Dermatological Manifestations in Pediatric Inflammatory Bowel Disease

 ,
,  ,
, 
Abstract
1. Introduction
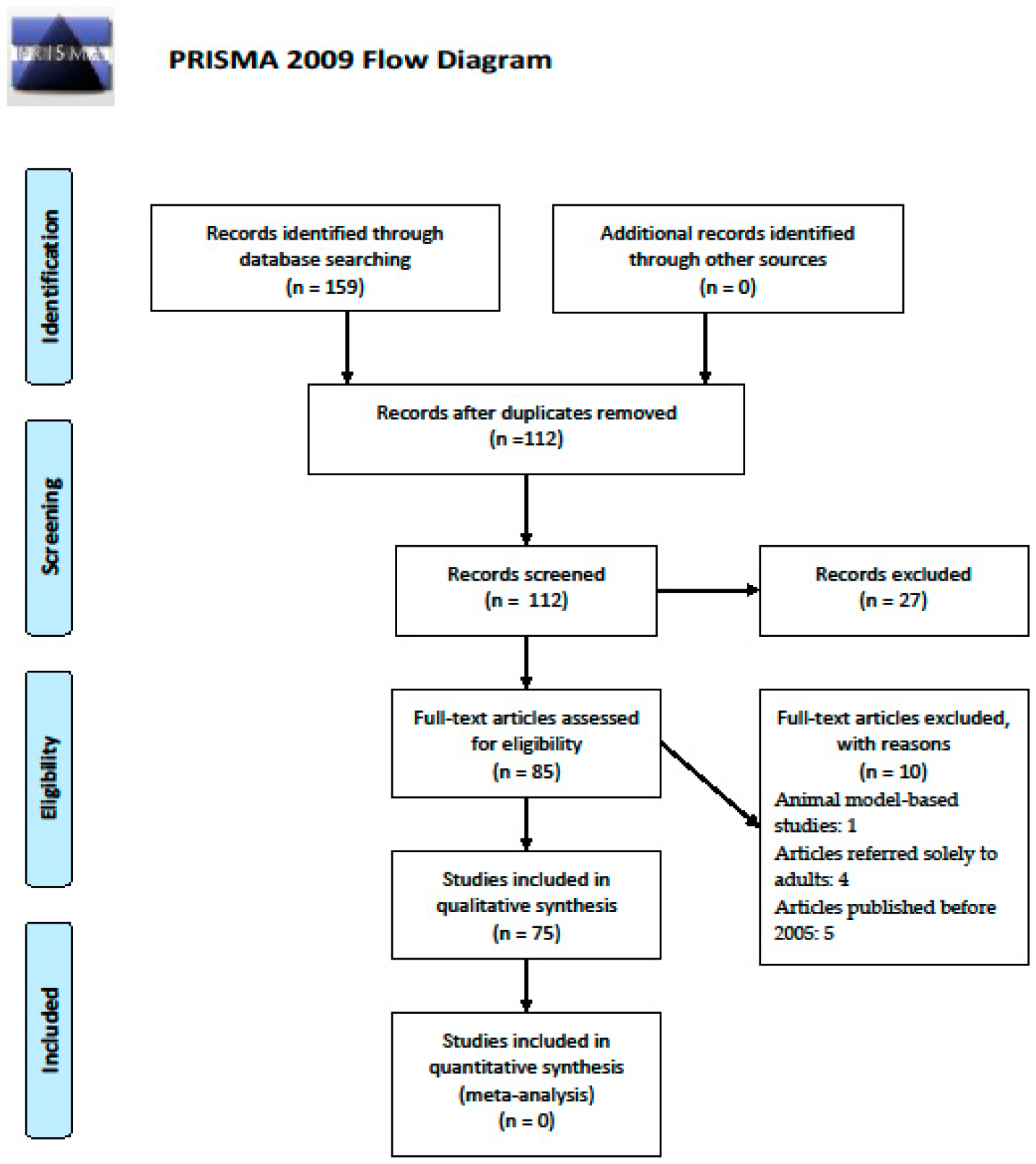
2. Material and Methods
3. Results
3.1. Specific Lesions
3.2. Reactivation Lesions
3.3. Manifestations Related to Malabsorption or Treatment
4. Discussions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; Martin de Carpi, J.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of Paediatric Ulcerative Colitis, Part 1: Ambulatory Care—An Evidence-based Guideline from European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatric Gastroenterol. Nutr. 2018, 67, 257–291. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN Revised Porto Criteria for the Diagnosis of Inflammatory Bowel Disease in Children and Adolescents. J. Pediatric Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef] [PubMed]
- Jose, F.A.; Garnett, E.A.; Vittinghoff, E.; Ferry, G.D.; Winter, H.S.; Baldassano, R.N.; Kirschner, B.S.; Cohen, S.A.; Gold, B.D.; Abramson, O.; et al. Development of Extraintestinal Manifestations in Pediatric Patients With Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2009, 15, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Kang, B.; Choe, B.H. The Difference in Extraintestinal Manifestations of Inflammatory Bowel Disease for Children and Adults. Transl. Pediatrics 2019, 8, 4–15. [Google Scholar] [CrossRef]
- Levine, J.S.; Burakoff, R. Extraintestinal Manifestations of Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2011, 7, 235–241. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta- Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Stawarski, A.; Iwańczak, B.; Krzesiek, E.; Iwańczak, F. Intestinal complications and extraintestinal manifestations in children with inflammatory bowel disease. Pol. Merkur. Lek. 2006, 20, 22–25. [Google Scholar]
- Rabeh, R.B.; Othman, A.B.; Bouyahya, O.; Mrad, S.M.; Boukthir, S. Extraintestinal manifestations of pediatric inflammatory bowel disease: A tunisian single-center experience. Arch. Dis. Child. 2019, 104, A1–A428. [Google Scholar]
- Mantegazza, C.; Angiero, F.; Zuccott, G.V. Oral manifestations of gastrointestinal diseases in children. Part 3: Ulcerative colitis and gastro-oesophageal reflux disease. Eur. J. Paediatr. Dent. 2016, 17, 248–250. [Google Scholar]
- Ribaldone, D.G.; Brigo, S.; Mangia, M.; Saracco, G.M.; Astegiano, M.; Pellicano, R. Oral Manifestations of Inflammatory Bowel Disease and the Role of Non-Invasive Surrogate Markers of Disease Activity. Medicines 2020, 7, 33. [Google Scholar] [CrossRef]
- Cohen, S.; Padlipsky, J.; Yerushalmy-Feler, A. Risk factors associated with extraintestinal manifestations in children with inflammatory bowel disease. Eur. J. Clin. Nutr. 2020, 74, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Lankarani, K.B.; Sivandzadeh, G.R.; Hassanpour, S. Oral manifestation in inflammatory bowel disease: A review. World J. Gastroenterol. 2013, 19, 8571–8579. [Google Scholar] [CrossRef] [PubMed]
- Trost, L.B.; McDonnell, J.K. Important cutaneous manifestations of inflammatory bowel disease. Postgrad. Med. J. 2005, 81, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Pazheri, F.; Alkhouri, N.; Radhakrishnan, K. Pyostomatitis Vegetans as an Oral Manifestation of Crohn’s Disease in a Pediatric Patient. Inflamm. Bowel Dis. 2010, 16, 2007. [Google Scholar] [CrossRef] [PubMed]
- Femiano, F.; Lanza, A.; Buonaiuto, C.; Perillo, L.; Dell’Ermo, A.; Cirillo, N. Pyostomatitis vegetans: A review of the literature. Med. Oral 2009, 14, E114–E117. [Google Scholar]
- Huang, B.L.; Chandra, S.; Shih, D.Q. Skin manifestations of inflammatory bowel disease. Front. Physiol. 2012, 3, 13. [Google Scholar] [CrossRef]
