A Telemedicine Approach to Covid-19 Assessment and Triage

 ,
, 
Abstract
1. Introduction
2. Covid-19 Presentation
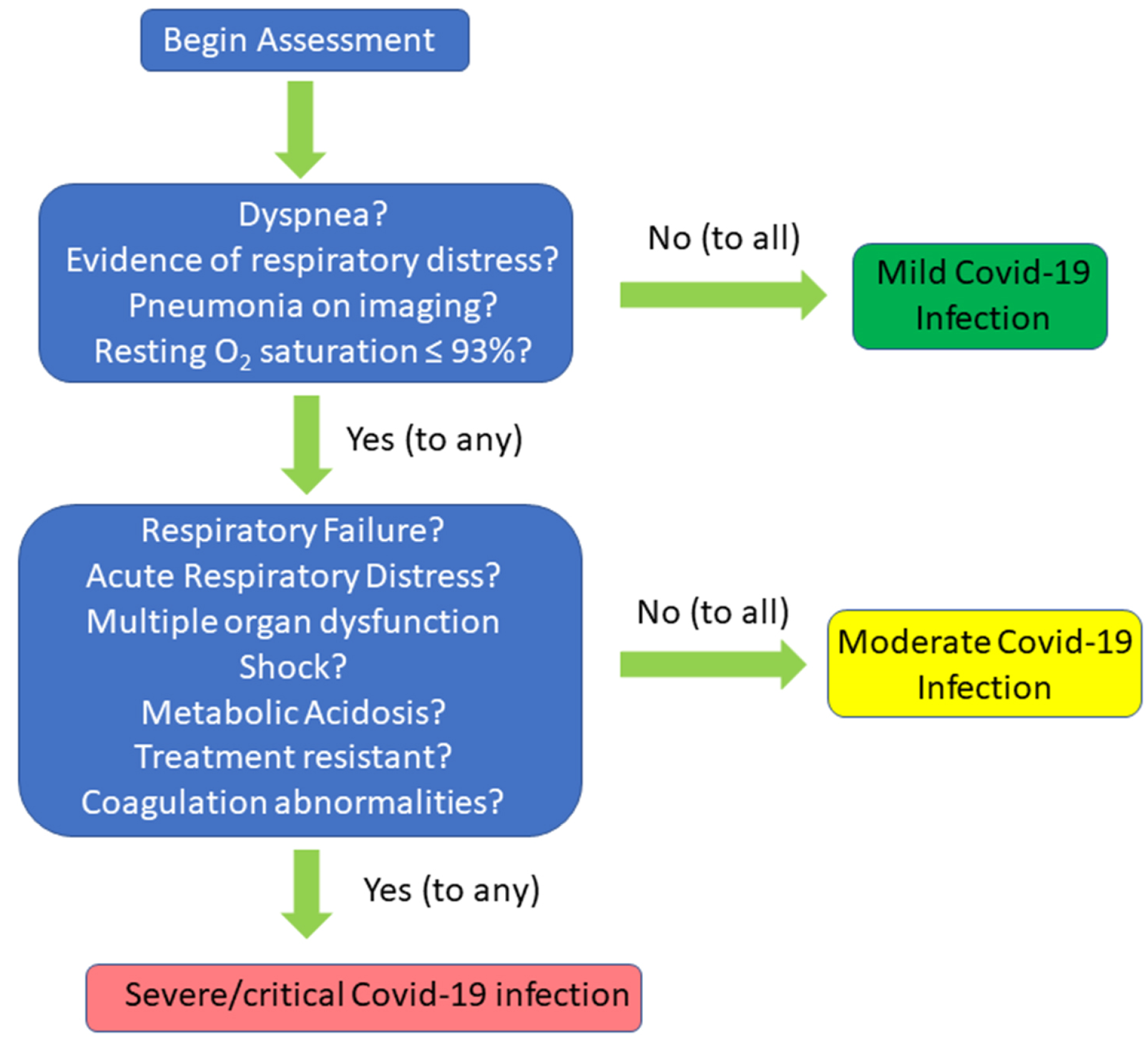
3. Criteria for Determining Severity
4. Covid-19 Risk Factors
5. Laboratory Findings and Imaging
6. The Telemedicine Evaluation
6.1. Initial Screen
- (1)
- Temperature Check
- (2)
- Covid-19 Screening Questions
6.2. Virtual Visit
6.2.1. Introduction, Consent, Symptom Check, Demographics
- Introduction: The physician greets the patient and introduces themselves. The patient’s location, name and date of birth are confirmed. The patient is asked whether an interpreter is needed and, if so, an interpreter is provided via a certified interpretation service (conferenced into the call).
