
Indication Criteria for Total Hip Arthroplasty in Patients with Hip Osteoarthritis—Recommendations from a German Consensus Initiative

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inauguration Workshop
- -
- No consensus, less than 50% agreement of the EKIT-Consensus-Panel;
- -
- Weak consensus, 50% to 74% agreement of the EKIT-Consensus-Panel;
- -
- Consensus, 75% to 94% agreement of the EKIT-Consensus-Panel;
- -
- Strong consensus, 95% or more agreement of the EKIT-Consensus-Panel [25].
2.2. Evidence Retrieval, Synthesis, and Derivation of Preliminary Recommendations
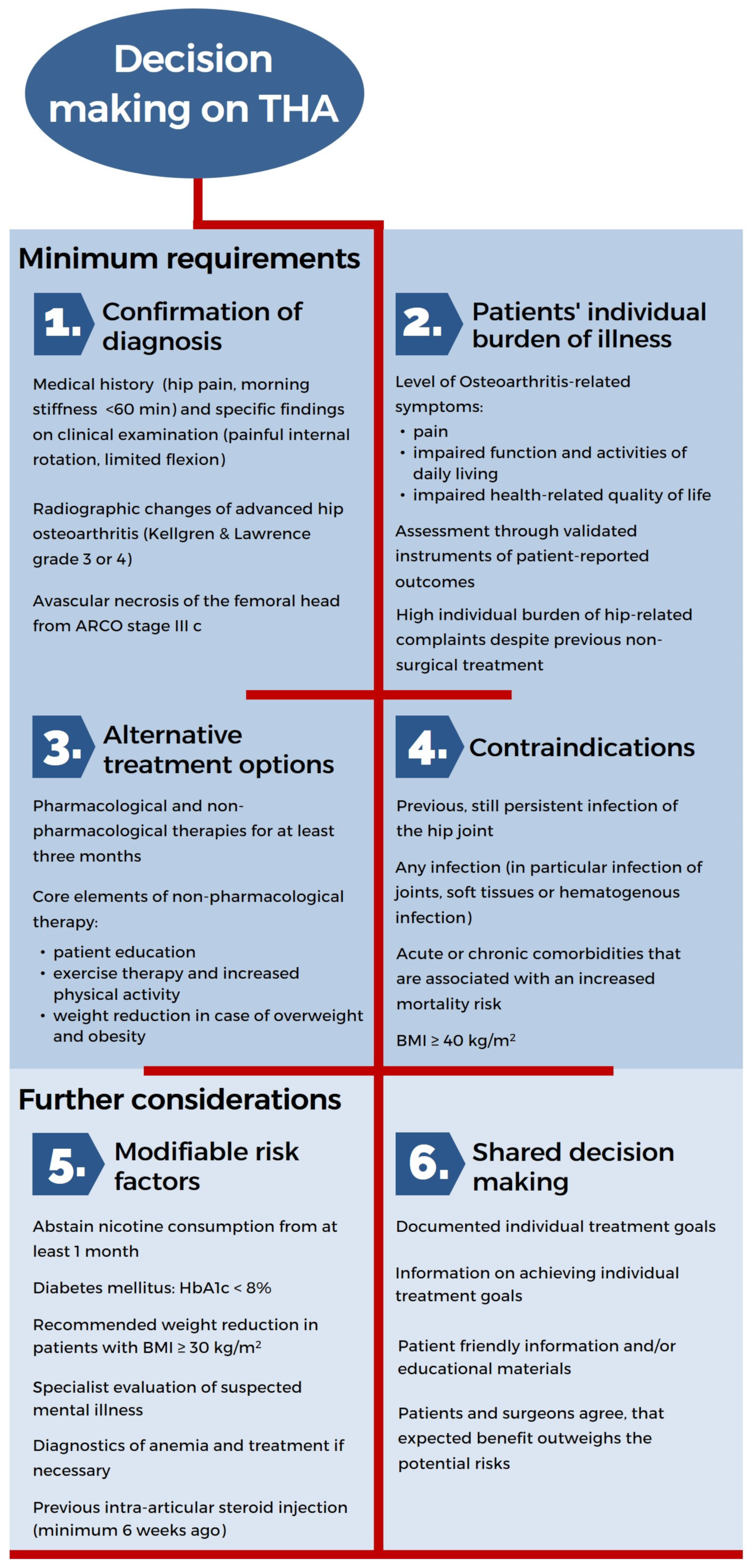
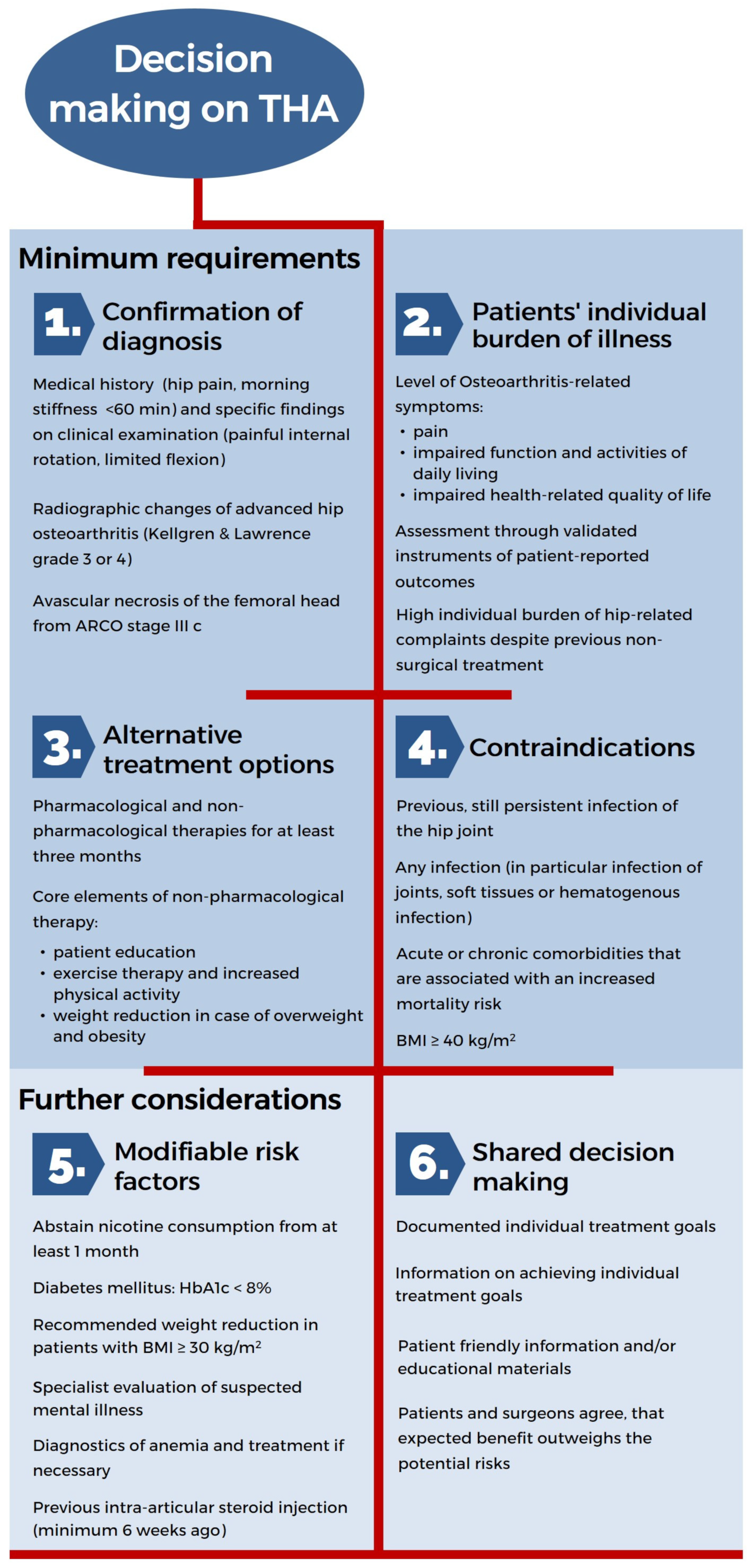
- (1)
- Confirmation of diagnosis;
- (2)
- Identification of a patient’s individual burden of illness;
- (3)
- Checking alternative treatment options;
- (4)
- Identification of contraindications;
- (5)
- Identification of modifiable risk factors;
- (6)
- Shared decision making.
