Assessment of Selected Anthropometric Parameters Influence on Balance Parameters in Children

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Błaszczyk, J. Kontrola stabilności postawy ciała. KOSMOS 1993, 42, 473–486. [Google Scholar]
- Held-Ziółkowska, M. Organizacja zmysłowa i biomechanika układu równowagi. Magazyn Otolaryngol. 2006, 5, 39–46. [Google Scholar]
- Atwater, S.W.; Crowe, T.K.; Deitz, J.C.; Richardson, P.K. Interrater and Test-Retest Reliability of Two Pediatric Balance Tests. Phys. Ther. 1990, 70, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Miko, I.; Szerb, I.; Szerb, A.; Bender, T.; Poór, G. Effect of a balance-training programme on postural balance, aerobic capacity and frequency of falls in women with osteoporosis: A randomized controlled trial. J. Rehabil. Med. 2018, 50, 542–547. [Google Scholar] [CrossRef]
- Ng, S.S.M.; Guo, X.; Liu, K.; Ki, W.; Louie, L.H.T.; Chung, R.C.; Macfarlane, D.J. Task-Specific Balance Training Improves the Sensory Organisation of Balance Control in Children with Developmental Coordination Disorder: A Randomised Controlled Trial. Sci. Rep. 2016, 6, 20945. [Google Scholar] [CrossRef]
- Condon, C.; Cremin, K. Static Balance Norms in Children. Physiother. Res. Int. 2013, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Paszko-Patej, G.; Terlikowski, R.; Kułak, W.; Sienkiewicz, D.; Okurowska-Zawada, B. Czynniki wpływające na proces kształtowania równowagi dziecka oraz możliwości jej obiektywnej oceny. Neurol. Dziecięca 2011, 20, 121–127. [Google Scholar]
- Lin, S.-I.; Woollacott, M.H. Postural Muscle Responses Following Changing Balance Threats in Young, Stable Older, and Unstable Older Adults. J. Mot. Behav. 2002, 34, 37–44. [Google Scholar] [CrossRef]
- Powers, C.M. The Influence of Altered Lower-Extremity Kinematics on Patellofemoral Joint Dysfunction: A Theoretical Perspective. J. Orthop. Sports Phys. Ther. 2003, 33, 639–646. [Google Scholar] [CrossRef]