- Consent: It is explained to the patient that to provide necessary care the virtual visit will be conducted as a replacement for an onsite visit in order to maintain the patient’s safety and the safety of our staff. Verbal consent to proceed with the virtual visit must be obtained. The provider advises the patients of the risks and benefits of the virtual visit. If the patient consents, then the provider documents that the patient understands the risks and benefits of the virtual/telephone visit as discussed and consents to the visit.
- Vital Information—It is helpful if the patient is able to assess their temperature and oxygen saturation. To assess oxygen saturation patients discharged with home oxygen are provided a pulse oximeter at the time of discharge.
- Symptoms—The assessment of the patient’s symptoms are based on Centers for Disease Control (CDC) guidelines [79]. This assessment is similar to the assessment done at the time of Covid-19 screening. Key symptoms that raise the index of suspicion for Covid-19 infection is answering “Yes” to ANY ONE of the highest priority questions or ANY TWO of the high priority symptoms in Table 1.
- Assessing clinical stability—it is important to identify patients who need an immediate onsite evaluation at a designated screening center or a hospital emergency department. These are locations where in-person Covid-19 evaluation and testing can take place. The following questions help determine which patients are unstable and need an immediate in-person evaluation:
- Is the oxygen saturation less than 90%?
- Is the temperature greater than or equal to 102 °F and not responding to antipyretics?
- Demographic data—data collected is based on factors that have been shown to be related to a higher incidence and/or severity of Covid-19 disease and must be taken into account in risk assessment as noted below.
- ○
- Age—greater than 65 are considered “vulnerable”
- ○
- Sex—males affected greater than females.
- ○
- Country of origin or race if relevant—endemic areas with high incidence. African-Americans and Hispanics are disproportionately affected.
- ○
- Travel history—pertinent if traveled to an endemic area. Recent travel (within the last 14 days)—Either international travel or travel within the United States, dates of travel, and destination.
6.2.2. The Telemedicine Medical History
- Chief complaint: reason for the visit in the patient’s own words.
- History of present illness (HPI): What symptoms are you experiencing and how long have you had these symptoms?
- In addition to the symptoms covered earlier, are you experiencing any of the following?
- ○
- Diarrhea
- ○
- Abdominal pain
- ○
- Nausea or vomiting
- Significant past medical history (PMH) (Table 2)
- List current medications
- Allergies
- Family history
6.2.3. The Telemedicine Physical Exam
7. Laboratory Testing
8. Patients Requiring Self-isolation or Quarantine
8.1. How to Self-Isolate/Quarantine
- Stay at home. Take every possible step to reduce going into public spaces. Avoid contact with others. Do not let anyone visit you in your home until your self-isolation/quarantine is over.
- Practice social distancing. If you have to leave your home, practice social distancing. This means trying to maintain a six-foot distance from others. Avoid using any kind of public transportation whenever you can. This includes ridesharing services and taxis.
- Practice good hygiene. Always cover your nose and mouth when you cough or sneeze. Use the crook of your arm (inside your elbow). Do not cough and sneeze into your hand. Wash your hands afterwards.
- Wash your hands. You should be washing your hands often with soap and water for at least 20 s. If soap and water are not available, use an alcohol-based sanitizer. Make sure that it contains at least 60% alcohol.
- Avoid sharing personal items. Do not share eating utensils and other personal items such as toothbrushes, drinking glasses, and water bottles.
- Clean surfaces. Disinfect surfaces you touch often such as cell phones, doorknobs, light switches, counters, tabletops, etc. Wash your clothes, bath and kitchen towels, clothes you sleep in, bedsheets and pillowcases regularly.
- Rest and drink plenty of fluids to stay hydrated.
