Towards an International Consensus on the Prevention, Treatment, and Management of High-Risk Substance Use and Overdose among Youth

 , ,
, ,  , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Panel Selection
2.2. Delphi Process
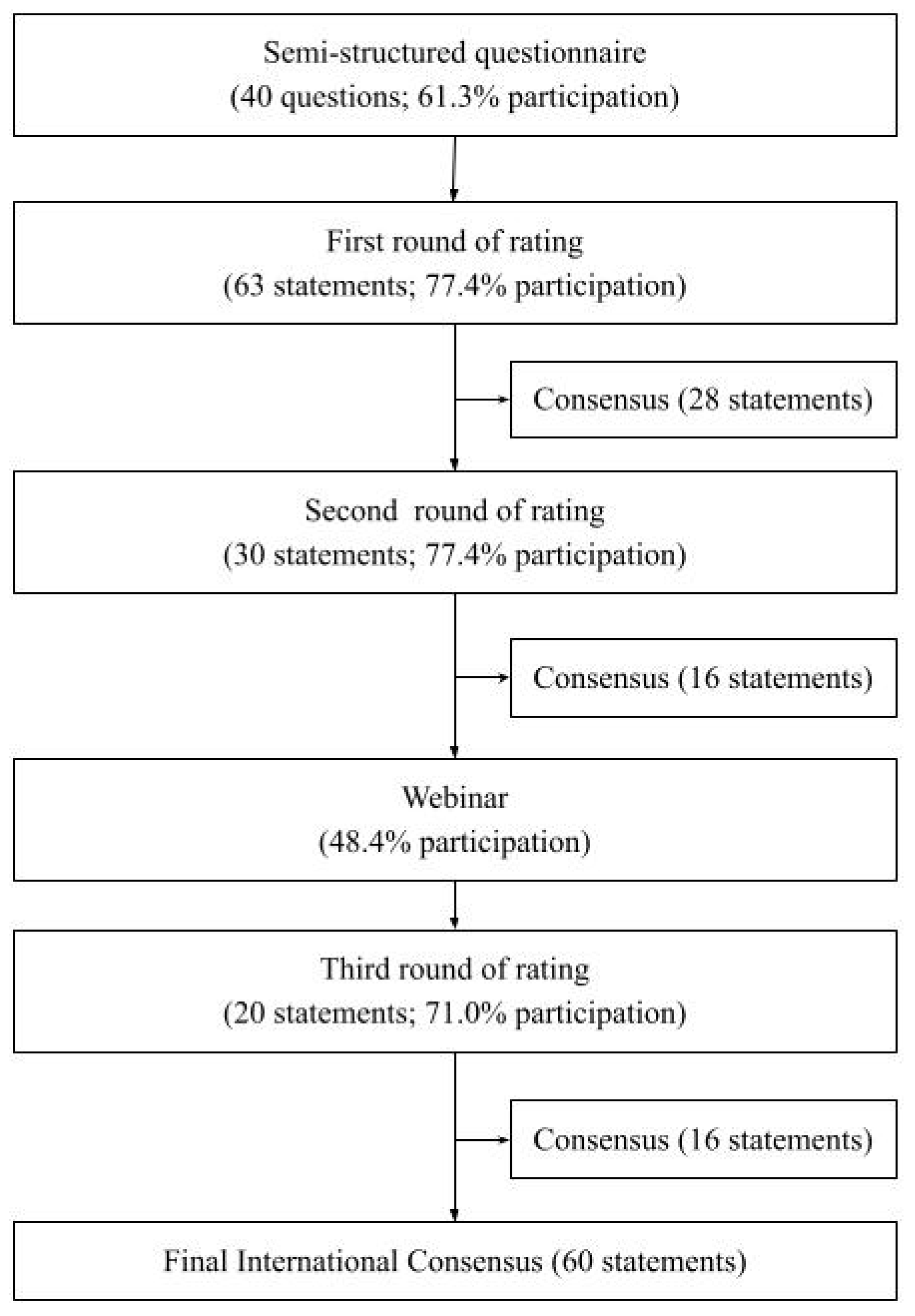
- A semi-structured questionnaire was constructed and organized into the following five domains with corresponding actionable goals: (a) outlining clinical risk, (b) determining target populations, (c) defining intervention goals, (d) recognizing evidence-based intervention strategies, (e) identifying appropriate treatment setting and expertise. The domains were identified through a non-systematic review of the literature and a published narrative literature review on treatment approaches for youth with high-risk opioid use and OUD [25]. Though the narrative literature review focused solely on opioid use, this Delphi study was more comprehensive due to the diversity of the expert panel and the different trends in substance use and overdose internationally. The final version of the semi-structured questionnaire included 40 questions (Supplementary Materials S1), which was sent to the international panel;
- Based on the responses collected from the semi-structured questionnaire, 63 initial statements were generated. These initial statements were designed by the research group (JNW, VT, JS, KJ, FC) and were meant to encapsulate the responses provided by the panelists. In some instances, statements were created from panelists’ responses verbatim, while others were slightly modified to ensure that the spirit of all responses was coherent with the statement;
- All statements were sent to the panelists who were asked to rate all statements on a scale of 1–5 (1 = strongly disagree, 2 = somewhat disagree, 3 = neutral, 4 = somewhat agree, 5 = strongly agree) based on their knowledge and clinical experience. If panelists disagreed with a statement, they were given the opportunity to provide comments on the content and/or the phrasing of the statement. Panelists were also able to propose additional statements;
- After all ratings were received, consensus was calculated. Consensus for each statement was defined as at least 95% of all ratings being greater than or equal to three (“strongly agree”, “somewhat agree”, and “neutral”), a procedure that has been used in recent consensus statements [49,50]. All statements without consensus were revised by the research group (JNW, VT, JS, KJ, FC) based on panelists’ feedback and sent out for a second round of rating, along with any additional statements proposed by the panelists;
- Consensus was calculated for this subgroup of statements using the same a priori defined rules. Statements that still did not reach expert consensus were deemed controversial and were discussed with the panelists during an online webinar;
- The purpose of the webinar was to have clear and robust direct verbal discussion that allowed disagreements to be aired and mutually understood and that facilitated a sense of the group having a clearly defined and shared goal [49]. The webinar was organized as follows: summary of results, discussion of identified areas of disagreement, revision of statements that did not reach consensus, and discussion on next steps and priorities. All statements discussed in the webinar were revised by the research group (JNW, VT, JS, KJ, FC) based on the comments made by the panelists and sent out for a third round of rating;
- Consensus was calculated for this subgroup of statements using the same a priori defined rules. The full text of the international consensus statement was then prepared by the research group (JNW, VT, JS, KJ, FC) and lead author (MK), and shared with the Delphi panel, with a final opportunity to comment on the text. Based on the final round of feedback and comments, the international consensus statement document was finalized.
