

Clinical Characteristics of Symptomatic Cholecystitis in Post-Gastrectomy Patients: 11 Years of Experience in a Single Center

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Patient Grouping
2.2. Statistics and Ethics
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakorafas, G.H.; Milingos, D.; Peros, G. Asymptomatic cholelithiasis: Is cholecystectomy really needed? A critical reappraisal 15 years after the introduction of laparoscopic cholecystectomy. Dig. Dis. Sci. 2007, 52, 1313–1325. [Google Scholar] [CrossRef] [PubMed]
- Sanders, G.; Kingsnorth, A.N. Gallstones. BMJ 2007, 335, 295–299. [Google Scholar] [CrossRef]
- Fukagawa, T.; Katai, H.; Saka, M.; Morita, S.; Sano, T.; Sasako, M. Gallstone formation after gastric cancer surgery. J. Gastrointest. Surg. 2009, 13, 886–889. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Hisanaga, M.; Kanehiro, H.; Yamada, Y.; Ko, S.; Nakajima, Y. Analysis of risk factors for the development of gallstones after gastrectomy. Br. J. Surg. 2005, 92, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Li, V.K.; Pulido, N.; Martinez-Suartez, P.; Fajnwaks, P.; Jin, H.Y.; Szomstein, S.; Rosenthal, R.J. Symptomatic gallstones after sleeve gastrectomy. Surg. Endosc. 2009, 23, 2488–2492. [Google Scholar] [CrossRef]
- Health Insurance Review and Assessment Service. Korea Healthcare Bigdata Hub; Health Insurance Review and Assessment Service: Wonju, Korea, 2021; Available online: http://opendata.hira.or.kr/ (accessed on 6 January 2020).
- Kimura, J.; Kunisaki, C.; Takagawa, R.; Makino, H.; Ueda, M.; Ota, M.; Oba, M.; Kosaka, T.; Akiyama, H.; Endo, I. Is routine prophylactic cholecystectomy necessary during gastrectomy for gastric cancer? World J. Surg. 2017, 41, 1047–1053. [Google Scholar] [CrossRef]
- Park, D.J.; Kim, K.H.; Park, Y.S.; Ahn, S.-H.; Park, D.J.; Kim, H.-H. Risk factors for gallstone formation after surgery for gastric cancer. J. Gastric Cancer 2016, 16, 98–104. [Google Scholar] [CrossRef]
- Iglézias Brandão de Oliveira, C.; Adami Chaim, E.; da Silva, B.B. Impact of rapid weight reduction on risk of cholelithiasis after bariatric surgery. Obes. Surg. 2003, 13, 625–628. [Google Scholar] [CrossRef]
- Jun, K.H.; Kim, J.H.; Kim, J.J.; Chin, H.M.; Park, S.M. Retrospective analysis on the gallstone disease after gastrectomy for gastric cancer. Gastroenterol. Res. Pract. 2015, 2015, 827864. [Google Scholar] [CrossRef]
- Yi, S.Q.; Ohta, T.; Tsuchida, A.; Terayama, H.; Naito, M.; Li, J.; Wang, H.X.; Yi, N.; Tanaka, S.; Itoh, M. Surgical anatomy of innervation of the gallbladder in humans and Suncus murinus with special reference to morphological understanding of gallstone formation after gastrectomy. World J. Gastroenterol. 2007, 13, 2066–2071. [Google Scholar] [CrossRef]