- Monitor your health. If you develop any symptoms or they get worse, call your health care provider or make an appointment with your virtual urgent care provider.
8.2. If You are Having Any Symptoms Such as Fever or Cough Follow These Additional Instructions:
- If there is an older adult (over the age of 65) in your home with organ failure, a weakened immune system or uncontrolled diabetes, this person should not share living space with you. If that is not possible, avoid close contact. Have separate sleeping arrangements. Prepare and eat meals separately as well. Use a separate bathroom if possible.
- If you must share a living space with high-risk family members, wear a mask when you are near them. Have as little contact with these people as possible until you no longer have a fever and cough.
- If you must leave your home and you are having any symptoms, wear a face mask, goggles and/or face shield.
8.3. When Can You Stop Self-Isolation/Quarantine?
- You have had no fever for 72 h (three full days) without the use of fever reducing medicines
- Other symptoms such as cough or shortness of breath have gotten better or are almost gone
- At least seven (7) days have passed since you first started having symptoms. Call your healthcare provider with any questions or if you are unsure whether you can stop self-isolation/quarantine
9. Management
10. Limitations of Telemedicine
11. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early transmission dynamics in wuhan, china, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Krajewska, J.; Krajewski, W.; Zub, K.; Zatoński, T. COVID-19 in otolaryngologist practice: A review of current knowledge. Eur. Arch. Oto Rhino Laryngol. 2020, 277, 1885–1897. [Google Scholar] [CrossRef] [PubMed]
- Hailey, D.; Roine, R.; Ohinmaa, A. Systematic review of evidence for the benefits of telemedicine. J. Telemed. Telecare 2002, 8, 1–7. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Zhang, P. Telemedicine in clinical setting. Exp. Ther. Med. 2016, 12, 2405–2407. [Google Scholar] [CrossRef]
- WHO. Telemedicine-Opportunities and Developments in Member States, 2nd ed.; WHO Press: Geneva, Switzerland, 2010; Available online: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf (accessed on 8 January 2020).
- Gutiérrez, J.; Kuperman, E.; Kaboli, P.J. Using telehealth as a tool for rural hospitals in the COVID-19 pandemic response. J. Rural. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Crump, W.J. Telemedicine: Has the time really finally arrived? J. Rural. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 pandemic, lessons for the future. Telemed. e-Health 2020, 26, 571–573. [Google Scholar] [CrossRef]
- Parmet, W.E.; Sinha, M.S. Covid-19—The law and limits of quarantine. N. Engl. J. Med. 2020, 382, e28. [Google Scholar] [CrossRef]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci 2020, 63, 706–711. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019-novel coronavirus (2019-nCoV) peumonia in Wuhan, China. SSRN Electron. J. 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Beltran-Corbellini, A.; Chico-García, J.L.; Martínez-Poles, J.; Rodríguez-Jorge, F.; Natera-Villalba, E.; Gómez-Corral, J.; Gómez-López, A.; Monreal, E.; Parra-Díaz, P.; Cortés-Cuevas, J.L.; et al. Acute-onset smell and taste disorders in the context of COVID-19: A pilot multicentre polymerase chain reaction based case–control study. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Heidari, F.; Karimi, E.; Firouzifar, M.; Khamushian, P.; Ansari, R.; Ardehali, M.M. Anosmia as a prominent symptom of COVID-19 infection. Rhinol. J. 2020, 58, 302–303. [Google Scholar] [CrossRef]
- Wee, L.E.; Chan, Y.F.Z.; Teo, N.W.Y.; Cherng, B.P.Z.; Thien, S.Y.; Wong, H.M.; Wijaya, L.; Toh, S.T.; Tan, T.T. The role of self-reported olfactory and gustatory dysfunction as a screening criterion for suspected COVID-19. Eur. Arch. Oto Rhino Laryngol. 2020, 277, 1–2. [Google Scholar] [CrossRef]