- Blasco-Alonso, J.; Girón-Fernández-Crehuet, F.; Lendinez-Ramírez, M.Á.; Gallego-Gutiérrez, S.; Pérez, S.L.; Serrano-Nieto, J.; Navas-López, V.M.; Sierra-Salinas, C. Metastatic Crohn’s Disease in Pediatrics. Rev. Esp. Enferm. Dig. 2016, 108, 598–603. [Google Scholar] [CrossRef]
- Bender-Heine, A.; Grantham, J.T.; Zaslau, S.; Jansen, R. Metastatic Crohn Disease: A Review of Dermatologic Manifestations and Treatment. Cutis 2017, 99, E33–E40. [Google Scholar]
- Lee, Y.A.; Chun, P.; Hwang, E.H.; Mun, S.W.; Lee, Y.J.; Park, J.H. Clinical Features and Extraintestinal Manifestations of Crohn Disease in Children. Pediatric Gastroenterol. Hepatol. Nutr. 2016, 19, 236–242. [Google Scholar] [CrossRef]
- Korelitz, B.I. Anal skin tags: An overlooked indicator of Crohn’s disease. J. Clin. Gastroenterol. 2010, 44, 151–152. [Google Scholar] [CrossRef]
- Keljo, D.J.; Markowitz, J.; Langton, C.; Lerer, T.; Bousvaros, A.; Carvalho, R.; Crandall, W.; Jonathan, E.; Griffiths, A.; Kay, M.; et al. Course and treatment of perianal disease in children newly diagnosed with Crohn’s disease. Inflamm. Bowel Dis. 2009, 15, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Kierkuś, J.; Szymańska, E.; Szymańska, S.; Ruszkowska, L. A case of pediatric patient with ulcerative colitis and extraintestinal skin manifestation-pyoderma gangrenosum. Postępy Nauk Med. 2014, 27, 178–180. [Google Scholar]
- Schoch, J.J.; Tolkachjov, S.N.; Cappel, J.A. Pediatric pyoderma gangrenosum: A retrospective review of clinical features, etiologic associations, and treatment. Pediatric Dermatol. 2017, 34, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Manda, G.; Finch, P.; Mponda, K. Pyoderma gangrenosum associated with Crohn’s disease in a Malawian teenage boy: Case report and review of literature. Trop. Dr. 2018, 48, 43–46. [Google Scholar] [CrossRef]
- Weinstein, M.; Turner, D.; Avitzur, Y. Erythema nodosum as a presentation of inflammatory bowel disease. Can. Med. Assoc. J. 2005, 173, 145–146. [Google Scholar] [CrossRef]
- Dotson, J.L.; Hyams, J.S.; Markowitz, J.; LeLeiko, N.S.; Mack, D.R.; Evans, J.S.; Pfefferkorn, M.D.; Griffiths, A.M.; Otley, A.R.; Bousvaros, A.; et al. Extraintestinal manifestations of pediatric inflammatory bowel disease and their relation to disease type and severity. J. Pediatric Gastroenterol. Nutr. 2010, 51, 140–145. [Google Scholar] [CrossRef]
- Schwartz, R.A.; Nervi, S.J. Erythema Nodosum: A Sign of Systemic Disease. Am. Fam. Physician 2007, 75, 695–700. [Google Scholar]
- Reddy, H.; Shipman, A.R.; Wojnarowska, F. Epidermolysis bullosa acquisita and inflammatory bowel disease: A review of the literature. Clin. Exp. Dermatol. 2013, 38, 225–230. [Google Scholar] [CrossRef]
- Russo, I.; Ferrazzi, A.; Zanetti, I.; Alaibac, M. Epidermolysis bullosa acquisita in a 17-year-old boy with Crohn’s disease. BMJ Case Rep. 2015. [Google Scholar] [CrossRef]
- Simonetti, O.; Postacchini, V.; Offidani, A. Cutaneous vasculitis and inflammatory bowel diseases. G. Ital. Dermatol. Venereol. 2015, 150, 233–236. [Google Scholar]
- Butts, G.T.; Bishop, P.R.; Wyatt, J.P.; Nowicki, M.J. Leukocytoclastic vasculitis in an adolescent with ulcerative colitis: Report of a case and review of the literature. SAGE Open Med. Case Rep. 2014. [Google Scholar] [CrossRef]
- Sridhar, S.; Maltz, R.M.; Boyle, B.; Kim, S.C. Dermatological Manifestations in Pediatric Patients with Inflammatory Bowel Diseases on Anti-TNF Therapy. Inflamm. Bowel Dis. 2018, 24, 2086–2092. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Jang, K.T.; Choe, Y.H.; Malik, P.S.; Broor, S.; Bakhshi, S.; Aroor, S. Azathioprine hypersensitivity presenting as sweet syndrome in a child with ulcerative colitis. Indian Pediatrics 2011, 48, 969–971. [Google Scholar] [CrossRef] [PubMed]