2.3. Ethics
3. Results
3.1. Semi-Structure Questionnaire
3.2. First Round of Rating
3.3. Second Round of Rating
3.4. Webinar
3.5. Third Round of Rating
3.6. Final Consensus
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erskine, H.E.; Moffitt, T.E.; Copeland, W.E.; Costello, E.J.; Ferrari, A.J.; Patton, G.; Degenhardt, L.; Vos, T.; Whiteford, H.A.; Scott, J.G. A heavy burden on young minds: The global burden of mental and substance use disorders in children and youth. Psychol. Med. 2014; Erratum in 2015, 45, 1551–1563. Available online: https://pubmed.ncbi.nlm.nih.gov/25534496 (accessed on 28 May 2021). [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. 10 Leading Causes of Death, United States [Internet]. Web-Based Injury Statistics Query and Reporting System. 2021. Available online: https://wisqars-viz.cdc.gov:8006/lcd/home (accessed on 28 May 2021).
- Eurostat. Being Young in Europe Today—Health [Internet]. Statistics Explained. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Being_young_in_Europe_today_-_health#Causes_of_death (accessed on 2 March 2022).
- Eurostat. Causes of Death—Deaths by Country of Residence and Occurrence [Internet]. Data Browser. 2022. Available online: https://ec.europa.eu/eurostat/databrowser/view/hlth_cd_aro/default/table?lang=en (accessed on 2 March 2022).
- Martins, S.S.; Sampson, L.; Cerdá, M.; Galea, S. Worldwide prevalence and trends in unintentional drug overdose: A systematic review of the literature. Am. J. Public Health 2015, 105, e29–e49. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Suicide a Leading Cause of Death Among Young Adults in High-Income Countries. Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/news/news/2014/09/suicide-a-leading-cause-of-death-among-young-adults-in-high-income-countries (accessed on 28 May 2021).
- Värnik, A.; Sisask, M.; Värnik, P.; Wu, J.; Kõlves, K.; Arensman, E.; Maxwell, M.; Reisch, T.; Gusmão, R.; Van Audenhove, C.; et al. Drug suicide: A sex-equal cause of death in 16 European countries. BMC Public Health 2011, 11, 61. [Google Scholar] [CrossRef]
- Statistics Canada. Table 13-10-0394-01 Leading Causes of Death, Total Population, by Age Group [Internet]. 2021. Available online: https://doi.org/10.25318/1310039401-eng (accessed on 22 May 2021).
- Haskins, J. Suicide, opioids tied to ongoing fall in US life expectancy: Third year of drop. Nation’s Health 2019, 49, 1–10. Available online: http://thenationshealth.aphapublications.org/content/49/1/1.2.abstract (accessed on 28 May 2021).
- Statistics Canada. Changes in Life Expectancy by Selected Causes of Death, 2017. In The Daily; 30 May 2019. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/190530/dq190530d-eng.htm (accessed on 28 May 2021).
- Krausz, M.; Westenberg, J.N.; Mathew, N.; Budd, G.; Wong, J.S.H.; Tsang, V.W.L.; Vogel, M.; King, C.; Seethapathy, V.; Jang, K.; et al. Shifting North American drug markets and challenges for the system of care. Int. J. Ment. Health Syst. 2021, 15, 86. [Google Scholar] [CrossRef]
- Alho, H.; Dematteis, M.; Lembo, D.; Maremmani, I.; Roncero, C.; Somaini, L. Opioid-related deaths in Europe: Strategies for a comprehensive approach to address a major public health concern. Int. J. Drug Policy 2020, 76, 102616. Available online: https://www.sciencedirect.com/science/article/pii/S0955395919303305 (accessed on 28 May 2021). [CrossRef]
- Mounteney, J.; Giraudon, I.; Denissov, G.; Griffiths, P. Fentanyls: Are we missing the signs? Highly potent and on the rise in Europe. Int. J. Drug Policy 2015, 26, 626–631. [Google Scholar] [CrossRef]
- ESPAD Group. ESPAD Report 2019: Results from European School Survey Project on Alcohol and Other Drugs. 2020. EMCDDA Joint Publications, Publications Office of the European Union. Available online: https://data.europa.eu/doi/10.2810/877033 (accessed on 28 May 2021).
- Orth, B.; Merkel, C. Die Drogenaffinität Jugendlicher in der Bundesrepublik Deutschland 2019; Federal Center for Health Education: Cologne, Germany, 2020.
- United Nations Office on Drugs and Crime (UNODC). UNODC Early Warning Advisory (EWA) on New Psychoactive Substances (NPS) [Internet]. 2021. Available online: https://www.unodc.org/LSS/Page/NPS (accessed on 25 November 2021).
