
Sexual Dysfunction in Women and Men with Psoriasis: A Cross-Sectional Questionnaire-Based Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Assessment of Sexual Problems, Erectile Dysfunction and Quality of Life
2.3. Statistical Analysis
3. Results
3.1. Psoriasis Severity, Location of Psoriatic Lesions and Comorbidities
3.2. Sexual Problems in Patients with Psoriasis
3.3. Erectile Problems
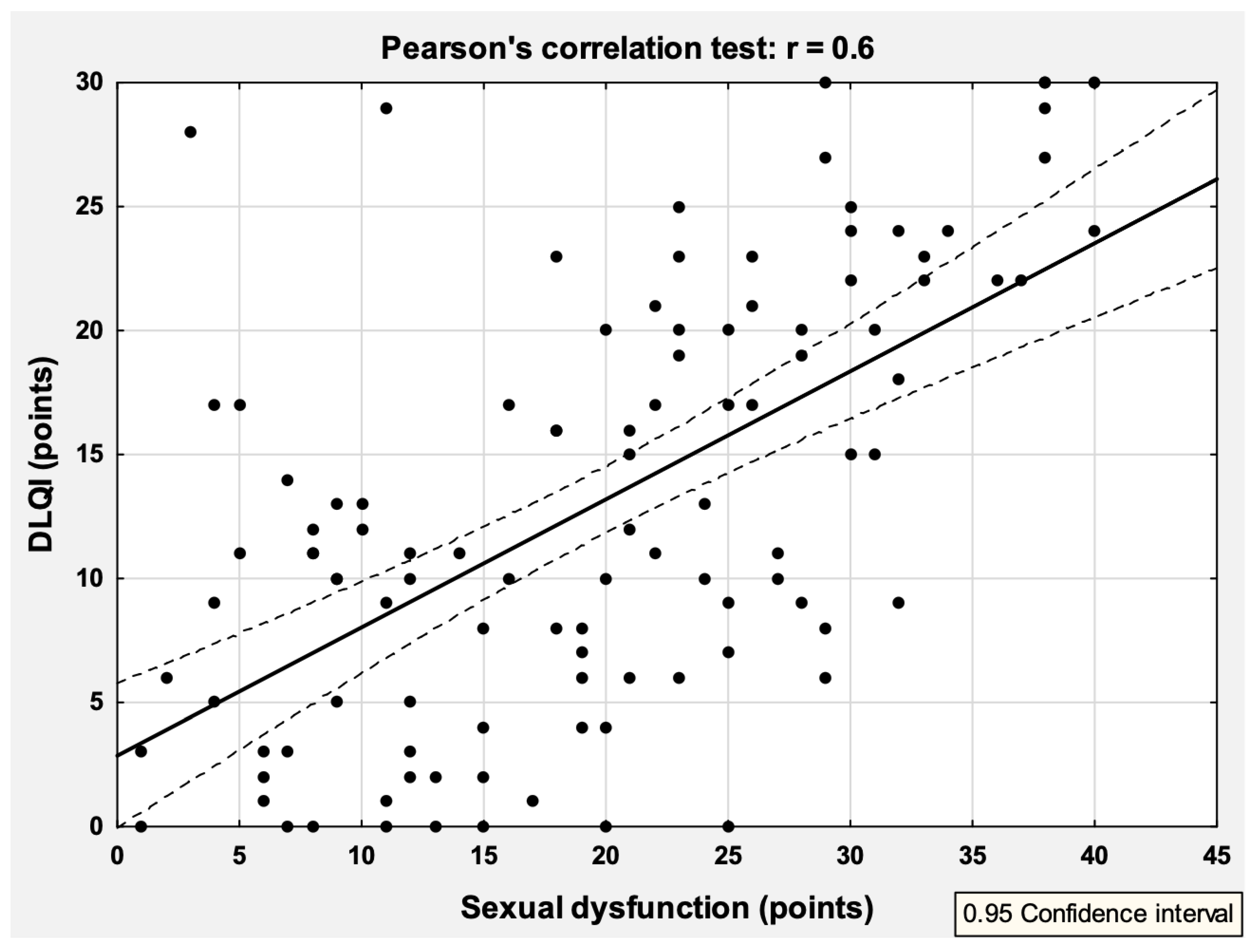
3.4. Correlation between Quality of Life and Sexual Problems
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Damiani, G.; Bragazzi, N.L.; Karimkhani Aksut, C.; Wu, D.; Alicandro, G.; McGonagle, D.; Guo, C.; Dellavalle, R.; Grada, A.; Wong, P.; et al. The Global, Regional, and National Burden of Psoriasis: Results and Insights From the Global Burden of Disease 2019 Study. Front. Med. 2021, 8, 743180. [Google Scholar] [CrossRef] [PubMed]
- Duarte, G.V.; Calmon, H.; Radel, G.; de Fátima Paim de Oliveira, M. Psoriasis and sexual dysfunction: Links, risks, and management challenges. Psoriasis 2018, 8, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Rizzi, M.; Radovanovic, D.; Airoldi, A.; Cristiano, A.; Conic, R.; Petrou, S.; Pigatto, P.D.M.; Bragazzi, N.; Colombo, D.; et al. Psoriasis and respiratory comorbidities: The added value of fraction of exhaled nitric oxide as a new method to detect, evaluate, and monitor psoriatic systemic involvement and therapeutic efficacy. BioMed Res. Int. 2018, 2018, 3140682. [Google Scholar] [CrossRef] [PubMed]
- Conic, R.R.; Damiani, G.; Schrom, K.P.; Ramser, A.E.; Zheng, C.; Xu, R.; McCormick, T.S.; Cooper, K.D. Psoriasis and psoriatic arthritis cardiovascular disease endotypes identified by red blood cell distribution width and mean platelet volume. J. Clin. Med. 2020, 9, 186. [Google Scholar] [CrossRef]
- Damiani, G.; Tacastacas, J.D.; Wuerz, T.; Miller, L.; Fastenau, P.; Bailey, C.; Chawa, M.S.; Argenas, A.; Fiore, M.; Cooper, K.D.; et al. Cognition/psychological burden and resilience in cutaneous T-cell lymphoma and psoriasis patients: Real-life data and implications for the treatment. BioMed Res. Int. 2022, 2022, 8802469. [Google Scholar] [CrossRef] [PubMed]
- Felbo, S.K.; Terslev, L.; Sørensen, I.J.; Skov, L.; Zachariae, C.; Østergaard, M. Musculoskeletal pain in patients with psoriasis and its influence on health-related quality of life: Results from a Danish population-based survey. Acta Derm. Venereol. 2021, 101, adv00553. [Google Scholar] [CrossRef]