- Kostiukow, A.; Rostkowska, E.; Samborski, W. Badanie zdolności zachowania równowagi ciała. Ann. Acad. Med. Stetin. 2009, 55, 102–109. [Google Scholar] [PubMed]
- Verbecque, E.; Vereeck, L.; Hallemans, A. Postural sway in children: A literature review. Gait Posture 2016, 49, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Dose-Response Relationships of Balance Training in Healthy Young Adults: A Systematic Review and Meta-Analysis. Sports Med. 2014, 45, 557–576. [Google Scholar] [CrossRef] [PubMed]
- Mraz, M.; Nowacka, U.; Skrzek, A.; Mraz, M.; Dębiec-Bąk, A.; Sidorowska, M. Postural stability of women at the age of 8–22 on the basis of posturographic examinations. Physiotherapy 2010, 18, 35–43. [Google Scholar] [CrossRef]
- Wolański, N. Rozwój Biologiczny Człowieka, 7th ed.; Wydawnictwo PWN: Warszawa, Poland, 2006. [Google Scholar]
- Roncesvalles, M.N.; Schmitz, C.; Zedka, M.; Assaiante, C.; Woollacott, M. From Egocentric to Exocentric Spatial Orientation: Development of Posture Control in Bimanual and Trunk Inclination Tasks. J. Mot. Behav. 2005, 37, 404–416. [Google Scholar] [CrossRef]
- Riach, C.; Starkes, J. Stability limits of quiet standing postural control in children and adults. Gait Posture 1993, 1, 105–111. [Google Scholar] [CrossRef]
- Berger, W.; Quintern, J.; Dietz, V. Stance and gait perturbations in children: Developmental aspects of compensatory mechanisms. Electroencephalogr. Clin. Neurophysiol. 1985, 61, 385–395. [Google Scholar] [CrossRef]
- Assaiante, C.; Mallau, S.; Viel, S.; Jover, M.; Schmitz, C. Development of Postural Control in Healthy Children: A Functional Approach. Neural Plast. 2005, 12, 109–118. [Google Scholar] [CrossRef]
- Sá, C.D.S.C.D.; Boffino, C.C.; Ramos, R.T.; Tanaka, C. Development of postural control and maturation of sensory systems in children of different ages a cross-sectional study. Br. J. Phys. Ther. 2017, 22, 70–76. [Google Scholar] [CrossRef]