- Cossio, M.L.; Genois, A.; Jantchou, P.; Hatami, A.; Deslandres, C.; McCuaig, C. Skin Manifestations in Pediatric Patients Treated With a TNF-Alpha Inhibitor for Inflammatory Bowel Disease: A Retrospective Study. J. Cutan. Med. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Courbette, O.; Aupiais, C.; Viala, J.; Hugot, J.P.; Louveau, B.; Chatenoud, L.; Emmanuelle, B.; Martinez-Vinson, C. Infliximab paradoxical psoriasis in a cohort of children with inflammatory bowel disease. J. Pediatric Gastroenterol. Nutr. 2019, 69, 189–193. [Google Scholar] [CrossRef]
- Peneau, A.; Savoye, G.; Turck, D.; Dauchet, L.; Fumery, M.; Salleron, J.; Lerebours, E.; Ligier, K.; Vasseur, F.; Dupas, J.L.; et al. Mortality and cancer in pediatric-onset inflammatory bowel disease: A population-based study. Am. J. Gastroenterol. 2013, 108, 1647–1653. [Google Scholar] [CrossRef]
- Deneau, M.; Wallentine, J.; Guthery, S.; O’Gorman, M.; Bohnsack, J.; Fluchel, M.; Bezzant, J.; Pohl, J.F. Natural killer cell lymphoma in a pediatric patient with inflammatory bowel disease. Pediatrics 2010, 126, e977–e981. [Google Scholar] [CrossRef]
- Rosenbaum, J.; Alex, G.; Roberts, H.; Orchard, D. Drug Rash with Eosinophilia and Systemic Symptoms Secondary to Sulfasalazine. J. Paediatr. Child Health 2010, 46, 193–196. [Google Scholar] [CrossRef]
- Ho, T.; Orenstein, L.A.; Boos, M.D.; White, K.P.; Fett, N.M. Cutaneous Small-Vessel Vasculitis in Two Children with Inflammatory Bowel Disease: Case Series and Review of the Literature. Pediatric Dermatol. 2017, 34, e235–e240. [Google Scholar] [CrossRef]
- Toussi, S.S.; Pan, N.; Walters, H.M.; Walsh, T.J. Infections in children and adolescents with juvenile idiopathic arthritis and inflammatory bowel disease treated with tumor necrosis factor–α inhibitors: Systematic review of the literature. Clin. Infect. Dis. 2013, 57, 1318–1330. [Google Scholar] [CrossRef]
- Sherlock, M.E.; Walters, T.; Tabbers, M.M.; Frost, K.; Zachos, M.; Muise, A.; Pope, A.; Griffiths, A.M. Infliximab-induced psoriasis and psoriasiform skin lesions in pediatric Crohn disease and a potential association with IL-23 receptor polymorphisms. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Nuti, F.; Viola, F.; Civitelli, F.; Alessandri, C.; Aloi, M.; Dilillo, A.; Del Giudice, E.; Cucchiara, S. Biological therapy in a pediatric crohn disease population at a referral center. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Savasan, S.; El-Baba, M. First episode of axillary acne inversa in a teenager on infliximab therapy for Crohn disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, e2–e3. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, L.K. Safety of TNF inhibitors in adolescents and children. Adolesc. Health Med. Ther. 2011, 2, 1–8. [Google Scholar] [CrossRef]
- Bradley, G.M.; Oliva-Hemker, M. Pediatric ulcerative colitis: Current treatment approaches including role of infliximab. Biol. Targets Ther. 2012, 6, 125. [Google Scholar] [CrossRef][Green Version]
- Krawiec, P.; Pac-Kożuchowska, E. Biomarkers and Hematological Indices in the Diagnosis of Iron Deficiency in Children with Inflammatory Bowel Disease. Nutrients 2020, 12, 1358. [Google Scholar] [CrossRef]
- Funato, M.; Fukao, T.; Sasai, H.; Hori, T.; Terazawa, D.; Kubota, K.; Ozeki, M.; Orii, K.; Kaneko, H.; Kondo, N. Successful treatment of pediatric immune thrombocytopenic purpura associated with ulcerative colitis. Pediatric Int. 2011, 53, 771–773. [Google Scholar] [CrossRef]