- Kodumudi, V.; Rajput, K. Pain management in painful psoriasis and psoriatic arthropathy: Challenging and intricately intertwined issues involving several systems. Curr. Pain Headache Rep. 2021, 25, 36. [Google Scholar] [CrossRef]
- Pojawa-Gołąb, M.; Reich, A. Skin pain in patients with atopic dermatitis or psoriasis: A web-based survey. Acta Derm. Venereol. 2020, 100, adv00258. [Google Scholar] [CrossRef]
- Ermertcan, A.T.; Temeltaş, G.; Deveci, A.; Dinç, G.; Güler, H.B.; Oztürkcan, S. Sexual dysfunction in patients with psoriasis. J. Dermatol. 2006, 33, 772–778. [Google Scholar] [CrossRef]
- Scambler, G.; Heijnders, M.; van Brakel, W.H. Understanding and tackling health-related stigma. Psychol. Health Med. 2006, 11, 269–270. [Google Scholar]
- Hrehorów, E.; Salomon, J.; Matusiak, Ł.; Reich, A.; Szepietowski, J.C. Patients with psoriasis feel stigmatized. Acta Derm. Venereol. 2012, 92, 67–72. [Google Scholar]
- Chen, A.; Beck, K.M.; Tan, E.; Koo, J. Stigmatization in psoriasis. J Psoriasis Psoriatic Arthritis 2018, 3, 100–106. [Google Scholar] [CrossRef]
- Wojciechowska-Zdrojowy, M.; Reid, A.; Szepietowski, J.C.; Wojciechowski, A. Analysis of sexual problems in men with psoriasis. J. Sex Marital Ther. 2018, 44, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Lakshmy, S.; Balasundaram, S.; Sarkar, S.; Audhya, M.; Subramaniam, E. A cross-sectional study of prevalence and implications of depression and anxiety in psoriasis. Indian J. Psychol. Med. 2015, 37, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Schielein, M.C.; Tizek, L.; Schuster, B.; Ziehfreund, S.; Biedermann, T.; Zink, A. Genital psoriasis and associated factors of sexual avoidance—A people-centered cross-sectional study in Germany. Acta Derm. Venereol. 2020, 100, adv00151. [Google Scholar] [CrossRef] [PubMed]
- Kurizky, P.S.; Martins, G.A.; Carneiro, J.N.; Gomes, C.M.; da Mota, L.M.H. Evaluation of the occurrence of sexual dysfunction and general quality of life in female patients with psoriasis. An. Bras. Dermatol. 2018, 93, 801–806. [Google Scholar] [CrossRef]
- Halioua, B.; Maccari, F.; Fougerousse, A.C.; Parier, J.; Reguiai, Z.; Taieb, C.; Esteve, E. Impact of patient psoriasis on partner quality of life, sexuality and empathy feelings: A study in 183 couples. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2044–2050. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Mercan, S.; Altunay, I.K.; Demir, B.; Akpinar, A.; Kayaoglu, S. Sexual dysfunctions in patients with neurodermatitis and psoriasis. J. Sex Marital Ther. 2008, 34, 160–168. [Google Scholar] [CrossRef]