- Dumas, T.M.; Ellis, W.; Litt, D.M. What Does Adolescent Substance Use Look Like During the COVID-19 Pandemic? Examining Changes in Frequency, Social Contexts, and Pandemic-Related Predictors. J. Adolesc. Health 2020, 67, 354–361. Available online: https://www.sciencedirect.com/science/article/pii/S1054139X20303311 (accessed on 28 May 2021). [CrossRef]
- Horigian, V.E.; Schmidt, R.D.; Feaster, D.J. Loneliness, mental health, and substance use among US young adults during COVID-19. J. Psychoact. Drugs 2020, 53, 1–9. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health; Publication Number PEP20-07-01-001; U.S. Department of Health and Human Services: Rockville, MD, USA, 2019.
- Alinsky, R.H.; Zima, B.T.; Rodean, J.; Matson, P.A.; Larochelle, M.R.; Adger, H.; Bagley, S.M.; Hadland, S.E. Receipt of Addiction Treatment after Opioid Overdose among Medicaid-Enrolled Adolescents and Young Adults. JAMA Pediatr. 2020, 174, e195183. [Google Scholar] [CrossRef]
- The Society for Adolescent Health and Medicine. Medication for Adolescents and Young Adults with Opioid Use Disorder. J. Adolesc. Health 2021, 68, 632–636. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Medication-Assisted Treatment of Adolescents with Opioid Use Disorders. Pediatrics 2016, 138, e20161893. [Google Scholar] [CrossRef] [PubMed]
- British Columbia Centre on Substance Use. Guideline Supplement Treatment of Opioid Use Disorder for. 2018. Available online: http://www.bccsu.ca/care-guidance-publications/ (accessed on 28 May 2021).
- Borodovsky, J.T.; Levy, S.; Fishman, M.; Marsch, L.A. Buprenorphine Treatment for Adolescents and Young Adults with Opioid Use Disorders: A Narrative Review. J. Addict. Med. 2018, 12, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Westenberg, J.N.; Tai, A.M.Y.; Elsner, J.; Kamel, M.M.; Wong, J.S.H.; Azar, P.; Vo, D.X.; Moore, E.; Mathew, N.; Seethapathy, V.; et al. Treatment approaches and outcome trajectories for youth with high-risk opioid use: A narrative review. Early Interv. Psychiatry 2021, 16, 207–220. [Google Scholar] [CrossRef]
- Wakeman, S.E.; Larochelle, M.R.; Ameli, O.; Chaisson, C.E.; McPheeters, J.T.; Crown, W.H.; Azocar, F.; Sanghavi, D.M. Comparative Effectiveness of Different Treatment Pathways for Opioid Use Disorder. JAMA Netw. Open 2020, 3, e1920622. [Google Scholar] [CrossRef]
- Hammond, C.J.; Gray, K.M. Pharmacotherapy for Substance Use Disorders in Youths. J. Child Adolesc. Subst. Abuse 2016, 25, 292–316. Available online: https://pubmed.ncbi.nlm.nih.gov/28082828 (accessed on 28 May 2021). [CrossRef] [PubMed]
- Hammond, C.J. The Role of Pharmacotherapy in the Treatment of Adolescent Substance Use Disorders. Child Adolesc. Child Adolesc. Psychiatr. Clin. N. Am. 2016, 25, 685–711. Available online: https://pubmed.ncbi.nlm.nih.gov/27613346 (accessed on 28 May 2021). [CrossRef] [PubMed]
- Squeglia, L.M.; Fadus, M.C.; McClure, E.A.; Tomko, R.L.; Gray, K.M. Pharmacological treatment of youth substance use disorders. J. Child Adolesc. Psychopharmacol. 2019, 29, 559–572. [Google Scholar] [CrossRef]
- Hadland, S.E.; Yule, A.M.; Levy, S.J.; Hallett, E.; Silverstein, M.; Bagley, S.M. Evidence-based treatment of young adults with substance use disorders. Pediatrics 2021, 147 (Suppl. 2), S204–S214. [Google Scholar] [CrossRef]
- Müller, C.; Trabi, T. “Österreichisches Modell” der Opioidsubstitution bei Minderjährigen. Mon. Kinderheilkd 2019, 167, 109–116. [Google Scholar] [CrossRef]
- Trabi, T.; Müller, C. Substanzbezogene Störungen bei Jugendlichen. Mon. Kinderheilkd 2019, 167, 101–108. [Google Scholar] [CrossRef]
- Krausz, R.M.; Westenberg, J.N.; Ziafat, K. The opioid overdose crisis as a global health challenge. Curr. Opin. Psychiatry 2021, 34, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; Von Sydow, K.; Beher, S.; Schweitzer-Rothers, J.; Retzlaff, R. Systemische therapie bei substanzstörungen: Historische entwicklung und aktuelle evidenzbasierte varianten. Sucht 2010, 56, 13–19. [Google Scholar] [CrossRef]
- Michels, I.I.; Stöver, H.; Gerlach, R. Substitution treatment for opioid addicts in Germany. Harm. Reduct. J. 2007, 4, 5. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Humphreys, K.; Shover, C.L.; Andrews, C.M.; Bohnert, A.S.B.; Brandeau, M.L.; Caulkins, J.P.; Chen, J.H.; Cuéllar, M.F.; Hurd, Y.L.; Juurlink, D.N. Responding to the opioid crisis in North America and beyond: Recommendations of the Stanford–Lancet Commission. Lancet 2022, 399, 555–604. [Google Scholar] [CrossRef]
- Levy, S.; Botticelli, M. Moving to a Medical Model of Substance Use Treatment of Youth. Pediatrics 2021, 147 (Suppl. 2), S262–S264. [Google Scholar] [CrossRef]