- Henry, B.M.; De Oliveira, M.H.S.; Benoit, J.; Lippi, G. Gastrointestinal symptoms associated with severity of coronavirus disease 2019 (COVID-19): A pooled analysis. Intern. Emerg. Med. 2020, Apr17, 1–3. [Google Scholar] [CrossRef]
- Wei, X.S.; Wang, X.; Niu, Y.R.; Ye, L.L.; Peng, W.B.; Wang, Z.H.; Yang, W.B.; Yang, B.H.; Zhang, J.C.; Ma, W.L.; et al. Diarrhea is associated with prolonged symptoms and viral carriage in COVID-19. Clin. Gastroenterol. Hepatol. 2020, 18, 1753–1759. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef]
- Han, C.; Duan, C.; Zhang, S.; Spiegel, B.; Shi, H.; Wang, W.; Zhang, L.; Lin, R.; Liu, J.; Ding, Z.; et al. Digestive symptoms in COVID-19 patients with mild disease severity. Am. J. Gastroenterol. 2020, 115, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.; Dávalos, F.; Berumen, J. Beware: Gastrointestinal symptoms can be a manifestation of COVID-19. Rev. Gastroenterol. Mex. 2020, 85, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef]
- Jiang, X.-L.; Zhang, X.-L.; Zhao, X.-N.; Li, C.-B.; Lei, J.; Kou, Z.-Q.; Sun, W.-K.; Hang, Y.; Gao, F.; Ji, S.-X.; et al. Transmission potential of asymptomatic and paucisymptomatic SARS-CoV-2 infections: A three-family cluster study in China. J. Infect. Dis 2020, 22, 1948–1952. [Google Scholar] [CrossRef]
- Wu, J.; Liang, J.; Zhou, H.; Peng, F.; Wang, B.; Jiang, W.; Jia, B.; Luo, T. Clinical features and outcomes of asymptomatic cases of SARS-CoV-2 infection. J. Infect. 2020, 81, e102–e103. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef]
- Hong, D.; Long, L.; Wang, A.Y.; Lei, Y.; Tang, Y.; Zhao, J.W.; Song, X.; He, Y.; Wen, E.; Zheng, L.; et al. Kidney manifestations of mild, moderate and severe coronavirus disease 2019: A retrospective cohort study. Clin. Kidney J. 2020, 13, 340–346. [Google Scholar] [CrossRef]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med Res. 2020, 7, 1–23. [Google Scholar] [CrossRef]
- Duan, J.; Wang, X.; Chi, J.; Chen, H.; Bai, L.; Hu, Q.; Han, X.; Hu, W.; Zhu, L.; Wang, X.; et al. Correlation between the variables collected at admission and progression to severe cases during hospitalization among patients with COVID-19 in Chongqing. J. Med. Virol. 2020, 10. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Bhat, R.; Hamid, A.; Kunin, J.R.; Saboo, S.; Batra, K.; Baruah, D.; Bhat, A.P. Chest imaging in patients hospitalized with COVID-19 infection—A case series. Curr. Probl. Diagn. Radiol. 2020, 49, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Niu, S.; Tian, S.; Lou, J.; Kang, X.; Zhang, L.; Lian, H.; Zhang, J. Clinical characteristics of older patients infected with COVID-19: A descriptive study. Arch. Gerontol. Geriatr. 2020, 89, 104058. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020. [Google Scholar] [CrossRef]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef]
- Borges do Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; Von Groote, T.C.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marušić, A.; Jerončić, A.; et al. Novel coronavirus infection (COVID-19) in humans: A scoping review and meta-analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef]
- Channappanavar, R.; Fett, C.; Mack, M.; Eyck, P.T.; Meyerholz, D.K.; Perlman, S. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. J. Immunol. 2017, 198, 4046–4053. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y.-N. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Shenoy, A.; Ismaily, M.; Bajaj, M. Diabetes and covid-19: A global health challenge. BMJ Open Diabetes Res. Care 2020, 8, e001450. [Google Scholar] [CrossRef]
- Smith, A.A.; Fridling, J.; Ibhrahim, D.; Porter, P.S. Identifying patients at greatest risk of mortality due to COVID-19: A New England perspective. West. J. Emerg. Med. 2020, 21, 785–789. [Google Scholar] [CrossRef]