- Łakuta, P.; Marcinkiewicz, K.; Bergler-Czop, B.; Brzezińska-Wcisło, L. How does stigma affect people with psoriasis? Postep. Dermatol. Alergol. 2017, 34, 36–41. [Google Scholar] [CrossRef]
- Jankowiak, B.; Kowalewska, B.; Krajewska-Kułak, E.; Kowalczuk, K.; Khvorik, D.F. The sense of stigmatization in patients with plaque psoriasis. Dermatology 2021, 237, 611–617. [Google Scholar] [CrossRef]
- Lim, D.S.; Bewley, A.; Oon, H.H. Psychological profile of patients with psoriasis. Ann. Acad. Med. Singap. 2018, 47, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Salvador-Rodriguez, L.; Martinez-Lopez, A. Association between psoriasis and sexual and erectile dysfunction in epidemiologic studies a systematic review. JAMA Dermatol. 2019, 155, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Meeuwis, K.A.; de Hullu, J.A.; van de Nieuwenhof, H.P.; Evers, A.W.; Massuger, L.F.; van de Kerkhof, P.C.; van Rossum, M. Quality of life and sexual health in patients with genital psoriasis. Br. J. Dermatol. 2011, 164, 1247–1255. [Google Scholar] [CrossRef]
- Bardazzi, F.; Odorici, G.; Ferrara, F.; Magnano, M.; Balestri, R.; Patrizi, A. Sex and the PASI: Patients affected by a mild form of psoriasis are more predisposed to have a more severe form of erectile dysfunction. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Almodovar-Real, A.; Ruiz-Carrascosa, J.C.; Naranjo-Sintes, R.J.; Jimenez-Moleon, J.J. Prevalence and associated factors of erectile dysfunction in patients with moderate to severe psoriasis and healthy population: A comparative study considering physical and psychological factors. Arch. Sex. Behav. 2016, 45, 2047–2055. [Google Scholar] [CrossRef]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; et al. Erectile dysfunction. Nat. Rev. Dis. Primers 2016, 2, 16003. [Google Scholar] [CrossRef]
- Kennedy, S.H.; Rizvi, S. Sexual dysfunction, depression, and the impact of antidepressants. J. Clin. Psychopharmacol. 2009, 29, 157–164. [Google Scholar] [CrossRef]


{kind=link}
| Age (Years) [Mean ± Standard Deviation (Min–Max)] | 48.0 ± 13.4 (18–76) |
|---|---|
| Psoriasis duration (years) [mean ± standard deviation (min-max)] | 19.0 ± 12.1 (1–55) |
| Education | |
| Primary school | 10 (9.2%) |
| Secondary school | 30 (27.5%) |
| High school | 38 (34.9%) |
| University | 31 (28.4%) |
| Domicile | |
| Countryside | 46 (42.2%) |
| A city with up to 50,000 inhabitants | 26 (23.9%) |