- Villarrasa-Sapiña, I.; García-Massó, X.; Serra-Añó, P.; García-Massó, X.; González, L.M.; Lurbe, E. Differences in intermittent postural control between normal-weight and obese children. Gait Posture 2016, 49, 1–6. [Google Scholar] [CrossRef]
- Peterson, M.L.; Christou, E.; Rosengren, K. Children achieve adult-like sensory integration during stance at 12-years-old. Gait Posture 2006, 23, 455–463. [Google Scholar] [CrossRef]
- Steindl, R.; Kunz, K.; Schrott-Fischer, A.; Scholtz, A. Effect of age and sex on maturation of sensory systems and balance control. Dev. Med. Child Neurol. 2006, 48, 477–482. [Google Scholar] [CrossRef]
- Nowotny, J. Ćwiczenia Korekcyjne w Systemie Stacyjnym; AWF: Katowice, Poland, 2001. [Google Scholar]
- World Health Organization Regional Office for Europe. Adolescent Obesity and Related Behaviours: Trends and Inequalities in the WHO European Region, 2002–2014; World Health Organization Regional Office for Europe: København, Denmark, 2017. [Google Scholar]
- Kułaga, Z.; Grajda, A.; Gurzkowska, B.; Wojtyło, M.A.; Góźdź, M.; Litwin, M.S. The prevalence of overweight and obesity among Polish school—Aged children and adolescents. Przegl. Epidemiol. 2016, 70, 641–651. [Google Scholar]
- Silferi, V.; Rougier, P.; Labelle, H.; Allard, P. Postural control in idiopathic scoliosis: Comparison between healthy and scoliotic subjects. Revue de Chirurgie Orthopedique et Reparatrice de L’appareil Moteur 2004, 90, 215–225. [Google Scholar] [CrossRef]
- Haumont, T.; Gauchard, G.C.; Lascombes, P.; Perrin, P.P. Postural Instability in Early-Stage Idiopathic Scoliosis in Adolescent Girls. Spine 2011, 36, E847–E854. [Google Scholar] [CrossRef]
- Walicka-Cupryś, K.; Skalska-Izdebska, R.; Drzał-Grabiec, J.; Sołek, A. Correlation between body posture and postural stability of school children. Adv. Rehabil. 2013, 27, 47–54. [Google Scholar] [CrossRef]