- Inoue, K.; Fuchigami, A.; Hosotani, R.; Kogire, M.; Huang, Y.S.; Miyashita, T.; Suzuki, T.; Tsuda, K.; Seino, Y.; Rayford, P.L.; et al. Release of cholecystokinin and gallbladder contraction before and after gastrectomy. Ann. Surg. 1987, 205, 27–32. [Google Scholar] [PubMed]
- Pezzolla, F.; Lantone, G.; Guerra, V.; Misciagna, G.; Prete, F.; Giorgio, I.; Lorusso, D. Influence of the method of digestive tract reconstruction on gallstone development after total gastrectomy for gastric cancer. Am. J. Surg. 1993, 166, 6–10. [Google Scholar] [CrossRef]
- Boerlage, T.C.C.; Haal, S.; Maurits de Brauw, L.; Acherman, Y.I.Z.; Bruin, S.; van de Laar, A.; Moes, D.E.; van Wagensveld, B.A.; de Vries, C.E.E.; van Veen, R.; et al. Ursodeoxycholic acid for the prevention of symptomatic gallstone disease after bariatric surgery: Study protocol for a randomized controlled trial (UPGRADE trial). BMC Gastroenterol. 2017, 17, 164. [Google Scholar] [CrossRef] [PubMed]
- Haal, S.; Guman, M.S.S.; Boerlage, T.C.C.; Acherman, Y.I.Z.; de Brauw, L.M.; Bruin, S.; de Castro, S.M.M.; van Hooft, J.E.; van de Laar, A.; Moes, D.E.; et al. Ursodeoxycholic acid for the prevention of symptomatic gallstone disease after bariatric surgery (UPGRADE): A multicentre, double-blind, randomised, placebo-controlled superiority trial. Lancet Gastroenterol. Hepatol. 2021, 6, 993–1001. [Google Scholar] [CrossRef]
- Lee, S.H.; Jang, D.K.; Yoo, M.W.; Hwang, S.H.; Ryu, S.Y.; Kwon, O.K.; Hur, H.; Man Yoon, H.; Eom, B.W.; Ahn, H.S.; et al. Efficacy and safety of ursodeoxycholic acid for the prevention of gallstone formation after gastrectomy in patients with gastric cancer: The PEGASUS-D randomized clinical trial. JAMA Surg. 2020, 155, 703–711. [Google Scholar] [CrossRef]
- Reynolds, W., Jr. The first laparoscopic cholecystectomy. JSLS 2001, 5, 89–94. [Google Scholar]
- Tazuma, S.; Unno, M.; Igarashi, Y.; Inui, K.; Uchiyama, K.; Kai, M.; Tsuyuguchi, T.; Maguchi, H.; Mori, T.; Yamaguchi, K.; et al. Evidence-based clinical practice guidelines for cholelithiasis 2016. J. Gastroenterol. 2017, 52, 276–300. [Google Scholar] [CrossRef]
- Fraser, S.A.; Sigman, H. Conversion in laparoscopic cholecystectomy after gastric resection: A 15-year review. Can. J. Surg. 2009, 52, 463–466. [Google Scholar]
- Sasaki, A.; Nakajima, J.; Nitta, H.; Obuchi, T.; Baba, S.; Wakabayashi, G. Laparoscopic cholecystectomy in patients with a history of gastrectomy. Surg. Today 2008, 38, 790–794. [Google Scholar] [CrossRef]