| A city with 50–150,000 inhabitants | 9 (8.3%) |
| A city with over 150,000 inhabitants | 28 (25.6%) |
| Earnings | |
| Earnings lower than PLN 2000 | 36 (33.0%) |
| Earnings from PLN 2000 to 5000 | 61 (56.0%) |
| Earnings from PLN 5000 to 10,000 | 9 (8.2%) |
| Earnings above PLN 10,000 | 3 (2.8%) |
| Marital status | |
| Single | 23 (21.1%) |
| Married | 65 (59.6%) |
| Divorced/Separated | 13 (11.9%) |
| Widow/Widower | 6 (5.5%) |
| Comorbidities | |
| Cardiovascular disease | 26 (23.9%) |
| Diabetes | 16 (14.7%) |
| Prostate adenoma | 2 (1.8%) |
| Malignancy | 3 (2.8%) |
| Other (endocrine, neurological, autoimmune diseases) | 23 (21.1%) |
| Psoriasis outbreaks during the year | |
| One or two per year | 72 (66.1%) |
| More than two per year | 8 (7.3%) |
| All the time (no remissions) | 17 (15.6%) |
| No recurrences of the disease (first psoriasis episode) | 6 (5.5%) |
| No answer | 6 (5.5%) |
| Specific location of skin lesions | |
| Face | 39 (35.8%) |
| Hands | 62 (56.9%) |
| Genital area | 50 (45.9%) |
| Scalp | 80 (73.4%) |
| Nails | 55 (50.5%) |
| Type of psoriasis * | |
| Plaque-type psoriasis | 91 (83.5%) |
| Palmoplantar pustular psoriasis | 14 (12.8%) |
| Psoriatic arthritis | 18 (16.5%) |
| Nail psoriasis | 16 (14.7%) |
| Scalp psoriasis | 28 (25.7%) |
| Family history of psoriasis | |
| Yes | 45 (41.3%) |
| No | 64 (58.7%) |
| Patient’s assessment of the psoriasis severity | |
| Mild | 8 (7.3%) |
| Moderate | 32 (29.4%) |
| Severe | 69 (63.3%) |
| Never | Occasionally | Sometimes | Often | All the Time | Missing Data | |
|---|---|---|---|---|---|---|
| Has your skin condition ever affected your sex life? | 19 (17.4%) | 20 (18.3%) | 21 (19.3%) | 32 (29.4%) | 14 (12.8%) | 3 (2.8%) |
| Do you think other people considered your skin problem as contagious disease? | 9 (8.3%) | 11 (10.1%) | 35 (32.1%) | 33 (30.3%) | 19 (17.4%) | 2 (1.8%) |
| Do you avoid social contacts because of your skin problem? | 24 (22.0%) | 24 (22.0%) | 22 (20.2%) | 25 (22.9%) | 12 (11.0%) | 2 (1.8%) |
| Do you avoid sexual contacts because of your skin problem? | 24 (22.0%) | 19 (17.4%) | 30 (27.5%) | 24 (22.0%) | 8 (7.3%) | 4 (3.7%) |
| Do you feel ashamed of your skin when you are together with your sexual partner? | 26 (23.9%) | 16 (14.7%) | 20 (18.3%) | 31 (28.4%) | 12 (11.0%) | 4 (3.7%) |
| Do you experience rejection due to your skin condition? | 42 (38.5%) | 15 (13.8%) | 30 (27.5%) | 13 (11.9%) | 6 (5.5%) | 3 (2.8%) |