- Aloi, M.; Cucchiara, S. Extradigestive manifestations of IBD in pediatrics. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 23–32. [Google Scholar]
- Keyal, U.; Liu, Y.; Bhatta, A.K. Dermatologic manifestations of inflammatory bowel disease: A review. Discov. Med. 2018, 25, 225–233. [Google Scholar]
- Zippi, M.; Pica, R.; De Nitto, D.; Paoluzi, P. Biological therapy for dermatological manifestations of inflammatory bowel disease. World J. Clin. Cases: WJCC 2013, 1, 74. [Google Scholar] [CrossRef]
- Evans, P.E.; Pardi, D.S. Extraintestinal manifestations of inflammatory bowel disease: Focus on the musculoskeletal, dermatologic, and ocular manifestations. Medscape Gen. Med. 2007, 9, 55. [Google Scholar]
- Shan, J.; Zhang, J. Impact of obesity on the efficacy of different biologic agents in inflammatory diseases: A systematic review and meta-analysis. Joint Bone Spine 2019, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Al-Mendalawi, M. Extraintestinal manifestations of pediatric inflammatory bowel disease in Saudi Arabia. Saudi J. Gastroenterol. 2018, 24, 307. [Google Scholar] [CrossRef] [PubMed]
- Navallo, L.; Gold, S.; Chernoff, K.; Sockolow, R.; Barfield, E. Tumor Necrosis Factor (TNF) Inhibitor Induced Psoriasis in Pediatric Patients with Inflammatory Bowel Disease: A Case Series. Inflamm. Bowel Dis. 2017, 23. [Google Scholar] [CrossRef]
- Bukhari, I.; Alzoubi, N.; Al-Quorain, A.A. Infliximab-induced psoriasis in a patient with Crohn’s disease. Saudi J. Med. Med. Sci. 2015, 3, 81. [Google Scholar]
- Greuter, T.; Bertoldo, F.; Rechner, R.; Straumann, A.; Biedermann, L.; Zeitz, J.; Ali, R.A. Extraintestinal manifestations of pediatric inflammatory bowel disease: Prevalence, presentation, and anti-TNF treatment. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 200–206. [Google Scholar] [CrossRef]
- Guariso, G.; Gasparetto, M.; Dalla Pozza, L.V.; D’Incà, R.; Zancan, L.; Sturniolo, G.; Facchin, P. Inflammatory bowel disease developing in paediatric and adult age. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 698–707. [Google Scholar] [CrossRef]
- Andrisani, G.; Guidi, L.; Papa, A.; Armuzzi, A. Anti-TNF alpha therapy in the management of extraintestinal manifestation of inflammatory bowel disease. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 890–901. [Google Scholar]
- Woo, V.L. Oral manifestations of Crohn’s disease: A case report and review of the literature. Case Rep. Dent. 2015, 2015, 830472. [Google Scholar] [CrossRef]
- Rizvi, S.A.; Elder, M.; Beasley, G. A novel manifestation of prolidase deficiency in a toddler diagnosed with very-early-onset crohn disease. J. Pediatr. Gastroenterol. Nutr. 2019, 69, e89. [Google Scholar] [CrossRef]
- Molnár, T.; Farkas, K.; Nagy, F.; Vass, N.; Szepes, Z.; Tiszlavicz, L.; Wittmann, T. Third case: Another pediatric patient with pyostomatitis vegetans and oral granuloma as one of the initial symptoms of Crohn’s disease. Inflamm. Bowel Dis. 2011, 17, E122–E123. [Google Scholar]
- Yang, B.; Wang, C.; Wang, N.; Pan, F.; Chen, S.; Zhou, G.; Yu, M.; Zhang, F. Childhood epidermolysis bullosa acquisita: Report of a Chinese case. Pediatric Dermatol. 2012, 29, 614–617. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Deroide, F.; Rustin, M. Pyoderma gangrenosum—A guide to diagnosis and management. Clin. Med. 2019, 19, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Turska, M.; Parada-Turska, J. Cutaneous Polyarteritis Nodosa. Wiad. Lek. 2018, 71, 73–77. [Google Scholar] [PubMed]
- Baumgart, D.C.; Sandborn, W.J. Inflammatory bowel disease: Clinical aspects and established and evolving therapies. Lancet 2007, 369, 1641–1647. [Google Scholar] [CrossRef]