- Ercan, M.; Bostanci, E.B.; Ulas, M.; Ozer, I.; Ozogul, Y.; Seven, C.; Atalay, F.; Akoglu, M. Effects of previous abdominal surgery incision type on complications and conversion rate in laparoscopic cholecystectomy. Surg. Laparosc. Endosc. Percutan. Tech. 2009, 19, 373–378. [Google Scholar] [CrossRef]
- Zhang, M.-J.; Yan, Q.; Zhang, G.-L.; Zhou, S.-Y.; Yuan, W.-B.; Shen, H.-P. Laparoscopic cholecystectomy in patients with history of gastrectomy. JSLS 2016, 20, e2016.00075. [Google Scholar] [CrossRef] [PubMed]
- Bencini, L.; Marchet, A.; Alfieri, S.; Rosa, F.; Verlato, G.; Marrelli, D.; Roviello, F.; Pacelli, F.; Cristadoro, L.; Taddei, A.; et al. The Cholegas trial: Long-term results of prophylactic cholecystectomy during gastrectomy for cancer-a randomized-controlled trial. Gastric Cancer 2019, 22, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Dakour-Aridi, H.N.; El-Rayess, H.M.; Abou-Abbass, H.; Abu-Gheida, I.; Habib, R.H.; Safadi, B.Y. Safety of concomitant cholecystectomy at the time of laparoscopic sleeve gastrectomy: Analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Surg. Obes. Relat. Dis. 2017, 13, 934–941. [Google Scholar] [CrossRef]
- Yardimci, S.; Coskun, M.; Demircioglu, S.; Erdim, A.; Cingi, A. Is concomitant cholecystectomy necessary for asymptomatic cholelithiasis during laparoscopic sleeve gastrectomy? Obes. Surg. 2018, 28, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Information Committee of the Korean Gastric Cancer Association. Korean Gastric Cancer Association-led nationwide survey on surgically treated gastric cancers in 2019. J. Gastric Cancer 2021, 21, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Harino, T.; Tomimaru, Y.; Yokota, Y.; Noguchi, K.; Shimizu, J.; Taguchi, T.; Yanagimoto, Y.; Suzuki, Y.; Hirota, M.; Tanida, T.; et al. Surgical outcome of laparoscopic cholecystectomy in patients with a history of gastrectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2020, 31, 170–174. [Google Scholar] [CrossRef]
- Liang, T.J.; Liu, S.I.; Chen, Y.C.; Chang, P.M.; Huang, W.C.; Chang, H.T.; Chen, I.S. Analysis of gallstone disease after gastric cancer surgery. Gastric Cancer 2017, 20, 895–903. [Google Scholar] [CrossRef]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepatobiliary Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef]
- Moreels, T.G. ERCP in the patient with surgically altered anatomy. Curr. Gastroenterol. Rep. 2013, 15, 343. [Google Scholar] [CrossRef]
- Seo, G.H.; Lim, C.S.; Chai, Y.J. Incidence of gallstones after gastric resection for gastric cancer: A nationwide claims-based study. Ann. Surg. Treat. Res. 2018, 95, 87–93. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Non-Gastrectomy (n = 1543) | Gastrectomy (n = 44) | p-Value |