- Hadland, S.E. How Clinicians Caring for Youth Can Address the Opioid-Related Overdose Crisis. J. Adolesc. Health 2019, 65, 177–180. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med16&NEWS=N&AN=31331540 (accessed on 28 May 2021). [CrossRef] [PubMed]
- Derefinko, K.J.; Brown, R.; Danzo, A.; Foster, S.; Brennan, T.; Hand, S.; Kunz, K. Addiction medicine training fellowships in North America: A recent assessment of progress and needs. J. Addict. Med. 2020, 14, e103–e109. [Google Scholar] [CrossRef]
- Andraka-Christou, B.; Capone, M.J. A qualitative study comparing physician-reported barriers to treating addiction using buprenorphine and extended-release naltrexone in US office-based practices. Int. J. Drug Policy 2018, 54, 9–17. [Google Scholar] [CrossRef]
- Hadland, S.E.; Park, T.W.; Bagley, S.M. Stigma associated with medication treatment for young adults with opioid use disorder: A case series. Addict. Sci. Clin. Pract. 2018, 13, 15. [Google Scholar] [CrossRef]
- Hadland, S.E.; Wood, E.; Levy, S. How the paediatric workforce can address the opioid crisis. Lancet 2016, 388, 1260–1261. [Google Scholar] [CrossRef]
- Bagley, S.M.; Hadland, S.E.; Carney, B.L.; Saitz, R. Addressing Stigma in Medication Treatment of Adolescents with Opioid Use Disorder. J. Addict. Med. United States 2017, 11, 415–416. [Google Scholar] [CrossRef]
- Jenkins, E.K.; Slemon, A.; Haines-Saah, R.J. Developing harm reduction in the context of youth substance use: Insights from a multi-site qualitative analysis of young people’s harm minimization strategies. Harm. Reduct. J. 2017, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, S.D.; Gaeta, J.M.; Hadland, S.E.; Hallett, E.; Marshall, B.D.L. Principles of harm reduction for young people who use drugs. Pediatrics 2021, 147 (Suppl. 2), S240–S248. [Google Scholar] [CrossRef] [PubMed]
- Somaini, B.; Grob, P. How and why AIDS changed drug policy in Switzerland. J. Public Health Policy 2012, 33, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Khazaal, Y.; Thorens, G.; Zullino, D.; Uchtenhagen, A. Understanding Swiss drug policy change and the introduction of heroin maintenance treatment. Eur. Addict. Res. 2014, 20, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. High-Risk Substance Use Among Youth. Adolescent and School Health. 2020. Available online: https://www.cdc.gov/healthyyouth/substance-use/index.htm (accessed on 22 April 2021).
- Ives, J.; Dunn, M.; Molewijk, B.; Schildmann, J.; Bærøe, K.; Frith, L.; Huxtable, R.; Landeweer, E.; Mertz, M.; Provoost, V.; et al. Standards of practice in empirical bioethics research: Towards a consensus. BMC Med. Ethics 2018, 19, 68. [Google Scholar] [CrossRef] [PubMed]
- Özgen, H.; Spijkerman, R.; Noack, M.; Holtmann, M.; Schellekens, A.S.A.; van de Glind, G.; Banaschewski, T.; Barta, C.; Begeman, A.; Casas, M.; et al. International consensus statement for the screening, diagnosis, and treatment of adolescents with concurrent attention-deficit/hyperactivity disorder and substance use disorder. Eur. Addict. Res. 2020, 26, 223–232. [Google Scholar] [CrossRef]
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; McKee, C.M.; Sanderson, C.F.; Askham, J.; Marteau, T. Consensus development methods, and their use in clinical guideline development. Health Technol. Assess. 1998, 2, 3. [Google Scholar] [CrossRef]
- Kredo, T.; Bernhardsson, S.; Machingaidze, S.; Young, T.; Louw, Q.; Ochodo, E.; Grimmer, K. Guide to clinical practice guidelines: The current state of play. Int. Soc. Qual. Health Care 2016, 28, 122–128. [Google Scholar] [CrossRef]
- Subramaniam, G.A.; Fishman, M.J.; Woody, G. Treatment of opioid-dependent adolescents and young adults with buprenorphine. Curr. Psychiatry Rep. 2009, 11, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Marsch, L.A.; Moore, S.K.; Borodovsky, J.T.; Solhkhah, R.; Badger, G.J.; Semino, S.; Jarrett, K.; Condon, K.D.; Rossettie, K.; Vincent, P.; et al. A randomized controlled trial of buprenorphine taper duration among opioid-dependent adolescents and young adults. Addiction 2016, 111, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.; Hadland, S.E.; Hallett, E.; Botticelli, M. Principles of Care for Young Adults with Substance Use Disorders. Pediatrics 2021, 147 (Suppl. 2), S195–S203. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.; Fast, D.; Hobbins, M.; McNeil, R.; Small, W. Social-structural factors influencing periods of injection cessation among marginalized youth who inject drugs in Vancouver, Canada: An ethno-epidemiological study. Harm. Reduct. J. 2017, 14, 31. [Google Scholar] [CrossRef]
- Patton, R.; Goerke, J.E.; Katafiasz, H. Systemic Approaches to Adolescent Substance Abuse. In The Handbook of Systemic Family Therapy; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2020; pp. 297–320. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781119438519.ch45 (accessed on 28 May 2021).