- Torres, J.; Buche, S.; Delaporte, E.; Colombel, J.F. Skin side effects of inflammatory bowel disease therapy. Inflamm. Bowel Dis. 2013, 19, 1086–1098. [Google Scholar] [CrossRef]
- Andrade, P.; Lopes, S.; Gaspar, R.; Nunes, A.; Magina, S.; Macedo, G. Anti-Tumor Necrosis Factor –α-Induced Dermatological Complications in a Large Cohort of Inflammatory Bowel Disease Patients. Dig. Dis. Sci. 2018, 63, 746–754. [Google Scholar] [CrossRef]
- Farhat, F.; Chandler, M.; Borum, M. Need for Counseling on Dermatologic Side Effects for IBD Patients on Immunologic Based Therapies. Inflamm. Bowel Dis. 2017, 23, S51. [Google Scholar] [CrossRef]
- Viola, F.; Civitelli, F.; Nuti, F.; Dilillo, A.; Alessandri, C.; Cavallari, N.; Aloi, M.; Cucchiara, P. Cutaneous events in pediatric patients receiving Adalimumab for Crohn’s disease: A case series. Dig. Liver Dis. 2012, 44, S115. [Google Scholar] [CrossRef]
- Ehrlich, S.; Mark, A.G.; Rinawi, F.; Shamir, R.; Assa, A. Micronutrient Deficiencies in Children with Inflammatory Bowel Diseases. Nutr. Clin. Pract. 2020, 35, 315–322. [Google Scholar] [CrossRef]
- Phanachet, P.; Shantavasinkul, P.C.; Chantrathammachart, P.; Rattanakaemakorn, P.; Jayanama, K.; Komindr, S.; Warodomwichit, D. Unusual manifestation of vitamin A deficiency presenting with generalized xerosis without night blindness. Clin. Case Rep. 2018, 6, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha Lima, B.; Pichi, F.; Lowder, C.Y. Night blindness and Crohn’s disease. Int. Ophthalmol. 2014, 34, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Weissman, S.; Aziz, M.; Saleem, S.; Hassan, A.; Sciarra, M. Acrodermatitis Enteropathica Associated With Inflammatory Bowel Disease. ACG Case Rep. J. 2019, 6, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.; Heng, L.; Shaodong, W.; Fangyu, W.; Zhenkai, W. Pellagra affecting a patient with Crohn’s disease. An. Bras. Dermatol. 2017, 92, 879–881. [Google Scholar] [CrossRef]
- Thornton, A.M.; Drummond, C.J. An unexpected case of pellagra. Med. J. Aust. 2014, 200, 546–548. [Google Scholar] [CrossRef]
- Trikudanathan, G.; Venkatesh, P.G.; Navaneethan, U. Diagnosis and Therapeutic Management of Extra-Intestinal Manifestations of Inflammatory Bowel Disease. Drugs 2012, 72, 2333–2349. [Google Scholar] [CrossRef]
- Passarini, B.; Infusino, S.D.; Barbieri, E.; Varotti, E.; Gionchetti, P.; Rizzello, F.; Morselli, C.; Tambasco, R.; Campieri, M. Cutaneous manifestations in inflammatory bowel diseases: Eight cases of psoriasis induced by anti-tumor-necrosis-factor antibody therapy. Dermatology 2007, 215, 295–300. [Google Scholar] [CrossRef]
- O’Brien, C.L.; Kiely, C.J.; Pavli, P. The microbiome of Crohn’s disease aphthous ulcers. Gut Pathog. 2018, 10, 44. [Google Scholar] [CrossRef]
- Danese, S.; Semeraro, S.; Papa, A.; Roberto, I.; Scaldaferri, F.; Fedeli, G.; Giovanni, G.; Gasbarrini, A. Extraintestinal manifestations in inflammatory bowel disease. World J. Gastroenterol. 2005, 11, 7227. [Google Scholar] [CrossRef]
- Bakelants, E.; van der Hilst, J.; Corluy, L.; Achten, R.; Gyssens, I.; Messiaen, P. The diagnostic tangle of pyoderma gangrenosum: A case report and review of the literature. Neth. J. Med. 2014, 72, 541–544. [Google Scholar]
- Brenner, E.J.; Long, M.D. Diagnosis and treatment of dermatologic diseases in inflammatory bowel disease. Curr. Opin. Gastroenterol. 2019, 35, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Keethy, D.; Mrakotsky, C.; Szigethy, E. IBD and Depression: Treatment Implications. Curr. Opin. Pediatrics 2014, 26, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Greenley, R.N.; Hommel, K.A.; Nebel, J.; Raboin, T.; Li, S.H.; Simpson, P.; Mackner, L. A meta-analytic review of the psychosocial adjustment of youth with inflammatory bowel disease. J. Pediatric Psychol. 2010, 35, 857–869. [Google Scholar] [CrossRef] [PubMed]