|---|---|---|---|
| Age (years, mean ± sd) | 57.58 ± 17.28 | 66.98 ± 11.78 | <0.001 |
| Gender | |||
| Male | 802 (52.0%) | 33 (75.0%) | 0.003 |
| Female | 741 (48.0%) | 11 (25.0%) | |
| ASA score | 2.54 ± 0.56 | 2.59 ± 0.58 | 0.650 |
| I | 18 (2.3%) | 1 (3.4%) | |
| II | 329 (42.2%) | 10 (34.5%) | |
| III | 428 (54.9%) | 18 (62.1%) | |
| IV | 5 (0.6%) | 0 (0.0%) | |
| BMI (kg/m2) | 25.31 ± 3.99 | 21.66 ± 3.20 | <0.001 |
| ICU admission days | 0.17 ± 1.37 | 0.07 ± 0.26 | 0.638 |
| Operation time (min, mean ± sd) | 102.51 ± 52.43 | 167.39 ± 82.95 | <0.001 |
| Stomach OP Hx | |||
| Subtotal gastrectomy | 35 (79.6%) | ||
| Total gastrectomy | 9 (20.4%) | ||
| Stomach OP duration (years, mean ± sd) | - | 11.54 ± 9.40 | |
| PTGBD insertion | |||
| No | 1396 (90.5%) | 35 (79.5%) | 0.016 |
| Yes | 147 (9.5%) | 9 (20.5%) | |
| PTGBD insertion (days, mean ± sd) | 8.17 ± 6.79 | 7.33 ± 2.60 | 0.715 |
| Post-op rescue (ERCP) procedure | |||
| No | 1535 (99.5%) | 44 (100.0%) | 0.892 |
| Yes | 8 (0.5%) | 0 (0.0%) | |
| Remnant CBD stone removal | 3 (0.2%) | ||
| Bile leak | 4 (0.25%) | ||
| Bile duct stenosis | 1 (0.05%) | ||
| From ER to operation (days, mean ± sd) | 4.05 ± 4.55 | 4.61 ± 4.63 | 0.415 |
| Postoperative hospital stay (days, mean ± sd) | 5.19 ± 6.89 | 8.20 ± 4.87 | 0.004 |
| Hospital stay (days, mean ± sd) | 9.24 ± 8.92 | 12.82 ± 6.66 | 0.008 |
| Variable | Non-Gastrectomy (n = 1543) | Gastrectomy (n = 44) | p-Value |
|---|---|---|---|
| Cholecystitis severity according to pathologic results | |||
| Gangrenous cholecystitis (gangrenous, ulceration, empyema) | 329 (21.2%) | 11 (26.3%) | 0.683 |
| Acute or chronic cholecystitis | 1190 (78.4%) | 32 (73.7%) | |
| Pathologic details | |||
| Acute cholecystitis | 462 (29.9%) | 15 (34.1%) | NA |
| Chronic cholecystitis | 728 (47.2%) | 17 (38.6%) | |
| Gangrenous GB (gangrenous, ulceration, empyema) | 329 (21.3%) | 11 (25.0%) | |
| GB cancer | 23 (1.5%) | 1 (2.3%) | |
| Other | 1 (0.1%) | 0 (0.0%) | |
| Operation time (min, mean ± sd) | 102.60 ± 52.82 | 164.87 ± 80.03 | <0.001 |
| Surgical approach | |||
| Open surgery | 127 (8.2%) | 17 (38.6%) | <0.001 |
| Laparoscopic surgery | 1416 (91.8%) | 27 (61.4%) | |
| Surgical extent | |||
| Only cholecystectomy | 1487 (96.4%) | 32 (72.7%) | <0.001 |
| Extended surgery | 56 (3.6%) | 12 (27.3%) | |
| Surgical method details | |||
| Open cholecystectomy | 93 (6.0%) | 8 (18.2%) | NA |
| Laparoscopic cholecystectomy | 1394 (90.3%) | 24 (54.5%) | |
| OC + Choledocolithotomy | 26 (1.7%) | 9 (20.5%) | |