| Are you stressed before sexual intercourse because of your skin condition? | 27 (24.8%) | 22 (20.2%) | 17 (15.6%) | 25 (22.9%) | 14 (12.8%) | 4 (3.7%) |
| Not at All | Yes, a Little | Yes, Markedly | Yes, Very Much | Missing Data | |
|---|---|---|---|---|---|
| Do you feel unattractive because of your skin disease? | 6 (5.5%) | 31(28.4%) | 34 (31.2%) | 36 (33.0%) | 2 (1.8%) |
| Do you feel embarrassed when skin lesions occur on visible body areas? | 5 (4.6%) | 33 (30.3%) | 30 (27.5%) | 39 (35.8%) | 2 (1.8%) |
| Do you feel embarrassed when skin lesions occur in the genital area? | 15 (13.8%) | 22 (20.2%) | 38 (34.9%) | 30 (27.5%) | 4 (3.7%) |
| Has your sexual activity decreased because of the skin problem? | 31 (28.4%) | 41 (37.6%) | 24 (22.0%) | 9 (8.3%) | 4 (3.7%) |
| Sexual Problems | p | DLQI | p | IIEF | p | |
|---|---|---|---|---|---|---|
| Age (years) | r = −0.03 | 0.77 | r = −0.08 | 0.39 | r = −0.33 | 0.01 |
| Psoriasis duration (years) | r = 0.06 | 0.51 | r = −0.02 | 0.87 | r = 0.0 | 1 |
| PASI (scores) | r = 0.2 | 0.04 | r = 0.36 | <0.001 | r = −0.15 | 0.24 |
| Gender | ||||||
| -Female | 20.6 ± 10.3 | 0.37 | 14.1 ± 8.7 | 0.26 | - | - |
| -Male | 18.8 ± 10.1 | 12.2 ± 8.7 | ||||
| Education | ||||||
| -Primary school | 19.2 ± 12.6 | 0.71 | 11.4 ± 9.5 | 0.71 | 13.0 ± 6.0 | <0.001 |
| -Secondary school | 21.4 ± 9.9 | 13.7 ± 8.0 | 18.3 ± 4.8 | |||
| -High school | 18.8 ± 10.2 | 12.0 ± 7.9 | 22.1 ± 2.6 | |||
| -University | 18.7 ± 10.0 | 14.0 ± 10.1 | 22.6 ± 4.9 | |||
| Domicile | ||||||
| -Countryside | 18.2 ± 10.9 | 0.71 | 13.0 ± 8.2 | 0.08 | 20.3 ± 4.6 | 0.26 |
| -A city with up to 50,000 inhabitants | 20.5 ± 7.9 | 9.7 ± 8.1 | 18.4 ± 6.3 | |||
| -A city with 50–150,000 inhabitants | 20.3 ± 10.1 | 16.2 ± 6.6 | 18.4 ± 6.4 | |||
| -A city with over 150,000 inhabitants | 20.7 ± 11.2 | 15.1 ± 9.9 | 22.1 ± 2.9 | |||
| Earnings | ||||||
| -Earnings lower than PLN 2000 | 19.7 ± 9.9 | 0.72 | 12.2 ± 7.6 | <0.05 | 15.9 ± 6.4 | <0.01 |
| -Earnings from PLN 2000 to 5000 | 20.0 ± 10.9 | 14.6 ± 9.4 | 21.4 ± 3.3 | |||
| -Earnings from PLN 5000 to 10,000 | 18.2 ± 7.4 | 6.7 ± 6.1 | 20.9 ± 5.3 | |||
| -Earnings above PLN 10,000 | 13.3 ± 6.7 | 9.3 ± 3.1 | 22.5 ± 3.5 | |||
| Marital status | ||||||
| -Single | 21.1 ± 10.4 | <0.05 | 14.0 ± 8.9 | 0.27 | 18.6 ± 6.7 | <0.001 |
| -Married | 18.2 ± 9.6 | 12.5 ± 8.7 | 21.3 ± 3.2 | |||
| -Divorced/Separated | 25.8 ± 10.6 | 16.1 ± 9.2 | 19.1 ± 5.0 | |||
| -Widow/Widower | 14.7 ± 10.7 | 8.3 ± 5.0 | 7.5 ± 2.1 | |||
| Cardiovascular disease | ||||||