- Szigethy, E.; Bujoreanu, S.I.; Youk, A.O.; Weisz, J.; Benhayon, D.; Fairclough, D.; Ducharme, P.; Gonzalez-Heydrich, J.; Keljo, D.; Srinath, A.; et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.P.; Clark, A.L.; Garnett, E.A.; Acree, M.; Cohen, S.A.; Ferry, G.D.; Heyman, M.B. Use of complementary medicine in pediatric patients with inflammatory bowel disease: Results from a multicenter survey. J. Pediatric Gastroenterol. Nutr. 2009, 48, 55. [Google Scholar] [CrossRef] [PubMed]
- Can, B.; Akan, H.; Topaloglu Demir, F.; Zindanci, I.; Cebeci, F.; Turkoglu, Z.; Kavala, M. Complementary and alternative therapies used by patients of pediatric dermatology outpatient clinics in Turkey: A multicenter study. Pediatric Dermatol. 2017, 34, 72–77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Specific lesions | Fissures and fistulas, aphthous stomatitis, pyostomatitis vegetans, metastatic Crohn’s disease, epidermolysis bullosa acquisita |
| Reactivation lesions | Erythema nodosum, pyoderma gangrenosum, aphthous stomatitis, necrotizing vasculitis, cutaneous polyarteritis nodosa, Sweet’s syndrome |
| Manifestations related to malabsorption or treatment | Acrodermatitis enteropathica, scurvy, purpura, pellagra, stomatitis-glossitis-angular cheilitis, paradoxical psoriasis, abnormal hair and nails |
| Miscellaneous lesions | Vitiligo, psoriasis, secondary amyloidosis, bowel associated dermatosis-arthritis syndrome |
| Author, Year of Publication | Country | Study Design | Number of Patients | Reported Dermatological Manifestations of Pediatric IBD | ||
|---|---|---|---|---|---|---|
| Specific Lesions | Reactivation Lesions | Lesions Related to Malabsorption/Medication | ||||
| Jose et al., 2009 [3] | USA | Retrospective | 1649 | Aphthous stomatitis (n = 53) | EN (n = 21); PG (n = 6) | Psoriasis (n = 2) |
| Jang et al., 2019 [4] | South Korea | Review | - | MCD, epidermolysis bullosa, erythema elevatum iutinum | EN, PG, Sweet’s Syndrome, polyarteritis nodosa | Psoriasis, alopecia |
| Levine et al., 2011 [5] | USA | Review | - | Oral aphthous stomatitis, genital ulcers, MCD, | EN, PG, Sweet’s syndrome | Psoriasis, eczematous lesions |
| Stawarski et al., 2006 [7] | Poland | Retrospective | 184 | Perianal changes, external intestinal fistulae | ||
| Mantegazza et al., 2016 [9] | Italy | Review | - | Pyostomatitis vegetans, oral aphthae | Glossitis, non-specific gingivitis, stomatitis, cheilitis, mucosal ulcers, lichen planus, diffuse pustules | |
| Ribaldone et al., 2020 [10] | UK, Italy | Review | - | Deep ulcerations, lip swelling, fissures, cobblestoning, aphthous stomatitis, pyostomatitis vegetans, | Angular cheilitis, mucogingivitis | |
| Cohen et al., 2020 [11] | Israel | Retrospective | 100 | Aphthous stomatitis | ||
| Lankarani et al., 2013 [12] | Iran | Review | - | Cobblestoning, lip swelling, fissures, aphthous stomatitis, perioral erythema with scaling, pyostomatitis vegetans, | Mucogingivitis, angular cheilitis | |
| Trost et al., 2005 [13] | USA | Review | - | Aphthous stomatitis, cobblestoning, pyostomatitis vegetans | PG, EN | |
| Pazheri et al., 2010 [14] | USA | Case Report | 1 | Pyostomatitis vegetans | ||
| Femiano et al., 2009 [15] | Italy | Review | - | Pyostomatitis vegetans | ||
| Huang et al., 2012 [16] | USA | Review | - | Perianal lesions, cobblestoning of the buccal mucosa, aphthous stomatitis, ulcers, pyodermatita vegetans, pyostomatita vegetans, acquired epidermolysis bullosa | EN, PG, neutrophilic dermatoses, leukocytoclastic vasculitis | Acrodermatitis enteropathica, pellagra, scurvy, purpura, xeroderma, unspecified eczema, hair loss, lichen planus, erythema multiforme, bullous dermatosis, Stevens–Johnson syndrome, acne, psoriasis |
