 398. [Google Scholar] [CrossRef]
- Calculate Sample Size Needed to Compare 2 Means: 2-Sample Equivalence. Available online: http://powerandsamplesize.com/Calculators/Compare-2-Means/2-Sample-Non-Inferiority-or-Superiority (accessed on 16 February 2022).
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R. Risk factors for renal dysfunction in type 2 diabetes: UK prospective diabetes study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.; Huang, P.; Qu, H.; Liu, C.; Chen, B.; Gao, M. The effect of healthy eating courses and voluntary exercise offered in the community on hyperlipidaemia. Taipei City Med. J. 2011, 8, 36–44. [Google Scholar]
- American Diabetes Association. Standards of Medical Care in Diabetes. Available online: http://care.diabetesjournals.org/content/41/Supplement_1/S38 (accessed on 16 February 2022).
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.-R.; Bakris, G.; Benson, G.; Brown, F.-M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. 2. classification and diagnosis of diabetes: Standards of medical care in diabetes-2022. Diabetes Care 2022, 45 (Suppl. 1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, M.-J.; Bennett, P.-N.; Fraser, S.-F.; Warmington, S.-A. Exercise interventions for improving objective physical function in patients with end-stage kidney disease on dialysis: A systematic review and meta-analysis. Am. J. Physiol. Renal Physiol. 2019, 316, F856–F872. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Sasaki, T.; Yamamoto, S.; Hayashi, H.; Ako, S.; Tanaka, Y. Effects of exercise on kidney and physical function in patients with non-dialysis chronic kidney disease: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 18195. [Google Scholar] [CrossRef] [PubMed]
- Collister, D.; Ferguson, T.; Komenda, P.; Tangri, N. The Patterns, Risk Factors, and Prediction of Progression in Chronic Kidney Disease: A Narrative Review. Semin Nephrol. 2016, 36, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, P.-J.; Lin, H.-C.; Chang, S.-T.; Hsu, J.-T.; Lin, W.-S.; Chung, C.-M.; Chang, J.-J.; Hung, K.-C.; Shih, Y.-W.; Chen, F.-C.; et al. Albuminuria and neck circumference are determinate factors of successful accurate estimation of glomerular filtration rate in high cardiovascular risk patients. PLoS ONE 2018, 13, e0185693. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-C.; Liao, M.-T.; Hsiao, P.-J.; Lu, C.-L.; Hsu, Y.-J.; Lu, K.-C.; Chu, P. Antiproteinuria effect of calcitriol in patients with chronic kidney disease and vitamin D deficiency: A randomized controlled study. J. Ren. Nutr. 2020, 30, 200–207. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Cravedi, P.; Remuzzi, G. Mechanisms and treatment of CKD. J. Am. Soc. Nephrol. 2012, 23, 1917–1928. [Google Scholar] [CrossRef] [Green Version]
- Stevens, P.-E.; Levin, A. Kidney disease: Improving global outcomes chronic kidney disease guideline development work group members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Heiwe, S.; Jacobson, S.-H. Exercise training for adults with chronic kidney disease. Cochrane Database Syst. Rev. 2011, 10, CD003236. [Google Scholar] [CrossRef]
- Heiwe, S.; Jacobson, S.-H. Exercise training in adults with CKD: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 64, 383–393. [Google Scholar] [CrossRef]
- Pei, G.; Tang, Y.; Tan, L.; Tan, J.; Ge, L.; Qin, W. Aerobic exercise in adults with chronic kidney disease (CKD): A meta-analysis. Int. Urol. Nephrol. 2019, 51, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.; Joshi, A.; Hise, M.-K. Association of physical activity and renal function in subjects with and without metabolic syndrome: A review of the third National Health and nutrition examination survey (NHANES III). Am. J. Kidney Dis. 2006, 48, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.-S.; Fisher, N.-D.; Forman, J.-P.; Curhan, G.-C. Physical activity and albuminuria. Am. J. Epidemiol. 2010, 171, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshinnia, F.; Wilt, T.-J.; Duval, S.; Esmaeili, A.; Ibrahim, H.-N. Weight loss and proteinuria: Systematic review of clinical trials and comparative cohorts. Nephrol. Dial. Transplant. 2010, 25, 1173–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glavinovic, T.; Ferguson, T.; Komenda, P.; Rigatto, C.; Duhamel, T.-A.; Tangri, N.; Bohm, C. CKD and sedentary time: Results from the Canadian health measures survey. Am. J. Kidney Dis. 2018, 72, 529–537. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Exercise Group (n = 106) | Non-Exercise Group (n = 123) | p |