2.3. EKIT-Consensus-Meeting
2.4. Development of a Checklist of Indication Criteria
3. Results
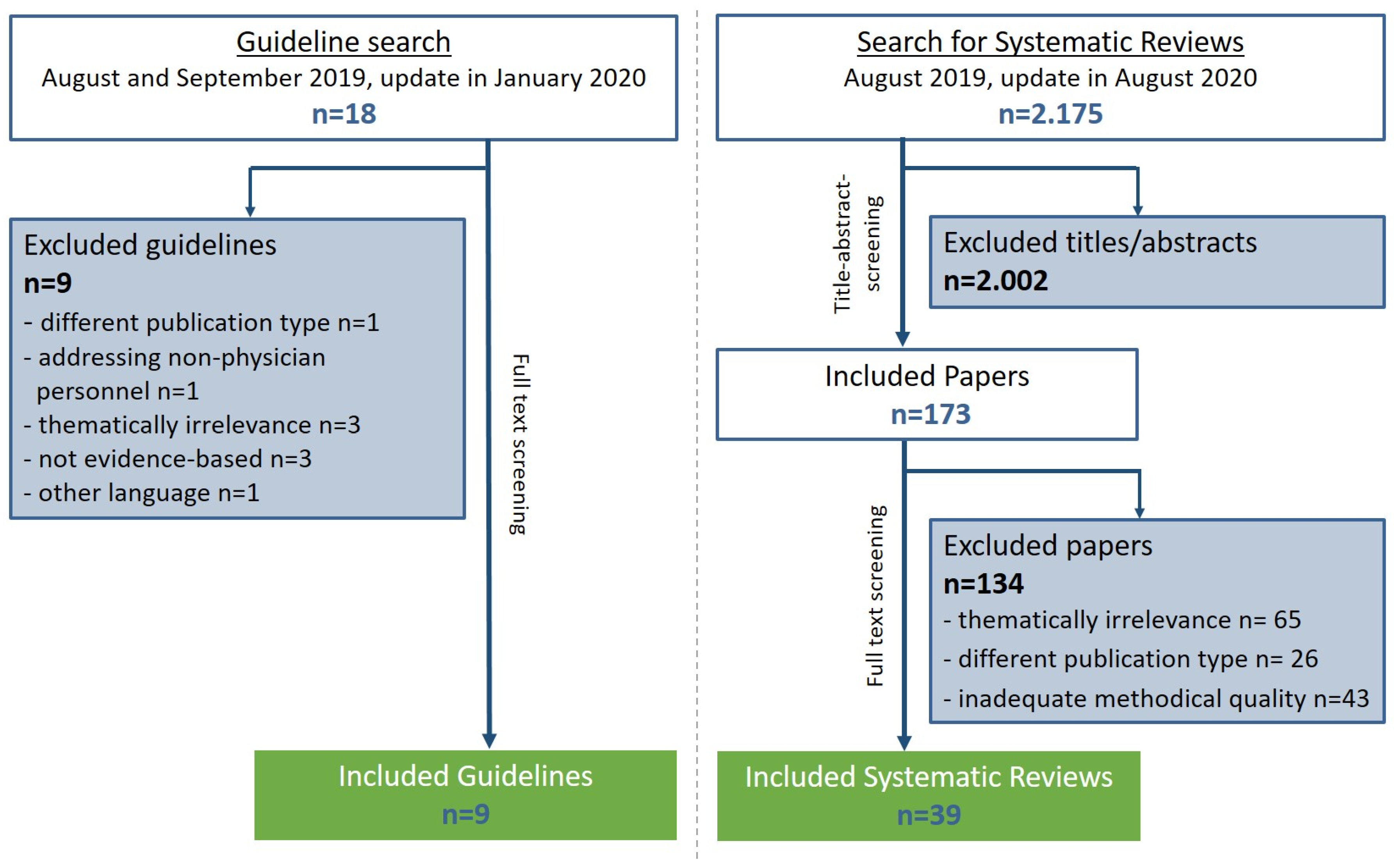
3.1. Evidence Retrieval
3.2. Consensus Voting
3.3. Development of a Checklist of Indication Criteria for THA in Hip OA
- (1)
- Ensure the diagnosis of hip OA via clinical examination and radiological signs;
- (2)
- Assess the patient’s individual burden of illness regarding hip-related complaints and health-related quality of life using validated measurement instruments;
- (3)
- Verify the use of alternative non-surgical therapies and their effectiveness during the last three months;
- (4)
- Confirm the absence of any contraindications.
- (5)
- Review of the medical implications regarding modifiable risk factors;
- (6)
- The patient’s individual treatment goals and the probability of their achievement.
4. Discussion
4.1. Main Findings
4.2. International Perspective
4.3. Clinical Considerations and Practical Implications
4.4. Strengths and Limitations
4.5. Implications for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Fernandes, L.; Hagen, K.B.; Bijlsma, J.W.J.; Andreassen, O.; Christensen, P.; Conaghan, P.; Doherty, M.; Geenen, R.; Hammond, A.; Kjeken, I.; et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann. Rheum. Dis. 2013, 72, 1125–1135. [Google Scholar] [CrossRef] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence (NICE). Osteoarthritis: Care and Management in Adults 2014. Available online: http://www.nice.org.uk/guidance/cg177 (accessed on 20 September 2019).