- Colné, P.; Frelut, M.; Peres, G.; Thoumie, P. Postural control in obese adolescents assessed by limits of stability and gait initiation. Gait Posture 2008, 28, 164–169. [Google Scholar] [CrossRef]
- Hue, O.; Simoneau, M.; Marcotte, J.; Berrigan, F.; Doré, J.; Marceau, P.; Marceau, S.; Tremblay, A.; Teasdale, N. Body weight is a strong predictor of postural stability. Gait Posture 2007, 26, 32–38. [Google Scholar] [CrossRef]
- Wyszyńska, J.; Podgórska-Bednarz, J.; Drzał-Grabiec, J.; Rachwał, M.; Baran, J.; Czenczek-Lewandowska, E.; Leszczak, J.; Mazur, A. Analysis of Relationship between the Body Mass Composition and Physical Activity with Body Posture in Children. BioMed Res. Int. 2016, 2016, 1851670. [Google Scholar] [CrossRef]
- McGraw, B.; McClenaghan, B.A.; Williams, H.G.; Dickerson, J.; Ward, D.S. Gait and postural stability in obese and nonobese prepubertal boys. Arch. Phys. Med. Rehabil. 2000, 81, 484–489. [Google Scholar] [CrossRef]
- Sun, F.-H.; Wang, L.; Wang, L. Effects of weight management program on postural stability and neuromuscular function among obese children: Study protocol for a randomized controlled trial. Trials 2015, 16, 143. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
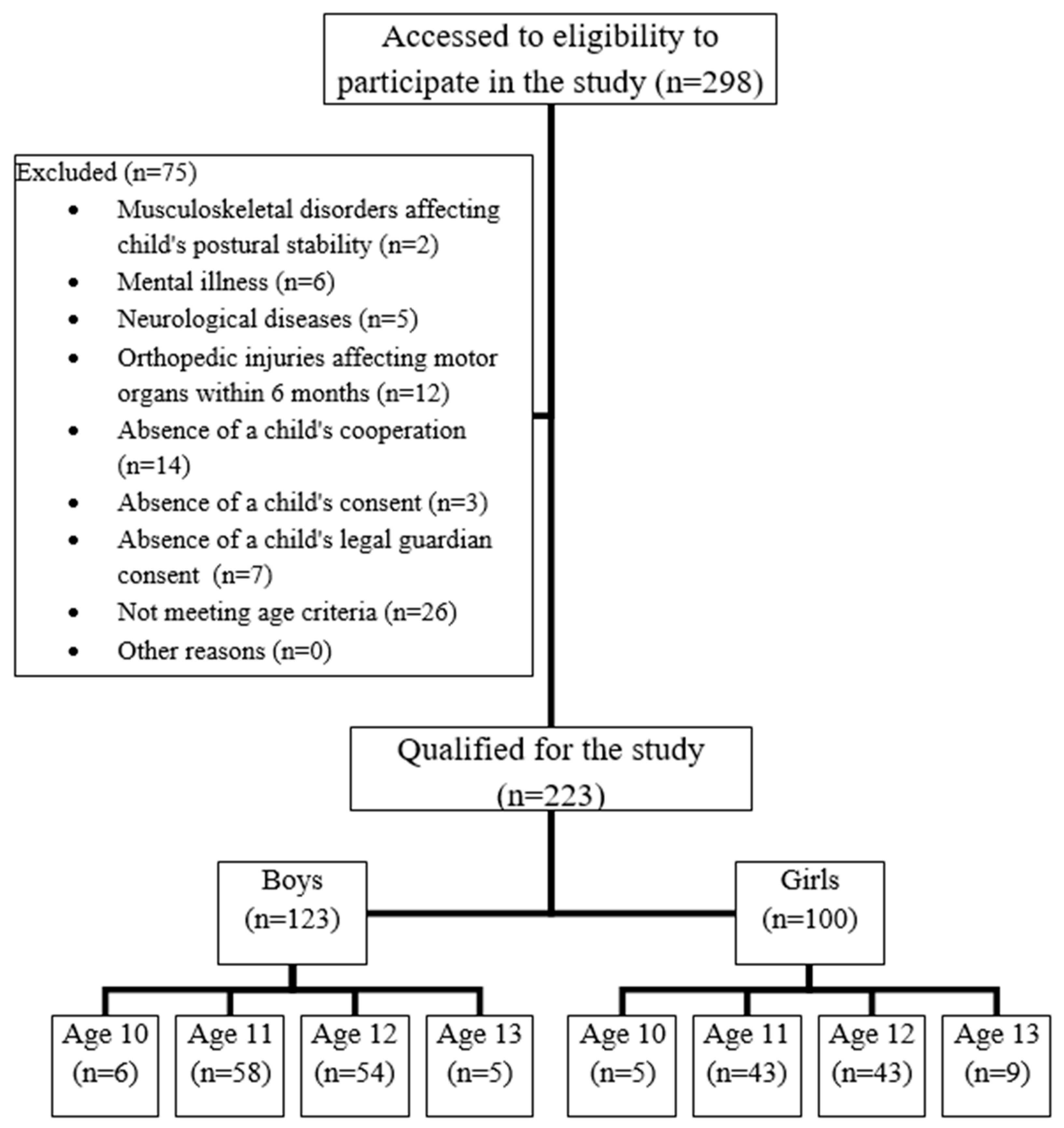
| Variable | Boys (n = 123) | Girls (n = 100) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| X | ±SD | Min | Max | X | ±SD | Min | Max | ||
| Age [y] | 11.46 | 0.66 | 10 | 13 | 11.55 | 0.72 | 10 | 13 | |
| Body mass [kg] | 41.97 | 11.08 | 25.1 | 70.8 | 42.14 | 8.8 | 24.5 | 77.0 | |
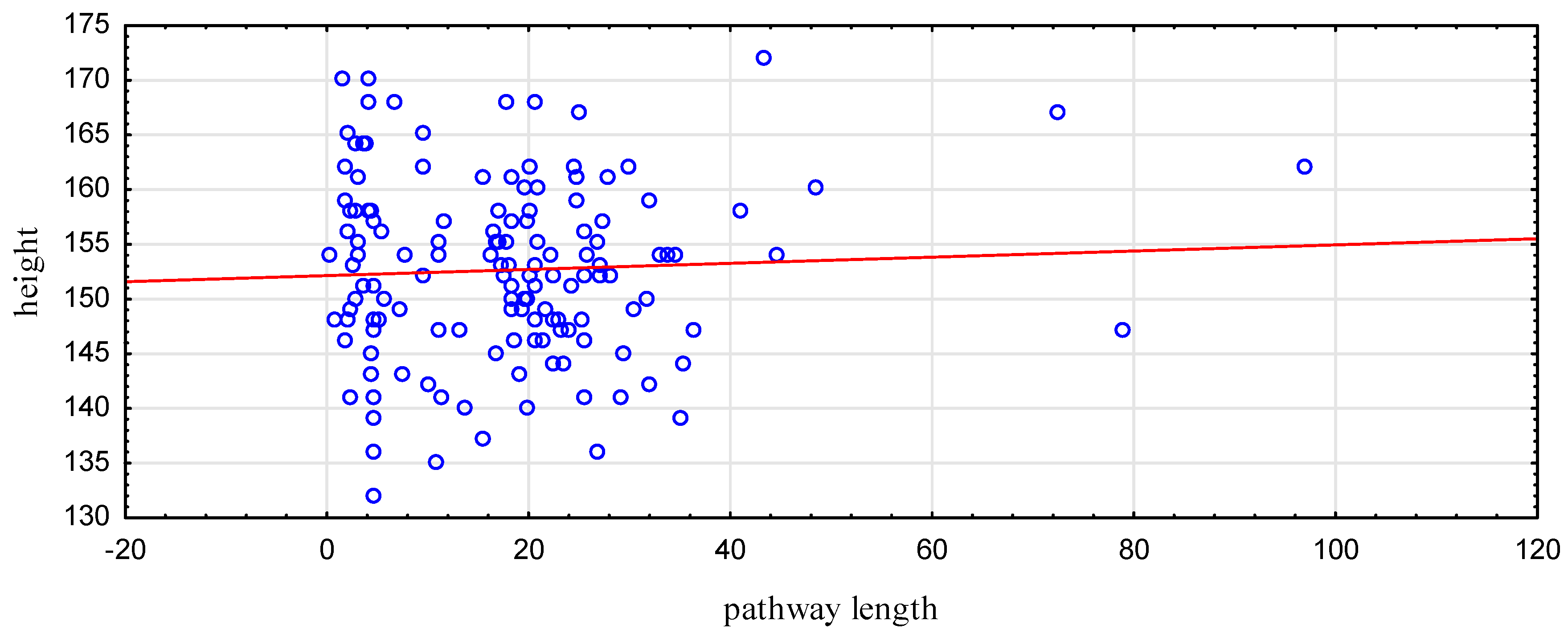
| Height [cm] | 148.63 | 8.88 | 131 | 172 | 147.51 | 9.23 | 125 | 170 | |
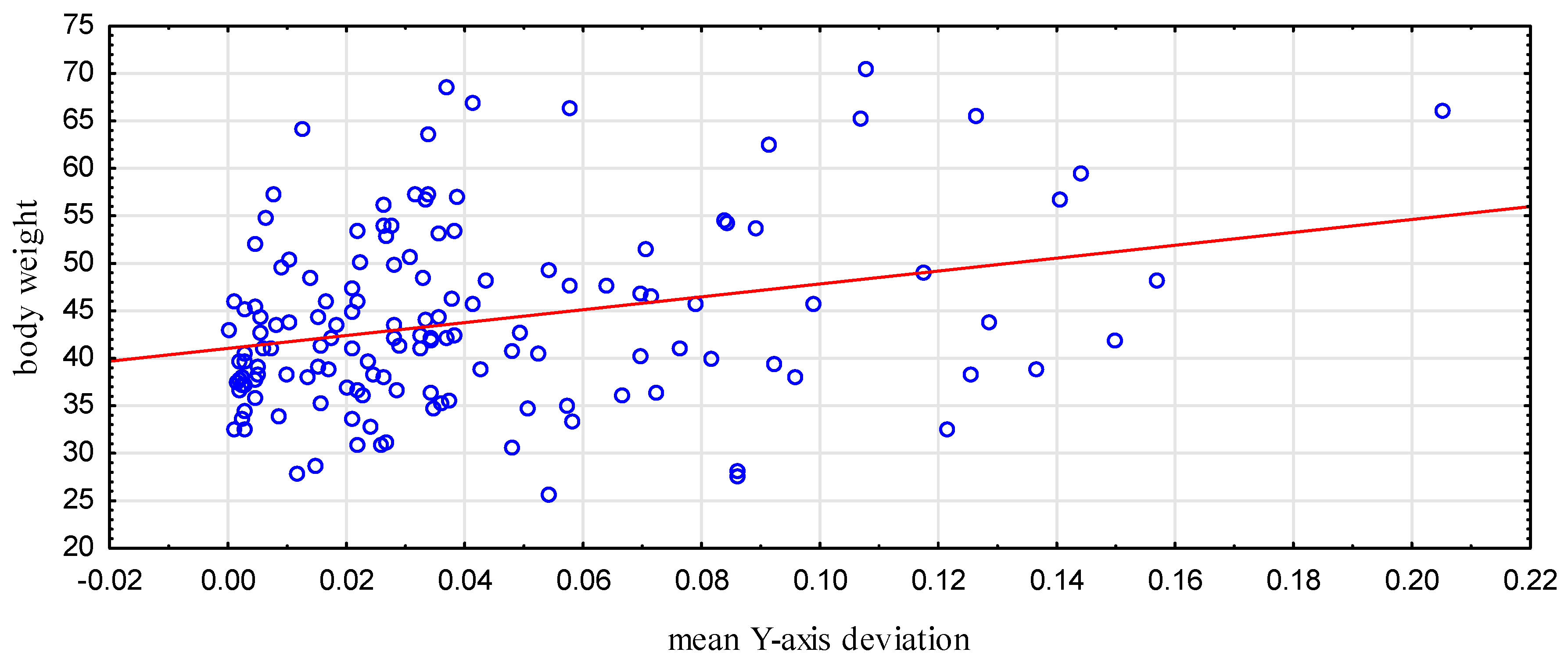
| Mean deviation from the axis | X | 0.072 | 0.06 | 0.004 | 0.308 | 0.07 | 0.06 | 0.001 | 0.29 |