- Rojas, L.M.; Ochoa, L.G.; Sánchez Ahumada, M.; Quevedo, A.; Muñoz, V.; Condo, C.; Prado, G. Parent attendance in a family-based preventive intervention delivered in Latin America and the United States. Health Promot. Pract. 2021, 22, 531–539. [Google Scholar] [CrossRef]
- Van Ryzin, M.J.; Roseth, C.J.; Fosco, G.M.; Lee, Y.; Chen, I.-C. A component-centered meta-analysis of family-based prevention programs for adolescent substance use. Clin. Psychol. Rev. 2016, 45, 72–80. Available online: https://www.sciencedirect.com/science/article/pii/S027273581530009X (accessed on 28 May 2021). [CrossRef]
- Austin, A.M.; Macgowan, M.J.; Wagner, E.F. Effective family-based interventions for adolescents with substance use problems: A systematic review. Res. Soc. Work Pract. 2005, 15, 67–83. [Google Scholar] [CrossRef]
- Tanner-Smith, E.E.; Wilson, S.J.; Lipsey, M.W. The comparative effectiveness of outpatient treatment for adolescent substance abuse: A meta-analysis. J. Subst. Abuse Treat. 2013, 44, 145–158. Available online: https://www.sciencedirect.com/science/article/pii/S0740547212001055 (accessed on 28 May 2021). [CrossRef]
- Bagley, S.M.; Chavez, L.; Braciszewski, J.M.; Akolsile, M.; Boudreau, D.M.; Lapham, G.; Campbell, C.I.; Bart, G.; Yarborough, B.J.H.; Samet, J.H. Receipt of medications for opioid use disorder among youth engaged in primary care: Data from 6 health systems. Addict. Sci. Clin. Pract. 2021, 16, 46. [Google Scholar] [CrossRef]
- Christie, G.; Marsh, R.; Sheridan, J.; Wheeler, A.; Suaalii-Sauni, T.; Black, S.; Butler, R. The Substances and Choices Scale (SACS)—The development and testing of a new alcohol and other drug screening and outcome measurement instrument for young people. Addiction 2007, 102, 1390–1398. [Google Scholar] [CrossRef]
- Knight, J.R.; Sherritt, L.; Shrier, L.A.; Harris, S.K.; Chang, G. Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Arch. Pediatr. Adolesc. Med. 2002, 156, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Schippers, G.M.; Broekman, T.G.; Buchholz, A.; Koeter, M.W.J.; van den Brink, W. Measurements in the Addictions for Triage and Evaluation (MATE): An instrument based on the World Health Organization family of international classifications. Addiction 2010, 105, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Merry, S.N.; Cargo, T.; Christie, G.; Donkin, L.; Hetrick, S.; Fleming, T.; Holt-Quick, C.; Hopkins, S.; Stasiak, K.; Warren, J. Debate: Supporting the mental health of school students in the COVID-19 pandemic in New Zealand–a digital ecosystem approach. Child Adolesc. Ment. Health 2020, 25, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Schwinn, T.M.; Schinke, S.P.; Keller, B.; Hopkins, J. Two- and three-year follow-up from a gender-specific, web-based drug abuse prevention program for adolescent girls. Addict. Behav. 2019, 93, 86–92. Available online: https://www.sciencedirect.com/science/article/pii/S0306460318311626 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Hickie, I.B. Implementing 21st century “end-to-end” and technology-enhanced care for young people. World Psychiatry 2022, 21, 79–81. Available online: https://pubmed.ncbi.nlm.nih.gov/35015351 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Warshawski, T.; Charles, G.; Moore, E.; Virani, A.; Preto, N.; Pollicino, A.; Warf, C. Building an Effective System of Care for Adolescents Following Opiate Overdose: Stabilization Care, Residential Secure Care, Family and Community Engagement, and Ethical Concerns. In Clinical Care for Homeless, Runaway and Refugee Youth; Springer: Berlin/Heidelberg, Germany, 2020; pp. 157–185. [Google Scholar]
- Warshawski, T.; Warf, C. It is time for an ethical, evidence-based approach to youth presenting to the ED with an opioid overdose. Paediatr. Child Health 2019, 24, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Bertolote, J.; McGorry, P. Early intervention and recovery for young people with early psychosis: Consensus statement. Br. J. Psychiatry 2005, 187 (Suppl. 48), s116–s119. [Google Scholar] [CrossRef]
- Cullberg, J.; Mattsson, M.; Levander, S.; Holmqvist, R.; Tomsmark, L.; Elingfors, C.; Wieselgren, I.M. Treatment costs and clinical outcome for first episode schizophrenia patients: A 3-year follow-up of the Swedish ‘Parachute Project’and Two Comparison Groups. Acta Psychiatr. Scand. 2006, 114, 274–281. [Google Scholar] [CrossRef]
- Gomes, T.; Tadrous, M.; Mamdani, M.M.; Paterson, J.M.; Juurlink, D.N. The Burden of Opioid-Related Mortality in the United States. JAMA Netw. Open 2018, 1, e180217. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med15&NEWS=N&AN=30646062 (accessed on 28 May 2021). [CrossRef]
- New Zealand Ministry of Health. New Zealand Practice Guidelines for Opioid Substitution Treatment [Internet]. Ministry of Health Wellington. 2014. Available online: https://www.health.govt.nz/system/files/documents/publications/nz-practice-guidelines-opioid-substitution-treatment-apr14-v2.pdf (accessed on 28 May 2021).
- Gowing, L.; Ali, R.; Dunlop, A.; Farrell, M.; Lintzeris, N. National Guidelines for Medication-Assisted Treatment of Opioid Dependence. Available online: https://www.health.gov.au/sites/default/files/national-guidelines-for-medication-assisted-treatment-of-opioid-dependence.pdf (accessed on 28 May 2021).