|---|---|---|---|
| Gender | 0.931 | ||
| Female | 61 (57.5) | 69 (56.1) | |
| Male | 45 (42.5) | 54 (43.9) | |
| Age (years) | 66.2 ± 10.1 | 61.9 ± 12.8 | <0.05 ** |
| HbA1c (%) | 6.89± 0.69 | 7.16 ± 1.05 | <0.05 ** |
| FPG (mg/dL) | 121.9 ± 25.7 | 140.5 ± 42.4 | <0.05 ** |
| Cholesterol (mg/dL) | 158.3 ± 27.2 | 158.5 ± 33.5 | 0.967 |
| TG (mg/dL) | 115.6 ± 53.6 | 150.2 ± 15.4 | <0.05 ** |
| Creatinine (mg/dL) | 0.81 ± 0.19 | 0.79 ± 0.19 | 0.628 |
| Uric acid (mg/dL) | 5.59 ± 1.35 | 5.85 ± 1.75 | 0.205 |
| HDL (mg/dL) | 50.3 ± 11.4 | 44.1 ± 9.26 | <0.05 ** |
| LDL (mg/dL) | 80.4 ± 21.6 | 84.1 ± 25.3 | 0.313 |
| UPCR (mg/gm) | 199.7 ± 36.4 | 244.6 ± 34.2 | 0.371 |
| UACR (mg/gm) | 7.66 ± 2.54 | 11.4 ± 2.41 | 0.285 |
| SBP (mmHg) | 130.9 ± 1.36 | 130.8 ± 1.31 | 0.955 |
| DBP (mmHg) | 76.8 ± 1.08 | 78.5 ± 1.18 | 0.287 |
| Albuminuria (mg/L) | 63.6 ± 196.0 | 112.0 ± 291.3 | 0.139 |
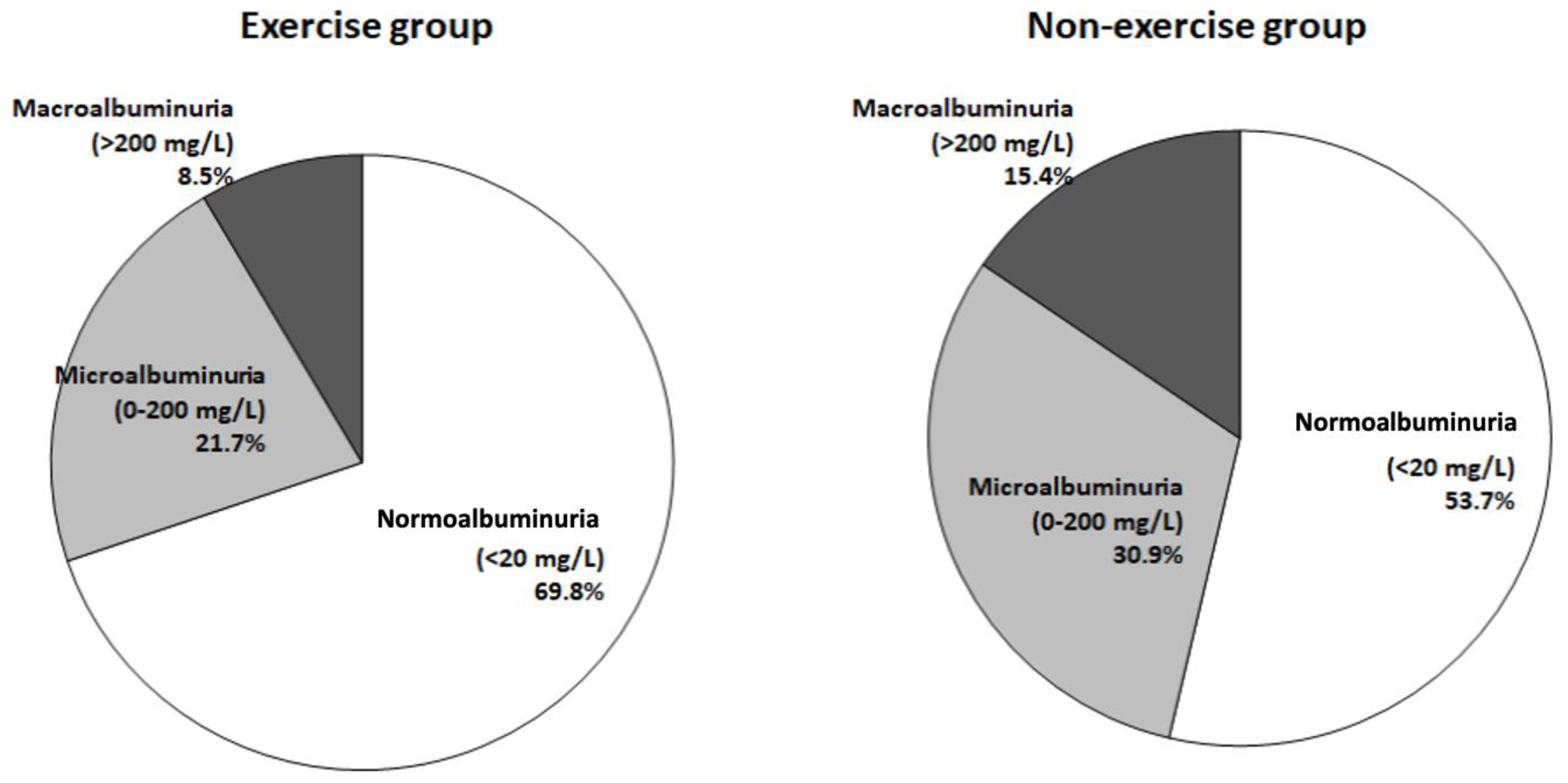
| Proteinuria Levels | Exercise Group (%) | Non-Exercise Group (%) | p |
|---|---|---|---|
| Normoalbuminuria (<20 mg/L) | 74 (69.8) | 66 (53.7) | <0.05 ** |
| Microalbuminuria (20–200 mg/L) | 23 (21.7) | 38 (30.9) | |
| Macroalbuminuria (>200 mg/L) | 9 (8.5) | 19 (15.4) |
| Variables | Normoalbuminuria (N = 140) | Microalbuminuria (N = 61) | Macroalbuminuria (N = 28) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Exercise (n = 74) | Non-Exercise (n = 66) | p | Exercise (n = 23) | Non-Exercise (n = 38) | p | Exercise (n = 9) | Non-Exercise (n = 19) | p | |
| HbA1c (%) | 6.81 ± 0.70 | 7.28 ± 1.06 | <0.05 ** | 7.04 ± 0.68 | 6.78 ± 0.99 | 0.452 | 7.49 ± 1.18 | 8.38 ± 1.57 | 0.169 |
| FPG (mg/dL) | 121.6 ± 26.8 | 143.0 ± 45.9 | <0.05 ** | 124.3± 18.1 | 129.3 ± 26.7 | 0.592 | 111.7 ± 53.0 | 154.4 ± 80.2 | 0.186 |
| Cholesterol (mg/dL) | 158.2 ± 27.6 | 157.1 ± 31.7 | 0.834 | 158.4 ± 25.8 | 157.5 ± 34.8 | 0.942 | 161.1 ± 40.6 | 178.8 ± 54.4 | 0.426 |
| TG (mg/dL) | 116.4 ± 54.9 | 132.8 ± 73.9 | 0.145 | 110.8 ± 46.1 | 169.2 ±28.6 | 0.148 | 105.8 ± 49.6 | 242.8 ± 214.8 | <0.05 ** |
| Uric acid (mg/dL) | 7.75 ± 18.3 | 5.77 ± 1.33 | 0.422 | 5.63 ± 1.17 | 5.60 ± 1.49 | 0.937 | 5.90 ± 1.78 | 5.96 ± 1.96 | 0.943 |