- Deutsche Gesellschaft für Orthopädie und Orthopädische Chirurgie (DGOOC). S2k-Leitlinie Koxarthrose (AWMF-Registernummer 033-001). 2019. Available online: https://www.awmf.org/leitlinien/detail/ll/033-001.html (accessed on 23 September 2019).
- Hermann, W.; Lambova, S.; Muller-Ladner, U. Current Treatment Options for Osteoarthritis. Curr. Rheumatol. Rev. 2018, 14, 108–116. [Google Scholar] [CrossRef]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Ferguson, R.J.; Palmer, A.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Institut für Qualitätssicherung und Transparenz im Gesundheitswesen (IQTIG). Qualitätsreport 2020. Available online: https://iqtig.org/downloads/berichte/2019/IQTIG_Qualitaetsreport-2020_2021-02-11.pdf (accessed on 26 July 2021).
- Ackerman, I.N.; Bohensky, M.A.; Zomer, E.; Tacey, M.; Gorelik, A.; Brand, C.A.; De Steiger, R. The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskelet. Disord. 2019, 20, 90. [Google Scholar] [CrossRef] [Green Version]
- Culliford, D.; Maskell, J.; Judge, A.; Cooper, C.; Prieto-Alhambra, D.; Arden, N.K.; COASt Study Group. Future projections of total hip and knee arthroplasty in the UK: Results from the UK Clinical Practice Research Datalink. Osteoarthr. Cartil. 2015, 23, 594–600. [Google Scholar] [CrossRef] [Green Version]
- Hooper, G.; Lee, A.J.-J.; Rothwell, A.; Frampton, C. Current trends and projections in the utilisation rates of hip and knee replacement in New Zealand from 2001 to 2026. N. Z. Med. J. 2014, 127, 82–93. [Google Scholar]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Nemes, S.; Gordon, M.; Rogmark, C.; Rolfson, O. Projections of total hip replacement in Sweden from 2013 to 2030. Acta Orthop. 2014, 85, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, A.B.; Johnsen, S.P.; Overgaard, S.; Soballe, K.; Sorensen, H.T.; Lucht, U. Total hip arthroplasty in Denmark: Incidence of primary operations and revisions during 1996–2002 and estimated future demands. Acta Orthop. 2005, 76, 182–189. [Google Scholar] [CrossRef]
- Pabinger, C.; Lothaller, H.; Portner, N.; Geissler, A. Projections of hip arthroplasty in OECD countries up to 2050. HIP Int. 2018, 28, 498–506. [Google Scholar] [CrossRef]
- Organisation Für Wirtschaftliche Zusammenarbeit und Entwicklung (OECD). Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Pabinger, C.; Geissler, A. Utilization rates of hip arthroplasty in OECD countries. Osteoarthr. Cartil. 2014, 22, 734–741. [Google Scholar] [CrossRef] [Green Version]
- Schäfer, T.; Pritzkuleit, R.; Jeszenszky, C.; Malzahn, J.; Maier, W.; Günther, K.; Niethard, F. Trends and geographical variation of primary hip and knee joint replacement in Germany. Osteoarthr. Cartil. 2013, 21, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Postler, A.; Lützner, C.; Lange, T.; Schmitt, J.; Lützner, J.; Günther, K.-P. Indikationsstellung zur Hüfttotalendoprothese—Die ärztliche Perspektive. Orthopäde 2021, 50, 278–286. [Google Scholar] [CrossRef]
- Gademan, M.G.J.; Hofstede, S.N.; Vlieland, T.P.M.V.; Nelissen, R.G.H.H.; De Mheen, P.J.M.-V. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet. Disord. 2016, 17, 463. [Google Scholar] [CrossRef] [Green Version]
- Deutsche Gesellschaft Für Orthopädie und Unfallchirurgie e.V. (DGOU). S3-Leitlinie “Evidenz- und Konsensbasierte Indikationskriterien zur Hüfttotalendoprothese bei Coxarthrose (EKIT-Hüfte)” (AWMF-Registernummer 187-001). Available online: https://www.awmf.org/leitlinien/detail/ll/187-001.html (accessed on 2 March 2022).
- Günther, K.P.; Deckert, S.; Lützner, C.; Lange, T.; Schmitt, J.; Postler, A. Hüfttotalendoprothese bei Coxarthrose—Evidenzbasierte und Patientenorientierte Indikationsstellung. Available online: https://www.aerzteblatt.de/archiv/221704/Huefttotalendoprothese-bei-Coxarthrose-evidenzbasierte-und-patientenorientierte-Indikationsstellung (accessed on 8 March 2022).