| Y | 0.05 | 0.06 | 0.0003 | 0.269 | 0.05 | 0.04 | 0.002 | 0.27 | |
| Pathway length | 22.78 | 12.85 | 5.87 | 83.2 | 23.28 | 13.81 | 5.69 | 96.95 | |
| Area | 0.88 | 0.56 | 0.1 | 2.76 | 0.89 | 0.49 | 0.1 | 2.49 | |
| Variable | Mean X-Axis Deviation | Mean Y-Axis Deviation | Pathway Length | |
|---|---|---|---|---|
| Entire study group | ||||
| Age | R | −0.006 | −0.05 | 0.07 |
| (p) | 0.93 | 0.42 | 0.28 | |
| Children aged 10 | ||||
| Body mass [kg] | R | −0.33 | 0.26 | 0.011 |
| (p) | 0.37 | 0.72 | 0.97 | |
| Height [cm] | R | 0.1 | 0.5 | −0.27 |
| (p) | 0.77 | 0.19 | 0.61 | |
| Children aged 11 | ||||
| Body mass [kg] | R | 0.18 | 0.03 | 0.12 |
| (p) | 0.07 | 0.79 | 0.23 | |
| Height [cm] | R | 0.16 | 0.02 | 0.07 |
| (p) | 0.1 | 0.86 | 0.45 | |
| Children aged 12 | ||||
| Body mass [kg] | R | 0.17 | 0.37 | 0.13 |
| (p) | 0.1 | <0.001 | 0.2 | |
| Height [cm] | R | 0.05 | 0.17 | 0.2 |
| (p) | 0.6 | 0.09 | 0.047 | |
| Children aged 13 | ||||
| Body mass [kg] | R | −0.03 | 0.46 | −0.07 |
| (p) | 0.92 | 0.17 | 0.84 | |
| Height [cm] | R | 0.18 | −0.29 | −0.28 |
| (p) | 0.59 | 0.37 | 0.4 | |
| Variable | Boys | Girls | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean X-axis Deviation | Mean Y-axis Deviation | Pathway Length | Area | Mean X-axis Deviation | Mean Y-axis Deviation | Pathway Length | |||
| Entire group | Age | R | 0.03 | 0.01 | 0.13 | 0.07 | −0.048 | −0.1 | 0.01 |
| (p) | 0.72 | 0.96 | 0.16 | 0.46 | 0.63 | 0.29 | 0.89 | ||
| Age 10 | Body mass [kg] | R | −0.1 | 0.53 | 0.47 | 0.46 | −0.78 | −0.67 | −0.9 |
| (p) | 0.83 | 0.34 | 0.39 | 0.4 | 0.25 | 0.31 | 0.19 | ||
| Height [cm] | R | 0.25 | 0.75 | 0.41 | 0.47 | −0.8 | −0.63 | −0.84 | |
| (p) | 0.64 | 0.19 | 0.45 | 0.39 | 0.24 | 0.34 | 0.22 | ||
| Age 11 | Body mass [kg] | R | 0.2 | 0.04 | 0.2 | 0.17 | 0.17 | −0.02 | −0.06 |
| (p) | 0.14 | 0.74 | 0.13 | 0.22 | 0.29 | 0.91 | 0.72 | ||