| LC + Choledocolithotomy | 22 (1.4%) | 3 (6.8%) | |
| Cholecystectomy with another operation (Small bowel resection, colon resection) | 4 (0.3%) | 0 (0.0%) | |
| Radical cholecystectomy | 4 (0.3%) | 0 (0.0%) | |
| Post-op bile duct problem (leak, stricture) | |||
| No | 1533 (99.4%) | 44 (100.0%) | 0.592 |
| Yes | 10 (0.6%) | 0 (0.0%) | |
| Surgical complication | |||
| No | 1525 (98.8%) | 44 (100.0%) | 0.471 |
| Yes | 18 (1.2%) | 0 (0.0%) | |
| Type of surgical complication | |||
| Leak, fistula, perforation | 12 (0.7%) | 0 (0.0%) | N/A |
| Stricture, obstruction | 1 (0.1%) | 0 (0.0%) | |
| Ileus | 1 (0.1%) | 0 (0.0%) | |
| Bleeding | 3 (0.2%) | 0 (0.0%) | |
| Other | 1 (0.1%) | 0 (0.0%) | |
| ICU admission due to a medical problem | |||
| No | 1531 (99.2%) | 44 (100.0%) | 0.557 |
| Yes | 12 (0.8%) | 0 (0.0%) | |
| ICU admission days (postoperative) | 0.17 ± 1.37 | 0.07 ± 0.26 | 0.686 |
| Area of medical problem | M/A | ||
| Lung | 8 (0.5%) | ||
| Renal | 3 (0.2%) | ||
| Infection | 4 (0.3%) | ||
| Cardio/Vascular | 4 (0.3%) | ||
| Death | |||
| No | 1531 (99.2%) | 44 (100.0%) | 0.557 |
| Yes | 12 (0.8%) | 0 (0.0%) | |
| Clavien–Dindo Classification | |||
| Mild complication (I–III) | 1523 (98.6%) | 44 (100.0%) | 0.526 |
| Severe complication (IV–V) | 21 (1.4%) | 0 (0.0%) | |
| IVa | 7 (0.45%) | 0 (0.0%) | |
| IVb | 2 (0.12%) | 0 (0.0%) | |
| V | 12 (0.83%) | 0 (0.0%) |
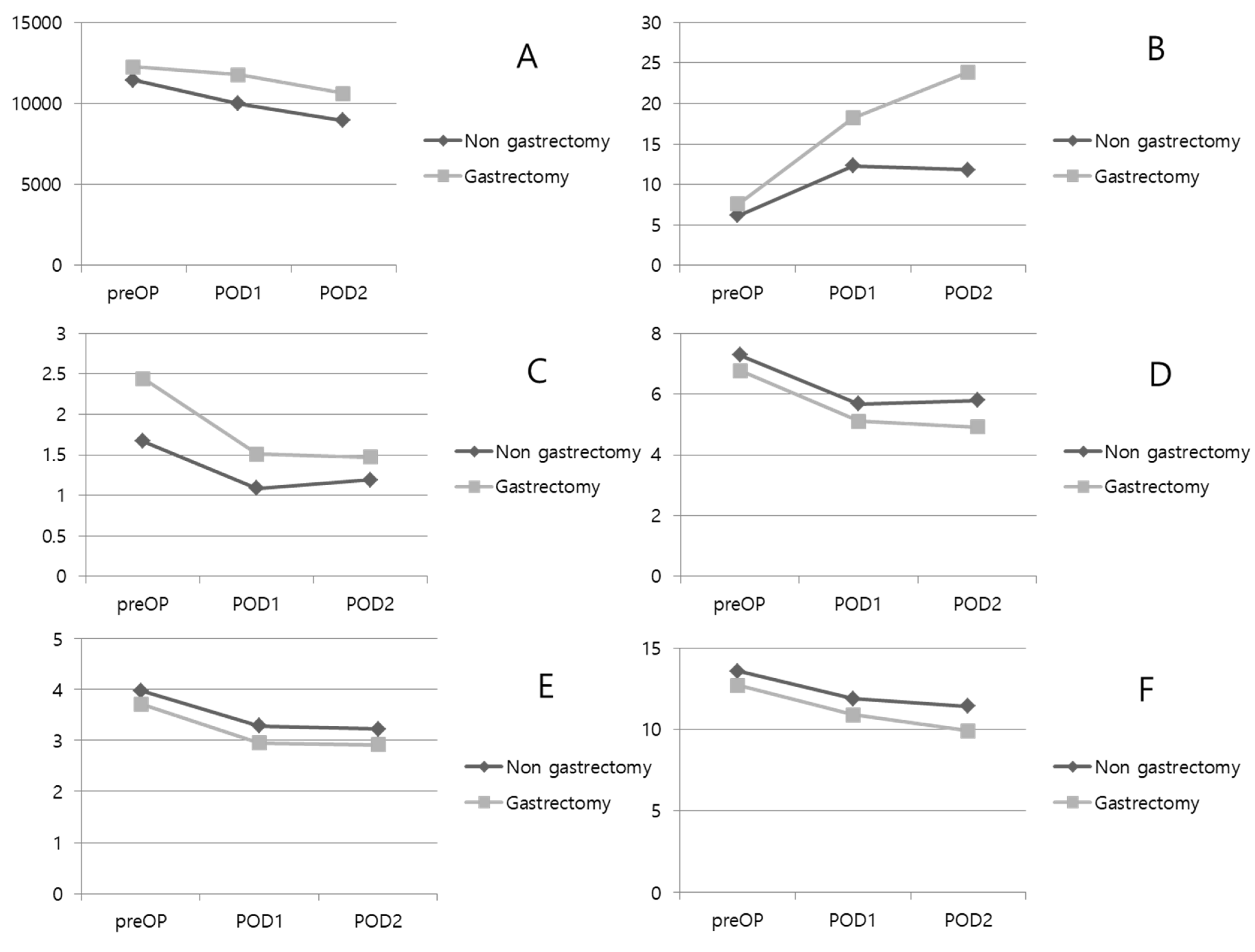
| Variable | Non-Gastrectomy (n = 1543) | Gastrectomy (n = 44) | p-Value |
|---|---|---|---|
| Pre-operative period | |||
| WBC | 11.45 ± 5.22 | 12.27 ± 7.21 | 0.497 |
| CRP | 6.18 ± 8.80 | 7.57 ± 9.57 | 0.332 |
| ANC | 9216.85 ± 5194.38 | 10,541.47 ± 7030.879 | 0.262 |
| Hb | 13.58 ± 1.78 | 12.69 ± 1.84 | 0.003 |
| Protein | 7.28 ± 0.63 | 6.78 ± 0.76 | <0.001 |
| Albumin | 3.98 ± 0.53 | 3.71 ± 0.44 | 0.003 |
| Creatinine | 1.02 ± 0.85 | 0.94 ± 0.39 | 0.566 |
| Bilirubin | 1.67 ± 1.93 | 2.44 ± 2.40 | 0.059 |
| AST | 120.20 ± 200.23 | 211.38 ± 278.12 | 0.055 |
| ALT | 116.84 ± 186.69 | 145.76 ± 158.89 | 0.283 |
| Post-operative day 1 | |||
| WBC | 9.98 ± 3.88 | 11.76 ± 5.17 | 0.043 |
| CRP | 12.32 ± 8.64 | 18.20 ± 9.63 | 0.248 |
| ANC | 8003.79 ± 3919.72 | 10,115.22 ± 5161.68 | 0.017 |
| Hb | 11.89 ± 1.72 | 10.88 ± 1.75 | <0.001 |
| Protein | 5.67 ± 0.66 | 5.11 ± 0.74 | <0.001 |
| Albumin | 3.28 ± 0.52 | 2.95 ± 0.41 | <0.001 |
| Creatinine | 0.98 ± 1.00 | 0.78 ± 0.28 | 0.421 |
| Bilirubin | 1.09 ± 0.99 | 1.51 ± 1.28 | 0.052 |
| AST | 66.39 ± 78.61 | 91.00 ± 103.28 | 0.154 |
| ALT | 71.80 ± 86.91 | 88.84 ± 93.23 | 0.280 |
| Post-operative day 2 | |||