- Günther, K.P.; Deckert, S.; Lützner, C.; Lange, T.; Schmitt, J.; Postler, A. Total Hip Replacement for Osteoarthritis-Evidence-Based and Patient-Oriented Indications. Dtsch Arztebl Int. 2021, 118, 730–736. [Google Scholar] [CrossRef]
- Association of the Scientific Medical Societies in Germany (AWMF). AWMF-Regelwerk Leitlinien: Strukturierte Konsensfindung. Available online: https://www.awmf.org/leitlinien/awmf-regelwerk/ll-entwicklung/awmf-regelwerk-03-leitlinienentwicklung/ll-entwicklung-strukturierte-konsensfindung.html (accessed on 2 March 2022).
- Scottish Intercollegiate Guidelines Network (SIGN). Search Filters. Available online: https://www.sign.ac.uk/what-we-do/methodology/search-filters/ (accessed on 22 October 2020).
- Association of the Scientific Medical Societies in Germany (AWMF). German Instrument for Methodological Guideline Appraisal (DELBI). Available online: https://www.leitlinien.de/hintergrund/leitliniengrundlagen (accessed on 2 March 2022).
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, J.; Lange, T.; Günther, K.-P.; Kopkow, C.; Rataj, E.; Apfelbacher, C.; Aringer, M.; Böhle, E.; Bork, H.; Dreinhöfer, K.; et al. Indication Criteria for Total Knee Arthroplasty in Patients with Osteoarthritis—A Multi-perspective Consensus Study. Z. Orthop. Unf. 2017, 155, 539–548. [Google Scholar] [CrossRef]
- Royal Australian College of General Practitioners. Guideline for the Management of Knee and Hip Osteoarthritis. 2nd edn. Available online: http://www.acsep.org.au/content/Document/guideline-for-the-management-of-knee-and-hip-oa-2nd-edition.pdf (accessed on 20 September 2019).
- American Academy of Orthopaedic Surgeons (AAOS). Management of Osteoarthritis of the Hip. Evidence-Based Clinical Practice Guideline. Available online: https://aaos.org/globalassets/quality-and-practice-resources/osteoarthritis-of-the-hip/oa-hip-cpg_6-11-19.pdf (accessed on 23 September 2019).
- National Institute for Health and Care Excellence (NICE). Joint Replacement (Primary): Hip, Knee and Shoulder. Available online: https://www.nice.org.uk/guidance/ng157 (accessed on 2 March 2022).
- Lange, T.; Deckert, S.; Beyer, F.; Hahn, W.; Einhart, N.; Roessler, M.; Sedlmayr, M.; Schmitt, J.; Lützner, J. An individualized decision aid for physicians and patients for total knee replacement in osteoarthritis (Value-based TKR study): Study protocol for a multi-center, stepped wedge, cluster randomized controlled trial. BMC Musculoskelet. Disord. 2021, 22, 783. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lützner, C.; Deckert, S.; Günther, K.-P.; Postler, A.E.; Lützner, J.; Schmitt, J.; Limb, D.; Lange, T. Indication Criteria for Total Hip Arthroplasty in Patients with Hip Osteoarthritis—Recommendations from a German Consensus Initiative. Medicina 2022, 58, 574. https://doi.org/10.3390/medicina58050574
Lützner C, Deckert S, Günther K-P, Postler AE, Lützner J, Schmitt J, Limb D, Lange T. Indication Criteria for Total Hip Arthroplasty in Patients with Hip Osteoarthritis—Recommendations from a German Consensus Initiative. Medicina. 2022; 58(5):574. https://doi.org/10.3390/medicina58050574
Chicago/Turabian StyleLützner, Cornelia, Stefanie Deckert, Klaus-Peter Günther, Anne Elisabeth Postler, Jörg Lützner, Jochen Schmitt, David Limb, and Toni Lange. 2022. "Indication Criteria for Total Hip Arthroplasty in Patients with Hip Osteoarthritis—Recommendations from a German Consensus Initiative" Medicina 58, no. 5: 574. https://doi.org/10.3390/medicina58050574
APA StyleLützner, C., Deckert, S., Günther, K.-P., Postler, A. E., Lützner, J., Schmitt, J., Limb, D., & Lange, T. (2022). Indication Criteria for Total Hip Arthroplasty in Patients with Hip Osteoarthritis—Recommendations from a German Consensus Initiative. Medicina, 58(5), 574. https://doi.org/10.3390/medicina58050574