- Stern, M. Perspectives of LGBTQ Youth and Pediatricians in the Primary Care Setting: A Systematic Review. J. Prim. Care Community Health 2021, 12, 21501327211044356. [Google Scholar] [CrossRef]
- Cave, L.; Cooper, M.N.; Zubrick, S.R.; Shepherd, C.C.J. Racial discrimination and child and adolescent health in longitudinal studies: A systematic review. Soc. Sci. Med. 2020, 250, 112864. Available online: http://www.sciencedirect.com/science/article/pii/S0277953620300836 (accessed on 28 May 2021). [CrossRef] [PubMed]
- Cabanis, M.; Outadi, A.; Choi, F. Early childhood trauma, substance use and complex concurrent disorders among adolescents. Curr. Opin. Psychiatry 2021, 34, 393–399. [Google Scholar] [CrossRef] [PubMed]
- López, C.M.; Andrews, A.R., III; Chisolm, A.M.; De Arellano, M.A.; Saunders, B.; Kilpatrick, D. Racial/ethnic differences in trauma exposure and mental health disorders in adolescents. Cult. Divers. Ethn. Minor. Psychol. 2017, 23, 382. [Google Scholar] [CrossRef]
- Komaromy, M.; Mendez-Escobar, E.; Madden, E. Addressing racial trauma in the treatment of substance use disorders. Pediatrics 2021, 147 (Suppl. 2), S268–S270. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Etkins, O.S. Racism and mental health. World Psychiatry 2021, 20, 194–195. [Google Scholar] [CrossRef] [PubMed]
- Yurasek, A.M.; Kemp, K.; Otero, J.; Tolou-Shams, M. Substance use screening and rates of treatment referral among justice-involved youth. Addict. Behav. 2021, 122, 107036. [Google Scholar] [CrossRef]
- Feldstein Ewing, S.W.; Venner, K.L.; Mead, H.K.; Bryan, A.D. Exploring racial/ethnic differences in substance use: A preliminary theory-based investigation with juvenile justice-involved youth. BMC Pediatr. 2011, 11, 71. Available online: https://pubmed.ncbi.nlm.nih.gov/21846356 (accessed on 28 May 2021). [CrossRef]
- McGorry, P.; Bates, T.; Birchwood, M. Designing youth mental health services for the 21st century: Examples from Australia, Ireland and the UK. Br. J. Psychiatry 2013, 202, s30–s35. [Google Scholar] [CrossRef]
- Guarino, H.M.; Marsch, L.A.; Campbell, W.S., III; Gargano, S.P.; Haller, D.L.; Solhkhah, R. Methadone maintenance treatment for youth: Experiences of clients, staff, and parents. Subst. Use Misuse 2009, 44, 1979–1989. [Google Scholar] [CrossRef]
- Van de Glind, G.; Brynte, C.; Skutle, A.; Kaye, S.; Konstenius, M.; Levin, F.; Mathys, F.; Demetrovics, Z.; Moggi, F.; Ramos-Quiroga, J.A. The international collaboration on ADHD and substance abuse (ICASA): Mission, results, and future activities. Eur. Addict. Res. 2020, 26, 173–178. [Google Scholar] [CrossRef]


{kind=link}
| Country | n (%) |
| Australia | 2 (6.5%) |
| Austria | 5 (16.1%) |
| Canada | 6 (19.4%) |
| Egypt | 1 (3.2%) |
| Germany | 3 (9.7%) |
| Italy | 1 (3.2%) |
| Netherlands | 2 (6.5%) |
| New Zealand | 2 (6.5%) |
| Switzerland | 6 (19.4%) |
| United States | 3 (9.7) |
| Profession | n (%) |
| Psychiatrist | 21 (67.7%) |
| Addiction psychiatry specialist | 13 |
| Child and adolescent psychiatry specialist | 4 |
| Dual specialist in addiction psychiatry and child and adolescent psychiatry | 5 |
| Pediatrician | 4 (12.9%) |
| Adolescent medicine specialist | 2 |
| Dual specialist in adolescent medicine and addiction medicine | 1 |
| Dual specialist in developmental-behavioural pediatrics and addiction medicine | 1 |
| Psychologist | 3 (9.7%) |
| Youth addiction specialist | 1 |
| Addiction medicine specialist | 1 |
| Mental health and addiction specialist | 1 |
| General Practitioner | 2 (6.5%) |
| Addiction medicine specialist | 1 |
| Psychosomatic medicine and psychotherapy specialist | 1 |
| Emergency Medicine Physician | 1 (3.2%) |
| A. Clinical Risks/Concurrent Conditions | |
| 1 | Screening for mental health problems, substance use problems, and related risks in primary care and other clinical settings is recommended for all youth. |
| 2 | It is recommended that screening be performed preferably with the adolescent alone (without the parent(s)/caretaker being present), and that discussions surrounding mental challenges, substance use, and related risks to be performed in an open and non-judgmental way. |
| 3 | It is recommended that youth who are known to be at risk of SUD due to mental health problems or a family history of SUD and mental health receive targeted prevention efforts and more frequent screening. |
| 4 | It is recommended that other critical domains be assessed among youth with high-risk substance use when deemed appropriate by primary care providers. These can include psychological distress, family history and family functioning, peer group and social functioning, high-risk behaviors, physical health, housing and financial situation, employment and academic capacity, coping strategies, and resilience. |
| 5 | It is recommended that trauma be carefully and methodically assessed among youth with high-risk substance use by providers that the youth can trust and feel comfortable sharing with. |
| 6 | Among youth with high-risk substance use, it is recommended that psychiatric assessments for mental health and substance use disorders be performed routinely using clinical guidelines for screening and assessment of mental health. |
| 7 | Among youth with high-risk substance use, it is recommended that physical health assessments for frequently occurring physical conditions, such as infectious complications be performed routinely using clinical guidelines for screening and assessment of physical health. |
| 8 | Among youth with high-risk substance use presenting with their first episode of psychosis, it is important to rule out transient causes of psychosis such as substance use or medical ailments. Youth must also be assessed for primary psychotic disorders. |
| 9 | Youth with high-risk substance use presenting with severe infections such as Hepatitis C and HIV must be offered treatment according to guidelines and be provided with the best guidance to make an informed decision. |
| 10 | It is recommended that protocols be in place for any youth who experiences serious, life-threatening outcomes such as overdose, consecutive binge drinking episodes, or strong suicidal ideation. |
| 11 | Protocols for youth who experience serious life-threatening outcomes should recommend that youth be provided with immediate access to counselling, case management, appropriate pharmacotherapy treatment, and the encouragement to notify and involve social support systems. |
| B. Target populations | |
| 1 | Services must be tailored to the developmental age of the individual and be substance-specific, severity-specific, and risk-specific. |
| 2 | Having parents with SUD is one of the most prominent risk factors for youth to develop SUD in adolescence and/or early adulthood; prevention and early identification are paramount for youth whose parents suffer from SUD. |