- Figliozzi, S.; Masci, P.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.; Caforio, A.L.; Georgiopoulos, G. Predictors of adverse prognosis in Covid-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 13362. [Google Scholar] [CrossRef]
- Butt, N.; Arshid, A.; Ahmad, S.A.; Khalid, N.; Kayani, W.T. Cardiovascular complications in COVID-19. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Anderson, M.; Geleris, J.; Anderson, D.; Zucker, J.; Nobel, Y.R.; Freedberg, D.; Small-Saunders, J.; Rajagopalan, K.N.; Greendyk, R.; Chae, S.-R.; et al. Body mass index and risk for intubation or death in SARS-CoV-2 infection. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Pilling, L.C.; Kuo, C.-L.; Kuchel, G.A.; Melzer, D. Preexisting comorbidities predicting COVID-19 and mortality in the UK biobank community cohort. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2020, 183. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Emami, A.; Javanmardi, F.; Pirbonyeh, N.; Akbari, A. Prevalence of underlying diseases in hospitalized patients with COVID-19: A systematic review and meta-analysis. Arch. Acad. Emerg. Med. 2020, 8, e35. [Google Scholar] [PubMed]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Van Dam, P.A.; Huizing, M.; Mestach, G.; Dierckxsens, S.; Tjalma, W.; Trinh, X.B.; Papadimitriou, K.; Altintas, S.; Vermorken, J.; Vulstekeb, C.; et al. SARS-CoV-2 and cancer: Are they really partners in crime? Cancer Treat. Rev. 2020, 89, 102068. [Google Scholar] [CrossRef] [PubMed]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; Lopes, G.D.L.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Lippi, G.; Simundic, A.-M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef]
- Ravi, N.; Cortade, D.L.; Ng, E.; Wang, S.X. Diagnostics for SARS-CoV-2 detection: A comprehensive review of the FDA-EUA COVID-19 testing landscape. Biosens. Bioelectron. 2020, 165, 112454. [Google Scholar] [CrossRef]
- Bustin, S.A.; Nolan, T. RT-qPCR Testing of SARS-CoV-2: A Primer. Int. J. Mol. Sci. 2020, 21, 3004. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef]
- Jesenak, M.; Brndiarova, M.; Urbancikova, I.; Rennerova, Z.; Vojtkova, J.; Bobcakova, A.; Ostro, R.; Banovcin, P. Immune parameters and COVID-19 infection—Associations with clinical severity and disease prognosis. Front. Microbiol. 2020, 10, 364. [Google Scholar] [CrossRef]
- Cao, W.; Li, T. COVID-19: Towards understanding of pathogenesis. Cell Res. 2020, 30, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Qiu, P.; Zhou, Y.; Wang, F.; Wang, H.; Zhang, M.; Pan, X.; Zhao, Q.; Liu, J. Clinical characteristics, laboratory outcome characteristics, comorbidities, and complications of related COVID-19 deceased: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2020, 1–10. [Google Scholar] [CrossRef]
- Lapić, I.; Rogić, D.; Plebani, M. Erythrocyte sedimentation rate is associated with severe coronavirus disease 2019 (COVID-19): A pooled analysis. Clin. Chem. Lab. Med. 2020, 58, 1146–1148. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Zhang, W.; Jin, R.; Liang, L.; Xu, B.; Hu, Z. Risk factors for disease progression in hospitalized patients with COVID-19: A retrospective cohort study. Infect. Dis. 2020, 52, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Li, S.; Sun, Q.; Zhu, J.; Chen, B.; Xiong, M.; Cao, G. Immune-Inflammatory parameters in COVID-19 Cases: A systematic review and meta-analysis. Front. Med. 2020, 7, 301. [Google Scholar] [CrossRef]
- Kavsak, P.A.; De Wit, K.; Worster, A. Emerging key laboratory tests for patients with COVID-19. Clin. Biochem. 2020, 81, 13–14. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Ng, J.J.; Choong, A.M. Thromboembolic events in patients with SARS-CoV-2. J. Vasc. Surg. 2020. [Google Scholar] [CrossRef]
- Salamanna, F.; Maglio, M.; Landini, M.P.; Fini, M. Platelet functions and activities as potential hematologic parameters related to Coronavirus disease 2019 (Covid-19). Platelets 2020, 2020, 1762852. [Google Scholar] [CrossRef]