| Blasco-Alonso et al., 2016 [17] | Spain | Case report | 4 | MCD | ||
| Bender-Heine et al., 2017 [18] | USA | Review | - | MCD | ||
| Lee et al., 2016 [19] | South Korea | Retrospective | 73 | Perianal abscesses and/or fistulas (n = 37), vulvitis (n = 1), anal skin tags (n = 25) | EN (n = 2) | |
| Korelitz et al., 2010 [20] | USA | Review | - | Anal skin tags | ||
| Keljo et al., 2009 [21] | USA | Retrospective | 276 | Perianal lesions (n = 41), skin tags and fissures (n = 13), fistulas and/or abscesses (n = 28) | ||
| Kierkuś et al., 2014 [22] | Poland | Case Report | 1 | PG | ||
| Schoch et al., 2017 [23] | USA | Retrospective | 13 | PG | ||
| Manda et al., 2017 [24] | Malawi | Case report | 1 | PG | ||
| Weinstein et al., 2005 [25] | USA | Case report | 1 | EN | ||
| Dotson et al., 2010 [26] | USA | Prospective | 1009 | Aphthous stomatitis, perianal disease | EN | |
| Schwartz et al., 2007 [27] | USA | Review | - | EN | ||
| Reddy et al., 2013 [28] | UK | Review | 1969 | Epidermolysis bullosa acquisita | ||
| Russo et al., 2015 [29] | Italy | Case report | 1 | Epidermolysis bullosa acquisita | ||
| Simonetti et al., 2015 [30] | Italy | Review | - | cutaneous vasculitis | ||
| Butts et al., 2014 [31] | USA | Case report and literature review | 1 | Dermatitis herpetiformis, epidermolysis bullosa acquisita | EN, PG, Sweet’s syndrome, necrotizing vasculitis, leukocytoclastic vasculitis | Psoriasis |
| Sridhar et al., 2018 [32] | USA | Retrospective | 409 | Infections (n = 28), psoriasis (n = 33), eczema (n = 10 | ||
| Kim et al., 2011 [33] | South Korea | Case report | 1 | Sweet’s syndrome 10 days after treatment with azathioprine | ||
| Cossio et al., 2020 [34] | Canada | Retrospective | 343 | Psoriasiform eruptions (n = 20); skin infections (n = 10); eczematous eruptions (n = 5); type IV hypersensitivity reactions (n = 3), lupus-like photosensitivity (n = 1), urticaria (n = 1), alopecia areata (n = 1), hidradenitis suppurativa (n = 1), pyoderma gangrenosum (n = 1), granuloma annulare (n = 1), acrocyanosis (n = 1) | ||
| Courbette et al., 2019 [35] | France | Retrospective | 147 | Infliximab-induced psoriasis (n = 20) | ||
| Peneau et al., 2013 [36] | France | Retrospective | 698 | Basal cell carcinoma (n = 2) | ||
| Deneau et al., 2010 [37] | USA | Case report | 1 | Aphthous stomatitis | Hemophagocytic lymphohistiocytosis, Epstein-Barr virus-positive natural killer T-cell lymphoma | |
| Rosenbaum et al., 2010 [38] | Australia | Case report | 1 | Drug rash and eosinophilia with systemic symptoms (DRESS) secondary to sulfasalazine | ||
| Ho et al., 2017 [39] | USA | Case report and literature review | 2 | Cutaneous small-vessel vasculitis | ||
| Toussi et al., 2013 [40] | USA | Systematic literature review | - | Abscess/cellulitis (n = 8) secondary to anti TNF agents | ||
| Sherlock et al., 2013 [41] | Canada | Retrospective | 172 | Psoriasis or psoriasiform skin lesions secondary to Infliximab | ||
| Nuti et al., 2014 [42] | Italy | Retrospective observational | 78 | Infusion reactions, psoriasis (n = 9), minor infections (herpes simplex infections, oral candidiasis, folliculitis)—secondary to biological therapy | ||
| Savasan et al, 2013 [43] | USA | Case report | 1 | Hidradenitis suppurativa secondary to Infliximab | ||
| McCluggage, 2011 [44] | USA | Review | - | Infusion or injection-site reactions secondary to anti-TNF agents | ||