| 3 | It is important that parents with SUD be supported in maintaining guardianship and provided with parenting guidance when appropriate; treatment should work towards stabilizing the family as a unit. |
| 4 | For youth whose parents suffer from SUD, special attention should be paid to the youth’s experiences and their relationships with their family members. |
| 5 | It is recommended that substance use and mental health care organizations routinely ask parents with SUD about family functionality to ensure the needs of the youth are being addressed. Protocols should be in place to notify specialized organizations and appropriate government ministries if there is suspicion of child abuse or family violence. |
| 6 | It is recommended that youth with high-risk substance use and living in marginalized environments be provided with supportive housing options in cooperation with engaged institutions (youth welfare services, treatment services, harm reduction services, etc.). |
| 7 | It is recommended that young females of childbearing age who are at risk of becoming pregnant whilst taking substances be provided with options for contraception with counselling and sexual health assessments as appropriate. |
| 8 | It is recommended that young females using substances who are expectant mothers be provided with access to supports that specifically address their needs including prenatal and postnatal care services, health education, and consulting services, as well as family planning services. |
| 9 | It is recommended that young females using substances who are expectant mothers be provided with support to help develop their capacity as caregivers and should be connected to services to address risks and encourage parenting. Foster care, adoption, and termination of pregnancy can also be options if desired by the expectant mother, and resources for each option should be available. |
| 10 | It is recommended that youth with concurrent conditions be specifically engaged with multidisciplinary teams specializing in dual diagnosis among youth. |
| 11 | It is recommended that youth with concurrent conditions be specifically offered psychoeducational activities to improve awareness about the triggering effects of substances and the worsening of psychiatric conditions. |
| 12 | It is recommended that youth with opioid use or regular stimulant use be provided with age-appropriate counseling, case management, family therapy, and pharmacotherapy, ideally all through the same treatment program for integrated care. Peer support, harm reduction services, selected preventive interventions, and health education should also be provided. |
| C. Intervention goals | |
| 1 | The objectives of treating youth with high-risk substance use are to reduce harm and mortality, prevent interference in adolescent development and substance-related impairment, and promote resilience and positive youth development. |
| 2 | SUD treatment should be goal-oriented, tailored to each individual, and provided in partnership with youth and others collaborating in their care. |
| 3 | It is recommended that all evidence-based interventions be available and used according to the needs and preferences of the patient in collaboration with the care team for maximal engagement. |
| 4 | Relapse is part of the symptomatology. Youth must be enabled to recognize what to do when the risk of relapse is high, or when a slip has occurred. Motivation interviewing, skills building, and mitigating risks of substance use are recommended to help attain goals. |
| 5 | It is important to discuss overdose in an open and direct way within a harm reduction framework. Youth who (intend to) use drugs should have access to a spectrum of youth-friendly harm reduction services and be encouraged to use them. |
| 6 | It is important to provide Naloxone/Narcan and education to the entire community surrounding a youth with high-risk substance use, including their family and friends. |
| 7 | It is recommended to warn youth prescribed opioids for pain management about the risks of substance misuse/overdose and be assessed frequently for step-down to appropriate medications, as directed by specific guidelines for clinicians. |
| 8 | If necessary, youth prescribed opioids for pain management and at high risk of prescription opioid misuse and/or opioid use disorder should be given Naloxone/Narcan and offered resources for prevention and treatment. |
| 9 | It is important for psychoeducation and risk management to be accessible in schools, in health systems, in vocational activities, in mainstream media, through online interventions, and in open discussions with the caring adults in their lives. |
| 10 | It is important for standard school-based programs to be provided as part of the curriculum to reduce barriers, increase primary prevention, and target early intervention for youth who are at risk. |
| 11 | It is important for all youth to have access to online tools for risk assessment and monitoring, which can provide them with the opportunity for personalised feedback, tailored information, and harm-reduction advice rapidly, while also being anonymous if desired. |
| D. Evidence-based intervention strategies | |
| 1 | It is recommended that psychosocial evidence-based intervention strategies include family therapy, motivational interviewing, counselling, cognitive behavioral therapy, and integrated treatment of concurrent disorders, and peer support should be offered to all youth with SUD. |
| 2 | For opioid use disorder, evidence-based medication treatments, including opioid agonist treatment (OAT), are recommended as the first-line intervention. |
| 3 | It is important that the range of medications for opioid use disorder (including buprenorphine, methadone, extended-release naltrexone, slow-release morphine, etc.) be available to youth and that medication choice be prioritized based on the preference and needs of the patient. |
| 4 | For high-risk cannabis use, behavioral interventions such as motivational interviewing, cognitive behavioral therapy, and family therapy are recommended. |
| 5 | For stimulant dependence, behavioral interventions such as contingency management, motivational interviewing, cognitive behavioral therapy, and family therapy are recommended. Medication may be required to manage problematic symptoms, particularly in stimulant withdrawal. |
| 6 | For benzodiazepine dependence, it is recommended that pharmacotherapy involving the gradual tapering of benzodiazepines be considered as first choice treatment if there is a chance of withdrawal. Regardless, behavioral interventions, such as contingency management, cognitive behavioral therapy, and family therapy, are also recommended along with symptomatic treatment. |