- Vidali, S.; Morosetti, D.; Cossu, E.; Luisi, M.L.E.; Pancani, S.; Semeraro, V.; Consales, G. D-dimer as an indicator of prognosis in SARS-CoV-2 infection: A systematic review. ERJ Open Res. 2020, 6, 00260-2020. [Google Scholar] [CrossRef]
- Oudkerk, M.; Kuijpers, D.; Oudkerk, S.F.; Van Beek, E.J. The vascular nature of COVID-19. Br. J. Radiol. 2020, 20200718. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zeng, W.; Wen, Y.; Zheng, Y.; Lv, F.; Xiao, K. COVID-19 pneumonia: CT findings of 122 patients and differentiation from influenza pneumonia. Eur. Radiol. 2020, 1–7. [Google Scholar] [CrossRef]
- Zhang, B.; Zhang, J.; Chen, H.; Chen, L.; Chen, Q.; Li, M.; Chen, Z.; You, J.; Yang, K.; Zhang, S. Novel coronavirus disease 2019 (COVID-19): Relationship between chest CT scores and laboratory parameters. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Awulachew, E.; Diriba, K.; Anja, A.; Getu, E.; Belayneh, F. Computed Tomography (CT) Imaging features of patients with COVID-19: Systematic review and meta-analysis. Radiol. Res. Pr. 2020, 2020, 1023506. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xia, L. Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Guneyli, S.; Atceken, Z.; Dogan, H.; Altinmakas, E.; Atasoy, K.C. Radiological approach to COVID-19 pneumonia with an emphasis on chest CT. Diagn. Interv. Radiol. 2020, 26, 323–332. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT findings in Coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology 2020, 295. [Google Scholar] [CrossRef]
- Anonymous. Powassan virus: Centers for disease control and prevention. Prog. Cardiovasc. Dis. 2020, 19, 108. [Google Scholar]
- Li, J.-W.; Han, T.-W.; Woodward, M.; Anderson, C.S.; Zhou, H.; Chen, Y.; Neal, B. The impact of 2019 novel coronavirus on heart injury: A systematic review and meta-analysis. Prog. Cardiovasc. Dis. 2020. [Google Scholar] [CrossRef]
- Deng, P.; Ke, Z.; Ying, B.; Qiao, B.; Yuan, L. The diagnostic and prognostic role of myocardial injury biomarkers in hospitalized patients with COVID-19. Clin. Chim. Acta 2020, 510, 186–190. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, taaa020. [Google Scholar] [CrossRef] [PubMed]
- Bajwah, S.; Wilcock, A.; Towers, R.; Costantini, M.; Bausewein, C.; Simon, S.T.; Bendstrup, E.; Prentice, W.; Johnson, M.J.; Currow, D.C.; et al. Managing the supportive care needs of those affected by COVID-19. Eur. Respir. J. 2020, 55, 2000815. [Google Scholar] [CrossRef]
- Panigrahy, D.; Gilligan, M.M.; Huang, S.; Gartung, A.; Cortés-Puch, I.; Sime, P.J.; Phipps, R.P.; Serhan, C.N.; Hammock, B.D. Inflammation resolution: A dual-pronged approach to averting cytokine storms in COVID-19? Cancer Metastasis Rev. 2020, 39, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Chen, W. Promise and challenges in the development of COVID-19 vaccines. Hum. Vaccines Immunother. 2020, 1–5. [Google Scholar] [CrossRef]
- Goel, N.A.; Alam, A.A.; Eggert, E.M.; Acharya, S. Design and development of a customizable telemedicine platform for improving access to healthcare for underserved populations. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 2658–2661. [Google Scholar] [CrossRef]
- Ramirez, A.V.; Ojeaga, M.; Espinoza, V.; Hensler, B.; Honrubia, V. Telemedicine in minority and socioeconomically disadvantaged communities amidst COVID-19 pandemic. Otolaryngol. Neck Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Kushalnagar, P. Towards health equity: Deaf adults’ engagement in social e-health activities and e-communication with health care providers. J. Heal. Commun. 2018, 23, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Senjam, S.S. Impact of COVID-19 pandemic on people living with visual disability. Indian J. Ophthalmol. 2020, 68, 1367. [Google Scholar] [CrossRef]