| WBC | 8.94 ± 3.99 | 10.62 ± 5.25 | 0.190 |
| CRP | 11.80 ± 7.54 | 23.89 ± 1.35 | 0.026 |
| ANC | 6726.37 ± 3922.23 | 8878.00 ± 5091.63 | 0.088 |
| Hb | 11.42 ± 1.95 | 9.91 ± 1.62 | 0.015 |
| Protein | 5.80 ± 0.76 | 4.91 ± 0.60 | <0.001 |
| Albumin | 3.22 ± 0.51 | 2.92 ± 0.37 | 0.048 |
| Creatinine | 0.95 ± 0.84 | 0.67 ± 0.28 | 0.328 |
| Bilirubin | 1.19 ± 1.20 | 1.47 ± 1.07 | 0.428 |
| AST | 53.20 ± 79.83 | 63.00 ± 44.18 | 0.685 |
| ALT | 72.70 ± 83.51 | 77.73 ± 73.84 | 0.843 |
| Variable | Non-Gastrectomy (n = 802) | Gastrectomy (n = 33) | p-Value |
|---|---|---|---|
| Age (years, mean ± sd) | 58.66 ± 16.19 | 65.07 ± 13.11 | 0.042 |
| ASA score | 2.55 ± 0.55 | 2.47 ± 0.62 | 0.544 |
| BMI (kg/m2) | 25.50 ± 8.62 | 21.77 ± 2.57 | 0.025 |
| Stomach OP Hx | |||
| Subtotal gastrectomy | 26 (78.8%) | ||
| Total gastrectomy | 7 (21.2%) | ||
| Stomach OP duration (years, mean ± sd) | - | 12.00 ± 10.48 | |
| ICU admission days (days, mean ± sd) | 0.25 ± 1.85 | 0.07 ± 0.27 | 0.612 |
| Operation time (min, mean ± sd) | 109.02 ± 54.54 | 157.41 ± 75.21 | <0.001 |
| Hospital stay (days, mean ± sd) | 9.57 ± 9.15 | 11.22 ± 5.54 | 0.351 |
| From ER to operation (days, mean ± sd) | 4.18 ± 5.08 | 3.74 ± 3.21 | 0.653 |
| Postoperative hospital stay (days, mean ± sd) | 5.39 ± 6.31 | 7.48 ± 5.15 | 0.089 |
| Clavien–Dindo Classification | |||
| Mild complication (I–III) | 789 (98.4%) | 33 (100.0%) | |
| Severe complication (IV–V) | 13 (1.6%) | 0 (0.0%) | |
| Cholecystitis severity according to pathologic results | |||
| Gangrenous cholecystitis (gangrenous, ulceration, empyema) | 209 (26.1%) | 8 (24.2%) | 0.798 |
| Acute or chronic cholecystitis | 584 (72.8%) | 25 (75.8%) | |
| Pathologic details | |||
| Acute cholecystitis | 242 (30.2%) | 13 (39.4%) | NA |
| Chronic cholecystitis | 342 (42.6%) | 12 (36.4%) | |
| Gangrenous GB (gangrenous, ulceration, empyema) | 209 (26.1%) | 8 (24.2%) | |
| GB cancer | 9 (1.1%) | 0 (0.0%) | |
| Surgical approach | |||
| Open surgery | 77 (9.6%) | 12 (36.4%) | <0.001 |
| Laparoscopic surgery | 725 (90.4%) | 21 (63.6%) | |
| Surgical extent | |||
| Only cholecystectomy | 767 (95.6%) | 26 (78.8%) | <0.001 |
| Extended surgery | 35 (4.4%) | 7 (21.2%) | |
| Surgical method details | |||
| Open cholecystectomy | 54 (6.7%) | 6 (18.2%) | NA |
| Laparoscopic cholecystectomy | 713 (88.9%) | 20 (60.6%) | |
| OC + Choledocolithotomy | 20 (2.5%) | 6 (18.2%) | |
| LC + Choledocolithotomy | 12 (1.5%) | 1 (3.0%) | |
| Cholecystectomy with another operation (Small bowel resection, colon resection) | 1 (0.1%) | 0 (0.0%) | |
| Radical cholecystectomy | 2 (0.2%) | 0 (0.0%) |