| 7 | As most new and established medications have not been systematically evaluated in young people, decisions about their use should be taken with reference to the evidence-base in adults or as evidence emerges in youth and include a collaborative risk-benefit analysis. |
| 8 | It is recommended to assess youth for informed decision-making capacity and engaged in appropriate assent or consent processes when choosing the appropriate treatment options. Parents/caretakers should be involved to support decision-making and treatment when appropriate. |
| 9 | Text message reminders, contingency management, case management, community support, and motivational interviewing are also recommended to enhance adherence and retention. |
| 10 | Educating the public, addressing the stigma, easing transition between the services, and training providers are all paramount in increasing overall access to OAT. |
| 11 | Inpatient rehabilitation should be considered for youth with high-risk substance use if this is the preference of the youth, if the social environment is toxic, if the housing situation is very unstable, if there is a long history of unsuccessful treatment attempts, or if there are severe negative medical, social, and psychological consequences to any other option. |
| 12 | Treatment approaches can be made developmentally appropriate by using language that is accessible to youth, by focusing on their goals, and by individualizing their treatment trajectories to meet their specific needs through youth/provider joint decision-making. |
| 13 | It is recommended to involve the parents/caretakers in the treatment process. Even in dysfunctional families or in the case of divorce, parents/caretakers remain a critical resource for recovery. Treatment or consultation can happen in different ways, from direct family sessions to parallel consultations. However, limited or no parental involvement should not be a barrier to treatment for youth. |
| 14 | Family involvement can be counterproductive in certain situations, such as significant family conflict, abusive relationships, violence, and estrangement. It is important for youth protection to be prioritized. |
| 15 | Youth should guide who is involved in their treatment, and this should be respected. It is critical to encourage effective autonomy while balancing that against the capacity for effective health-directed decision making. Disclosure to others collaborating in their care should be performed with careful consideration of the risks of mistrust and disengagement. However, if youth or others are at risk of significant harm, breach of confidentiality needs to be considered. |
| 16 | If the parents/caretakers do not support treatment initially (often due to a misunderstanding or preconceived notion), their involvement should continue to be encouraged via education, enhancing trust, and relieving concerns. It is important that interventional strategies work with parents/caretakers and youth in parallel, until they agree to have common sessions. |
| E. Appropriate treatment settings and expertise | |
| 1 | Peer support and case managers are quintessential to all treatment settings, with seamless transitioning and hand-off between all treatment settings. |
| 2 | It is important for emergency department and intensive care admissions to act as a youth-friendly touchpoint and gateway for screening, brief intervention, and referral to treatment. |
| 3 | It is recommended that youth admitted to emergency departments and intensive care units be immediately linked to case-managers, offered a private space for visits from caregivers, referred to substance use treatment, and be connected to therapy depending on their preferences. |
| 4 | All services, including outreach and harm reduction, must be low-threshold, youth-friendly, and stigma-free. They have to be interesting and safe to youth. |
| 5 | All services must have seamless transitions and referrals to treatment centers for youth interested. |
| 6 | Easy transportation to and from services, flexible hours that work for youth, and the possibility of online interventions (texting, social media, apps) are recommended. |
| 7 | Professionals must be empowered and feel comfortable dealing with high-risk substance use among youth, no matter their specialization. The healthcare system as a whole must be better trained in dealing with high-risk substance use among youth. |
| 8 | It is important to provide physicians involved in the care of youth with specialty-appropriate education and training for proper referral or management of high-risk substance use among youth. |
| 9 | There is an urgent need for more clinical research, such as randomized controlled trials and high-quality observational studies, which focuses on improving models of care for high-risk substance use in adolescents and young adults. Explicit clinical research on high-risk substance use among adolescents and young adults needs to become a priority. |
| 10 | Critical data about serious adverse events among youth who use substances, including non-fatal and fatal overdose events, as well as about treatment capacity (including the number of young patients dispensed OAT and the number of youth OAT prescribers), must be collected, analyzed, and reported in a timely fashion. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krausz, M.; Westenberg, J.N.; Tsang, V.; Suen, J.; Ignaszewski, M.J.; Mathew, N.; Azar, P.; Cabanis, M.; Elsner, J.; Vogel, M.; et al. Towards an International Consensus on the Prevention, Treatment, and Management of High-Risk Substance Use and Overdose among Youth. Medicina 2022, 58, 539. https://doi.org/10.3390/medicina58040539
Krausz M, Westenberg JN, Tsang V, Suen J, Ignaszewski MJ, Mathew N, Azar P, Cabanis M, Elsner J, Vogel M, et al. Towards an International Consensus on the Prevention, Treatment, and Management of High-Risk Substance Use and Overdose among Youth. Medicina. 2022; 58(4):539. https://doi.org/10.3390/medicina58040539
Chicago/Turabian StyleKrausz, Michael, Jean N. Westenberg, Vivian Tsang, Janet Suen, Martha J. Ignaszewski, Nickie Mathew, Pouya Azar, Maurice Cabanis, Julie Elsner, Marc Vogel, and et al. 2022. "Towards an International Consensus on the Prevention, Treatment, and Management of High-Risk Substance Use and Overdose among Youth" Medicina 58, no. 4: 539. https://doi.org/10.3390/medicina58040539
APA StyleKrausz, M., Westenberg, J. N., Tsang, V., Suen, J., Ignaszewski, M. J., Mathew, N., Azar, P., Cabanis, M., Elsner, J., Vogel, M., Spijkerman, R., Orsolini, L., Vo, D., Moore, E., Moe, J., Strasser, J., Köck, P., Marian, C., Dürsteler, K. M., ... Choi, F. (2022). Towards an International Consensus on the Prevention, Treatment, and Management of High-Risk Substance Use and Overdose among Youth. Medicina, 58(4), 539. https://doi.org/10.3390/medicina58040539