- Chang, Y.-W.; Hsu, P.-Y.; Wang, Y.; Chang, P.-Y. Integration of online and offline health services: The role of doctor-patient online interaction. Patient Educ. Couns. 2019, 102, 1905–1910. [Google Scholar] [CrossRef]
- Rosen, C.B.; Joffe, S.; Kelz, R.R. COVID-19 moves medicine into a virtual space. Ann. Surg. 2020, 272, 159. [Google Scholar] [CrossRef]
- Gordon, H.S.; Solanki, P.; Bokhour, B.G.; Gopal, R.K. I’m not feeling like i’m part of the conversation patients’ perspectives on communicating in clinical video telehealth visits. J. Gen. Intern. Med. 2020, 35, 1751–1758. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually perfect? telemedicine for Covid-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med. Inform. Assoc. 2020, 27, 1132–1135. [Google Scholar] [CrossRef] [PubMed]
- Ratwani, R.M.; Brennan, D.; Sheahan, W.; Fong, A.; Adams, K.; Gordon, A.; Calabrese, M.; Hwang, E.; Smith, M.; Booker, E. A descriptive analysis of an on-demand telehealth approach for remote COVID-19 patient screening. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| If “Yes” to ANY ONE of the following highest priority questions, the patient is not permitted to enter the clinic. |
| (1) Have you had a temperature of 100 °F or greater in the past 7 days? |
| (2) Have you been diagnosed with Covid-19 in the past 14 days? |
| (3) Have you had contact with a known confirmed Covid-19 positive person in the last 14 days? |
| (4) Do you have a cough? |
| (5) Do you have shortness of breath or difficulty breathing? |
| If “Yes” to having ANY TWO of the following high priority symptoms in the past 14 days, then the patient is not permitted to enter the clinic. The patient/visitor will be provided with the information to schedule a virtual visit: |
| (1) Fever |
| (2) Cough |
| (3) Repeated shaking with chills |
| (4) Muscle pain |
| (5) Headache |
| (6) Sore throat |
| (7) New loss of taste or smell |
| Do you have any of the following pre-existing medical conditions? |
|---|
| Chronic lung disease |
| COPD |
| Asthma |
| Diabetes (type I or II) |
| History of heart disease, myocardial infarction, angioplasty, stent placement, coronary artery bypass graft |
| Valvular heart disease |
| Chronic kidney disease Chronic liver disease Immune system disorder or compromise Past surgeries |
| General. Look for: any apparent distress, toxic/nontoxic appearance |
| Head. Normocephalic. atraumatic |
| Eyes. Observe whether extraocular movements are intact; look for scleral icterus |
| Ears. Appearance of external ears |
| Throat. Facilitated: oropharyngeal viewing with flashlight |
| Neck. Observe for full range of motion and midline trachea |
| Respiratory. Is there distress or use of accessory respiratory muscles? |
| Abdomen. Facilitated: nondistended and nontender? |
| Neurologic. Check for alertness without focal deficits, observe gait |
| Psychologic. Mood and affect; assess for appropriate relation with provider via camera |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reiss, A.B.; De Leon, J.; Dapkins, I.P.; Shahin, G.; Peltier, M.R.; Goldberg, E.R. A Telemedicine Approach to Covid-19 Assessment and Triage. Medicina 2020, 56, 461. https://doi.org/10.3390/medicina56090461
Reiss AB, De Leon J, Dapkins IP, Shahin G, Peltier MR, Goldberg ER. A Telemedicine Approach to Covid-19 Assessment and Triage. Medicina. 2020; 56(9):461. https://doi.org/10.3390/medicina56090461
Chicago/Turabian StyleReiss, Allison B., Joshua De Leon, Isaac P. Dapkins, George Shahin, Morgan R. Peltier, and Eric R. Goldberg. 2020. "A Telemedicine Approach to Covid-19 Assessment and Triage" Medicina 56, no. 9: 461. https://doi.org/10.3390/medicina56090461
APA StyleReiss, A. B., De Leon, J., Dapkins, I. P., Shahin, G., Peltier, M. R., & Goldberg, E. R. (2020). A Telemedicine Approach to Covid-19 Assessment and Triage. Medicina, 56(9), 461. https://doi.org/10.3390/medicina56090461