| Bradley et al., 2012 [45] | USA | Review | - | Rashes (Thiopurine immunomodulators), hirsutism (Calcineurin inhibitors) | ||
| Krawiec et al., 2020 [46] | Poland | Observational | - | Alopecia, stomatitis, glossitis secondary to iron deficiency | ||
| Funato et al., 2011 [47] | Japan | Case Report | 1 | Multiple purpuric lesions | ||
| Aloi, 2009 [48] | Italy | Review | - | Perianal skin tags, oral aphthous ulcers, MCD | EN, PG | |
| Keyal et al., 2018 [49] | China | Review | - | Perianal and oral lesions, MCD | EN, PG, Sweet’s syndrome, Bowel-associated dermatosis-arthritis syndrome, Pyodermatitis-pyostomatitis vegetans, SAPHO syndrome (acne conglobata or fulminans, pustulosis, hidradenitis suppurativa, dissecting cellulitis of the scalp) | Phrynoderma, stomatitis-glossitis-angular cheilitis, scurvy, seborrheic-type dermatitis, bruising, petechiae, dry skin, eczema, slow wound healing, hair hypopigmentation, glossitis, nail abnormalities, acrodermatitis enteropathica, eczematous and psoriasiform skin eruptions, skin and soft tissue infections |
| Zippi et al., 2013 [50] | Italy | Review | - | EN, PG | Paradoxical psoriasis | |
| Evans et al., 2007 [51] | USA | Review | - | Aphthous stomatitis | EN, PG | |
| Shan et al., 2019 [52] | China | Retrospective | 161 | Aphthous ulcer (n = 39), skip lesions (n = 19), perianal disease | ||
| Al-Mendalawi et al, 2018 [53] | Saudi Arabia | Retrospective | 66 | EN, PG | ||
| Navallo et al, 2017 [54] | USA | Case series | 5 | paradoxical psoriasis secondary to Infliximab (n = 3) and Adalimumab (n = 1), eczema, pityriasis rosea | ||
| Bukhari et al., 2015 [55] | Saudi Arabia | Case report | 1 | Infliximab-induced psoriasis | ||
| Greuter et al., 2017 [56] | Switzerland | Retrospective | 329 | Aphthous stomatitis | EN, PG | Psoriasis |
| Guariso et al., 2010 [57] | Italy | Retrospective | 133 | Perianal disease (n = 17), oral aphthous lesions (n = 4) | EN (n = 4) | |
| Andrisani et al., 2012 [58] | Italy | Review | - | EN, PG | ||
| Woo et al., 2015 [59] | Case report | 1 | Mucosal erythema, mucosal-colored swellings, and ulcerations of the gingiva, nodular swelling of the interdental papillae, tissue tags, polyps, aphthous ulcerations, perioral dermatitis | Angular cheilitis, stomatitis, glossitis | ||
| Rizvi et al, 2019 [60] | USA | Case report | 1 | Cutaneous ulcerations secondary to prolidase deficiency in a toddler with very-early-onset CD | ||
| Ben Rabeh et al, 2019 [8] | Tunisia | Retrospective | 14 | Ulcerative skin eruption | EN | vitiligo |
| Molnar et al, 2011 [61] | Hungary | Case report | 1 | Skin tags, swelling of the lips, oral mucosa, pyostomatitis vegetans | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaconescu, S.; Strat, S.; Balan, G.G.; Anton, C.; Stefanescu, G.; Ioniuc, I.; Stanescu, A.M.A. Dermatological Manifestations in Pediatric Inflammatory Bowel Disease. Medicina 2020, 56, 425. https://doi.org/10.3390/medicina56090425
Diaconescu S, Strat S, Balan GG, Anton C, Stefanescu G, Ioniuc I, Stanescu AMA. Dermatological Manifestations in Pediatric Inflammatory Bowel Disease. Medicina. 2020; 56(9):425. https://doi.org/10.3390/medicina56090425
Chicago/Turabian StyleDiaconescu, Smaranda, Silvia Strat, Gheorghe G. Balan, Carmen Anton, Gabriela Stefanescu, Ileana Ioniuc, and Ana Maria Alexandra Stanescu. 2020. "Dermatological Manifestations in Pediatric Inflammatory Bowel Disease" Medicina 56, no. 9: 425. https://doi.org/10.3390/medicina56090425
APA StyleDiaconescu, S., Strat, S., Balan, G. G., Anton, C., Stefanescu, G., Ioniuc, I., & Stanescu, A. M. A. (2020). Dermatological Manifestations in Pediatric Inflammatory Bowel Disease. Medicina, 56(9), 425. https://doi.org/10.3390/medicina56090425