| -Yes | 18.2 ± 9.8 | 0.43 | 11.0 ± 7.2 | 0.18 | 16.4 ± 5.9 | <0.01 |
| -No | 20.0 ± 10.3 | 13.6 ± 9.1 | 20.9 ± 4.5 | |||
| Diabetes | ||||||
| -Yes | 18.8 ± 10.5 | 0.74 | 10.9 ± 7.8 | 0.29 | 18.3 ± 5.8 | 0.24 |
| -No | 19.7 ± 10.2 | 13.4 ± 8.8 | 20.4 ± 4.9 | |||
| Location of skin lesions | ||||||
| -Face | 22.4 ± 9.0 | 0.03 | 14.9 ± 8.5 | 0.1 | 19.6 ± 5.6 | 0.69 |
| -Hands | 21.2 ± 10.7 | 0.05 | 14.7 ± 9.0 | 0.02 | 20.1 ± 4.8 | 0.94 |
| -Genital area | 22.2 ± 10.3 | 0.01 | 15.8 ± 8.8 | 0.001 | 19.3 ± 5.8 | 0.4 |
| -Scalp | 19.6 ± 10.3 | 0.91 | 13.8 ± 8.9 | 0.09 | 20.6 ± 5.0 | 0.18 |
| -Nails | 20.5 ± 9.6 | 0.31 | 12.8 ± 8.8 | 0.83 | 20.7 ± 4.7 | 0.3 |
| Type of psoriasis | ||||||
| -Plaque-type psoriasis | 19.9 ± 10.4 | 0.47 | 12.8 ± 9.0 | 0.75 | 20.3 ± 5.0 | 0.45 |
| -Palmoplantar pustular psoriasis | 17.1 ± 9.9 | 0.36 | 12.5 ± 8.7 | 0.86 | 20.3 ± 5.6 | 0.97 |
| -Psoriatic arthritis | 20.9 ± 7.5 | 0.54 | 12.3 ± 8.3 | 0.74 | 20.2 ± 3.7 | 0.9 |
| -Nail psoriasis | 18.9 ± 11.2 | 0.8 | 10.9 ± 8.6 | 0.33 | 22.8 ± 2.7 | 0.1 |
| -Scalp psoriasis | 19.0 ± 11.1 | 0.78 | 13.4 ± 9.1 | 0.78 | 23.2 ± 1.7 | 0.02 |
| Family history of psoriasis | ||||||
| -Yes | 18.5 ± 10.3 | 0.36 | 12.7 ± 8.7 | 0.76 | 20.8 ± 5.0 | 0.27 |
| -No | 20.3 ± 10.1 | 13.2 ± 8.7 | 19.4 ± 5.1 | |||
| Patient’s assessment of psoriasis severity | ||||||
| -Mild | 11.5 ± 9.0 | 0.001 | 3.6 ± 3.4 | <0.001 | 18.2 ± 6.2 | 0.63 |
| -Moderate | 16.2 ± 9.1 | 9.8 ± 7.9 | 20.4 ± 4.7 | |||
| -Severe | 22.1 ± 9.9 | 15.6 ± 8.3 | 20.1 ± 5.1 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kędra, K.; Janeczko, K.; Michalik, I.; Reich, A. Sexual Dysfunction in Women and Men with Psoriasis: A Cross-Sectional Questionnaire-Based Study. Medicina 2022, 58, 1443. https://doi.org/10.3390/medicina58101443
Kędra K, Janeczko K, Michalik I, Reich A. Sexual Dysfunction in Women and Men with Psoriasis: A Cross-Sectional Questionnaire-Based Study. Medicina. 2022; 58(10):1443. https://doi.org/10.3390/medicina58101443
Chicago/Turabian StyleKędra, Kamila, Kinga Janeczko, Izabela Michalik, and Adam Reich. 2022. "Sexual Dysfunction in Women and Men with Psoriasis: A Cross-Sectional Questionnaire-Based Study" Medicina 58, no. 10: 1443. https://doi.org/10.3390/medicina58101443
APA StyleKędra, K., Janeczko, K., Michalik, I., & Reich, A. (2022). Sexual Dysfunction in Women and Men with Psoriasis: A Cross-Sectional Questionnaire-Based Study. Medicina, 58(10), 1443. https://doi.org/10.3390/medicina58101443