| Variable | Subtotal Gastrectomy (n = 35) | Total Gastrectomy (n = 9) | p-Value |
|---|---|---|---|
| Age (years, mean ± sd) | 65.51 ± 12.15 | 64.89 ± 10.59 | 0.557 |
| Gender | |||
| Male | 25 (71.4%) | 8 (88.9%) | 0.281 |
| Female | 10 (28.6%) | 1 (11.1%) | |
| BMI (kg/m2) | 21.76 ± 3.48 | 21.27 ± 1.81 | 0.572 |
| Previous gastrectomy type | |||
| Subtotal gastrectomy, Billroth I | 11 (31.4%) | ||
| Subtotal gastrectomy, Billroth II | 19 (54.3%) | ||
| Subtotal gastrectomy, Roux-en-Y | 4 (11.4%) | ||
| Proximal gastrectomy | 1 (2.9%) | ||
| Total gastrectomy, Roux-en-Y | 9 (100%) | ||
| Surgical approach | |||
| Open | 13 (37.1%) | 4 (44.4%) | 0.688 |
| Laparoscopic | 22 (62.9%) | 5 (55.6%) | |
| Surgical extent | |||
| Only cholecystectomy | 26 (74.3%) | 6 (66.7%) | 0.647 |
| Extended surgery | 9 (25.7%) | 3 (33.3%) | |
| ASA score | 2.67 ± 0.48 | 2.20 ± 0.83 | 0.095 |
| Pathologic diagnosis | |||
| Gangrenous cholecystitis (gangrenous, ulceration, empyema) | 9 (25.7%) | 3 (33.3%) | 0.647 |
| Acute or chronic cholecystitis | 26 (74.3%) | 6 (66.7%) | |
| Operation time (min, mean ± sd) | 169.57 ± 80.03 | 158.89 ± 98.29 | 0.735 |
| Gastrectomy duration (years, mean ± sd) | 12.72 ± 10.5 | 7.25 ± 4.80 | 0.040 |
| From ER to operation (days, mean ± sd) | 4.97 ± 4.99 | 3.22 ± 2.63 | 0.159 |
| Postoperative hospital stay (days, mean ± sd) | 8.43 ± 5.26 | 7.33 ± 3.00 | 0.554 |
| Hospital stay (days, mean ± sd) | 13.40 ± 7.34 | 10.56 ± 1.59 | 0.258 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.S.; Cha, B.; Kim, S.H.; Yi, J.W.; Kim, K.D.; Choi, M.S.; Heo, Y.S. Clinical Characteristics of Symptomatic Cholecystitis in Post-Gastrectomy Patients: 11 Years of Experience in a Single Center. Medicina 2022, 58, 1451. https://doi.org/10.3390/medicina58101451
Choi YS, Cha B, Kim SH, Yi JW, Kim KD, Choi MS, Heo YS. Clinical Characteristics of Symptomatic Cholecystitis in Post-Gastrectomy Patients: 11 Years of Experience in a Single Center. Medicina. 2022; 58(10):1451. https://doi.org/10.3390/medicina58101451
Chicago/Turabian StyleChoi, Yun Suk, Boram Cha, Sung Hoon Kim, Jin Wook Yi, Kyeong Deok Kim, Moon Suk Choi, and Yoon Seok Heo. 2022. "Clinical Characteristics of Symptomatic Cholecystitis in Post-Gastrectomy Patients: 11 Years of Experience in a Single Center" Medicina 58, no. 10: 1451. https://doi.org/10.3390/medicina58101451
APA StyleChoi, Y. S., Cha, B., Kim, S. H., Yi, J. W., Kim, K. D., Choi, M. S., & Heo, Y. S. (2022). Clinical Characteristics of Symptomatic Cholecystitis in Post-Gastrectomy Patients: 11 Years of Experience in a Single Center. Medicina, 58(10), 1451. https://doi.org/10.3390/medicina58101451