| Height [cm] | R | 0.14 | 0.05 | 0.15 | 0.22 | 0.3 | −0.11 | −0.14 | |
| (p) | 0.3 | 0.66 | 0.27 | 0.1 | 0.053 | 0.49 | 0.38 | ||
| Age 12 | Body mass [kg] | R | 0.03 | 0.33 | 0.1 | 0.13 | 0.37 | 0.45 | 0.17 |
| (p) | 0.84 | 0.02 | 0.45 | 0.34 | 0.02 | 0.01 | 0.26 | ||
| Height [cm] | R | 0.003 | 0.18 | 0.21 | 0.18 | 0.12 | 0.17 | 0.2 | |
| (p) | 0.98 | 0.2 | 0.13 | 0.2 | 0.43 | 0.26 | 0.2 | ||
| Age 13 | Body mass [kg] | R | −0.52 | 0.67 | 0.73 | 0.94 | 0.37 | −0.26 | −0.63 |
| (p) | 0.41 | 0.31 | 0.28 | 0.18 | 0.44 | 0.59 | 0.2 | ||
| Height [cm] | R | −0.16 | −0.02 | −0.07 | 0.72 | 0.32 | −0.75 | −0.37 | |
| (p) | 0.79 | 0.97 | 0.9 | 0.27 | 0.5 | 0.14 | 0.44 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turon-Skrzypinska, A.; Uździcki, A.; Przybylski, T.; Szylinska, A.; Marchelek-Myśliwiec, M.; Rył, A.; Rotter, I. Assessment of Selected Anthropometric Parameters Influence on Balance Parameters in Children. Medicina 2020, 56, 176. https://doi.org/10.3390/medicina56040176
Turon-Skrzypinska A, Uździcki A, Przybylski T, Szylinska A, Marchelek-Myśliwiec M, Rył A, Rotter I. Assessment of Selected Anthropometric Parameters Influence on Balance Parameters in Children. Medicina. 2020; 56(4):176. https://doi.org/10.3390/medicina56040176
Chicago/Turabian StyleTuron-Skrzypinska, Agnieszka, Artur Uździcki, Tomasz Przybylski, Aleksandra Szylinska, Małgorzata Marchelek-Myśliwiec, Aleksandra Rył, and Iwona Rotter. 2020. "Assessment of Selected Anthropometric Parameters Influence on Balance Parameters in Children" Medicina 56, no. 4: 176. https://doi.org/10.3390/medicina56040176
APA StyleTuron-Skrzypinska, A., Uździcki, A., Przybylski, T., Szylinska, A., Marchelek-Myśliwiec, M., Rył, A., & Rotter, I. (2020). Assessment of Selected Anthropometric Parameters Influence on Balance Parameters in Children. Medicina, 56(4), 176. https://doi.org/10.3390/medicina56040176