| Creatinine (mg/dL) | 0.83 ± 0.18 | 0.80 ± 0.19 | 0.327 | 0.69 ± 0.16 | 0.79 ± 0.17 | 0.101 | 0.91 ± 0.15 | 0.89 ± 0.15 | 0.827 |
| eGFR (mg/dL) | 89.7 ± 18.2 | 93.7 ± 21.4 | 0.242 | 100.7 ± 27.9 | 92.9 ± 20.1 | 0.385 | 79.9 ± 12.4 | 81.5 ± 14.6 | 0.800 |
| HDL (mg/dL) | 49.8 ± 11.6 | 43.9 ± 8.93 | <0.05 ** | 53.1 ± 10.4 | 45.7 ± 9.94 | 0.064 * | 52.1 ± 10.3 | 43.3 ± 10.7 | 0.064 * |
| LDL (mg/dL) | 80.9 ± 21.8 | 84.4 ± 23.1 | 0.366 | 77.7 ± 21.0 | 81.8 ± 26.8 | 0.667 | 80.3 ± 24.2 | 87.0 ± 29.5 | 0.580 |
| Variables | Normoalbuminuria (N = 140) | Microalbuminuria (N = 61) | Macroalbuminuria (N = 28) | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| HbA1c (%) | 0.85 (0.50–1.45) | 0.558 | 1.25 (0.61–2.58) | 0.543 | 0.72 (0.36–1.45) | 0.718 |
| FPG (mg/dL) | 0.99 (0.97–1.00) | 0.061 * | 0.99 (0.98–1.01) | 0.312 | 0.99 (0.98–1.01) | 0.312 |
| TG (mg/dL) | 1.00 (0.99–1.01) | 0.779 | 1.00 (0.99–1.01) | 0.203 | 1.02 (1.00–1.03) | <0.05 ** |
| HDL (mg/dL) | 1.06 (1.01–1.10) | <0.05 ** | 1.05 (0.99–1.12) | 0.133 | 1.24 (1.08–1.44) | <0.05 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, H.-Y.; Huang, Y.-H.; Wu, S.-W.; Chang, F.-H.; Tsuei, Y.-W.; Fan, H.-C.; Chiang, W.-F.; Hsiao, P.-J. The Effects of Exercise Habit on Albuminuria and Metabolic Indices in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Medicina 2022, 58, 577. https://doi.org/10.3390/medicina58050577
Kuo H-Y, Huang Y-H, Wu S-W, Chang F-H, Tsuei Y-W, Fan H-C, Chiang W-F, Hsiao P-J. The Effects of Exercise Habit on Albuminuria and Metabolic Indices in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Medicina. 2022; 58(5):577. https://doi.org/10.3390/medicina58050577
Chicago/Turabian StyleKuo, Hsin-Yi, Ya-Hui Huang, Su-Wen Wu, Feng-Hsun Chang, Yi-Wei Tsuei, Hsin-Chiung Fan, Wen-Fang Chiang, and Po-Jen Hsiao. 2022. "The Effects of Exercise Habit on Albuminuria and Metabolic Indices in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study" Medicina 58, no. 5: 577. https://doi.org/10.3390/medicina58050577
APA StyleKuo, H.-Y., Huang, Y.-H., Wu, S.-W., Chang, F.-H., Tsuei, Y.-W., Fan, H.-C., Chiang, W.-F., & Hsiao, P.-J. (2022). The Effects of Exercise Habit on Albuminuria and Metabolic Indices in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Medicina, 58(5), 577. https://doi.org/10.3390/medicina58050577